[A]t the end, Hugh Wallace still remembered there were 43,560 square feet in an acre.
Surrounded by family on April 19, just before a lethal cocktail was administered to legally end his life, making him the first Albertan to do so in this province, his son asked him the question he feared he may one day not be able to answer.
“Hugh always said if he got to the point where he couldn’t remember how many square feet were in an acre, he didn’t want to go on,” said his widow, Evie.
“At the end, he scored the winning goal in the last second of play.”
Alberta Health Services this week revealed 31 Albertans have so far been granted physician-assisted deaths, two dozen of those coming after the federal government lifted the legal prohibition against the practise in June, following a 2015 Supreme Court ruling.
Wallace, who at 75 had endured a quarter-century of multiple sclerosis before contracting aggressive lung cancer, was an engineer, and at his heart an uncompromising pragmatist, said Evie, who has since become an advocate for assisted death, speaking around the province.
“He wanted to go out with his brain intact,” Evie said.
“He didn’t want to go out in a coma, with a catheter and wearing Depends. That wasn’t him.”
Wallace, like a handful of trailblazers before him, had gone before the courts earlier this year seeking an exemption against the law outlawing assisted death in the Canadian Criminal Code.
In February, Hanne Schafer became the first Alberta woman granted the legal right to take her own life, but, after struggling to find a doctor in her own province, had to go to B.C. for the procedure. A second Alberta woman also went to B.C. to have a doctor assist in her death after a ruling in May.
But Wallace was able to find an Alberta doctor willing to help him die on his own terms, opening the door to others seeking the same release. As of Tuesday, the lead for medical assistance in dying preparedness for AHS, Dr. James Silvius, said two to four patients a week are taking advantage of the service, numbers he admits are somewhat surprising.
Evie said though her husband was suffering in the waning days of his life, he found some comfort in being able to have some control of how he passed on.
“It was an incredibly positive experience,” she said. “He was able to say his goodbyes to everybody and the doctors were fantastic. They were amazing human beings.”
Evie added the doctors involved in his care had meetings with both family and Wallace privately to ensure there were no signs of coercion before he underwent the procedure.
While her family’s experience was positive, the 73-year-old widow noted those who choose assisted death need to make sure everybody’s on the same page, and there are no lingering issues to resolve.
“It’s something for people to really look at their family dynamics before they go through with this,” Evie said.
“If there’s a lot of unfinished business in a family, it’s fertile ground for explosions.”
After 51 years of marriage, Evie said she is left with wonderful memories of the man she deeply loved, and not a shadow of regret about watching Hugh end his own life.
“At the end, we didn’t have any tears left in us. It was a good day.”
Death was a topic that wasn’t discussed in Adrienne Lawson Thompson’s home growing up. The Los Angeles native says it was such a taboo topic, that her own mother didn’t even reveal what illness she was stricken with before she died.
“She didn’t want to disclose things to me because ‘Oh, you’re young. I don’t want to be a burden to you. You have your children, recently married.’ And we don’t look at it that way, as being a burden,” Thompson says.
She believes not talking about death is pretty prevalent in the African American community. And when faced with death, many African Americans lean on their faith.
“Trust in your faith that if God will heal you, he will heal you,” Thompson says.
And it’s that trust that may lead many African Americans not to participate in California’s End of Life Option Act.
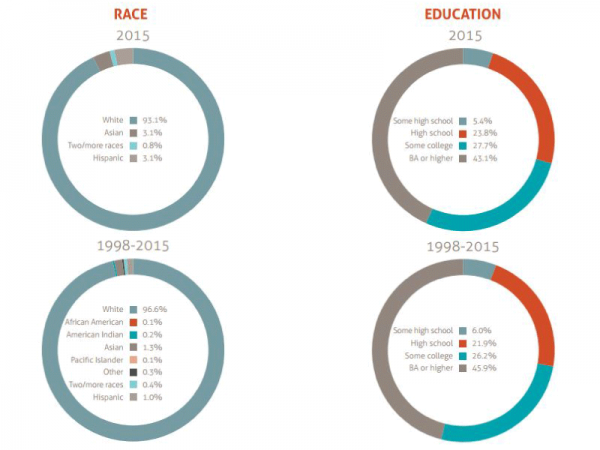
“Very few have used the law that are Hispanic, Asian or Black,” says George Eighmey, president of Death with Dignity in Oregon. He says requests are generally made by people who are white and highly educated.
Demographics of Oregon’s Death with Dignity Act Recipients.
In Oregon, between 1998 and 2015, 97.1 percent of participants were white, according to the Oregon Health Authority.
Last year in Washington, 98 percent of participants were also white, according to the Washington Department of Public Health.
But while Oregon and Washington have largely white populations, California’s demographics are much different. Latinos are 39 percent of the population and Asians and African Americans make up 15 percent and 6 percent of the state’s population, respectively.
“Our demographics are really, very different and we don’t know yet who is going to be asking about this option with the intent of participating,” says Lael Duncan, medical director of consulting services at the Coalition for Compassionate Care of California.
Britta Guerrero, executive director of Sacramento Native American Health Center, says when members of her community face terminal illness, trust in their culture and their own healers is also important.
“We would seek maybe to see a medicine person and try to receive doctoring from a cultural perspective, a spiritual perspective,” Guerrero says.
In addition to these cultural and spiritual differences, there’s also the country’s history of using people of color for medical experiments.
“I think we have a long-term distrust for the medical and health care system,” Guerrero says.
CynthiaPerrilliat, executive director of Alameda County Care Alliance, says trust in the health care system is also a major issue in the African American community due to medical experiments like the Tuskegee Study of Untreated Syphilis in the Negro Male.
“Black men that had syphilis not being treated, the role that the government, quote, unquote, had to play in that, the role of the health system in that,” Perrilliat says.
It’s too early to tell whether this dark history will affect minority participation in the End of Life Option here in California.
The Department of Public Health will release a report on participation in the law, including a racial and ethnic breakdown, next summer.
[D]uring the bleakest, most vulnerable period of their lives, terminally ill patients should be able to count on top-notch care and generous doses of compassion. But in one key area, Canada’s Catholic hospitals are letting them down.
At St. Paul’s Hospital in Vancouver, a dying 84-year-old patient who had requested a medically assisted death was required to go to another hospital, and his last day was pure agony as an ambulance shuffled him between institutions. St. Paul’s would not even permit him to be assessed for assisted death on its premises.
Catholic health providers across the country have said that while medically assisted dying is now legal, their faith does not allow them to participate. “These organizations neither prolong dying nor hasten death, and that’s a pretty fundamental value for them,” says the president of the Catholic Health Alliance of Canada.
We have argued before that individual choice must be the over-arching principle behind assisted dying decisions. While, in accordance with strict legal rules, a patient should be able to request assisted death, individual medical practitioners should not be forced to provide it against their own ethics.
But individual rights don’t apply to publicly funded institutions. If no individual health care expert in a Catholic hospital will personally support a medically hastened death, the publicly funded institution itself must still find a qualified practitioner who will. Forcing those in pain and mental distress to leave the site in order to obtain even an end-of-life assessment is simply inhumane.
In Ottawa, the situation is particularly complicated for Bruyère Continuing Care, a Catholic facility. Although organizations that support Catholic health care don’t want even a conversation about assisted dying to take place there, the Bruyère is the only publicly funded, complex palliative-care option in this region. To its credit, it appears to recognize that it must be more flexible.
A Bruyère administrator told the Citizen that if a patient requested information, the facility would be bound to acquiesce. If the patient were too ill to be assessed off-site – which is likely in palliative cases – the assessment, at least, could be done without moving the patient. Still, the person would have to transfer elsewhere to actually obtain a medically hastened death.
Provincial governments must step in – yet in Ontario, at least, regulations aren’t expected until 2017. Why should a publicly funded institution be permitted to refuse a service to the dying that is legal and that could be performed on its premises with considerably less agony than exiling the patient?
Force individual medical practitioners to end a life? No. Tell institutions to follow the law? Yes. A dignified ending shouldn’t be hostage to institutional beliefs.
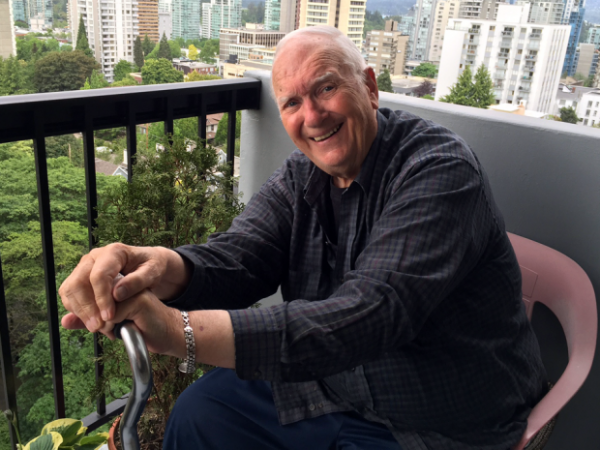
Ian Shearer’s daughter, Jan, says she was surprised by his request for doctor-assisted death, but she realized that he was dying “a slow, painful” death.
Ian Shearer had had enough of the pain and wanted a quick, peaceful end, his life marred by multiple afflictions.
But the Vancouver man’s family says his last day alive became an excruciating ordeal after the Catholic-run hospital caring for him rebuffed his request for a doctor-assisted death, forcing him to transfer to another hospital.
The combination of the cross-town trip and inadequate pain control left Shearer, 87, in agony through most of his final hours, says daughter Jan Lackie.
“To hear him crying out, screaming … was just horrible,” said Lackie, breaking into tears as she recalled the day in late August. “That’s what keeps me from sleeping at night … I don’t want any other person to go through what he did.”
Shearer’s experience at St. Paul’s Hospital highlights one of the thorniest issues concerning assisted death: the decision of most faith-based — but taxpayer-funded — health-care facilities to play no part in a practice made legal by the Supreme Court of Canada and federal legislation.
Ian Shearer and daughter Jan Lackie.
Lackie said the suffering her father endured shows why it is important that church-governed facilities, including dozens of hospitals, nursing homes and hospices across Canada, be required to allow assisted deaths within their walls.
“We have nine judges who said ‘Yes’ to medical assistance in dying,” she said. “I don’t understand how the Vatican has so much power, even here in Canada.”
But the bill that implemented the Supreme Court’s ruling in June does not oblige any institution to permit the practice.
And Catholic health organizations say their objection to assisted death flows from deeply held beliefs, while noting there are numerous other, less contentious procedures available at some facilities but not others.
“Life is sacred and the dignity of the person is important,” said Michael Shea, president of the Catholic Health Alliance of Canada. “These organizations neither prolong dying nor hasten death, and that’s a pretty fundamental value for them.”
Shaf Hussain, a spokesman for Providence Health Care, which operates St. Paul’s, said he could not comment on Shearer’s case specifically. But under a policy finalized this summer, he said, the Catholic organization arranges to transfer patients as comfortably as possible when they express a desire for assisted death.
Even the medical assessment required under the law and the signing of consent forms must take place outside Providence properties.
“All feedback we take very seriously,” said Hussain. “We’ll be working with our partners in the health care system to ensure the patients’ needs do come first … and to minimize the discomfort and pain.”
Shearer, a retired accountant originally from Calgary, suffered from spinal stenosis – a narrowing of the spine that can put pressure on the spinal cord – heart disease, kidney failure and, toward the end, sepsis, said his daughter.
He spent about three weeks at St. Paul’s, the closest hospital to where he lived in Vancouver, said the Calgary woman. The spinal condition was so debilitating, “just to touch him, he would scream.”
Lackie said she was surprised by his request, but supportive, realizing that her father was dying “a slow, painful” death.
It would be days, however, before Shearer was transferred to Vancouver General, and on the designated date – Aug. 29 – the ambulance arrived more than three hours late, said the daughter.
The man’s dose of the pain drug fentanyl had been reduced to ensure he was lucid enough to consent to the assisted death, but as time wore on the pain grew worse, and there was a shortage of the narcotic on his ward, she said.
Already in agony, Shearer cried out desperately with each bump during the four-kilometre ambulance ride, said Lackie.
He eventually received the series of injections ending his life at Vancouver General, a “beautiful,” peaceful death, she said.
Jan Lackie holds father Ian Shearer’s hand on his last day, when a Catholic hospital’s refusal to consider his request for assisted death forced a painful transfer to another hospital.
Dr. Ellen Wiebe, a B.C. physician who has carried out several assisted deaths, provided the service for Shearer, one of three patients from St. Paul’s she has seen for the same reason.
To get around the hospital’s ban on patients even being assessed there, she said she makes “flower visits:” masquerading as a friend bringing a bouquet.
Assisted-death bans can not only lead to suffering during the transfer itself, but effectively deny patients the right in areas where there is no alternative to the faith-based institution, said Shanaaz Gokool, head of the group Dying with Dignity.
“This is going to be a real issue, and it’s going to be a real issue across the country.”
The facilities are causing vulnerable patients suffering because of a decision that benefits only the institution, argued Juliet Guichon, a bioethicist at the University of Calgary.
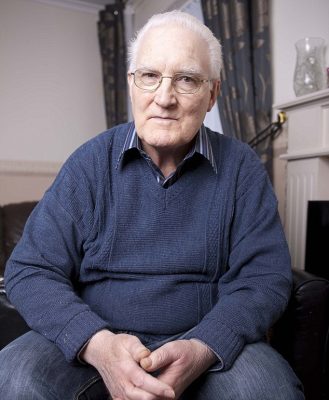
[A]fter almost 20 years of living with a pacemaker, Nina Adamowicz decided she no longer wanted the device that was keeping her alive.
It had been implanted in 1996, and for the first decade it ‘improved’ her life and symptoms — she had a form of hereditary heart disease.
The pacemaker sent regular electrical pulses to keep her heart beating steadily, and she was grateful for ‘being given extra time’, she later recalled.
However, she then had a heart attack and her health declined so that by 2014, her heart was working at just 10 per cent of its capacity.
Last year, Polish-born Ms Adamowicz, 71, who had lived in the UK for more than 30 years, revealed she wanted the pacemaker turned off, even though she knew it would lead to her death.
After almost 20 years of living with a pacemaker, Nina Adamowicz decided she no longer wanted the device that was keeping her alive
It was like being ‘in line for execution and being told “not yet”, she said in an interview for BBC Radio 4.
‘It’s not about “I want to die”, I’m dying,’ she added.
After a series of medical examinations and psychological tests to determine whether she understood what switching off her pacemaker would mean, doctors agreed, and last October Ms Adamowicz went into a local hospice with her family for the pacemaker to be turned off – a procedure that took 20 minutes.
She described her body as feeling heavy and she felt a little nauseated – but she also felt at peace, her family told the BBC.
She slept through the night, returned home in the morning and died that night.
Her case – thought to be the first of its kind in the UK – raises profound ethical issues about when it is right to turn off someone’s pacemaker, or indeed withdraw other medical treatment such as dialysis for kidney failure, if that’s what they want.
In fact the law itself is very clear on this point, according to Miriam Johnson, professor of palliative medicine at Hull York Medical School.
‘A mentally competent adult has the right to refuse medical treatment, whether it is turning off a pacemaker or stopping dialysis, even if that treatment is prolonging their life and withdrawing it will lead to their death,’ she says.
‘By turning off the device, the disease or illness will kill the person, not the doctor.’
However, some doctors feel it’s uncomfortably close to euthanasia — the difference is that euthanasia involves overriding Nature.
Some doctors feel that turning off a pacemaker is uncomfortably close to euthanasia — the difference is that euthanasia involves overriding Nature
‘The difficulty with a case like this is that when a patient is dependent on a pacemaker, there is a direct connection between withdrawing the treatment and them dying within the next few hours,’ adds Professor Johnson, explaining that doctors’ role after all is to protect the vulnerable.
Around 35,000 patients in the UK have a pacemaker fitted each year. The device’s role is to keep the heart beating steadily – it gives it a boost by delivering electrical impulses so that the heart contracts and produces a heartbeat.
The computerised match-box sized device is implanted just under the skin, usually just below the left shoulder and electrical leads are then fed down a vein into the heart.
‘In a significant number of pacemaker cases if you suddenly took the pacemaker away, the heart would stop beating,’ explains Dr Adam Fitzpatrick, a consultant cardiologist and electrophysiologist at Manchester Royal Infirmary and Alexandra Hospital, Cheadle.
He adds: ‘It is very unusual for a patient to ask for their pacemaker to be turned off.’
Even if the patient is dying, a pacemaker does not need to be switched off, says the British Heart Foundation.
‘A pacemaker’s purpose is not to restart the heart and it won’t cause discomfort to someone who’s dying,’ said a spokesperson for the British Heart Foundation
‘Its purpose is not to restart the heart and it won’t cause discomfort to someone who’s dying,’ said a spokesperson.
But the picture is slightly different with other heart devices such as Implantable cardioverter defibrillators (ICDs) which are used to correct an abnormal heart rhythm rather than helping the heart beat steadily.
These devices, implanted in around 9,000 people in the UK every year, kick in when an abnormal heart rhythm occurs which can cause sudden cardiac arrest (where the heart stops beating).
Implanted under the collarbone as a pacemaker is, they work by firing a small electric shock into the heart to kick-start it (some pacemakers have this function too).
This might happen once every few months or not even for years.
However, this can be both painful and traumatic, especially at the end of life, and can lead to a prolonged and distressing death by continuing to give electric shocks.
In one particularly upsetting case reported in a US medical journal, a man suffered 33 shocks as he lay dying in his wife’s arms — the ICD ‘got so hot that it burned through his skin’, his wife later reported.
Implantable cardioverter defibrillators work a bit differently from a pacemaker, as they are used to correct abnormal heart rhythm with an electrical current
‘Dying patients often have multi-organ failure which can cause metabolic and chemical changes that may trigger arrhythmias, faulty heart beats and in turn activate the ICD,’ explains Dr James Beattie, a consultant cardiologist at the Heart of England NHS Foundation Trust, Birmingham.
‘If the device goes off when the patient is conscious, the shock is like a blow to the chest, causing discomfort and distress. It may also fire repeatedly.
‘This may result in a distressing death for the patient and distress for the families.’
Yet despite this suffering, 60 per cent of hospice patients do not have their implant deactivated before death, according to U.S. research published in the Annals of Internal Medicine.
Furthermore, a 2011 survey by the National Council for Palliative Care suggested that only 40 per cent of UK hospices have access to the technology to deactivate the device urgently, potentially risking an undignified and painful death in hundreds of patients should they suddenly deteriorate.
Switching off the device involves holding a magnet over it, temporarily closing a magnetic switch incorporated in it.
To turn it off permanently the device has to then be reprogrammed remotely using a ‘wand’ attached to a computer.
Despite the risk of suffering, 60 per cent of hospice patients do not have their implant deactivated before death, according to U.S. research
Medical professionals and families face a number of dilemmas when deciding whether to turn off an ICD.
One is the difficulty in accurately predicting when the patient is reaching the end of their life.
‘Determining this isn’t always clear, especially with a condition such as heart failure when patients may have survived crises over many years,’ explains Professor Johnson.
‘This can be complicated further if the patient is suffering from dementia and unable to make decisions about their care.’
There is also an understandable reluctance by patients and their families to take away anything that can prolong life.
‘Patients and their families frequently think of the device as entirely beneficial,’ says Professor Johnson.
‘There is also often unrealistic expectation about what doctors are able to do to keep people alive.’
Many doctors shy away from these conversations, too. A 2008 report from the National Audit Office found a significant lack of confidence in handling end-of-life care across all medical specialities — with cardiologists topping the league.
‘Given they are trained to save lives, talking about death can be seen as professional defeat,’ says Dr Beattie.
But if patients and doctors don’t have that conversation ‘we’re storing up trouble because decisions then have to be made at times of crisis and without planning’, says Simon Chapman, of the National Council for Palliative Care.
New guidance for patients and medical staff to guide them through the ethical minefield of withdrawing heart devices was published earlier this year in the journal Heart.
Just how difficult making such decision can be was dramatically highlighted in the case of Fred Emery.
When his health suddenly went downhill six years ago, doctors recommended turning off the defibrillator that had been keeping him alive for the past 14 months.
When Fred Emery’s health suddenly went downhill six years ago, doctors recommended turning off the defibrillator that had been keeping him alive for the past 14 months
The 73-year-old former manual worker from Kings Langley, Hertfordshire, had had the matchbox-sized device implanted in his chest following a 26-year battle with heart disease.
During that time he’d had two heart attacks, and had already undergone two triple heart bypass operations as well as having several stents (tiny metal tubes) inserted to prevent his arteries blocking.
However, Fred then developed heart failure and ventricular tachycardia — a potentially fatal heart rhythm
Having a defibrillator not only helped with the heart failure, but also any sudden cardiac arrest triggered by the faulty heart rhythm.
But Fred’s condition deteriorated and doctors suggested that as he was nearing the end of his life, it was time to turn off this life-line — to spare him and his family the ordeal of it repeatedly jolting his heart back to life when his body had reached the natural moment of death.
However, despite doctors’ predictions, Fred pulled through and later had the defibrillator reactivated, and it went on to save his life several times before his death this year. His family was angry that doctors had written him off before his time.
Despite doctors’ predictions, Fred pulled through and later had the defibrillator reactivated, and it went on to save his life several times before his death this year
‘It was awful when they told him to turn it off,’ his wife Shirley, 70, told Good Health. ‘Fred was taken ill at 4pm, and by the next morning the defibrillator was turned off. It was too soon to make that decision — he wasn’t himself and was under pressure to switch it off.
‘After it was reactivated, Fred had six more years. Without the ICD we would have lost him several years ago.
‘He kept it on until a week before his death. By then his heart was working at 15 per cent, he was in a hospice and there was no coming back so we made a decision to turn it off to give him some dignity at the end. He knew what was happening.
“People told me stories about my dad, some made me cry and some made me laugh, I would be heartbroken if I thought that my laughing would indicate that I didn’t care.”
[G]rief is complex.
No one can explain grief to you and no one can tell you how to deal with it. You can speak to counselors, and read approved leaflets on dealing with losing someone and even they cannot tell you how the grief process will work.
So a newspaper certainly has no right to do so.
A well-known newspaper publication recently wrote an article about a young girl who went on a night out. If you’re looking for the news there’s a reason you can’t find it.
The young woman’s mother had died by suicide in a story that was covered in depth by the media, aside from that, this young girl is no different to anyone else who loses a parent.
The story detailed what she wore on the night out and tried to highlight that it was ‘just weeks’ after her mother’s death.
The tone of the story seemed to want to illustrate that there is an issue with the fact that she went out with her friends.
This was two months after her mother died.
A young girl went out with her friends two months after her mother passed away and a newspaper highlighted it as a news story.
This brings to light a very real problem in the media and even in the public when it comes to grief.
This is an example of grief shaming. That is, judging someone for the way they deal with losing someone close to them. Judging them for being too happy, or for attending events, or maintaining somewhat of a normal life on the outside.
No one can tell someone how to grieve. Even those who have suffered from grief can’t judge another person for not doing it in the same way.
Just because someone is seen to be enjoying themselves after a death doesn’t mean they are not sad, and even if they are not sad now, that does not mean that they won’t be at another time.
For many people, laughing, smiling and having fun is a coping mechanism. We are told ‘they would want you to be happy’ and ‘they would want you to enjoy yourself’ but are we judged by others for doing that?
During my dad’s wake, family and friends approached me to tell me stories about what a brilliant man he was, some made me cry and some made me laugh, I would be heartbroken if I thought that my laughing would indicate that I didn’t care.
I remember attending a birthday party about six weeks after he died. For me the more time that passed the harder it got, so a party seemed like something I could do to try and feel normal and to forget about it.
I enjoyed myself, I spoke to people I hadn’t seen in ages, and then, someone came up to me and said ‘sorry about your dad, Megan’. There and then I felt guilty for being there. It wasn’t her fault, she was being kind, but I brought it upon myself to feel guilty, which was obviously completely wrong.
However, if I went on the internet the next day and saw the article previously mentioned, I would have felt a million times worse.
I was thirteen, unlike the woman in the story above, I wasn’t old enough to hit the drink or head to a club, but I’m almost certain if it happened now I’d drink a few whiskeys, I don’t see that would mean that I did not miss my dad.
The newspaper headline purposely phrases ‘two months’ as ‘just weeks’ to make it somehow seem worse and more recent. Two months can fly by after death or it can drag on. But that’s not the point.
Even if it was two days, she had every right to do what she wanted to do.
Grief hit me, when my dad died, but only briefly, only the day of the burial, then it all turned into a weird dream and it wouldn’t hit me again for a few weeks. It comes in and out but never fades away completely. Even now, eight years later I have days that are harder than they were those two months after he died.
Should I still be sitting at home?
If we waited for grief to go away before we left the house, we would never step outside the door again.
The loss reminds us of love. That we loved, and that we were loved.
By Nivida Chandra
[G]rief is that which makes you feel like a giant void has been created inside of you. In its most awful form, it’s that feeling of having your most vital organs ripped out, and being commanded to live nonetheless.
Various “manuals” of grief will tell you more about how to feel when you’re grieving, including the famous five steps that you’ll go through, and also how long grief should last.
I lost my grandmother in June and some people have wondered openly how it’s still affecting me, three months later. I’m not offended, but it did surprise me enough to think about it. And so I began thinking about the expiration of grief.
The answer lies in understanding the difference between the end of our grief within, and end of grief as it appears to those around us. When thinking about presenting grief to others, I think of tears and rage. This is limited to the immediate aftermath of the loss.
As time passes, irrespective of whether we heal internally or not, the expectation is that the tears and rage transform into smiles and acceptance, supported by cliches on how life moves on. It’s almost as if, with time, we console others about how “fine” we are in the face of loss, and that they need not dig deep to find that right thing to say which will make us feel better.
I think this is because we all implicitly understand how uncomfortable people can feel in the face of someone else’s loss. This is not a good or bad thing, it just is.
While this discomfort is human and true, what is equally true is that it is compounded by a cultural dictation of quotas. People have quotas of how much of our grief they can and want to and should take. The “can” and “want” are prescribed by our personal relations and unique personalities
As time passes, irrespective of whether we heal internally or not, the expectation is that the tears and rage transform into smiles and acceptance.
But the “should” is culturally granted by an unsaid hierarchy of losses. We learn in society what is a big loss, a small loss, and how to respond to different losses.
For instance, parental death warrants more grief, and therefore more support, than grandparental death. And nothing is worse than your child’s death. Similarly, loss of marriage allows for more grief and subsequent condolences than, say, losing a job.
People keep these in mind when deciding how to console and for how long. Beyond that, they wonder, they question sanity, therapists are sought and so on. And I get that. I do. As people we like to be happy, and if something or someone is not being able to achieve that or is dampening our own, we try to correct that.
I get it. But personal grief doesn’t follow these cultural norms. It just goes on and on, till time repairs it or memory obscures it. It’s indefinite. For those viewing someone else’s grief, it passes and people heal, but from the inside, it just changes from open declaration to silent acceptance. It doesn’t end, it just morphs into something more comfortable for others to witness.
How can grief end? When we’re grieving an irreparable loss, we’re faced with finality. Ironic as this may sound, finality doesn’t end. Loss is always final, endless.
I realised today that this endlessness, this feeling of never again, makes me entirely helpless. I’m powerless. This feeling flows from me to the one who’s trying to console me, creating in them the same powerlessness.
Just as we’re powerless against our loss, they’re powerless against our grief. The consolers resort to jokes, to helpful cliches (this too shall pass) and they’re not wrong, neither are they cruel. They’re just insufficient and they will remain so.
So I keep it within (and then find myself writing about it, so not doing a very good job of keeping it within). I grieve in my dreams. I grieve in my memories. But it’s not always so dramatic. I grieve while driving too. Or while writing.
It just manifests in all these private spaces, that’s all. I think a part of us doesn’t want the grief to go away. Because that might delegtimise, within our own heart, how very important that loss was.
The loss reminds us of love. That we loved, and that we were loved.
So I know that when you’re grieving, like me, you too would like to know when the persistent vacuuming of your insides will end. But we’re grieving finality, and we’re grieving the loss of love.
And I think that it doesn’t really end. We’ll always grieve, but maybe we’ll grieve a little less each day, till the grief itself becomes a painless memory, which we can hold on to forever.