Heart disease and cancer still top the list as the leading causes of death in the United States, but the gap is closing between the two. A new report out from the Centers for Disease Control and Prevention looks at the shifting trends in Americans’ health and mortality, and the conditions most likely to take lives.
In 2014, a total of 2,626,418 deaths were reported in the United States, and the age-adjusted death rate decreased 1 percent to a record low.
Bob Anderson, chief of the CDC’s Mortality Statistics Branch, told CBS News the 15 leading causes of death in 2014 remained the same as in 2013.
“We all have to die of something at some point. When you’re looking at these categories you have to account for the fact that there are competing risks, but you can’t avoid death,” said Anderson.
Why the list, then?
“We want to create a society where we live as long as we can, as healthy as we can,” he said. Crunching the data provides researchers with information that will help develop prevention programs, he explained.
Anderson, who oversaw the production of the National Center for Health Statistics report, shared some insights into the top ten:
1. Heart disease
While heart disease has topped the list for years now, the actual number of deaths and the death rate for heart disease has come down by quite a bit over recent decades, said Anderson.
“The decline goes back about 50 years. For trends in heart disease, you see a substantial increase from the beginning of 20th century to 1950 or so, and then it starts to come down. It mirrors the rise and decline in smoking in the United States
“What we’ve seen in last 20 or 30 years is rapid decline in heart disease. The decline has been fairly rapid and rapid enough so it’s sort of overshadowed the aging of the population,” said Anderson.
However, a new study published this week in JAMA Cardiology, by Kaiser Permanente researchers, shows that the decline in deaths from heart disease and stroke has slowed, nearly leveling out since 2011.
2. Cancer
Cancer has seen a gradual rise in deaths over time although death rates have declined gradually since 1990. While smoking cessation’s perks were pretty quickly reflected in a drop in heart disease-related deaths, the increasing number of cancer deaths reflect the longer term damage smoking can do, as well as a growing aging population.
“Cancer tends to occur a little bit later, it’s a more chronic issue. It kills you later than heart disease does on average,” said Anderson. “You see this increase in cancer mortality — a lot of it is lung cancer.”
He noted that the gap between heart disease and cancer deaths has narrowed substantially over time.
3. Chronic lower respiratory diseases
Chronic obstructive pulmonary disease (COPD), largely due to smoking, makes up the majority of deaths in this category. It also includes deaths from chronic bronchitis, emphysema and asthma. Again, smoking earlier in life or throughout life plays a large part in respiratory disease deaths, including secondhand smoke-related illnesses.
4. Accidents
Motor vehicle accidents, unintentional drug overdoses, and accidental falls and other injuries make up this category.
“The largest proportions of these are motor vehicle accidents and drug overdoses,” said Anderson, noting that this category does not include intentional overdoses that lead to suicide. The number of accidental drug-related deaths has been on the rise amid a growing epidemic of heroin and opioid painkiller addiction.
Deaths from motor vehicle accidents declined when seat belts and car seats for kids were mandated. “They have made a huge difference,” he added.
5. Stroke
Cerebrovascular disease, or stroke, is not considered heart disease — it involves blood vessels.
“Stroke is centered on the brain, heart disease is centered on heart. Both infarction, a blockage in blood vessels leading to the brain, and hemorrhage due to things like brain aneurisms, are included,” said Anderson.
This is another category that has dropped substantially, he added.
“For a long time cerebrovascular disease was the third leading cause of death and now it’s at five. Smoking and healthy behaviors and our ability to treat these diseases have had an impact. We’ve gotten very good at treating cardiovascular disease generally and that’s had an impact on both heart disease and stroke deaths. It’s a combination of both prevention and treatment,” Anderson said.
“A lot of the increase we’ve seen has to do with better diagnosis. Folks who work on this have come up with better diagnostic criteria. Some of these [deaths] may have in previous years been reported as dementia, which goes to a separate category,” said Anderson.
But not all of the increase has to do with better diagnosis and reporting, he noted.Alzheimer’s risk tends to increase with age, so as there have been substantial declines in heart disease and stroke, more people are living to older ages and developing Alzheimer’s.
7. Diabetes
Diabetes has bobbled up and down on the top ten list over the years.
“It hasn’t changed a whole lot over last 10 years or so. There are different risk factors. Some are inherited, like in type 1 diabetes. Much of type 2 is associated with obesity. Diabetes is also connected with other diseases, such as cardiovascular disease,” said Anderson.
He said diabetes-related deaths are likely under reported — physicians may not make it the primary cause of death on a death certificate, but “if you look at any mention of diabetes on death certificates, cases where it’s a contributing factor, the numbers are much much larger.”
There are about 76,000 deaths caused by diabetes each year, but it is listed as a contributing factor in death on close to 245,000 death certificates annually, Anderson said.
8. Influenza and pneumonia
“You have to be careful here,” Anderson said. “These are not all flu-related deaths. We combine influenza and pneumonia because we use this combination category for flu mortality surveillance. Perhaps as much as 20 percent of deaths in this category are actually associated with the flu. A lot of these deaths are elderly folks who, say, have a stroke and are in the hospital and may develop pneumonia from being in a static position.”
He said that the deaths that specifically mention flu tally only about 3,000 to 5,000 deaths a year. The deaths in this category associated with flu tend to fluctuate by flu season, but the numbers due solely to pneumonia stay pretty stable over time.
“The fluctuations in this category help us determine the effects of flu season on mortality. So that’s why these two are combined,” he explained.
9. Kidney disease
This category includes chronic kidney issues, including kidney failure or end-stage renal disease.
“A large proportion of this category is renal failure. Some are probably related to diabetes in some way, or heart disease and heart failure, and high blood pressure. It’s always been on the second half of the list, at least in recent memory,” Anderson said.
10. Suicide
Suicide is the nation’s 10th leading cause of death, and the number of cases has been on the rise. “The rate of suicide has gone up nearly steadily since 1999,” Sally Curtin, a statistician with the National Center for Health Statistics at the CDC, said when the latest figures were released this spring.
“It has typically been there between number 10 and 15, but occasionally it has popped up into the top ten and it’s something we’re keeping our eye on,” said Anderson.
Other causes
Blood poisoning, chronic liver disease and Parkinson’s disease didn’t make the top 10 list, but aren’t far behind.
“Parkinson’s is a fairly important category. It’s one of those that’s gone up — the numbers have increased over time,” Anderson said. It wasn’t on the list in the year 2000, for example.
A study out earlier this year also suggested medical errors can be blamed for a significant number of deaths each year, although they were not included on this list. Anderson said many physicians likely do not report medical errors on death certificates.
Another significant cause of death, HIV/AIDS, has been declining since its peak in 1995, but the disease still takes a high toll among men in certain age groups. For men ages 25-34, HIV/AIDS was the 8th leading cause of death in 2014.
Life expectancy
The report also found that life expectancy at birth is 78.8 years, unchanged since 2012. Life expectancy rose for black males, Hispanic males and females, and non-Hispanic black males. Life expectancy shrunk for non-Hispanic white femalesfrom 2013 to 2014, possibly due to a rise in opioid use and suicide.
Preliminary data for 2015 suggest the death rate is going up. The Centers for Disease Control and Prevention posted the numbers earlier this month. They are based on a preliminary look at 2015 death certificates. The overall death rate rose to nearly 730 deaths per 100,000 people last year, from about 723 the year before.
“I think, ideally, what we would like to see is people living well into their nineties and even early 100s in relatively good health, and dying as things just kind of wear out. That’s what I’d like to see,” Anderson said. “That’s one of the reasons for creating these lists.”
Christopher Beemer, a 75-year-old Brooklynite, is impressed with how well his wife, Carol, maintains friendships with other women and wonders why this valuable benefit to health and longevity “doesn’t come so easily to men.”
Among various studies linking friendships to well-being in one’s later years, the 2005 Australian Longitudinal Study of Aging found that family relationships had little if any impact on longevity, but friendships increased life expectancy by as much as 22 percent.
Mr. Beemer urged me to explore ways to promote male friendships, especially for retired men who often lose regular contact with colleagues who may have similar interests and experiences.
After Marla Paul, a Chicago-area writer, wrote a book, “The Friendship Crisis: Finding, Making, and Keeping Friends When You’re Not a Kid Anymore,” about establishing meaningful friendships with other women, she was inundated with requests from men to give equal treatment to male friendships.
“A lot of men were upset because I didn’t include them,” Ms. Paul told me. “They felt that making and keeping friends was a lot harder for men, that close friendships were not part of their culture. They pointed out that women have all kinds of clubs, that there’s more cultural support for friendships among women than there is for men.”
In a study in the 1980s about the effect on marriage of child care arrangements, two Boston-area psychiatrists, Dr. Jacqueline Olds and Dr. Richard Stanton Schwartz, found that, “almost to a man, the men were so caught up in working, building their careers and being more involved with their children than their own fathers had been, something had to give,” Dr. Schwartz said. “And what gave was connection with male friends. Their lives just didn’t allow time for friendships.”
In their book, “The Lonely American: Drifting Apart in the Twenty-First Century,” the doctors, who are a husband-and-wife team, noted a current tendency for men to foster stronger, more intimate marriages at the expense of nearly all other social connections.
When these men are older and work no longer defines their social contacts, “there’s a lot of rebuilding that has to be done” if they are to have meaningful friendships with other men, Dr. Schwartz said in an interview.
From childhood on, Dr. Olds said, “men’s friendships are more often based on mutual activities like sports and work rather than what’s happening to them psychologically. Women are taught to draw one another out; men are not.”
Consciously or otherwise, many men believe that talking about personal matters with other men is not manly. The result is often less intimate, more casual friendships between men, making the connections more tenuous and harder to sustain.
Dr. Olds said, “I have a number of men in my practice who feel bad about having lost touch with old friends. Yet it turns out men are delighted when an old friend reaches out to revive the relationship. Men might need a stronger signal than women do to reconnect. It may not be enough to send an email to an old friend. It may be better to invite him to visit.”
Some married men consider their wives to be their best friend, and many depend on their wives to establish and maintain the couple’s social connections, which can all but disappear when a couple divorces or the wife dies.
Differences between male and female friendships start at an early age. Observing how his four young granddaughters interact socially, Mr. Beemer said, “They have way more of that kind of activity than boys have. It may explain why as adults they continue to do a much better job of it.”
In defense of his gender, he observed, “Men have a harder time reaching their emotions and are less likely than women to reveal their emotional side. But when you have a real friendship, it’s because you’ve done just that.”
He has found that “it’s important to expose yourself and be honest about what’s going on. If you reveal yourself in the right way to the right person, it will be just fine. There are risks, you can’t force it. Sometimes it doesn’t work — you get a don’t-burden-me-with-that kind of response and you know to back off. But more often men will respond in kind.”
Mr. Beemer has worked hard to establish and maintain valuable relationships with other men of a similar vintage. He joined a men’s book group that meets monthly, and after about two years, he said, “it became a group where the members really mean something to one another.”
He’s also in a men’s walking group that meets three times a week and gathers after each walk to share more conversation and a snack at a local cafe. When one member of the group had a heart attack, they visited him, cheering him up with the latest gossip and a favorite cafe snack.
“What sustains relationships over time is a regular rhythm of seeing each other,” Dr. Schwartz said. “It’s best to build a regular pattern of activities rather than having to make a special effort to see one another.”
He recalls “curing” a 70-year-old patient of his loneliness by encouraging him to join a bunch of guys who regularly dined and joked around at a neighborhood Panera Bread. “There are a lot of cafes in the Boston area where small groups of older men get together for breakfast everyday,” Dr. Schwartz said.
Dr. Olds said of her husband, “Richard has a regular group phone call with friends who live in different parts of the country. We program it into our schedule or it would disappear.”
Among other ways men can make new friends in their later years are participating in classes, activities, trips and meals at senior centers; taking continuing education courses at a local college; joining a gym or Y and taking classes with people you then see every week; volunteering at a local museum, hospital, school or animal shelter; attending worship services at a religious center; forming a group that plays cards or board games together; perhaps even getting a dog to walk in the neighborhood.
After my dentist’s wife died, he made several new friends and enjoyed lovely dinners with other men when he joined a group called Romeo, an acronym for retired old men eating out.
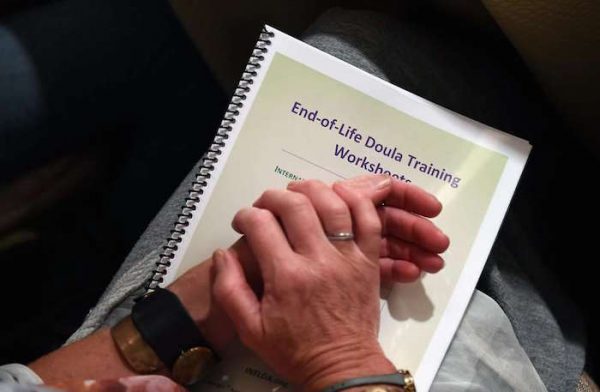
Henry Fersko-Weiss, co-founder and president of the International End of Life Doula Association, conducts a session at the association’s training at the Omni Hotel in San Francisco.
The emotional crumbling started when she was 14 and a friend was killed in a car crash. Three years later, her father died when his helicopter exploded. When she was in her 30s, her brother committed suicide.
By the time a close friend was murdered three years ago, the coping skills Bonnie Ludwig had for dealing with death were shattered — and she found herself one day on her knees on a sidewalk, sobbing obliviously.
Therapy gave healing, which allowed her to help comfort dying dogs at the pet care company she runs — and which soon led to her sitting in a San Francisco hotel room on Friday, learning how to help people die better.
Ludwig, 45, was taking a class in how to become a “death doula,” someone who helps shepherd the dying and their families into loving, peaceful exits. The man who founded the craft in 2003, Henry Fersko-Weiss, is guiding her and 47 other students through a weekend-long course on handling what for many seems like the worst moment possible — but, if handled deftly, can be a beautiful journey to whatever lies just beyond a heartbeat.
‘Learn to let go’
“Humans hold onto life so tightly,” said Ludwig, who flew up from San Diego to take the $600 training at the Omni Hotel. “We need to learn to let go better. We grieve so badly in our culture, and I have found it is sacred and an honor to be with animals when they die. Now I want to be able to do that with people.”
Fersko-Weiss, 68, has trained more than 1,000 people in his discipline, and this was his first session in San Francisco. People come to his trainings for many reasons, he said — some from pain, like Ludwig, some because they’ve already helped others die and feel a calling to do more. But they all have one thing in common.
“I have found that the people who come to these trainings have a great deal of compassion and want to serve people at this incredible period in their lives — death,” said Fersko-Weiss, who lives in the small town of Warwick, N.Y. “They are self-selecting. Like me, they feel this is a way they can really do some good and help. It’s very intense and very important.”
The idea of finding a better way of dealing with the obliteration of life came to Fersko-Weiss when he was a hospice volunteer and saw too many people missing the last breaths, not saying the words they wanted to say before passing, not feeling complete in what they were leaving behind.
Laura Statton attends the training session by the International End of Life Doula Association at the Omni Hotel in San Francisco.
He had a friend who was training at the time as a birth doula — a midwife of sorts, who helps birthing moms and their partners stay comfortable and well-centered — and he found the approach so dynamic he took the course himself.
What he learned there led him to co-found the International End of Life Doula Association. Doula, in ancient Greek, means “woman who serves.”
“It’s just our human nature that we want to be reassured as we die,” Fersko-Weiss said. “We’re going into the unknown, and everybody has fear of passing that boundary between life and death.
“I believe the only thing that counts at the end is having people we love, someone at your bedside, talking to you, telling them how much they love them, reassuring them it’s going to be OK. Those things are important.”
Calming techniques
Students learn techniques for calming the dying and their family and friends, and then they help them find the right kind of intimacy to say the things that need to be said. To cut to the chase about what they want to be remembered for, to compile scrapbooks. To face the end with grace.
Lori Goldwyn attends the training session by the International End of Life Doula Association at the Omni Hotel.
Sometimes doulas ease pain by having the dying visualize soothing times in their lives or by giving therapeutic touch. And they help plan what the final moments will be like. Sometimes people want candles burning, certain clothes, favorite poems read out loud. Doulas stay at the bedside, ready to recognize when death is minutes away — mottled skin, fingernails turning blue, other clues — so everyone can be prepared.
Cynthia Imperatore, who lives in New Jersey and is helping Fersko-Weiss at this weekend’s training, found that sometimes the simplest actions are the most important.
Recently she was helping a son sit vigil with his terminally ill mother, and found herself sitting at the woman’s bedside, holding her hand while the son stood stiffly at the foot of the bed with a TV blaring in the background. The final minutes were near. It didn’t feel right.
“I had him turn off the TV, put on some classical music, and I said, ‘Come here and hold your mother’s hand,’” said Imperatore. “So he came, and then I said, ‘Tell her these things’ — in Spanish, because that’s what his mother spoke. I said, ‘Tell her she’s done everything right. Tell her you’re grateful. Tell her you love her. Tell her what she did mattered.’
“And what happened is that these were the last words she heard,” Imperatore said. “He didn’t have to carry a sense of unfulfillment with him. It was good.
“What we do is not morbid,” she said with a gentle smile. “It’s a privilege to be there when people are dying. Death takes us to a place where we seek meaning, makes you question what is life. And sometimes it can make you appreciate life more.”
While laughter provides plenty of health benefits, laughing uncontrollably for a longer duration carries health risk for individuals with heart ailments.
Laugh your way to good health. This is one piece of advice that often works in improving overall well-being. A good hearty laugh can work wonders in relieving stress. There is no better feeling than being with someone who makes you laugh. However, it appears that laughing too hard continuously may not be as good as it seems.
The British Medical Journal in its recent report highlights the ill-effects of excessive laughing in people suffering from various medical conditions. The research was carried out by University of Birmingham’s R. E. Ferner and Oxford University’s J. K. Aronson.
A normal laugh where there is no excessive sound is indeed good for the cardiovascular system. However, excessive laughter causes the blood pressure to increase substantially, putting too much pressure on the heart. A defective heart due to medical conditions like coronary artery disease and congestive heart failure (CHF) may not be able to handle such excessive pressure.
Intense laughter also increases the heart rate considerably, which patients with heart conditions are unlikely to tolerate for long. To put it simply, a faulty heart might not be able to sustain the increased heart rate associated with hard laughter.
Excessive laughter can also be fatal to people affected with cerebral aneurysm. Laughing out vigorously can considerably increase intracranial pressure (ICP refers to pressure inside the skull). This can cause the aneurysm to burst, which may lead to stroke. Even people with other neurological disorders are advised to avoid uncontrollable laughter to keep complications at bay.
Laughter-induced Asthma
People suffering from asthma should also stay away from laughing too hard. In one study, patients noticed that their symptoms (chest pain and coughing) worsened due to excessive laughing. However, it was observed that laughter-induced asthma wasn’t a case of medical emergency.
Also, the patients reported that when they can manage their asthma well, symptoms do not flare up when laughing for a longer duration. This means that exacerbation of symptoms due to laughter indicates that asthma is not being managed properly. Nevertheless, intense laughter may trigger asthma attacks. Hence, patients ought to take a cautionary approach when it comes to laughing loudly.
Laughing too hard also puts excessive strain on the chest muscles. Hence, people affected with respiratory conditions such as collapsed lung are often advised to avoid laughing loudly.
Laughter-induced Syncope
It is observed that intense laughter increases the breathing rate and when this continues for a longer duration, say for 10 to 15 minutes, it can be risky even to healthy individuals.
People have experienced shortness of breath during fits of laughter. There also have been reports of people losing their consciousness temporarily (for around 3 to 5 minutes); some have blacked out for a few seconds due to unrestrained laughter. Experts warn that excessive laughter tends to cause hyperventilation, which carries health risk but is unlikely to result in death.
A fit of hysterical laughter can also cause hernia to bulge out. Jaw trauma such as a dislocated jaw can also be one of the side effects of laughing too much. Excessive laughter is also responsible for triggering cataplexy, a condition that is marked by sudden temporary loss of muscle function.
Dr. Martin Samuels, professor of neurology at Harvard Medical, opines that extreme strong feelings related to sorrow or happiness stimulate an area of the brain corresponding to fight or flight response. During a fight or flight response, chemicals like adrenaline are released into the body. Too much of adrenaline can be detrimental to health, particularly the heart. So handling emotions (good or bad) in a better way is necessary to manage overall health.
Death from Laughter
There also have been confirmed reports of people laughing their way to death. In one instance, in 1989, Ole Bentzen, a Danish audiologist while watching a heist-comedy film A Fish Called Wanda went into uncontrollable fits of laughter. He began laughing so intensely that his heart started beating very fast and the heart rate was found to be fluctuating between 250 to 500 heartbeats per minute. This eventually caused cardiac arrest.
In another instance, in 1975, Alex Mitchell from England had uncontrollable fits of laughter while watching a television episode of Goodies, a popular British comedy series telecasted during the 1970s. He laughed hard non-stop for 25 minutes, which left him breathless due to severe heart failure. Later, it was found that Alex was a patient of long QT syndrome, a rare congenital heart disorder. This heart ailment may also have contributed to his death.
On the whole, experts say that contributory factors such as an underlying medical condition are likely to have played a role in causing deaths due to laughter. However, the fact remains that laughing too hard for long, although not fatal, can cause breathlessness.
Keep in mind that continuous fits of laughter can be risky but that doesn’t mean you should avoid laughing altogether. A good hearty laugh on a daily basis is in fact considered an elixir of life but make sure that the laughter-inducing moments do not leave you out of breath.
A patient at Houston’s Ben Taub Hospital waits on a stretcher in the hallway for space in the emergency room to open up.
Doris Portillo keeps the door to her father’s old room closed to avoid remembering the last few months of his life. It’s a small room, barely large enough for a bed, a small bureau, and a television, all of which are long gone. This is where she, her siblings, and her nephew cared for her father, Aquilino Portillo—feeding him, lifting him out of bed to take him to the bathroom, doing their best to clean the sores that festered beneath his weight.
A naturalized citizen from El Salvador, Portillo brought her parents to the United States in 2001 and sponsored their green cards so that she could take care of them as they aged. In late 2013, when Aquilino was diagnosed with end-stage metastatic prostate cancer, she discovered how difficult taking care of him would be.
Portillo’s insurance through her employer—she works nights cleaning offices for the City of Houston—didn’t cover her father, and the family couldn’t afford to buy insurance for him. They tried to determine if he could qualify for Medicare, the federal health benefit for the aging, or Medicaid, the state-run health insurance for the poor, but were given conflicting responses depending on whom they talked to. Confused by the requirements and limited by her poor English, Portillo applied for Medicaid for her father, but never got a response. So, for the better part of a year, the Portillos carted Aquilino back and forth to the emergency room in a wheelchair, where they would wait for hours, sometimes all night, simply to have his pain medications refilled.
As Aquilino’s condition worsened, he could no longer be moved from his bed to see a doctor. His body was riddled with tumors. His legs became too heavy for him to move, and his pain became unbearable. “It was ugly, ugly and scary, to see a loved one dying,” Portillo says in Spanish. “And if that person is your father, it’s something indescribable.”
By the time Portillo found out about a small county program that sends health workers to the homes of low-income, bedridden patients, her father had been at home without pain medication for two and a half months. The nurse practitioner who came, spurred by Aquilino’s obvious suffering, rushed to order medication to make him more comfortable. Two days later, when the morphine had barely had a chance to soothe him, he was gone.
“Sometimes people die and death is sweeter,” Portillo says. “I don’t think death is ever sweet, but they suffer less. My father suffered so much, he really fought to leave us.”
Portillo is not alone. Some 28 million people in the United States do not have health insurance, and for the dying and their families, lack of insurance is devastating. Though the care needs that arise with terminal illness are simple, they are often prohibitively difficult to meet without insurance. The uninsured and their families are left to navigate public and charity end-of-life care options that vary widely across the country, if they are available at all. There are no data on how or where the uninsured access this care, and the scope of unmet need is virtually unknown. What is known is that, at the end of their lives, many uninsured people quite literally cannot afford to die with dignity.
* * *
For the most part, patients with insurance have a choice when they receive a terminal diagnosis. Some choose to exhaust all possible avenues for fighting their disease, hoping conventional treatments or experimental drugs will prolong their lives. But when treatment fails or its toll is too great, the quality of a person’s final months or weeks often matters more than prolonging them. Doctors tend to steer those patients toward hospice, the holistic form of palliative care that focuses on treating symptoms in order to make a patient more comfortable and functional as they near death.
One of the fundamental tenets of hospice care is that patients and their families will have a better experience of death if the patient dies at home, among loved ones and familiar surroundings. The actual care is fairly simple, and focuses on managing symptoms and making the most of the time the patient has left. Family members administer most of this care, with support from the hospice team (a doctor, nurses, and often a social worker, chaplain, or volunteers), whose oft-repeated motto is to “care for the caregivers.”
Hospice began on the fringes in the 1960s and ’70s, somewhat at odds with the American medical-industrial complex. Hospice for Medicare-enrolled adults can’t begin until curative treatment has been abandoned, something that’s difficult for many patients, their families, and even their doctors to do. But hospice has gained a mainstream foothold over the last few decades, as doctors and patients have increasingly accepted that “life-extending” treatments can make dying more painful, often with little or no benefit to the patient. The vast majority of hospice recipients—about 85.5 percent—access the service through Medicare, and the proportion of Medicare beneficiaries using hospice before they die has more than doubled since 2000. The Centers for Medicaid and Medicare Services recently began reimbursing doctors for time spent explaining the benefits of hospice to their Medicare-funded patients, further encouraging hospice advocates, who see a lack of awareness as the fundamental barrier preventing patients from getting good end-of-life care.
But what about the millions of uninsured poor Americans who simply have no way to pay for that care? While Medicare, Medicaid, and most private insurers cover hospice, millions of Americans—mostly working-pooradults under 65—don’t have access to an insurance program. In most of the 19 states that have not accepted the Affordable Care Act’s Medicaid expansion, for example, qualifying for Medicaid is almost impossible unless you’re a child, pregnant, a parent on welfare, elderly, or disabled (only Wisconsin is finding ways other than the federal expansion to cover its childless adults). In these states, more than 3 million adults fall into what’s called the ACA “coverage gap”: They don’t qualify for Medicaid under the states’ rules, but make too little to qualify for federal subsidies on the government-run insurance marketplaces. To put this in perspective, in order to qualify for those federal subsidies, a household has to make at least 100 percent of the federal poverty level—about $20,000 a year for a family of three.
The country’s 11 million undocumented immigrants face particularly high barriers to accessing health care, including hospice, as they are legally barred from enrolling in any federally funded insurance program. Some 63 percent of the undocumented population goes without insurance coverage, and studies show that they tend to seek health care less in general, partly due to fears that interacting with any authority could lead to deportation.
Today, more than 76 percent of hospice patients are white, and terminally ill patients are less likely to die at home the lower their incomes. In many poor urban communities, less than 5 percent of the dying receive hospice care in the last six months of life.
Public-health systems around the country are trying to address these disparities, and Harris County, where Aquilino Portillo lived, provides a stark example of just how difficult it is for local safety nets to fill this care gap. Texas has the highest rate of uninsured residents in the country, with nearly 1 million uninsured people in Harris County alone—roughly 22 percent of its population. For employed adults under 65, that number is closer to 30 percent. The Houston area has an expansive health-care safety net that serves the poor, including many private hospitals and clinics that provide some care for free. But it’s the county’s taxpayer-funded hospital district, Harris Health, that is ultimately responsible for providing healthcare to those who can’t afford it. Like many public-health systems around the country, it struggles to handle its uninsured population while simultaneously facing perennial budget problems, due in part to the chronic poverty of its patients. Difficult decisions must be made and priorities set; only so much can be done to care for the dying when so many others need treatment.
Harris Health doesn’t offer hospice, but it pieces together something similar through in-hospital consultations, a palliative-care clinic, and the house-calls program that Doris Portillo found too late. Low-income patients can use these services with financial assistance from the county, which used to come in the form of a laminated “Gold Card,” a name that locals still use to refer to the benefit. But applying for this financial assistance takes precious time—Doris Portillo says she spent a month away from her job trying to get her father Gold Card eligibility—and many people eligible for the benefit are not able to use it. While low-income undocumented immigrants in Harris County are entitled to Gold Card assistance, for example, providing proof of residence and income to establish eligibility can be difficult, since they often share housing and work as day laborers for cash. It’s an unspoken truth in Harris County that the hospital district serves those who can pull together the correct documentation to prove their eligibility for financial assistance, those who can endure the system’s chronically long wait times, and those who can essentially coordinate their own care. Like the Portillos, many end up getting end-of-life care the only way they know how—at the emergency room.
Dr. Ricardo Nuila, a hospitalist at Ben Taub, the largest of Harris Health’s three hospitals, describes the county’s emergency rooms as a kind of revolving door for terminally ill poor people. The uninsured tend to find out about serious illnesses like cancer later than the insured, since they use primary health care less frequently and are twice as likely to postpone or go without medical care due to cost than those with insurance. This means that by the time many uninsured patients seek care, their symptoms are acute and require immediate attention in an emergency room. But even those in non-emergency condition simply see no alternative to the ER—federal law requires emergency providers to stabilize a patient’s symptoms regardless of his ability to pay. Once that’s done, the patient is usually sent home; for terminal patients, this cycle only repeats as their condition worsens.
“That’s one of the most concerning things when you’re working in the hospital and you walk through the emergency room,” Nuila says. “The patients might actually have their pain and their suffering well controlled with medications at home, but they’re in the emergency room just to get prescriptions.”
Emergency rooms are brutal places for the dying. Patients and their families can spend entire days waiting to be seen by a doctor. In 2013, a local news channel reported 14-hour wait times at Ben Taub, with as many as 100 people at a time filling the reception area. Terminally ill patients must describe their symptoms again and again as they pass through various levels of triage, often undergoing tests or procedures intended to lay the groundwork for treatment they know is futile. Once admitted to the hospital, they are disturbed every couple of hours by nurses checking vital signs, even if the patient has only hours to live. There are the sounds and smells of other patients, and the comings and goings of a legion of hospital workers. “You’re dying in a semi-public place,” says Nulia. “That can be very difficult for somebody who’s trying to have an environment of respect for their dying one.”
Hospitalists like Nuila try to send terminally ill patients home with as much medication as possible and some sense of how to keep their symptoms at bay. The textbook next step for insured patients, he says, is to suggest hospice so that families can get the proper care at home. But he knows that many of his patients can’t afford it. “In a way, we’ve just sort of come to accept poor outcomes for unfunded patients,” he notes. “We just say, ‘OK, let’s hope that they get hospice services, or charity hospice kicks in.’”
According to the National Hospice and Palliative Care Organization, only around 1 percent of hospice services in the United States are delivered free of charge to families who otherwise have no way to pay for them. Nonprofit hospice centers are often required to provide some charity care, but there are no government guidelines as to who should receive it or how much of it should be available in a given geographical area. One-fifth of all hospices nationwide provide no charity care.
Nuila estimates that Ben Taub is able to connect unfunded patients with charity hospice only about half the time, though Harris Health doesn’t officially keep track of that number. It is rare for charity care to be flat-out unavailable, but for indigent terminally ill patients who often have only days to live, the wait time—commonly four to six weeks—is as good as nothing. When they can’t get a patient into hospice, the already overworked doctors, social workers, and case managers at the hospital do their best to piece together the next-best thing.
Alexie Cintron is one of those doctors. A palliative-care specialist who provides serious-illness consultations for hospitalized patients at Ben Taub, he also runs an outpatient palliative-care clinic for patients who are staying at home. Provided the patient is covered by a Gold Card and can make it to the clinic to see him, Cintron can show family members how to care for their dying loved one and send them home with equipment like a hospital bed or a bedside commode, and they can get prescriptions filled through the system’s own pharmacy at Ben Taub.
“Essentially, I’m kind of a hospice doctor by default,” Cintron says. “We can’t find them hospice, we don’t provide hospice as a system, and so I’m the fallback.” But the help that Cintron provides is a far cry from the comprehensive and consistent care provided by hospice, and he and the nurse practitioner he works with can stretch their time only so far. “Many times we struggle with being able to support the family enough so that we try to keep this patient from bouncing back to the hospital in the next week or so.”
For poor families, the difficulty of providing good care for their loved one often stretches far beyond the health-care system itself. “If they have to take three different buses in order to get to our clinic, they might not be able to make it in time [for an appointment],” Cintron says. Money is often an issue—even with financial assistance from the county, which can lower the cost of filling a prescription to as little as $8, some people are unable to afford their medicines. Then there’s the scarce resource of time. Family members have to take off work or find child care, and they must make time to keep appointments, get prescriptions filled, and apply for financial assistance. This is all before they’ve spent any time actually caring for their dying loved one.
For at least some indigent patients, however, Harris Health does provide something akin to hospice care in the home. Dr. Anita Major is director of the system’s geriatric house-calls program, the one that was able to visit Aquilino Portillo only once before he died. The service began in the 1980s, but has expanded its patient load fourfold since 2010 in an effort to address the need for home care in the community. It’s not hospice, she says—partly because it generally involves less frequent visits, less comprehensive support, and only serves patients who are unable to leave their homes for medical appointments—but it’s pretty close. Like many uninsured people, however, Major’s poorest patients often connect with home care only when their illness has reached a crisis point and the extremity of their symptoms requires hospitalization anyway. “The problem is we meet them and, you know, 10 days later they’ve died,” Major says. “And we really should have met them a year before that.”
But the most vulnerable population, says Major, are those who never cross paths with the system—people who may be eligible for county health services but don’t know it or can’t access them. For every family like the Portillos, who find care too late, there are likely many more who never find it at all. “I think it’s a lot more than I’m aware of,” says Major. “Those are the people that I think really are suffering, and they’re just invisible to us.”
* * *
Nationwide, it is hard to say just how many people who want or need end-of-life palliative care are forced to go without it. One recent nationwide survey assessing the availability of palliative care in general (including for nonterminal patients) showed that, while the prevalence of palliative programs in hospitals is steadily increasing, fewer than half of the country’s rural or isolated hospitals offer the option at all, let alone to unfunded patients. Statistics on hospice itself are generally tracked through utilization by Medicare and Medicaid beneficiaries, and there is no database for how or where the uninsured access the service.
“It’s difficult to measure unmet need,” says Carol Spence, vice president for research and quality at the National Hospice and Palliative Care Organization. She adds that quantifying hospice access is complicated by its elective nature. “There’s not a defined population that should have hospice like there is for a given illness,” she says. “Hospice is a choice.” But it’s a choice many of the dying poor don’t have.
For safety-net providers, expanding access to hospice is not a simple question of funding the service itself. Though outpatient hospice services cost on average 15 times less than treating the dying in a hospital—between $100 and $200 per day for hospice versus close to $3,000 per day in a Texas public hospital—offering hospice through public systems like Harris Health would actually increase the overall cost to those systems. Public hospitals tend to have far more demand for care than they can meet, so a bed vacated by a patient transferring to hospice will immediately be filled, and the hospice patient’s care will amount to a new expenditure. Like many public-health systems around the country, Harris Health is facing a deficit this fiscal year—$8 million—even after cutting overtime for its staff and reducing the number of people who qualify for Gold Card assistance. Because these systems are struggling to fund even their preventive care, adding to their deficits to treat the already dying is simply not an option.
The underlying reality is that local safety nets can only be expected to do so much for America’s uninsured, whose real problem, especially at the end of life, is that they don’t have insurance. According to the National Hospice and Palliative Care Organization, the most efficient way to increase access to hospice for low-income patients is to provide insurance coverage to the nation’s 28 million people who currently don’t have it. “It’s better to insure people ahead of time than to subsidize safety-net care after the fact,” insists Charles Begley, a veteran health-care researcher at the University of Texas School of Public Health. “There are many very valuable, very important, very cost-effective health-care services that this limited, publicly funded health-care system cannot address.”
Not only would insurance allow indigent patients to use the same hospice providers as the more well-off, but the consistent access to primary care that comes with being insured would make them more likely to hear about the service and choose to use it earlier in their illness. At the same time, Begley adds, insurers would have a financial incentive to make hospice a more visible and readily available option throughout the health-care system. Safety-net providers could focus their resources on acute and preventive care, and everyone would be better off.
But the United States is a long way from providing insurance to all. Four of the five states with the highest uninsured rates have decided not to expand their Medicaid programs under the Affordable Care Act, or even to set up their own insurance exchanges. According to the Kaiser Family Foundation, nearly 5 million more people nationwide would qualify for Medicaid—and gain access to hospice coverage—if their states chose to expand. If Texas were to expand its Medicaid program under the ACA, it would bring in nearly $6 billion in new federal funding and insure 2 million low-income adults, nearly 400,000 of them in Harris County alone.
In the current political climate, however, that seems unlikely to happen. Texas and the other eighteen states that have refused to expand Medicaid coverage currently rely on temporary federal funding to reimburse their safety net systems for the uncompensated care of uninsured patients. While half of Harris Health’s $1.3 billion budget comes from county property taxes, for example, about a quarter of it comes from these reimbursements. (Harris Health’s palliative-care services, including the house-calls program, were either created or expanded to their current level using this funding.) US Health and Human Services Secretary Sylvia Burwell has made it clear that while the federal government won’t punish states for not expanding Medicaid, it does expect them to come up with a viable long-term alternative in return for continued funding. Policy-makers in Texas, as in other Republican-controlled states, claim they merely want the freedom to design their own indigent-care systems without federal constraints, but the Texas legislature has made no move to put a long-term strategy in place. Analysts like Begley believe that lawmakers are waiting for the results of the 2016 election to determine their next moves—and in the meantime, safety-net funding is far from secure.
The election could, indeed, be a turning point. Donald Trump, the presumptive Republican presidential nominee, has vowed to repeal the Affordable Care Act—a move that health-policy experts warn would reverse the real progress the law has made in insuring low-income Americans. The Democrats would do the opposite: Presumptive presidential nominee Hillary Clinton plans to expand the ACA toward a goal of universal coverage, while Bernie Sanders proposes placing all Americans and undocumented immigrants under a federally administered, single-payer healthcare program.
“This is another make-or-break election for the Affordable Care Act,” said David Blumenthal, president of the Commonwealth Fund, a health-care research foundation, addressing a conference at the Harvard Law School in January. At the same time, he added, “we are now, for the first time in a generation, actively debating how far left to go with health-care policy.”
But until that debate results in tangible changes in how the health-care system works, the burden of caring for those who are dying in poverty will remain mostly on the shoulders of families like the Portillos, who simply do what they can to ease their loved one’s pain when the system isn’t there to support them.
“Of course,” says Portillo, “there is another way.” And, of course, she’s right.
All my life, my walls have been painted different shades of white, and beige. Ordinary, predictable hues, “normal” and controllable in feel.
My childhood bedroom was a cool shade of white, with Tiger Beat pull-out posters and a 1978 World Champions Yankees poster from Burger King thumbtacked to my bulletin board. My college dorm room walls were made of cinder block with the gum-tacked picture collages I had made of my family, high school and camp friends. My first New York City apartment was a rental — with eggshell painted walls. The Georgia O’Keefe print I had picked up at Bed and Bath, added some warmth, the pastel palette calming. But the walls around me, I always kept those in tones of white, off-white, and beige.
When I got married to my boyfriend of four years, and a year later gave birth to our beautiful son, we moved to the New Jersey suburbs. And yes, we painted our walls different shades of white and beige in our new home.
In 2004, the oldest of my two sisters needed me. She’d been battling stage 4 ovarian cancer for seven years, and we’d learned I was a stem cell donor match, and her best chance to beat her cancer. So, I took time off from my job, and brought my two-year-old-son back and forth for each of my sister’s two-week long treatments at M.D. Anderson in Houston.
A few months before her treatments began, my sister was still living back in Atlanta, at home with her husband and two daughters. “What’s this?” her husband asked after work one night, upon seeing the scattered paintbrushes and Benjamin Moore color wheel. “Life’s too short for beige,” my sister said. It only took a week for every room in their house to get a fresh coat of paint. From rooms of white and off white to bold and bright-colored walls.
As my sister fought her battle, I fought my own. Like the tick of a kaleidoscope, my entire world of control tumbled and rotated; suddenly, my life of white walls felt unstable and discomforting.
Perhaps it was also when I began to realize that my sister’s doctor, the one I had first laid eyes on during round one of the stem cell transplant, was my perfect match. She explained how my blood and stem cells could save my sister, but she also opened my eyes to understanding how my sister’s “you can’t control what life will throw at you, but you can control how you deal with it” philosophy directly related to the safe and normal box I had created for myself all those years, and the reality I had been trying to shove away.
My big sister, who walked the hallways of the MD Anderson Cancer Center in her Fresh Produce clothes and her bald head held high with a Life is Good baseball hat covering it, even during a time of grave uncertainty, with her cross body canvas handbag adorned with different sized John Kerry for President buttons — in Texas, aka Bush country.
The truth is, I was a gay woman trying to convince myself it would be easier to live surrounded by safe, white hued walls rather than within my own colorful world.
My sister knew of my decision to live my truth before she passed away, a year after her transplant. Her doctor, today my wife, and I live together in our suburban New Jersey colonial. We have three children, two of whom are named after my beautiful and brave sister. And our walls? All of them are painted the brightest and boldest colors of the Crayola box. Just how we like it.
Today’s posting comes to us via Clare O’Leary | Palliative Care Educator | Mary Potter Hospice | Wellington, New Zealand
Maori digital stories about caring for kaumatua (elders) at the end of life. Teaching resource for nursing students, nurses and other health professionals who want to know more about Maori whanau (family) end of life needs and priorities.