Taboos around death and dying are increasing the risk of elderly patients “on their dying journey” being subjected to unwanted and invasive medical procedures against their wishes, experts say.
Associate Professor Magnolia Cardona, from the Gold Coast’s Bond University, has led a PhD study into the use of rapid response system treatments on elderly hospital patients nearing end of life.
Professor Cardona said the research, published in the Joint Commission Journal on Quality and Public Safety, studied the files of more than 700 patients who received calls for medical emergency teams during hospitalisation at a large Sydney teaching hospital.
A medical emergency team usually consists of two or three specialists from the intensive care unit focused on maintaining life when a patient is in a hospital ward.
The research further focused on patients aged 80 and over, and found that 40 per cent were subjected to invasive procedures such as intubation, intensive monitoring, intravenous medications, transplants and resuscitation attempts.
Ten per cent of those patients already had medical orders in place limiting treatment, or requesting do-not-resuscitate.
“Those orders … are usually issued by their doctors in consultation with families,” Professor Cardona said.
Professor Cardona said the research showed the conflict between increasingly rapid medical advances, public perception of the capabilities of medical experts to revive or prolong life, and the emotive issue of death.
The findings were similar to those of 2017 studies conducted in Europe, but Professor Cardona said the Australian researchers had expected to find a smaller percentage of such incidents.
The research found that elderly patients in their last year of life were frequent users of ambulance and hospital services, including intensive care units, and that health professionals often felt under pressure to administer “aggressive” treatments.
“Health professionals do not always fully discuss a prognosis with families, or may lack the confidence to discuss patients’ preferences for care and treatment at the end of life,” the research said.
“They may decide to continue intensive treatment based on concerns about the family’s legal or emotional reactions, or in an attempt to avoid an in-hospital death, generally perceived as a ‘failure’.”
“Often these frequently heroic medical interventions do not improve patient survival and instead prolong suffering and adversely affect the quality of death.”
The study found that while patients under 80 years of age may benefit from such aggressive techniques, patients over 80 were less likely to benefit.
Professor Cardona also said it was critical that families and elderly people, or people with terminal illnesses, had open conversations about the decisions ahead, and wrote on paper their personal wishes, or appointed someone trusted as their medical representative.
Due to techniques such as CPR being treated as a cure-all on television shows and movies, Professor Cardona said the public often had some misconceptions about the safety and appropriateness of such techniques, particularly for elderly people.
She said the research would hopefully encourage both families and medical professionals to have fresh conversations about patient needs and values, and ensure the wishes of elderly patients were respected as they neared the end of life.
Professor Cardona said she hoped medical professionals could also think critically about the “do no harm” principle when faced with patients facing death of natural causes.
“The conclusion of the study that perhaps clinicians need to take a step back when they identify these flags of imminent death and offer a different alternative of management,” she said.
“That is the pathway of care of comfort care, and that includes giving the patient pain relief, other symptom control, psychosocial support and grief counselling for the families.
“And all of these of course preceded by an honest conversation with the patient and family about the poor prognosis, the inevitability of death and the fact that not every death should be considered a failure.
In 1998, Cindy Spence watched in horror as her hospitalized, cancer-stricken father-in-law was denied the massage he desperately requested. Then and there, the Texas woman’s career path became clear.
“He entered a pain-filled and despondent state in which the only thought that gave him any pleasure at all was to have a hospice therapist come to his hospital room,” Spence recalls. But in 1998, massage therapy was contraindicated for cancer patients. The thinking was that massage would spread cancer cells or might break a tumor.
“That just felt wrong to me,” Spence says.
Now Spence is one of hundreds of hospice massage therapists nationwide, working at the T. Boone Pickens Center at Faith Presbyterian Hospice in Dallas. MK Brennan, president of the Society for Oncology Massage, estimates that at least 250 U.S. hospitals provide hospice massage, and the number is growing.
According to the American Massage Therapy Association (AMTA), massage therapy was a $16 billion industry in the country in 2017 — more than twice the revenues of a decade earlier.
“Ever since the 1940s and ’50s, we’ve been working to establish ourselves as health care providers rather than adult entertainers,” Brennan says.
This perception had changed little when massage therapist Irene Smith basically launched the hospice massage field in 1982. Nor had the other part of the equation — hospice care — caught on.
“You had two topics within the field that have been very scary to the general public,” Smith says. “Massage was not a mainstream modality of care for many, many years, and death has never been a dinner-table conversation until the past decade.”
It didn’t help that, at least literally, we were not a “touchy-feely” society.
“Touch has been very misunderstood,” Smith says. “Touch is in the forefront of neuroscience, with more information coming to the mainstream public in relation to the positive outcomes of being touched. More and more people are becoming aware of its benefits from birth to death.”
That’s why Smith founded the influential California-based Everflowing program, whose mission is “to teach mindful touching and the practice of therapeutic presence as opportunities to recognize and express tenderness in caregiving.”
The Public Presses the Issue of Hospice Massage
Integration of massage at medical facilities often requires public demand. As hospice massage therapists toiled as freelancers and volunteers, patients and their families saw the benefits of the practice and increasingly have come to insist on it.
“We have seen a definite acceptance and growth for requesting massage,” says Meg Robsahm, an independent hospice massage therapist in Rochester, Minn. “We have also seen an increase in hospice companies adding it to their service menus simply because of demand.”
Massage therapist Theresa J. Herman of Allina Health’s hospice program out of Minneapolis has observed a similar progression.
“I started as a volunteer. The patients were beginning to ask for this, so all the big [facilities] realized they couldn’t provide coverage with just volunteers,” Herman says. “Insurance wouldn’t cover it, so we had to come up with donations, philanthropy or pulling it out of little corners of the budget.”
Still, Brennan says, staff positions for hospice massage therapists remain relatively limited, and there are few signs that insurers will start including it in their standard coverage. On the contrary, independent massage therapists are strongly advised to buy liability coverage to work in hospice care.
Touching in Many Ways
At least for now, advocates for hospice massage have research on their side.
According to the AMTA, a 2014 study focused on integrating massage therapy into palliative care found “statistically significant changes in pain, anxiety, relaxation and inner peace of patients, decreasing both pain intensity and anxiety while increasing the patients’ sense of relaxation and inner peace.” (Palliative, or comfort, care is appropriate for people of any age at any stage of a serious illness. Hospice care is generally for those who have six or fewer months to live and who are no longer receiving active treatment.)
The study’s results are why these therapists recognize that their role is, as Smith puts it, “to comfort — not cure — to validate, to honor, to soothe and to respect.”
Other therapists often point to the wide-ranging, even holistic nature of their work.
“The dying process involves physical, spiritual, mental and emotional pain,” Spence says. “RNs can work with the physical pain, chaplains with the spiritual pain and social workers with the mental and emotional pain. I feel that massage and music therapy are the only ones that treat all of those modalities.”
Getting the Family Involved
Smith and her peers strive to have family members present during hospice massage sessions, not just to observe but to participate — to learn how to be gentle with touch.
“Families sometimes have no way to connect with their loved ones, and massage can offer that connection,” Robsahm says. “It can bring a sense of peacefulness in the end stages.”
Families are generally relieved that their loved ones are finding relief and relaxation.
“Especially as someone is close to death — say 48 hours — if I’m in the midst of that family and they’re interested, I will have them sit next to me and have them do what I do,” Robsahm says. “At a certain point, my time will be up, and they will get to be the person to hold their hand, stroke their neck, put oil or lotion on their feet.”
The patient and the family are not alone in reaping something profound out of the experience, according to Spence.
“I have made a commitment to find every ounce of joy,” Spence says. “I knew when I came in that there would be a lot of sorrow, but I didn’t know I would laugh with patients and their families as much as I have.”
Or, as Robsahm puts it: “It moves beyond physical contact. We touch people’s bodies, and in the end, we touch them in their soul.”
Our mortality is not something to be overcome. It is integral to our humanity.
By Allison Arieff
Consider this fact of modern life: Nearly all of the technological products that we buy and use are designed with planned obsolescence in mind. They are built specifically to fail after a relatively short period — one year, two, maybe five. If you doubt that, think about how often you have to replace your smartphone. Gadgets are designed to die.
The irony, however, is that the same Silicon Valley culture that produces these gadgets seems to be obsessed with living forever.
Today’s “life extension” movement includes venture capitalists like the tech billionaire Peter Thiel pouring money into anti-aging and life extension start-ups. (While the rumor that Mr. Thiel receives regular blood transfusions from 18-year olds turned out to be false, there is, of course, an actual company — Ambrosia Plasma — that provides young plasma infusions for $8,000 a liter.) And Google launched the biotech company Calico to increase its “understanding of the biology that controls lifespan,” and bolstered that goal by conducting research on the long-living naked mole rat, a species that shows little to no signs of aging.
In recent years, the lure of disrupting death has become a hot industry. Paul Bennett, a partner at the design consultancy IDEO, was among the first to tap into it. A profile in The California Sunday Magazine in 2015 described an epiphany he had: “ ‘Oh,’ he told himself. ‘You need to redesign death.’ ” Since then, an entire new market has flourished. Death as a conduit for innovation. Death as a participatory exhibition. Death as the organizing principle for networking dinners. Death as an app.
There are now people who refer to themselves as “longevity entrepreneurs,” who see death not as a problem but rather as something to be eliminated. Instead of pursuing a good death, why die at all? Beneath the surface of this quest for eternal life seems to be an unwillingness on the part of its proponents to imagine the world without themselves in it.
In a very fundamental way, this tendency is inhuman.
In her new book, “Natural Causes: An Epidemic of Wellness, the Certainty of Dying, and Killing Ourselves to Live Longer,” Barbara Ehrenreich writes: “You can think of death bitterly or with resignation, as a tragic interruption of your life, and take every possible measure to postpone it. Or, more realistically, you can think of life as an interruption of an eternity of personal nonexistence, and seize it as a brief opportunity to observe and interact with the living, ever-surprising world around us.”
I was taken by Ms. Ehrenreich’s formulation, this notion that our experience of life, though unique to us, is just part of a broader continuum. Our time here is but a blip, and when we leave, the great world continues to spin. As such, the appreciation of our own lives has much to do with the ever-increasing awareness of its relative brevity. It is this — an awareness and acceptance of our own mortality — that makes us human. And it is the impetus, I’d argue, for living our lives to the fullest.
There was a brief period in my own life — less than two years — in which I got married, lost my mother to cancer, had a miscarriage, bought a house and gave birth to a child. Experiencing all this in so short a time span made me feel almost too human. That barrage of ends and beginnings left me intensely aware of the fragility of life as well as enthralled by the glorious intensity of it: I lost and simultaneously gained so much. Today this awareness of the temporal nature of it all leaves me determined to seize, observe and interact with the days that remain. It is the knowledge of how quickly, sometimes tragically, things can change or disappear that fuels my urgency to be in the present.
As a teenager I remember lamenting how horrible and unfair life was, only to have my parents respond that one couldn’t appreciate the good without experiencing the bad. Back then, hearing that was annoying; as an adult, it remains annoying, but it is also completely true.
It is rare for us to give much thought to the challenges we would face if there were no end to our time on earth. Would the condition of our bodies affect the condition of our minds? Would everyone live forever, or just those with the means to afford it? Could you opt out of eternal life? Would inequality dissolve, or would it become even more of an intractable problem? Would we still gain the empathy, wisdom and insight that can come with age?
Technological breakthroughs can be life-changing. But I believe that our humanity — our humanness — is inextricably intertwined with the fact of our mortality. And no scientific fountain of youth can ever cause that to change.
Is it better to declutter and move to something smaller long before the inevitable happens?
By Rebecca Huntley
Four years ago, a dear friend of the family, ‘Jane’, died of bowel cancer.
Jane had helped me around the house and looked after my first daughter, from the time she was a baby up until she went to school. We kept in touch over the years, and soon after my twins were born, she got the diagnosis.
The last time I saw her she was frail and could barely walk.
Sitting on the couch together in her daughter’s apartment, she took my hand and said, “Everything I have left I am wearing. I’ve got rid of the lot. I don’t want the kids to have to mess around with all my things when I’m gone”.
I was so impressed, not just by Jane’s organisation and foresight (which I knew all about), but by her generosity.
Leaving very few possessions behind was one of the greatest parting gifts she could give to her children.
Since then I’ve been thinking a lot about the things we leave behind when we die.
By ‘things’, I don’t mean the intangibles like the life lessons, memories and enduring love that sustain family and friends. Or the legacy of work done in our professional lives or the unpaid work in the community.
But the actual things. Candlesticks. Sporting trophies. Mugs.
You know, the kind of items that we occasionally wonder might be worth some mind-boggling sum if we ever managed to take them to an Antiques Roadshow. The millions, maybe billions of items, continuously gathering dust in the houses and apartments across the nation.
Of course, it has something to do with my stage of life.
As I head towards 50, I see many of my friends going through the emotionally draining and physically exhausting process of helping a sick or widowed parent pack up and sell a family home.
Friends tell me about the days and nights spent working through boxes and boxes of candlesticks, sporting trophies and mugs with an ailing or grieving parent.
And spending days working out what goes in the bin, gets donated to charity, given away or taken to the next dwelling, which is by necessity a half or a quarter of the size of the home they’re leaving.
“No candlesticks, just memories.”
It’s also a story echoed in the research I do with Australians.
And, on the whole, a story mostly told by daughters and granddaughters. In fact, I’ve found it’s largely these women responsible for this forced decluttering and managing of parents’ affairs at this time of life.
It takes its toll on these women, not just physically and emotionally, but even financially as they have to pull back from work to play this caring role.
It often comes at a time when the daughters are at the tail end of caring for their own children. A time when they thought they might have a chance to increase their paid work, or spend time and energy on personal goals.
Then suddenly, these women have responsibilities to parents almost as demanding as those associated with small children — with all the uncertainty and disruption, and far less of the joy that comes with looking after little ones.
In my role as a social researcher, I’ve met mothers trying to support a child through a final year of school — at the same time as helping a widowed parent find retirement living and pack up and sell their family home.
Death-induced decluttering. At the very moment you should be taking time and energy to grieve, you are knee-deep in cardboard boxes and vintage knick-knacks.
Decluttering is a global trend in affluent countries like Australia, led by a slew of ‘less is more’ advocates like author Marie Kondo and Oprah’s organising guru, Peter Walsh.
There’s Swedish death cleaning, döstädning, which is the practice of mindfully clearing out one’s own possessions during later years.
Not to mention the influential effects of the ABC’s War on Waste and how it’s challenging all of us to be more aware of what we buy and what we toss.
Death cleaning helps those family and friends we leave behind, but it’s emotionally draining and physically exhausting.
They’re all terrific developments. Although I worry that these messages sometimes get framed in terms of ‘good taste’ and ‘shame’.
Is it easier for some of us to declutter than it is for others? Is there a ‘clutter divide’ where the more affluent you are, the easier it is to live with less?
A single wealthy man who can afford a sparsely and elegantly decorated apartment in the centre of the city can certainly make do with fewer things, compared to a larger family living in the suburbs without social and cultural amenities within walking distance.
That said, visiting thousands of houses all over Australia for my work has made me realise many of us are living in homes full of things we find hard to get rid of — that is, until something forces us to.
Downsizing in a crisis (death, financial difficulty, illness) is doubly distressing.
I wonder whether it makes better sense to chuck the stuff and move to something smaller long before the inevitable happens.
If I am lucky enough to die of old age, I know what I want to leave behind. Saying goodbye to Jane on that couch confirmed it for me.
I will shuffle off this mortal coil with nothing left but a silk nightie, some precious paintings on the walls around me, and a handful of photos in my bony hands.
Aaron McQ, 50, sits in his Seattle apartment on Jan. 31. The interior and urban designer had been battling leukemia and a rare form of amyotrophic lateral sclerosis, or ALS, for five years.
A former world traveler, triathlete and cyclist McQ had been in pain and physical decline for years. Last fall, he decided to use Washington state’s 2009 Death With Dignity law to end his suffering.
In the end, it wasn’t easy for Aaron McQ to decide when to die.
The 50-year-old Seattle man — a former world traveler, triathlete and cyclist — learned he had leukemia five years ago, followed by an even grimmer diagnosis in 2016: a rare form of amyotrophic lateral sclerosis, or ALS.
An interior and urban designer who legally changed his given name, McQ had been in pain and physical decline for years. Then the disease threatened to shut down his ability to swallow and breathe.
“It’s like waking up every morning in quicksand,” McQ said. “It’s terrifying.”
Last fall, McQ decided to use Washington state’s 2009 Death With Dignity law to end his suffering. The practice, approved in seven states and the District of Columbia, allows people with a projected six months or less to live to obtain lethal drugs to end their lives.
Although the option was legal, actually carrying it out was difficult for McQ, who agreed to discuss his deliberations with Kaiser Health News. He said he hoped to shed light on an often secretive and misunderstood practice.
“How does anyone get their head around dying?” he said, sitting in a wheelchair in his apartment in late January.
More than 3,000 people in the U.S. have chosen such deaths since Oregon’s law was enacted in 1997, according to state reports. Even as similar statutes have expanded to more venues — including, this year, Hawaii — it has remained controversial.
California’s End of Life Option Act, which took effect in 2016, was suspended for three weeks this spring after a court challenge, leaving hundreds of dying patients briefly in limbo.
Supporters say the practice gives patients control over their own fate in the face of a terminal illness. Detractors — including religious groups, disability-rights advocates and some doctors — argue such laws could put pressure on vulnerable people and that proper palliative care can ease end-of-life suffering.
Thin and wan, with silver hair and piercing blue eyes, McQ still could have passed for the model he once was. But his legs shook involuntarily beneath his dark jeans and his voice was hoarse with pain during a three-hour effort to tell his story.
“How do you decide?”
Last November, doctors told McQ he had six months or less to live. The choice, he said, became not death over a healthy life, but a “certain outcome” now over a prolonged, painful — and “unknowable” — end.
“I’m not wanting to die,” he said. “I’m very much alive, yet I’m suffering. And I would rather have it not be a surprise.”
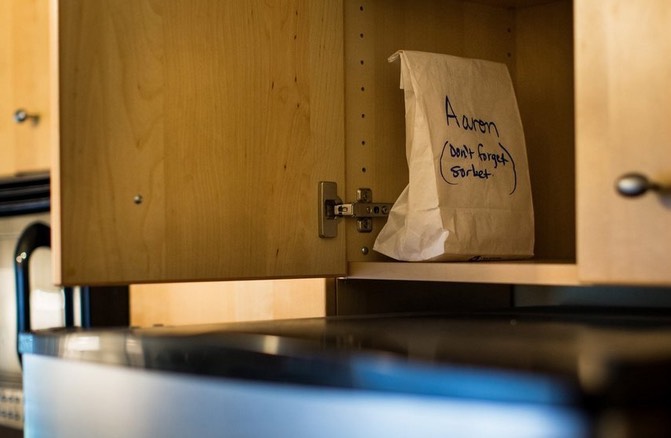
In late December, a friend picked up a prescription for 100 tablets of the powerful sedative secobarbital. For weeks, the bottle holding the lethal dose sat on a shelf in his kitchen.
“I was not relaxed or confident until I had it in my cupboard,” McQ said.
Aaron McQ stored his aid-in-dying prescription in a brown paper bag in the cabinet above the refrigerator. He filled the prescription in late December, planning to use them within weeks. The hard part was deciding exactly when to die.
At the time, he intended to take the drug in late February. Or maybe mid-March. He had wanted to get past Christmas, so he didn’t ruin anyone’s holiday. Then his sister and her family came for a visit. Then there was a friend’s birthday and another friend’s wedding.
“No one is ever really ready to die,” McQ said. “There will always be a reason not to.”
Many people who opt for medical aid-in-dying are so sick that they take the drugs as soon as they can, impatiently enduring state-mandated waiting periods to obtain the prescriptions.
Data from Oregon show that the median time from first request to death is 48 days, or about seven weeks. But it has ranged from two weeks to more than 2.7 years, records show.
Neurodegenerative diseases like ALS are particularly difficult, said Dr. Lonny Shavelson, a Berkeley, Calif., physician who has supervised nearly 90 aid-in-dying deaths in that state and advised more than 600 patients since 2016.
“It’s a very complicated decision week to week,” he said. “How do you decide? When do you decide? We don’t let them make that decision alone.”
Philosophically, McQ had been a supporter of aid-in-dying for years. He was the final caregiver for his grandmother, Milly, who he said begged for death to end pain at the end of her life.
By late spring, McQ’s own struggle was worse, said Karen Robinson, McQ’s health- care proxy and friend of two decades. He was admitted to home hospice care, but continued to decline. When a nurse recommended that McQ transfer to a hospice facility to control his growing pain, he decided he’d rather die at home.
“There was part of him that was hoping there were some other alternative,” Robinson said.
McQ considered several dates — and then changed his mind, partly because of the pressure that such a choice imposed.
“I don’t want to talk about it because I don’t want to feel like, now you gotta,” he said.
Coconut water, vodka, friends
Along with the pain, the risk of losing the physical ability to administer the medication himself, a legal requirement, was growing.
“I talked with him about losing his window of opportunity,” said Gretchen DeRoche, a volunteer with the group End of Life Washington, who said she has supervised hundreds of aid-in-dying deaths.
Finally, McQ chose the day: April 10. Robinson came over early in the afternoon, as she had often done, to drink coffee and talk — but not about his impending death.
“There was a part of him that didn’t want it to be like this is the day,” she said.
Aaron McQ and his friend Karen Robinson go boating on Seattle’s Portage Bay in 2013, before he fell ill with leukemia and a rare form of ALS, or amyotrophic lateral sclerosis.
DeRoche arrived exactly at 5:30 p.m., per McQ’s instructions. At 6 p.m., McQ took anti-nausea medication. Because the lethal drugs are so bitter, there is some chance patients won’t keep them down.
Four close friends gathered, along with Robinson. They sorted through McQ’s CDs, trying to find appropriate music.
“He put on Marianne Faithfull. She’s amazing, but, it was too much,” Robinson said. “Then he put on James Taylor for, like, 15 seconds. It was ‘You’ve Got a Friend.’ I vetoed that. I said, ‘Aaron, you cannot do that if you want us to hold it together.’”
DeRoche went into a bedroom to open the 100 capsules of 100-milligram secobarbital, one at a time, a tedious process. Then she mixed the drug with coconut water and some vodka.
Just then, McQ started to cry, DeRoche said. “I think he was just kind of mourning the loss of the life he had expected to live.”
After that, he said he was ready. McQ asked everyone but DeRoche to leave the room. She told him he could still change his mind.
“I said, as I do to everyone: ‘If you take this medication, you’re going to go to sleep and you are not going to wake up,’” she recalled.
McQ drank half the drug mixture, paused and drank water. Then he swallowed the rest.
His friends returned, but remained silent.
“They just all gathered around him, each one touching him,” DeRoche said.
Very quickly, just before 7:30 p.m., it was over.
“It was just like one fluid motion,” DeRoche said. “He drank the medication, he went to sleep and he died in six minutes. I think we were all a little surprised he was gone that fast.”
The friends stayed until a funeral-home worker arrived.
“Once we got him into the vehicle, she asked, ‘What kind of music does he like?’” Robinson recalled. “It was just such a sweet, human thing for her to say. He was driving away, listening to jazz.”
McQ’s friends gathered June 30 in Seattle for a “happy memories celebration” of his life, Robinson said. She and a few others kayaked out into Lake Washington and left McQ’s ashes in the water, along with rose petals.
In the months since her friend’s death, Robinson has reflected on McQ’s decision to die. It was probably what he expected, she said, but not anything that he desired.
“It’s really tough to be alive and then not be alive because of your choice,” she said.
“If he had his wish, he would have died in his sleep.”
As the world still reels from the death of Aretha Franklin, it’s hard to believe she could have been sick for some time, had a special-needs son — along with three other children, not to mention her estate and other assets — and didn’t have a will at the time of her death.
Yet, surprisingly, she’s not the only famous person to die without a will.
And according to Forbes, a whopping 64 percent of Americans have no will. In a 2015 survey, some cited that they haven’t gotten around to it, while others said they just don’t feel it’s urgent.
What could be off-putting about creating a will? Perhaps facing the thought of your own death, the fact that it can be pricey, or that most people may not know where to start, making it an intimidating endeavor.
Still, with typically more funds than the average American, it’s hard to understand how a famous person could not have a will.
Here are 14 celebrities who died with no will:
Aretha Franklin
After battling advanced pancreatic cancer, Franklin died at the age of 76 in her Detroit home. According to her attorney, he had requested she create a trust time and again, but the Queen of Soul never got around to it. There hasn’t been a dollar figure released on the value of her assets, but her attorney said her lack of a will means it will soon become public in probate court. Her four sons have already filed a document listing themselves as interested parties, courthouse paperwork shows.
Prince
Despite being careful about his music distribution, Prince, whose fortune was estimated at $150 million to $300 million, had no will. Prince’s sister, and his only full sibling, said he had no surviving spouse, no children and no living parents, and asked for the appointment of a special administrator to his estate, the continuation of his business affairs and determination of heirs. Prince had five other living half-siblings.
Kurt Cobain
Nirvana’s frontman, whose estimated value has been in excess of $450 million, was found dead of an apparent suicide in April 1994. His wife, Courtney Love, and daughter would inherit his estate, but they met many legal battles over copyright and other issues, which were highlighted because of Cobain’s lack of planning.
Amy Winehouse
After dying from apparent alcohol poisoning at the age of 27, Winehouse’s parents wound up with her fortune of $4.66 million. Her ex-husband, Blake Fielder-Civil, did not receive anything.
Pablo Picasso
The artist had no will when he died at the age of 91 in 1973, despite having $4.5 million in cash, $1.3 million in gold, stocks and bonds, thousands of drawings, paintings and sculptures, five homes and more (his estate was valued at $250 million, or $770 million in today’s dollars). Because his relations were complicated, a fight over how his estate would be distributed went on for years and cost tens of millions of dollars. Everything was eventually divided between his widow, children and grandchildren.
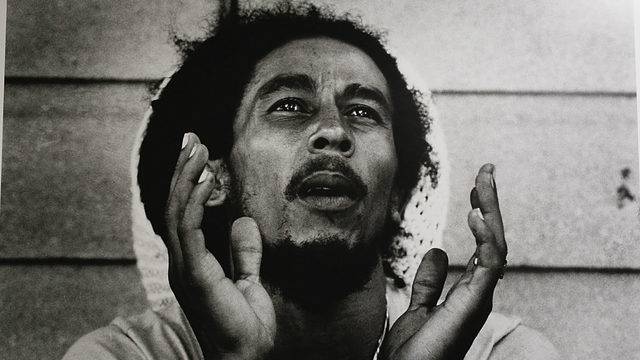
Bob Marley
When he died at the age of 36 after battling cancer, Marley had no will. Because of Jamaican law, his wife, Rita, received only 10 percent of his fortune, while the rest of his estate was divided between his 11 children. They were all additionally awarded the entitlement to his name and likeness.
Howard Hughes
The billionaire entrepreneur had no will when he died at the age of 70. His $1.5 billion fortune (valued at $6.4 billion today) was eventually split between 22 cousins.
Barry White
The soulful singer, who died at 58 from a stroke related to kidney failure, had no will, despite his health problems. His ex-wives, girlfriends and children, in turn, were left to battle over his multimillion dollar estate.
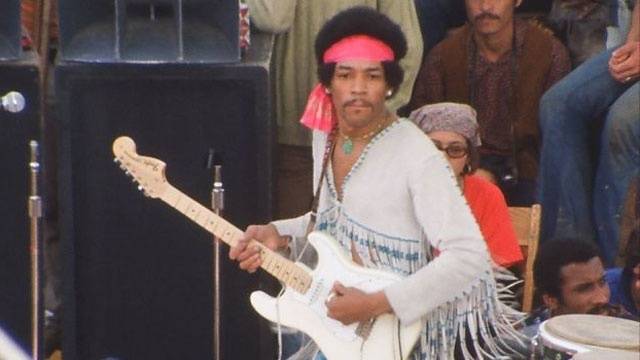
Jimi Hendrix
At only 27 years old, he was found dead of an apparent overdose in 1970. His fortune was passed to his father, but when his father died, he left Hendrix’s sister, Jane, in charge of the estate. In turn, the guitarist’s siblings fought over licensing agreements related to his image. They were set to go to trial, but a settlement was reached before they could make it there.
Tupac
At the time of the 25-year-old rapper’s slaying, he was not married and had no children. With no will, his mother inherited his estate.
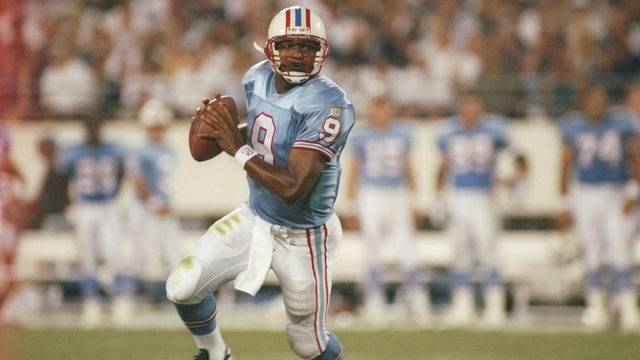
Steve McNair
The NFL quarterback was killed in a murder-suicide in 2009 and left behind a wife and four children. With no signed will at that time, much of McNair’s money has been tied up in litigation. McNair’s wife sued his mother and evicted her from a home her son had gifted her while he was still alive.
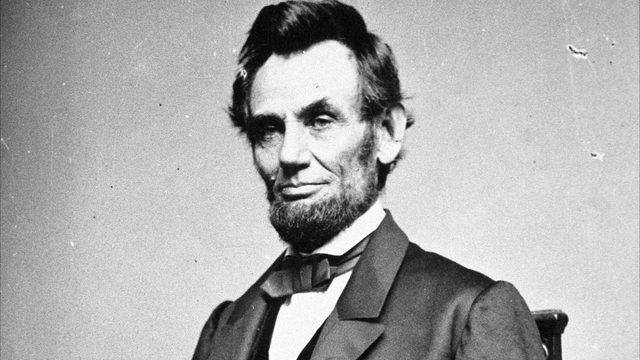
Abraham Lincoln
The 16th president of the United States, who was also a lawyer, was shot on April 14, 1865 and died the next day at the age of 56. His estate of $85,000 (which would be worth $1.2 million in today’s dollars) was eventually divided between his widow and two sons.
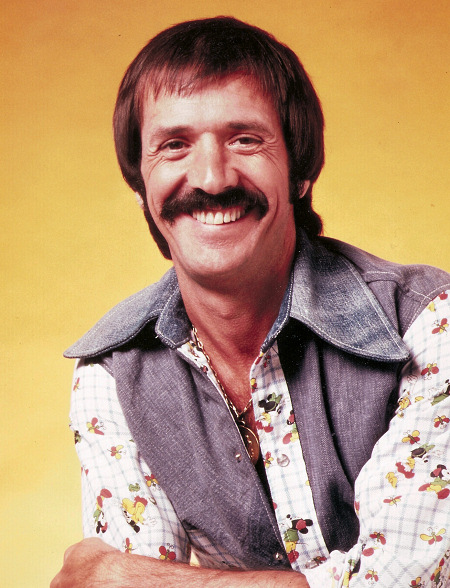
Sonny Bono
After dying in a skiing accident in 1998, the singer-turned-politician’s wife, Mary Bono, had to go through probate court in order to become the executor of his estate. Ultimately, the estate was divided between Sonny’s two children and Mary.
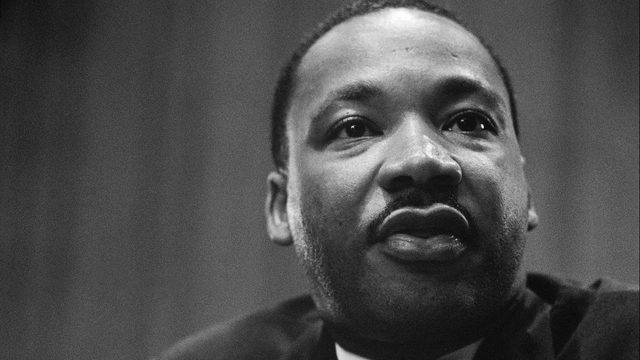
Martin Luther King Jr.
The civil rights leader was shot to death at the age of 39. Though he was only estimated to be worth $30,000 ($209,000 in today’s dollars), the heirs couldn’t agree on a best way to split his assets and were still fighting it out as of 2015.
The recent, untimely deaths of Kate Spade, reportedly from depression-related suicide, and of Anthony Bourdain, also from apparent suicide, came as a surprise to many. How could a fashion designer and businesswoman known for her whimsical creations and a chef, author and television personality who embodied a lust for life be depressed enough to end their lives? Crushing sadness can hide behind many facades.
According to a report by the US Centers for Disease Control and Prevention (CDC), suicide rates for adults in the United States are on the rise; since 1999, suicide rates in 25 states increased by more than 30%. In the US, suicide accounted for nearly 45,000 deaths in 2016.
Each person who dies by suicide leaves behind an estimated six or more “suicide survivors” — people who’ve lost someone they care about deeply and are left grieving and struggling to understand.
The grief process is always difficult. But a loss through suicide is like no other, and grieving can be especially complex and traumatic. People coping with this kind of loss often need more support than others, but may get less. Why? Survivors may be reluctant to confide that the death was self-inflicted. And when others know the circumstances of the death, they may feel uncertain about how to offer help.
What makes suicide different
The death of a loved one is never easy to experience, whether it comes without warning or after a long struggle with illness. But several circumstances set death by suicide apart and make the process of bereavement more challenging. For example:
A traumatic aftermath. Death by suicide is sudden, sometimes violent, and usually unexpected. Depending on the situation, survivors may need to deal with the police or handle press inquiries. While still in shock, they may be asked if they want to visit the death scene. Sometimes officials discourage the visit as too upsetting; other times they encourage it. “Either may be the right decision for an individual. But it can add to the trauma if people feel that they don’t have a choice,” says Jack Jordan, Ph.D., clinical psychologist in Wellesley, MA and co-author of After Suicide Loss: Coping with Your Grief.
Recurring thoughts. A suicide survivor may have recurring thoughts of the death and its circumstances, replaying over and over the loved one’s final moments or their last encounter in an effort to understand — or simply because the thoughts won’t stop coming. Some suicide survivors develop post-traumatic stress disorder (PTSD), an anxiety disorder that can become chronic if not treated. In PTSD, the trauma is involuntarily re-lived in intrusive images that can create anxiety and a tendency to avoid anything that might trigger the memory.
Stigma, shame, and isolation. There’s a powerful stigma attached to mental illness (a factor in most suicides). Many religions specifically condemn the act as a sin, so survivors may understandably be reluctant to acknowledge or disclose the circumstances of such a death. Family differences over how to publicly discuss the death can make it difficult even for survivors who want to speak openly to feel comfortable doing so. The decision to keep the suicide a secret from outsiders, children, or selected relatives can lead to isolation, confusion, and shame that may last for years or even generations. In addition, if relatives blame one another — thinking perhaps that particular actions or a failure to act may have contributed to events — that can greatly undermine a family’s ability to provide mutual support.
Mixed emotions. After a homicide, survivors can direct their anger at the perpetrator. In a suicide, the victim is the perpetrator, so there is a bewildering clash of emotions. On one hand, a person who dies by suicide may appear to be a victim of mental illness or intolerable circumstances. On the other hand, the act may seem like an assault on, or rejection of, those left behind. So the feelings of anger, rejection, and abandonment that occur after many deaths are especially intense and difficult to sort out after a suicide.
Need for reason. “What if” questions can arise after any death. What if we’d gone to a doctor sooner? What if we hadn’t let her drive to the basketball game? After a suicide, these questions may be extreme and self-punishing — unrealistically condemning the survivor for failing to predict the death or to successfully intervene. In such circumstances, survivors tend to greatly overestimate their own contributing role — and their ability to affect the outcome.
“Suicide can shatter the things you take for granted about yourself, your relationships, and your world,” says Dr. Jordan. Some survivors conduct a psychological “autopsy,” finding out as much as they can about the circumstances and factors leading to the suicide. This can help develop a narrative that makes sense.
Sometimes a person with a disabling or terminal disease chooses suicide as a way of gaining control or hastening the end. When a suicide can be understood that way, survivors may feel relieved of much of their what-if guilt. “It doesn’t mean someone didn’t love their life,” says Holly Prigerson, Ph.D., professor of psychiatry at Harvard Medical School and Director of Psycho-Oncology Research, Psychosocial Oncology and Palliative Care at Dana-Farber Cancer Institute.
Support from other survivors
Suicide survivors often find individual counseling (see “Getting professional help”) and suicide support groups to be particularly helpful. There are many general grief support groups, but those focused on suicide appear to be much more valuable.
“Some people also find it helpful to be in a group with a similar kinship relationship, so parents are talking to other parents. On the other hand, it can be helpful for parents to be in a group where they hear from people who have lost a sibling — they may learn more about what it’s like for their other children,” says Dr. Jordan.
Some support groups are facilitated by mental health professionals; others by laypersons. “If you go and feel comfortable and safe — [feel] that you can open up and won’t be judged — that’s more important than whether the group is led by a professional or a layperson,” says Dr. Prigerson. Lay leaders of support groups are often themselves suicide survivors; many are trained by the American Foundation for Suicide Prevention.
For those who don’t have access to a group or feel uncomfortable meeting in person, Internet support groups are a growing resource. In a study comparing parents who made use of the Internet and those who used in-person groups, the Web users liked the unlimited time and 24-hour availability of Internet support. Survivors who were depressed or felt stigmatized by the suicide were more likely to gain help from Internet support services.
You can join a support group at any time: soon after the death, when you feel ready to be social, or even long after the suicide if you feel you could use support, perhaps around a holiday or an anniversary of the death.
Getting professional help
Suicide survivors are more likely than other bereaved people to seek the help of a mental health professional. Look for a skilled therapist who is experienced in working with grief after suicide. The therapist can support you in many ways, including these:
helping you make sense of the death and better understand any psychiatric problems the deceased may have had
treating you, if you’re experiencing PTSD
exploring unfinished issues in your relationship with the deceased
aiding you in coping with divergent reactions among family members
offering support and understanding as you go through your unique grieving process.
A friend in need
Knowing what to say or how to help someone after a death is always difficult, but don’t let fear of saying or doing the wrong thing keep you from reaching out to a suicide survivor. Just as you might after any other death, express your concern, pitch in with practical tasks, and listen to whatever the person wants to tell you. Here are some special considerations:
Stay close. Families often feel stigmatized and cut off after a suicide. If you avoid contact because you don’t know what to say or do, family members may feel blamed and isolated. Ignore your doubts and make contact. Survivors learn to forgive awkward behaviors or clumsy statements, as long as your support and compassion are evident.
Avoid hollow reassurance. It’s not comforting to hear well-meant assurances that “things will get better” or “at least he’s no longer suffering.” Instead, the bereaved may feel that you don’t want to acknowledge or hear them express their pain and grief.
Don’t ask for an explanation. Survivors often feel as though they’re being grilled: Was there a note? Did you suspect anything? The survivor may be searching for answers, but your role for the foreseeable future is simply to be supportive and listen to what they have to say about the person, the death, and their feelings.
Remember his or her life. Suicide isn’t the most important thing about the person who died. Share memories and stories; use the person’s name (“Remember when Brian taught my daughter how to ride a two-wheeler?”). If suicide has come at the end of a long struggle with mental or physical illness, be aware that the family may want to recognize the ongoing illness as the true cause of death.
Acknowledge uncertainty. Survivors are not all alike. Even if you are a suicide survivor yourself, don’t assume that another person’s feelings and needs will be the same as yours. It’s fine to say you can’t imagine what this is like or how to help. Follow the survivor’s lead when broaching sensitive topics: “Would you like to talk about what happened?” (Ask only if you’re willing to listen to the details.) Even a survivor who doesn’t want to talk will appreciate that you asked.
Help with the practical things. Offer to run errands, provide rides to appointments, or watch over children. Ask if you can help with chores such as watering the garden, walking the dog, or putting away groceries. The survivor may want you to sit quietly, or perhaps pray, with him or her. Ask directly, “What can I do to help?”
Be there for the long haul. Dr. Jordan calls our culture’s standard approach to grief the “flu model”: grief is unpleasant but is relatively short-lived. After a stay at home, the bereaved person will jump back into life. Unfortunately, that means that once survivors are back at work and able to smile or socialize again, they quickly get the message that they shouldn’t talk about their continuing grief. Even if a survivor isn’t bringing up the subject, you can ask how she or he is coping with the death and be ready to listen (or respect a wish not to talk about it). Be patient and willing to hear the same stories or concerns repeatedly. Acknowledging emotional days such as a birthday or anniversary of the death — by calling or sending a card, for example — demonstrates your support and ongoing appreciation of the loss.