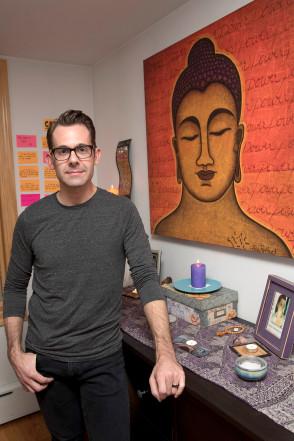
Chad Lewis charges $20 to $25 an hour to assist the gravely ill and their families.
[W]hen Chad Lewis’ mother passed away seven years ago from complications from diabetes, he couldn’t stop thinking about her death. “It wasn’t loving and sweet,” he says. “It was chaotic and angry and scary.”
So Lewis, a 39-year-old who lives in Astoria, set out to find a better way to process the end of life, ultimately making a career shift from Broadway stage manager to death doula.
Doulas who aid women in giving birth have been trendy for years, but now a different type of support person is helping people navigate life’s other major passage. Dying people and their loved ones are hiring death doulas to help them coordinate end-of-life care and vigils, plan funerals and provide a sympathetic but unattached ear.
The profession first came into being in the early aughts and is growing increasingly popular. In 2014, Suzanne O’Brien launched the New York City-based Doulagivers, an online training program for death doulas.
“I can hardly keep up with demand,” says O’Brien, who also holds monthly seminars at an Upper West Side branch of the New York Public Library.
The process usually starts with a patient deciding how they want to die and outlining that with the doulas.
“It’s similar to a birthing plan … Where [do] you want to die? What kind of room you want to die in? What [do] you want to be looking at? What [do] you want it to smell like?” says Shelby Kirillin, 41, a Richmond, Va.-based death doula. She charges between $1,000 and $3,000 as a retainer fee, and asks for payment upfront to avoid chasing down money posthumously. She’ll also work pro bono if a situation merits it.
The “scary” death of Chad Lewis’ mother led him to become a doula.
“I had one young girl say she wanted to die in a yurt,” says Kirillin of a client who’s currently planning her own death. The girl’s cancer condition makes a yurt too impractical, so Kirillin is getting creative. “We decided on mosquito netting over her bed, and twinkle lights to look like stars.” After she takes her last breath, her loved ones will put wildflowers in her hair.
Death doulas also help out after someone passes. Lewis, who charges $20 to $25 per hour, likes to create a basic plan to take care of issues such as child care, grocery shopping and bill payment, to clear up mental space for grieving families.
And more than anything, the professionals help patients process what they’re going through.
“Families buffer pain — you hate to see people you love in pain. And doulas aren’t buffers,” says Kirillin. “Instead of saying, ‘OK, let’s see if we can give you meds,’ I’ll say, yeah, ‘I bet you are in pain. Tell me about it — what does it feel like?’”
When Richmond resident Mel Titus’ best friend of 31 years, Kim, was entering the final stages of her battle with cervical and breast cancers last year, they were introduced to Kirillin.
They were skeptical at first, but Kim (whose last name is being withheld for personal reasons) decided on a death doula so she could manage her death the way she did her life. “She was a processor,” says Titus. “She really liked that she could come up with a plan and do things a certain way.”
And for Titus, Kirillin provided emotional support during an impossible time. “I would have tough days, and I’d call Shelby, and she’d walk me through it,” she says.
Kirillin helped the duo plan Kim’s visitor schedule, and what music they’d play and books they’d read in the final days. Taking care of logistics freed them up to reminisce about Kim’s life, and even laugh about how things were going. “We actually had some funny moments, believe it or not,” says Titus. “It’s sad, but it can be a happy thing, too.”
[I]n the six years since my father died, I’ve visited the cemetery where his ashes are interred exactly twice—the second time only because of the Jewish tradition of unveiling, where the initial graveside funeral service is followed within a year by a ceremony to uncover and dedicate the headstone. It’s not that returning would be too difficult. It’s more like the reverse: I fear an inability to perform the sadness and solemnity the pilgrimage seems to require. I miss my dad, but the cemetery, nestled alongside the highways and strip malls of suburban South Jersey, fails to evoke him in any meaningful way. It’s a site associated with him only retroactively, for the worst of all possible reasons. Where I’m supposed to feel his presence, there’s only a void.
FROM HERE TO ETERNITY: TRAVELING THE WORLD TO FIND THE GOOD DEATH by Caitlin Doughty
Los Angeles-based mortician and writer Caitlin Doughty argues that such feelings result from the failures of America’s death industry, which has become “more expensive, more corporate, and more bureaucratic than any other on Earth.” According to the National Funeral Directors’ association, the median cost of traditional funeral with a viewing and burial was $7,181 in 2014; Doughty cites the current average at $8,000 to $10,000. 14 percent of US funeral homes are run by publicly traded firms. Service Corporation International, the largest funeral services provider in the US, operates over 2,000 funeral homes employing more than 24,000 people. The $20-billion industry often pushes grief to the margins by pressuring families to make a series of high-stakes decisions on a very short timeline—most funeral homes come to pick up a body within an hour of being contacted.
In some cases, funeral homes deliberately exploit families for financial gain at a time of profound vulnerability. A 2013 undercover investigation conducted by the Federal Trade Commission revealed that up to one in five American funeral homes engage in “deceptive and manipulative practices.” The offenders violated the 1984 Funeral Rule, which stipulates that funeral homes must provide itemized price lists. The compulsory bundling of products and services is prohibited: They can’t require that you buy a traditional varnished casket when all you want is a cremation; an inexpensive, unfinished wooden box must be made available. And the law bans the aggressive sale of products that are not required by law, like the use of a hearse to transport remains to a cemetery. Though most funeral homes keep dedicated websites, few display their prices online, which makes it challenging to compare costs.
With its focus on profits, the industry has also changed the way we treat dead bodies. As recently as a hundred years ago, “no one would have questioned a wife washing and dressing the body of her husband,” Doughty writes, “or a father carrying his son to the grave in a homemade coffin.” The Civil War is oftenidentified as the point at which practices began to shift. Embalming became more common as soldiers’ bodies were transported from the South to the North. It gained even more popularity after Abraham Lincoln’s funeral train tour, which took his embalmed corpse to 180 cities between Washington D.C. and Springfield, Illinois. Now, the United States is the only country in the world in which chemical conservation of the dead is common practice—a process that can cost anything from $495 to over $1,000. What was once a practical solution with a historically specific context has become a profitable norm, despite, according to the CDC, providing no public health benefit.
In her book From Here to Eternity: Traveling the World to Find the Good Death, Doughty tries to find a better way to die and to grieve, seeking out death rituals from the Western United States to Japan, Spain, Indonesia, and beyond. It sounds a bit like Eat, Pray, Die, but her project is much larger than its premise first implies. She is searching not for personal spiritual enlightenment or the morbid titillation of thana-tourism, but for practical, radical alternatives to our corporatized death industry. Her travels illuminate a host of compelling possibilities for better funerals and a less fraught relationship with our dead. But the book also reveals a larger failure of our culture to allow for mourning and grieving after the last goodbye. If it is hard to navigate the death care industry, it is harder still to work out how to live with grief.
On her travels, Doughty finds many rituals that involve prolonged contact with corpses—prolonged, at least, by American standards. All around the world, she meets people less troubled by the physical reality of dead bodies, whether those bodies are burned to ash, mummified, “decomposting,” or lying under glass in their natural, un-embalmed state. In Japan she visits a corpse hotel where families may rent a suite that looks like an ordinary condo and “just be with the body, free from the performance required at a formal viewing.” And at the Rinkai crematory, Doughty learns about the practice of kotsuage. According to this custom, families are escorted into a room called a shūkotsu-shitsu after a cremation, where they pick up their loved one’s remaining bone fragments and place them gently into an urn.
In North Carolina, Doughty spends time at Western Carolina University’s Forensic Osteology Research Station (FOREST), where corpses donated to science are turned into compost. The bodies are laid to rest in a wooded research facility, blanketed with alfalfa and woodchips, covered in a silver shroud, and in the hot sun to turn into dark, nutrient-rich soil after a period of weeks. The project is still in its experimental phase, but the FOREST researchers hope it will become a green solution with a therapeutic arc. Families will ultimately be invited to collect the soil made from the body of their loved one and with it, cultivate new life.
Doughty finds her most extreme example of dead body positivity in Tana Toraja in Indonesia. For Torajans, the border between the living and the dead is porous. Corpses frequently remain in the home for a period of weeks, months, or even years, and are cared for like any other member of the family—bathed, fed, dressed, and spoken to. After they are finally buried, following elaborate community funerals, bodies are periodically exhumed during what is called the ma’nene’. Families have the opportunity to reunite, and even picnic, with their dead; they can make animal sacrifices they may not have been able to afford at the time of the original burial. What sounds grisly to some is, to the Torajans, both tender and sacred: “Hauling someone out of their grave years after their death is not only respectful,” Doughty writes, “but it provides a meaningful way to stay connected to their dead.”
Doughty’s chatty calm in the presence of dead bodies and her arguments against American squeamishness are admirable. But it feels, at times, like From Here to Eternity’s focus on death comes at the expense of grief. This is not a failure of the project so much as its shape; the nature of Doughty’s inquiry makes grief a secondary concern. It does appear sporadically: In the chapter on the Day of the Dead, she travels to Mexico with her friend Sarah to visit a mummy museum, as well as the altars families erect to honor the people they’ve lost that year. Sarah is still reeling from the decision to obtain a late-term abortion when her fetus was diagnosed with trisomy 13, and Doughty writes about the isolation of Sarah’s grief, her feeling that the inability to move on from the loss had made her “radioactive” to her friends and coworkers. Her loss, and the future she had imagined, is devastatingly rendered. There is a digression, too, on the Western funeral industry’s fixation on “dignity,” by which they really mean silence, composure, and repression—this, too, is a moment of genuine feeling, and Doughty shows that though her tone is often light, she has the capacity to move and enrage.
But just as often, Doughty fails to engage with the realities of mourning. At an open-air cremation she attends in Crestone, Colorado, she professes to witness the “pall of grief [lifting] from the circle.” I don’t doubt the power of this ceremony. But the implication that it was able to dispel sadness—that such a thing is possible, or even desirable, at a funeral—gives me pause. Worse, in the book’s epilogue, she writes, “A sense of purpose helps the mourner grieve. Grieving helps the mourner begin to heal.” This is a neat, linear progression; in other words, it’s exactly what the experience of grief is not.
There is more to death and dying than funerals.From Here to Eternity is in some ways a missed opportunity to explore how the profit motive has distorted our experience of death—not just burial, but all the feeling that comes after a body is buried. In The Last Word, Julia Cooper writes of the difficulty of grieving under late capitalism. The amorphous, endless, and unpredictable nature of grief puts it fundamentally at odds with pressures “to be efficient, to progress, to—most of all—get back to work.” But, she writes, “mourning doesn’t work that way. There is no timeline because the work of grieving is never done. There is nothing efficient or productive about loss, but there it is all the same.” Grieving is the enemy of work, and we’re expected to suppress the former in the interest of the latter.
Minimizing the pain of personal loss, Cooper argues, is in service of “maintaining productivity for the benefit of a capitalist system.” Public displays of grief are shunned in part because they undermine the relentless positivity our economic system feeds on. The isolation of those who are unable to successfully curb their mourning is “a socially enforced strategy of our neoliberal era.” The repression of grief is also materially enforced: The standard paid bereavement leave, where it does exist, is three days. At Facebook, COO and Lean In author Sheryl Sandberg changed the company’s bereavement policy following the sudden death of her husband in 2015; the company now offers employees a comparatively generous 20 days paid leave following the loss of an immediate family member.
In the op-ed Sandberg wrote for The New York Times about her children’s experience of bereavement, she talks about grief in the language of business. The death of a parent is “adversity”; the word “resilience” is used six times, while “grieving” makes one appearance. Sandberg writes of her son and daughter’s loss (and her own) alongside the story of a friend’s child who was bullied at summer camp, with the implication that both experiences can be “overcome” with the same set of therapeutic tools. Sandberg’s approach isn’t insincere; original or not, the idea that “there is no wrong way to grieve” is an important one. But for those who don’t find this way of thinking helpful, our culture offers few other ways to address grief and work.
Caitlin Doughty’s mission to reimagine the death industry—to cast out our shame and fear of the dead—is an important one, for which she makes the case well and with good humor. More humane and meaningful rituals around death would doubtless ease the transition into the new reality that awaits the living after a traumatic loss. For my part, I look forward to one day spreading what I’ve kept of my father’s ashes, at a site less dour than a New Jersey tomb. But reforming our funeral industrial complex is only the beginning of the work ahead of us.
Despite living in a country that delivers some of the best health care in the world, we often settle for end-of-life care that is inconsistent with our wishes and administered in settings that are unfamiliar, even dangerous. In California, for example, 70 percent of individuals surveyed said they wish to die at home, yet 68 percent do not.
Instead, many of us die in hospitals, subject to overmedication and infection, often after receiving treatment that we do not want. Doctors know this, which may explain why 72 percent of them die at home.
Using data from the Dartmouth Atlas — a source of information and analytics that organizes Medicare data by a variety of indicators linked to medical resource use — we recently ranked geographic areas based on markers of end-of-life care quality, including deaths in the hospital and number of physicians seen in the last year of life. People are accustomed to ranking areas of the country based on availability of high-quality arts, universities, restaurants, parks and recreation and health-care quality overall. But we can also rank areas based on how they treat us at an important moment of life: when it’s coming to an end.
It turns out not all areas are created equal. Critical questions abound. For example, why do 71 percent of those who die in Ogden, Utah, receive hospice care, while only 31 percent do in Manhattan? Why is the rate of deaths in intensive care units in Cedar Rapids, Iowa, almost four times that of Los Angeles? Why do only 12 percent of individuals in Sun City, Ariz., die in a hospital, while 30 percent do in McAllen, Texas?
Race and other demographics in a given area certainly matter. One systematic review of more than 20 studies showed that African American and Hispanic individuals utilize advance-care planning and hospice far less than whites. More research is needed to explore these differences and to close these gaps and demand high-quality, personalized care for people of all races.
But race and demographics don’t provide all the answers. For instance, Sarasota and St. Petersburg, Fla., are only 45 miles apart and have similar ethnic demographics. Yet we found that they score quite differently on several key quality metrics at the end of life.
A variety of factors probably contribute to our findings. Hospice, which for 35 years has provided team-based care, usually at home, to those nearing the end of life and remains enormously successful and popular, is underutilized. Most people enroll in hospice fewer than 20 days before death, despite a Medicare benefit that allows patients to stay for up to six months. Hospice enrollment has been shown to be highly dependent on the type of doctor that you see. In fact, one study among cancer patients with poor prognoses showed that physician characteristics (specialty, experience with practicing in an inpatient setting, experience at hospitals, etc.) mattered much more than patient characteristics (age, gender, race, etc.) in determining whether patients enrolled in hospice. For example, oncologists and doctors practicing at nonprofit hospitals were far more likely than other doctors to recommend hospice.
Also, physicians in a given geographic area are likely to have similar approaches to health care. They may collectively differ from physicians in another area in their familiarity and comfort with offering hospice care to a patient. This may explain why hospice enrollment significantly varies among geographic regions.
Palliative care, which focuses on alleviation of suffering, is often misunderstood by doctors as giving up. Health professionals’ lack of longitudinal, substantive training in end-of-life care only compounds the problem.
Perhaps most important, fewer than half of Americans have had a conversation about their end-of-life wishes — a process known as advance care planning — and only one-third have expressed those wishes in writing for a health-care provider to follow when they become seriously ill. If people do not have a clear sense of their end-of-life wishes, it is easy to imagine that they may be swayed by a physician’s recommendation.
The private sector has led the way in addressing the underutilization of hospice and improving end-of-life care. For instance, health insurers such as Aetna have devised programs integrating nurse-led case management services for seriously ill individuals, reducing costly and undesired emergency room visits while increasing appropriate hospice referrals. And start-ups including Aspire Health are working with communities to provide palliative care in people’s homes while devising algorithms to help payers and providers identify individuals who might benefit from palliative and hospice care.
Congress also is considering bipartisan solutions consistent with best practices. Congressional leaders have recently introduced several pieces of legislation that would test new models of care for those facing advanced illness, support health professionals in training for end-of-life care and ensure that barriers are removed for consumers to access care.
And Medicare, via its Innovation Center, has led the way in testing promising care models to support those at the end of life, including the Medicare Care Choices Model, which allows individuals to receive hospice care alongside traditional, curative treatment.
But the secret sauce may be a shift in culture. We will not improve the death experience until we demand that our public- and private-sector leaders act and that our local health professionals encourage person-centered end-of-life care.
As with any social change, progress will be driven by a growing awareness and a desire for justice among families and patients. There are good and bad places to die in America. However, to ensure a better death for all, we must confront not just geographic disparities but also our resistance to thinking about death.
[T]he news was bad. Mimi, a woman in her early 80s, had been undergoing treatment for lymphoma. Her husband was being treated for bladder cancer. Recently, she developed chest pain, and a biopsy showed that she had developed a secondary tumor of the pleura, the space around one of her lungs. Her oncology team’s mission was to share this bad news.
Mimi’s case was far from unique. Each year in the U.S., over 1.6 million patients receive hospice care, a number that has been increasing rapidly over the past few years. What made Mimi’s case remarkable was not the grimness of her prognosis but her reaction to it.
When the members of the team walked into Mimi’s hospital room, she was lying in bed holding hands with her husband, who was perched beside her on his motorized wheelchair. The attending oncologist gulped, took a deep breath, and began to break the news as gently as he could. Expecting to meet a flood of tears, he finished by expressing how sorry he was.
To the team’s surprise, however, no tears flowed. Instead Mimi looked over at her husband with a broad smile and said, “Do you know what day this is?” Somewhat perplexed, the oncologist had to admit that he did not. “Today is very is special,” said Mimi, “because it was 60 years ago this very day that my Jim and I were married.”
The team members reacted to Mimi with astonishment. How could an elderly woman with an ailing husband who had just been told that she had a second, lethal cancer respond with a smile? Compounding the team’s amazement, she then went on to share how grateful she felt for the life she and her husband had shared.
Mimi thanked the attending oncologist and the members of the team for their care, remarking how difficult it must be to deliver bad news to very sick patients. Instead of feeling sorry for herself, Mimi was expressing sympathy for the people caring for her, exhibiting a remarkable generosity of spirit in the face of a grim disease.
The members of the team walked out of Mimi’s room shaking their heads in amazement. Once they reached the hallway, the attending physician turned and addressed the group: “Mimi isn’t the only person in that room with cancer, but she is surely the sickest. And yet,” he continued, to nods all around, “she is also the healthiest of any of us.”
“Be thine own palace, or the world’s thy jail.” – John Donne
Disease need not define us
Mimi’s reaction highlights a distinction between disease and illness, the importance of which is becoming increasingly apparent. Simply put, a body has a disease, but only a person can have an illness. Different people can respond very differently to the same diagnosis, and those differences sometimes correspond to demographic categories, such as male or female. Mimi is a beautiful example of the ability to respond with joy and gratitude in the face of even life’s seemingly darkest moments.
Consider another very different patient the cancer team met with shortly after Mimi. Ron, a man in his 40s who had been cured of lymphoma, arrived in the oncology clinic expecting the attending oncologist to sign a form stating that he could not work and therefore qualified for disability payments. So far as the attending knew, there was no reason Ron couldn’t hold a job.
Ron’s experience of disease was very different from Mimi’s, a phenomenon familiar to cancer physicians. Despite a dire prognosis, Mimi was full of gratitude. Ron, by contrast, though cured of his disease and apparently completely healthy, looked at his life with resentment, even anger. He felt deeply wronged by his bout with cancer and operated with a sense that others should do what they could to help make it up to him.
Mimi was dying but content with her life. Ron was healthy but filled with bitterness. Both patients had the same diagnosis – cancer – but the two human beings differed dramatically, and so too did their illness experiences. Mimi felt blessed by 60 years of a good marriage, while Ron saw in his cancer just one more example of how unfair life had been to him.
“Death be not proud, though some have called thee Mighty and dreadful, for thou art not so…” – John Donne
The real meaning of health
When the members of the cancer team agreed that Mimi was the healthiest person in the room, they were thinking of health in terms of wholeness or integrity. In fact, the word health shares the same source as the word whole, implying completeness or fullness. Ron felt repeatedly slighted, but Mimi looked at life from a perspective of abundance.
A full life is not necessarily marked by material wealth, power over others, or fame. Many people who live richly do so modestly and quietly, never amassing fortunes, commanding legions, or seeing their picture in the newspaper. What enriches their lives is not success in the conventional sense but the knowledge that they have done their best to remain focused on what really matters.
Mimi easily called to mind many moments when she and those she cared about shared their company and their love. Any sense of regret or sorrow over what might have been quickly gave way to a sense of gratitude for what really was, still is, and will be. Her outlook on life was shaped by a deep conviction that it had a meaning that would transcend her own death.
When someone has built up a life ledger full of meaningful experiences, the prospect of serious illness and death often do not seem so threatening. For Mimi, who had lived most of her days with a keen awareness that they would not go on forever, death’s meaning had been transformed from “Life is pointless” to “Make every day count.”
Mimi regarded the prospect of dying as a lens through which to view the meaning of life. She saw her illness as another adventure through which she and Jim would pass. Death would separate them, but it would also draw them closer together, enabling them to see more clearly than ever how much their love meant to them.
From Mimi’s point of view, death is not a contaminant, fatally introduced to life at its final stage. Instead death is a fire that burns away all that is not essential, purifying a person’s vision of what is most real and most worth caring about. Though not happy to be ill, Mimi was in a profound sense grateful for death. Her sentiments echo those of the poet John Donne:
“One short sleep past and we wake eternally: And death shall be no more; death, thou shalt die.”
As a doctor, Diana Anderson has often used the phrase, but rethinks it after losing a loved one
By Diana Anderson
“It was a good death,” the doctor said after one of our patients passed away while I was a resident physician on the night shift. The same line, I remembered, ends one of my favourite movies, Legends of the Fall, when Brad Pitt’s character dies at an old age from a bear attack.
My role throughout the night had been to adjust the medication. I would frequently check on my patient’s vital signs and update his family huddled at the bedside of the elderly man.
“How long will it be, Doctor?” they would ask each time I approached.
But I could not say for certain. “Most likely a few more hours, or less,” I would reply, based on the vital signs, the medications but mostly on a clinical gestalt I was learning.
As a physician-in-training, I would go on to use the “good death” expression. At that time, it carried a meaning of death free from lines and tubes, medications administered for comfort and family at the bedside. But I question this expression now, after the death of Baba, my grandmother.
Baba lived alone in her house, feeding her backyard birds and squirrels religiously, and reading The Economist and National Geographic regularly.
My sister and I were lucky to have a grandmother by our side as children and even luckier to have her with us so far into our adult years as a guide and confidante. Baba and I kept in touch with frequent calls and weekly letters by mail. Through writing, she and I shared a unique bond. In the last letter I wrote her, I told her how much her life had impacted and touched us. For me, that meant inspiring a role working with older people.
Shortly after her 97th birthday, Baba fell and was no longer able to live on her own. I moved into her small house for two weeks as we secured a bed at a nearby nursing home. Even after working as a physician for days at a time without sleep, nothing could compare to the exhaustion I felt as a full-time caregiver.
Each time I changed her diapers, Baba became tearful, saying she felt humiliated and was a burden. Nevertheless, she found a way to laugh, recalling that she had changed my diapers as an infant and now “I am the baby who needs changing.” We chuckled over that each evening.
In the nursing home, her frailty seemed to increase rapidly. She was sad and cried often. Living in one room was “not really life,” she said to me a few days before she died.
She was suffering, but the best medicines seemed to be not what physicians could prescribe. It was the family visits, access to sunshine, nature views and the pet-therapy sessions – those brought smiles and a certain calmness that no pharmaceutical therapy ever could. The day before she died, she told me to “live life to the fullest, even if that means experiencing pain and heartache in addition to the joy and happiness.”
Baba wished often to simply fall asleep and not wake up and had concerns over how she would die. “I am ready to go,” she would say to me, “I have no more purpose.” I would tell her she was greatly needed, as the anchor to our little family – our supply of strength and endurance. She served as the one to go to for a listening ear and for her life wisdom. We were not ready to let her go.
One day, I got the call.
“You should come now. We think she is dying.” How many times have I made that same call to families, to tell them to come in but to drive carefully?
We did not drive carefully or slowly that night. A second call minutes later stated that, after some oxygen, she had regained her mental status and was speaking again, so perhaps I did not need to come back. The gas pedal was pressed even harder, the doctor in me knew too much to be comforted by those words.
Baba died 18 hours later.
Although she was still lucid when I arrived, she was in pain and visibly distressed. When I took her hand, she knew my name, but asked if she must be dreaming. “No, it’s not a dream, Baba, I am here.”
Overnight, there were limited orders for palliative medications. As a physician, I felt powerless and assumed my role as granddaughter. By morning I called my family and said they should come.
The day-shift palliative nurse immediately assessed the situation and ordered medications. She then asked me when to administer them. I knew that once we began, Baba would be with us less and less. My parents, sister and our dog, Bilirubin, assembled around her bed. Baba’s eyes lit up to the sensation of Bili’s furry coat on her hand. She knew our names. “Go ahead,” I said to the nurse.
Over the next few hours, Baba’s breathing slowed considerably. Dying takes time. Each time I thought her last breath came, she would then take another. When no breaths came for many minutes, I put my head on her chest and felt nothing – no heartbeat, no breath and no life.
After her death, I cried often for many days.
As a physician, I would call what Baba went through a “good death.” She passed away almost as she had wished, as if she had simply fallen asleep. She did not experience a massive heart attack or stroke, she did not endure trauma and she was not bedridden with painful lines and tubes. She had her whole family around, her hands were held and she was told she was loved. How could this be anything but a good death?
But as a family member, I wouldn’t call this a good death. It was simply a difficult death. There really is no other kind of death when you lose someone so close. Perhaps the last line in the movie should not have been that it was a good death, but rather, “It was a good life.”
David Wynn, 62, and Carolyn Lyon, 74, in Santa Ana, Calif., volunteer at a hospital where they accompany patients who are near death and don’t have loved ones to be with them in their final hours.
[W]hen patients are near death, and don’t have loved ones to be with them, David Wynn and Carolyn Lyon rush to the hospital.
“They have no one for various reasons, you know, they’ve outlived family, they’ve never married,” Lyon says.
For about six years, Lyon has been comforting patients in their final hours at St. Joseph Hospital in Orange, Calif.; for Wynn, it’s been about nine years.
“For some reason I always wonder about the person’s mother,” David Wynn says. “She saw him first, and I saw him last. It was her and me that are the bookends of this person’s life. So each time that I leave a patient who has died, there is this element of sadness.”
But this kind of work also has its rewards. Wynn remembers one man who was estranged from his family.
“I was sitting there with him and I heard somebody at the door. Turns out it’s his son,” Wynn says. “And he, I guess, felt a little bit uncomfortable, and so he asked me to stay.”
Then, the patient’s daughter came in. “These are people who hadn’t seen each other in maybe 10 or 20 years,” Wynn says.
While the family members exchanged apologies, Wynn recalls the daughter saying, “I don’t even know why I was angry at you, I don’t even remember.”
“And they said, ‘We’re going to try to be a family again,’ ” Wynn says.
“You know, we talk about the last senses to go would be the sense of touch and hearing,” Wynn says. “And I hope that there was enough left of the dad that he had some sense that this bad situation had been healed through his death.”
Wynn says he felt honored, simply to witness that reconciliation, at the end of the man’s life.
[O]nly a tiny percentage of Canadians who’ve received medical assistance to end their lives has chosen to self-administer a lethal drug cocktail.
But that could change now that secobarbital — the drug most commonly used for assisted suicide in other countries — is available in Canada.
Secobarbital is considered the best way for suffering individuals who want to control the manner of their death as much as possible, including administering the medication themselves.
“It’s kind of the barbiturate of choice because (its) quicker onset and duration is such that the dying period is reduced,” said Dr. Stefanie Green, president and co-founder of the Canadian Association of MAID Assessors and Providers.
“Much of the other recipes cause an extended dying period to happen, which is not always successful.”
Health Canada reports that from June 2016 to June 2017 — the first year in which medical assistance in dying (MAID) was legal in Canada — a total of 1,982 individuals received an assisted death. Of those, just five were self-administered deaths.
Green said the unavailability of secobarbital may, at least in part, explain the small number of self-administered deaths.
In general, orally ingested drug cocktails present some difficulties that are not associated with those injected intravenously: they taste bad, they can induce nausea and vomiting, the patient can fall asleep before the entire dose is consumed, which can ultimately cause it to be ineffective.
“You want to mitigate those factors as best as possible,” Green said. “So if you’re going to choose to use a barbiturate and an oral cocktail, this (secobarbital) would be the best one.”
Among other things, she said secobarbital is more soluble than other barbiturates, meaning it can be dissolved in a smaller volume of liquid, thereby reducing the risk that patients won’t consume the entire dose.
Green expects that self-administered deaths will increase somewhat now that secobarbital is available.
“There are certainly a significant amount of people who want to be the ones to have the control, who want to be the ones with the medication in their hand, who want to say, ‘I’m going to take this to my backyard and drink it when I darn well please, thank you very much,”‘ she said.
The drug may be particularly helpful in rural or remote areas where it may be difficult to find a nearby physician or nurse practitioner willing to provide an assisted death, Green added. Individuals in those areas may find it easier to get a prescription for a lethal dose of secobarbital that they can administer themselves.
Because it is fast-acting, secobarbital may also make the self-administration option more viable in a province like British Columbia, where Green practices and which requires a physician to be present throughout the assisted dying process, even when the patient self-administers the medication. That was not feasible when the barbiturates used could take hours, or even days, to work, she said.
Secobarbital, once widely used as a sedative decades ago, has not been available in Canada for years. That it is now is largely due to Jocelyn Downie, a professor of law and medicine at Dalhousie University and a passionate advocate of medical assistance in dying.
When she realized few people were using the self-administration option, Downie said she explored ways to make secobarbital available. She discovered that the cost and time required to get the drug approved for marketing in Canada was a big obstacle so she found “an alternate path:” persuading a pharmaceutical products company to provide the active ingredients for the medication that can be compounded, or mixed, by a pharmacist to produce secobarbital.
Since the company doesn’t want its name publicized, Green said her organization is acting as “the middleman.” It will provide the necessary contact information to health care providers and pharmacists who are helping patients who choose the self-administered death option.
“For those of us in the field, it’s good news, it’s very good news to be able to offer this extra option to our patients, some of which we know will take it and we’ll be happy to provide a better quality product for them,” said Green.