CENSUS
By Jesse Ball
272 pp. Ecco/HarperCollins Publishers. $25.99.
[J]esse Ball is one of our most prolific experimentalists. His last few novels, starting with the excellent “Silence Once Begun,” demonstrate a mature style that feels less like an experiment than a means to communicate deep emotional truths without the clutter of too many narrative conventions.
“Census,” Ball’s eighth and latest novel, may be his most emotionally affecting book to date. It is also his most transparent. In a candid preface, Ball explains that he wrote “Census” in memory of his brother, Abram Ball, who had Down syndrome. Ball sets out to write a book that captures “what it is like to know and love a Down syndrome boy or girl.”
In “Census,” a father and son journey across a nameless, dystopian land. The father, a recent widower and retired doctor, has just received news that he is dying. Both he and his wife had always meant to travel, but because their son was born with Down syndrome, they talked themselves out of it. The cruelty of others kept them from the road: “Ever since he was born, our lives, my wife’s, mine, bent around him like a shield.” Now, with his wife passed on, his son grown and his own end very near, he devises a plan to become a census taker, which will take him and his adult son on a cross-country road trip.
The census itself is part of the novel’s central mystery. It is both a survey of the population and an existential measurement. The father explains, “I must, in speaking to a person, know what is special about that individual, and that data must pass through me … in such a way that what is … most special about the nation … could be known and felt.” He asks participants to tell their own unique stories, after which they are marked — tattooed — on a rib, proof that they have been tallied. While the census may sound like an Orwellian device, Ball is more concerned with his characters’ emotional lives than with authoritarian foreboding. The father and son move from region to region, entering strangers’ homes, administering the census. With each new encounter a story from the narrator’s life is revealed. The best of these recall him falling in love with his wife, a renowned clown and performance artist who is also one of the novel’s most dynamic characters. In one lovely scene, prompted by his encounter with two eccentric sisters who conjure the Beales of “Grey Gardens,” the narrator remembers a performance in which giant pieces of silverware, a knife and fork, hovered overhead as his wife and other clowns evaded them. In a novel that ruminates so heavily on death, such memories provide a celebratory sense of joy.
While Ball accomplishes the stated goal of his preface, bringing the son with Down syndrome to life, the census itself leaves a little to be desired. If the narrator aims to hear each citizen’s story, that which is “most particular, most special,” he never shares enough details to make a lasting impression. This creates a kind of flatline with regard to the central conceit. Without more of the particulars, “the small, the overlooked,” it’s hard to understand what the census is meant to measure.
Yet the spare and episodic encounters do take us to some tender places. In one scene, a mother who raised a girl with Down syndrome recognizes the narrator as someone who sees what she sees in their children: “They experience the world just as we do, maybe even in a clearer light.” More than a dystopian tale, “Census” is a profound and stirring meditation on love, loss and paternity.
That sounds judgmental, but it’s more akin to wishful thinking.
While death is a certainty, it’s rarely a goal, so we tend to resist, to worry, to grasp at new treatments or old beliefs.
But the emerging death doula movement offers another option: We can’t change the destination, but we can improve the journey.
The term doula is more linked to childbirth, describing someone present during labor to help a mother feel safe and comfortable. There’s no medical role; doulas are companions and listeners. They attend.
End-of-life doulas, also called death doulas or death midwives, similarly are attuned to a dying person’s emotional needs.
“It’s about filling a gap that the system doesn’t acknowledge,” said Christy Marek, an end-of-life doula from Lakeville. “The system is designed to tend the body. But when you get into the lonely feelings, the mess of real life, the expectations and beliefs around dying — those things don’t fit into the existing system.”
In some ways, death doulas signal a return to earlier times, when ailing parents lived with children, when life-extending options were fewer.
“Death was more of a ritual, really laboring with someone as they were dying,” said Jeri Glatter, vice president of the International End of Life Doula Association (INELDA) in New Jersey.
Family and friends “felt a sense of acceptance and completion and a knowledge that they had fully honored someone,” she said. “It’s the most loving act that they could do.”
Over time, though, “we became a very medicated society — and thank God for that. I don’t want to diminish that,” Glatter said. But medical options can create a sense of disconnect with our inevitable mortality. When those options are exhausted, “we say we’ll house them, make sure they have medication and have a bed that goes up and down.
“But people are saying, ‘I don’t feel OK about this.’ ”
Marek is the first end-of-life doula in Minnesota certified by INELDA, credited with creating the first death doula program for hospitals and hospices in 2003. It offered its first public training in 2015; last year, 700 people attended 18 sessions. Several other groups in Minnesota and elsewhere offer training and doula directories.
Glatter said the trend has roots with those who used birth doulas in the 1980s.
“These people now are burying their parents. Just as with birth, as we labor into the world fully engaged in that process, they’re saying, ‘I want to be fully engaged in this process.’ Doulas are the bookends of life.”
How can we do this together?
What does it mean to be fully engaged? Whatever the dying person wants it to mean.
“Is the person having their own experience, instead of trying to meet the expectations of the family?” Marek asked. “I’m there to create a space for the person who is dying to ask, ‘How can we do this together?’ ”
One woman, for example, asked Marek to tell everyone that she wanted acknowledgment — a greeting — each time someone entered her room, “even though it may look like she’s sleeping.”
Marek added, “I have no agenda other than reflecting to that person what they are saying, what they are feeling. I can give directions to family and friends, which is a comfort to the dying person because then people around them know what to do — and they feel listened to.”
As part of a new field, doulas occupy a niche among doctors, family, hospice and other factors. Sometimes, doulas fill practical needs, gathering paperwork or helping with funeral plans, particularly if relatives are distant, either geographically or emotionally.
More often, though, their roles are more personal: creating a vigil environment, writing letters to loved ones, helping family members recognize the signs of dying such as a change in breath and, finally, helping survivors deal with their loss.
Glatter said that doctors or hospital personnel sometimes worry that a doula will infringe upon medical decisions. But doulas have no medical role, and may even be able to provide information that doesn’t come up in medical conversations, “such as, ‘Do you know there’s a son with a restraining order?’ ”
Doulas’ lack of medical standing also enables consistency. Doctors may change. Hospice care may be suspended. “But a doula provides a continuity of care no matter what treatments are being done or not,” Marek said.
Dying as a creative process
Marek, 47, appears to wear not a speck of makeup. The physical transparency mirrors her comfort with the emotions that dying can expose. But it took her years to reach this point.
With a degree in child psychology, she intended to work with youngsters. Then she met a child life specialist, a field of which she’d never heard, describing someone who works with children with acute, often fatal, illnesses.
“It was like a lightning bolt went through me,” she said. “I knew that someday I would work with people who are dying. And it scared the pants off me!”
She went on to do other work, in the course of which she explored yoga, shamanism, writing, painting and more. She studied to become an anam cara, from pre-Christian Celtic spirituality that translates as “soul friend.”
Every few years, the idea of working with dying people surfaced, but never took hold. Then, five years ago, she learned about applying doula principles to the dying process. This time, the idea came cast as “the creative process at the end of your life,” and her path was clear.
“I feel like this has been following me my whole life,” Marek said. She took the training through INELDA, which includes vigil planning, working with the survivors, and self-care for doulas themselves. She founded a business, Tending Life at the Threshold.
“As doulas, we’re trying to normalize the experience of death,” Marek said.
She recalled one woman who said that her mother would love it if Marek would read the book of Psalms or a Hail Mary. “And I told her, ‘I can certainly do that. But it would be more meaningful if you did.’ ”
Once family members and friends learn that it’s OK to “lean into the pain,” she said, they may find a sense of comfort and ease with dying that, in turn, proves a gift to their loved one.
Another support system
Karen Axeen had been sick for what seemed like forever, after years of breast cancer and ovarian cancer and other chronic illnesses.
After spending almost all of 2016 in the hospital, she decided to enter hospice care. She also decided that she wanted a doula at her side.
“She kind of fell into the idea, talking with the hospital social workers,” said her daughter, Laura Fennell, who lives in Marshall, Minn. “I don’t live close by, so I think it was really helpful for her.”
Working with Marek, Axeen developed what’s often called a legacy project. In this case, she wrote several letters to each of her six grandchildren, to be read as they grow older.
“She wrote letters to be read on their 16th and 18th birthdays, on their wedding days, on the first day they have kids of their own,” Fennell said.
“I think I probably would have been lost after my mom had passed away, but Christy had everything organized,” she added. “It’s definitely a great service for those who don’t have family in the area.”
End-of-life doulas “are another support system,” Fennell said. “It was important for Mom to be able to get to know someone closely and have them walk her through the final process of life.”
Axeen died on Sept. 23, 2017, at age 57.
‘We know how to die’
Some death doulas volunteer with hospices or churches. Others work in hospitals, while others set up private practices.
Glatter mentioned a California prison where inmates with life sentences became end-of-life doulas “because they wanted to be able to care for their own,” she said. “They’re really an extraordinary group of men who wanted to pay their debt to society by helping other inmates as they die.”
An article in Money magazine included death doulas among “seven new jobs that reflect what’s important in 2017.” Also listed, compost collectors and vegan butchers.
The death doula trend reflects gradually more open attitudes toward death. Surveys show that 80 percent of Americans would prefer to die at home if possible, but few are able to. Yet the landscape slowly is changing. Hospital deaths slowly declined from 2000 to 2010. In that time, deaths in the home grew from 23 percent to 27 percent. Deaths in nursing homes held steady at about 20 percent.
The Centers for Disease Control suggested that the shifts reflect more use of hospice care. As the dying process becomes, for some, more grounded in the home, end-of-life doulas may become more familiar and, in Marek’s vision, help make death a natural part of life.
She reached that vision, in part, during an outdoor meditation project she began in 2014. For 1,000 days, she meditated for 20 minutes outdoors, no matter the weather. (It’s on Instagram as wonderofallthings.)
“Sometimes I’d be thinking, ‘This is awful. But that’s OK,’ ” she said. “It helped me develop a tolerance for whatever is happening, and to stay close to the fact that none of us is immune to the cycles of nature, including death.
“If you can sit when it’s uncomfortable — to be able to sit in the unknown — that’s huge.”
While family members may not be at peace with someone’s death, she added, they can be at ease with it as a natural outcome of life.
“One thing I believe firmly is that we know how to do this,” she said. “We know how to die, like every creature of nature does. We just need to get out of our own way.”
[P]eople still sometimes discuss the question of how you could tell that you were talking to some form of artificial intelligence rather than an actual human being. One of the more persuasive suggested answers is: “Ask them how they feel about dying.” Acknowledging that our lifespan is limited and coming to terms with this are near the heart of anything we could recognise as what it means to be human.
Once we discovered that Neanderthals buried their dead with some ritual formality, we began to rethink our traditional species snobbery about them and to wonder whether the self-evident superiority of homo sapiens was as self-evident as all that. Thinking about dying, imagining dying and reimagining living in the light of it, this is – just as much as thinking about eating, sex or parenting – inseparable from thinking about our material nature – that to have a point of view at all we have to have a physical point of view, formed by physical history. Even religious systems for which there is a transition after death to another kind of life will take for granted that whatever lies ahead is in some way conditioned by this particular lifespan.
Conversely, what the great psychoanalytic thinker Ernest Becker called “the denial of death” is near the heart of both individual and collective disorders: the fantasy that we can as individuals halt the passage of time and change, and the illusions we cherish that the human race can somehow behave as though it were not in fact embedded in the material world and could secure a place beyond its constraints. Personal neurosis and collective ecological disaster are the manifest effects of this sort of denial. And the more sophisticated we become in handling our environment and creating virtual worlds to inhabit and control, the looser our grip becomes on the inexorable continuity between our own organic existence and the rest of the world we live in.
It’s a slightly tired commonplace that we moderns are as prudish in speaking about death as our ancestors were in speaking about sex. But the analogy is a bit faulty: it’s not simply that we are embarrassed to talk about dying (although we usually are), more that we are increasingly lured away from recognising what it is to live as physical beings. As Kathryn Mannix bluntly declares at the beginning of her book about pallia-tive care, “It’s time to talk about dying”. That is if we’re not to be trapped by a new set of superstitions and mythologies a good deal more destructive than some of the older ones.
Each of these books in its way rubs our noses in physicality. Caitlin Doughty’s lively (and charmingly illustrated) cascade of anecdotes about how various cultures handle death spells out how contemporary Western fastidiousness about dead bodies is by no means universally shared. We are introduced to a variety of startling practices – living with a dead body in the house, stripping flesh from a relative’s corpse, exhuming a body to be photographed arm in arm with it… all these and more are routine in parts of the world. And pervading the book is Doughty’s ferocious critique of the industrialisation of death and burial that is standard in the United States and spreading rapidly elsewhere.
Doughty invites us to look at and contemplate alternatives, including the (very fully described) composting of dead bodies, or open-air cremations. A panicky urge to get bodies out of the way as dirty, contaminated and contaminating things has licensed the development of a system that insists on handing over the entire business of post-mortem ritual to costly and depersonalising processes that are both psychologically and environmentally damaging (cremation requires high levels of energy resource, and releases alarming quantities of greenhouse gases; embalming fluid in buried bodies is toxic to soil). Doughty has pioneered alternatives in the US, and her book should give some impetus to the growing movement for “woodland burial” in the UK and elsewhere. At the very least, it insists that we have choices beyond the conventional; we can think about how we want our dead bodies to be treated as part of a natural physical cycle rather than being transformed into long-term pollutants, as lethal as plastic bags.
Talking about choices and the reclaiming of death from anxious professionals takes us to Kathryn Mannix’s extraordinary and profoundly moving book. Mannix writes out of many years’ experience of end-of-life care and presents a series of simply-told stories of how good palliative medicine offers terminally ill patients the chance of recovering some agency in their dying. Those who are approaching death need to know what is likely to happen, how their pain can be controlled, what they might need to do to mend their relationships and shape their legacy. And, not least, they need to know that they can trust the medical professionals around to treat them with dignity and patience.
Mannix’s stories are told with piercing simplicity: and there is no attempt to homogenise, to iron out difficulties or even failures. A recurrent theme is the sheer lack of knowledge about dying that is common to most of us – especially that majority of us who have not been present at a death. Mannix repeatedly reminds us of what death generally looks like at the end of a degenerative disease, carefully underlining that we should not assume it will be agonising or humiliating: again and again, we see her explaining to patients that they can learn to cope with their fear (she is a qualified cognitive behavioural therapist as well as a medical professional). It is not often that a book commends itself because you sense quite simply that the writer is a good person; this is one such. Any reader will come away, I believe, with the wish that they will be cared for at the end by someone with Mannix’s imaginative sympathy and matter-of-fact generosity of perception.
Sue Black’s memoir is almost as moving, and has something of the same quality of introducing us to a few plain facts about organic life and its limits. She moves skilfully from a crisp discussion of what makes us biologically recognisable as individuals and how the processes of physical growth and decay work to an account of her experience as a forensic anthropologist, dedicated to restoring and making sense of bodies whose lives have ended in trauma or atrocity. The most harrowing chapter (and a lot of the book is not for those with weak stomachs) describes her investigations at the scene of a massacre in Kosovo: it is a model of how to write about the effect of human evil without losing either objectivity or sensitivity.
Perhaps what many readers will remember most vividly is her account of her first experience of working as a student with a cadaver. For all the stereotypes of the pitch-dark and tasteless humour of medical students in this situation, the truth seems to be that a great number of them actually develop a sense of relatedness and indebtedness to the cadavers they learn on and from. Black writes powerfully about the sense of absorbing wonder, as the study of anatomy unfolds, of the way in which it reinforces an awareness of human dignity and solidarity – and of feeling “proud” of her cadaver and of her relation with it.
For what it’s worth, having taken part in several services for relatives of those who have donated their bodies to teaching and research, I can say that the overwhelming feeling on these occasions has been what Black articulates: a moving mutual gratitude and respect. And the book is pervaded by the sense of fascinated awe at both the human organism and the human self that comes to birth for her in the dissecting room.
Richard Holloway writes not as a medical professional but as a former bishop, now standing – not too uneasily – half in and half out of traditional Christian belief, reflecting on his own mortality and the meaning of a life lived within non-negotiable limits. His leisurely but shrewd prose – with an assortment of poetic quotation thrown in – is a good pendant to the closer focus of the other books, and he echoes some of their insights from a very different perspective. Medicine needs to be very wary indeed of obsessive triumphalism (the not uncommon attitude of seeing a patient’s death as a humiliation for the medical professional); the imminence of death should make us think harder about the possibility and priority of mending relations; the fantasy of everlasting physical life is just that – not a hopeful prospect, but the very opposite.
He has some crucial things to say about the politics of the drive towards cryogenic preservation. Even if it were possible (unlikely but at best an open question) it is something that will never be available to any beyond an elite; any recovered or reanimated life would be divorced from the actual conditions that once made this life, my life, worth living; how would a limited physical environment cope with significant numbers of resuscitated dead? The book deserves reading for these thoughts alone, a tough-minded analysis of yet another characteristic dream of the feverish late-capitalist individual, trapped in a self-referential account of what selfhood actually is.
****
Odd as it may sound, these books are heartening and anything but morbid. Mannix’s narratives above all show what remarkable qualities can be kindled in human interaction in the face of death; and they leave you thinking about what kind of human qualities you value, what kinds of people you actually want to be with. The answer these writers encourage is “mortal people”, people who are not afraid or ashamed of their bodies, those bundles of rather unlikely material somehow galvanised into action for a fixed period, and wearing out under the stress of such a rich variety of encounter and exchange with
the environment.
None of these books addresses at any great length the issues of euthanasia and assisted dying, but the problem is flagged: Black says briskly that she hopes for a change in the law (but is disarmingly hesitant when it comes to particular cases), while Mannix, like a large number of palliative care professionals, strikes a cautionary note. She tells the story of a patient who left the Netherlands for the UK because he had become afraid of revealing his symptoms fully after being (with great pastoral sensitivity and kindness) encouraged by a succession of doctors to consider ending his life. “Be careful what you wish for,” is Mannix’s advice; and she is helpfully clear that there are real options about the ending of life that fall well short of physician-assisted suicide.
Like all these authors, she warns against both the alarmist assumption that most of us will die in unmanageable pain and powerlessness and the medical amour propre that cannot discern when what is technically possible becomes morally and personally futile – when, that is, to allow patients to let go. The debate on assisted dying looks set to continue for a while yet; at least what we have here goes well beyond the crude slogans that have shadowed it, and Mannix’s book should lay to rest once and for all the silly notion occasionally heard that palliative care is a way of prolonging lives that should be economically or “mercifully” ended.
The most important contribution these books make is to keep us thinking about what exactly we believe to be central to our human condition. It is not a question to answer in terms simply of biological or neurological facts but one that should nag away at our imagination. How do we want to be? And if these writers are to be trusted, deciding that we want to be mortal is a way of deciding that we want to be in solidarity with one another and with our material world, rather than struggling for some sort of illusory release.
Richard Holloway doesn’t quite say it in these terms, but the problem of a humanity that doesn’t need to die is that it will be a humanity that needs no more births. The price of a humanity that actually grows and changes is death. The price of eternal life on earth is an eternal echo chamber. As someone once said around this time of year: “Unless a grain of wheat falls to the ground and dies, it remains only a single seed.”
Waiting for the Last Bus: Reflections on Life and Death
Richard Holloway Canongate, 176pp
All that Remains: a Life in Death
Sue Black Doubleday, 368pp
From Here to Eternity: Travelling the World to Find the Good Death
Caitlin Doughty Weidenfeld & Nicolson, 272pp
With the End in Mind: Dying, Death and Wisdom in an Age of Denial
Kathryn Mannix William Collins, 352pp
Many writers have tried to encourage conversations about dying, often with the aim of helping us achieve a ‘good death’.
Intensive care specialist Charlie Corke.
By Jane Mccredie
[A]t dusk some years ago, I walked past an open doorway in the southern Italian village of Paestum. Just inside, a body lay on a table, candles surrounding it, as locals filed in and out, paying their respects.
It struck me at the time how different this was from the general Australian experience, where the end of life is sanitised, hidden and often medicalised to the point of cruelty.
For centuries, our ancestors would have tended their dying relatives, washed their bodies, stood vigil over them in the homes where they lived and died. Many people around the world still do this, of course, but we in the West are more likely to end our days in aged care or, worse, a hospital intensive care unit. We may be subjected to futile, traumatic interventions right up to the moment we take our last breath.
In recent years a number of writers have sought to encourage franker conversations about dying, often with the stated aim of helping us to achieve a “good death”. Notable local books have come from intensive care physician Ken Hillman, general practitioner Leah Kaminsky and science writer Bianca Nogrady. But the reluctance to talk about death remains.
“It has become taboo to mention dying,” writes British palliative care physician Kathryn Mannix in With the End in Mind:
This has been a gradual transition, and since we have lost familiarity with the process, we are now also losing the vocabulary that describes it. Euphemisms like “passed” or “lost’’ have replaced “died” and “dead”. Illness has become a “battle”, and sick people, treatments and outcomes are described in metaphors of warfare. No matter that a life was well-lived, that an individual was contented with their achievements and satisfied by their lifetime’s tally of rich experiences: at the end of their life they will be described as having “lost their battle”, rather than simply having died.
We must reclaim the language of dying, Mannix argues. Clear, unambiguous conversations about what is ahead offer support to the dying person as well as those who will mourn their death. “Pretence and well-intentioned lies” separate the dying from those they love, wasting the limited time they have left. Mannix first discovered the power of straightforward language as a junior doctor when a superior offered to describe to an anxious patient “what dying will be like”. “If he describes what? I heard myself shriek in my head.”
The senior doctor went on to describe in detail the pattern of dying he had observed over years of practice: increasing tiredness, more time spent sleeping, a gradual drift into unconsciousness, followed by changed respiratory rhythms until the breath finally stopped. “No sudden rush of pain at the end. No feeling of fading away. No panic. Just very peaceful … ” he told the patient.
Back in the tearoom, he told the young Dr Mannix this was probably the most helpful gift they could give their patients. “Few have seen a death,” he explained. “Most imagine dying to be agonised and undignified. We can help them to know that we do not see that, and that they need not fear that their families will see something terrible.” Mannix was left amazed that it was possible to be this honest with patients, revising her “ill-conceived beliefs about what people can bear”, beliefs that could have prevented her from having the courage to tell the truth.
Over the decades since that paradigm-shifting experience, she helped countless people of all ages and backgrounds through the final stages of their lives. Their stories are threaded through this moving and informative book. “The process of dying is recognisable,” Mannix writes:
There are clear stages, a predictable sequence of events. In the generations of humanity before dying was hijacked into hospitals, the process was common knowledge and had been seen many times by anyone who lived into their thirties or forties. Most communities relied on local wise women to support patient and family during and after a death, much as they did (and still do) during and after a birth. The art of dying has become a forgotten wisdom, but every deathbed is an opportunity to restore that wisdom to those who will live, to benefit from it as they face other deaths in the future, including their own.
In Letting Go: How to Plan for a Good Death, Australian intensive care specialist Charlie Corke offers practical tools to help people make and communicate decisions about how they would want to be treated at the end of life.
Corke’s professional experience leads him to paint a very different picture of dying from that offered by Mannix. The specialties of intensive and palliative care are in some ways polar opposites: intensive care does everything possible to ward off the inevitable, while palliative care accepts death, seeking to ease the patient’s approach to it.
Corke admires the triumphs of modern medicine and the many achievements of his specialty, but he has also seen how easy it is for medical treatment to go too far. Most of us will die in old age, after a long period of declining health, he writes. One crisis or another will lead to us being taken to hospital by ambulance where, in the absence of clear instructions from us, medical intervention will escalate:
We will spend our last days connected to machines, cared for by strangers, and separated from our family. We will experience significant suffering, discomfort and indignity, receiving increasingly intense treatment that has a diminishing chance of success. Medical technology will dominate our last days and weeks. Our family will be excluded from the bedside, huddled in the waiting room, while “important” things are done to us. Time for connection and comforting, for any sort of intimacy or the opportunity to say goodbyes, will be missed …
Books on dying: With the End in Mind; Letting Go; Every Note Played
The purpose of this book is to help people avoid that outcome. Corke offers clear advice on questions to ask doctors, on writing and sharing a plan, and on appointing a substitute decision-maker to step in if we are unable to express our own views.
Above all, he stresses the importance of clear, unambiguous communication about what we want to happen at the end of life. If there is any doubt about our wishes, maximum intervention will be the result:
Wishes matter, but it can be difficult to get them heard. Wanting to be saved is easy. “To do whatever is required to save” is what everyone wants to do for you, needs to do, and is expected to do. It’s what our medical system is designed to do. It’s the default; it’s what you get. When we want to set limits, it’s more difficult …
All in all, this is a useful how-to manual for everybody who will at some point face death (which is of course all of us).
In Every Note Played, Lisa Genova chooses a different form to explore the end of life.
Over the decade since publication of her first novel, Still Alice, which was filmed with Julianne Moore in the lead role, Genova has mined her background as a neuroscientist for fictional material, producing novels about dementia, autism, traumatic brain injury and Huntington’s disease. In her fifth novel, she turns her attention to amyotrophic lateral sclerosis, telling the story of Richard, an acclaimed concert pianist diagnosed with the disease at the height of his career.
ALS is the central, and strongest, character in this book, dwarfing the somewhat one-dimensional human actors and the overneat redemptions they achieve. The merciless progression of the neurodegenerative condition is described with elegant, sometimes gruesome, precision as Richard loses the ability to control first his arms, then legs and, ultimately, everything but his eyes
As in the real-life case studies presented by Corke and Mannix, the approach of death presents Richard and those close to him with appalling dilemmas: How much can we ask of others? How far should we go to preserve life? What does quality of life mean?
Richard’s state of mind as his disease progresses is not helped by the hearty refusal of his brothers to accept the inevitability of his fate. “What are you doing to fight it?” one asks when he sees Richard in a wheelchair. “You gotta stay positive. You should go to the gym, lift some weights and strengthen your leg muscles. If this disease starts stealing your muscle mass, you get ahead of it and build more. You beat it.”
Richard manages a slurred response — “Goo-i-de-a” — while privately wondering at his footballer brother’s incomprehension of his condition:
Is living at any cost winning? ALS isn’t a game of football. This disease doesn’t wear a numbered jersey, lose a star player to injury, or suffer a bad season. It is a faceless enemy, an opponent with no Achilles’ heel and an undefeated record … High tide is coming. The height and grandeur of the sand castle doesn’t matter. The sea is eventually going to rush in, sweeping every single grain of sand away.
Richard’s brothers, like all of us, might have benefited from a share in what Mannix refers to as her “peculiar familiarity with death”:
Strangely, this is not a burden or a sadness, but a lightning of perspective and a joyful spark of hope, a consciousness that everything passes, whether good or bad, and the only time we can really experience is this present, evanescent moment.
For a time, eating and relaxing among the dead was a national pastime.
A small group picnics on ledger-style tombstones in Historic St. Luke’s Ancient Cemetery. The photo is not dated but is believed to have been taken prior to St. Luke’s 1957 Pilgrimage Service.
[W]ithin the iron-wrought walls of American cemeteries—beneath the shade of oak trees and tombs’ stoic penumbras—you could say many people “rest in peace.” However, not so long ago, people of the still-breathing sort gathered in graveyards to rest, and dine, in peace.
During the 19th century, and especially in its later years, snacking in cemeteries happened across the United States. It wasn’t just apple-munching alongside the winding avenues of graveyards. Since many municipalities still lacked proper recreational areas, many people had full-blown picnics in their local cemeteries. The tombstone-laden fields were the closest things, then, to modern-day public parks.
In Dayton, Ohio, for instance, Victorian-era women wielded parasols as they promenaded through mass assemblages at Woodland Cemetery, en route to luncheon on their family lots. Meanwhile, New Yorkers strolled through Saint Paul’s Churchyard in Lower Manhattan, bearing baskets filled with fruits, ginger snaps, and beef sandwiches.
A historic image of the Woodland Cemetery in Dayton, Ohio.
One of the reasons why eating in cemeteries become a “fad,” as some reporters called it, was that epidemics were raging across the country: Yellow fever and cholera flourished, children passed away before turning 10, women died during childbirth. Death was a constant visitor for many families, and in cemeteries, people could “talk” and break bread with family and friends, both living and deceased.
“We are going to keep Thanksgivin’ with our father as [though he] was live and hearty this day last year,” explained a young man, in 1884, on why his family—mother, brothers, sisters—chose to eat in the cemetery. “We’ve brought somethin’ to eat and a spirit-lamp to boil coffee.”
The picnic-and-relaxation trend can also be understood as the flowering of the rural cemetery movement. Whereas American and European graveyards had long been austere places on Church grounds, full of memento mori and reminders not to sin, the new cemeteries were located outside of city centers and designed like gardens for relaxation and beauty. Flower motifs replaced skulls and crossbones, and the public was welcomed to enjoy the grounds.
Enjoying a book and a snack in a Lower Manhattan cemetery.
Eating in graveyards had—and still has historical precedent. People picnic among the dead from Guatemala to parts of Greece, and similar traditions involving meals with ancestors are common throughout Asia. But plenty of Americans believed that picnics in local cemeteries were a “gruesome festivity.” This critique, notably from older generations, didn’t stop young adults from meeting up in graveyards. Instead it led to debate over proper conduct.
In some parts of the country, such as Denver, the congregations of grave picnickers grew to such numbers that police intervention was even considered. The cemeteries were becoming littered with garbage, which was seen as an affront to their sanctity. In one report about these messy gatherings, the author wrote, “thousands strew the grounds with sardine cans, beer bottles, and lunch boxes.”
Though the macabre picnics were considered “nuisances” in some communities, they did give participants a sort of admired air. One reporter lauded the fact that the picnickers looked “happy under discouraging circumstances,” and even said it was a trait “worthy of cultivation.” The fad of casual en plein air dining among the crypts would soon come to an end, though.
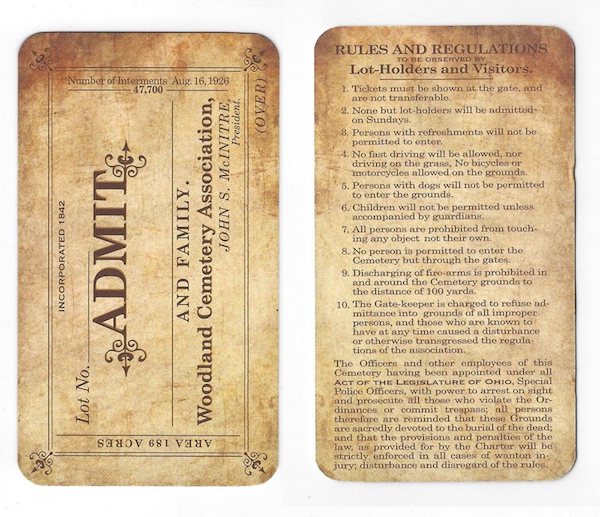
A reproduction of an admittance pass to Woodland Cemetery from 1926; it notably prohibits bringing in refreshments.
Cemetery picnics remained peripheral cultural staples in the early 20th century; however, they began to wane in popularity by the 1920s. Medical advancements made early deaths less common, and public parks were sprouting across the nation. It was a recipe for less interesting dining venues.
Today, more than 100 years since Americans debated the trend, you’d be hard-pressed to find many cemeteries—especially those in big cities—with policies or available land that allow for picnics. Green-Wood Cemetery in Brooklyn, for example, has a no picnic rule.
But the fad isn’t entirely dead in the United States. The country’s immigrant population includes families carrying on traditions that call for meals with departed loved ones, and cemeteries will hold occasional public events in the spirit of this era. There are still scattered graveyards where you can picnic among tombstones, too, particularly if you know someone with a sizable family lot. In those cases, all you need is a picnic basket filled with treats, and you and your undaunted party can partake in an old American tradition. Just remember to clean up after yourselves. The penalties for doing otherwise may be grave.
[L]ocal medical schools are in the process of a curricula revamp that will train students to focus more on end-of-life care, making Massachusetts the first in the nation to reach a statewide commitment to quality of life.
“Massachusetts is really leading the way on this. It led the way on universal health care, on gay marriage, and it’s leading the way on this, too,” said Dr. Atul Gawande, a surgeon at Brigham and Women’s Hospital and author of the book “Being Mortal.” “I’ve learned the question is not do you fight or do you give up. The question really is, what are we fighting for? What’s the quality of life we can fight for?”
The Massachusetts Coalition for Serious Illness Care has orchestrated the effort among four local institutions: Harvard Medical School, Boston University School of Medicine, Tufts University School of Medicine and University of Massachusetts Medical School.
Gawande, co-founder of the coalition, said Massachusetts has the opportunity to create a national model for medical schools across the country.
It’s an important shift, he said, from the fix-it mentality that many doctors are taught to possess. He said the extent of his end-of-life training amounted to an hour of discussion in the first two years of medical school.
“You go in focusing on wanting to be a hero and fix things,” Gawande said. “Teaching people in med school what it means to be an effective clinician for giving people cutting-edge care for quality of life — as opposed to quantity of life — is a neglected skill.”
The medical schools are taking inventory of what skills they’re already teaching and will add various training methods including role play patient actors. UMass Medical School’s simulation lab is already starting to be used for skills that extend beyond sewing and suturing, said Dr. Jennifer Reidy, the school’s chief of palliative care.
Medical students will be required to have conversations with people about breaking difficult news, prognosis and end-of-life planning.
“We’re using it to teach complex communication procedures,” Reidy said. “We want to ensure our newest clinicians are well-situated to practice these skills.”
The changes will be implemented in full by the beginning of next academic year, Reidy said.
Tiffany Chen, a third-year medical student at UMass, said the topic of death is still taboo even in the medical field.
“It’s really hard to talk about death, and it’s hard to conceptualize,” Chen said. “But death is not a failure and there’s always something you can do for a patient. If we can infiltrate the medical field with that mindset, we could do a lot of good.”
The final months of a person’s life are a confusing time for both the person and his or her family. Not only do final preparations have to be made, but the emotional stress of impending loss leaves many overwhelmed as grief makes tough decisions increasingly onerous.
Often, families seek professional help in the form of assisted living centers to alleviate the burden as their loved ones age. But once a patient receives a diagnosis that he most likely has less than six months to live, a new option becomes available: Hospice care.
Lee Read, a case manager with Hospice of the Piedmont, manages more than two dozen hospice patients at the Greenbrier and Hollymead locations of RoseWood Village Assisted Living centers, most of whom have dementia. Her organization, a community-based non-profit headquartered next to Sentara Martha Jefferson Hospital, focuses on end-of-life care for patients living all across Central Virginia. Read’s ultimate responsibility, and the company’s vision statement, is to make sure “nobody dies alone or in pain.”
Lee Read speaks on the phone at the RoseWood Village assisted living home on Greenbrier Drive near the nurses work station. Read’s job involves constant calls with doctors, family members of patients, insurers and other Hospice of the Piedmont staff.
In doing that, she manages the medications, equipment orders, triage care, dietary requirements and everything else her patients need to remain comfortable. She also serves as a liaison for the insurance companies, doctors and family members involved with her ever-changing caseload. While most healthcare professionals develop relationships with their clientele, hospice workers watch almost all of their patients die, making the emotional impact an additional challenge.
“I think over time you develop a thick skin,” Read said. “Otherwise, you could take on so much [emotion] that you become almost debilitated or think that you really can solve all those [health] problems, and [you] can’t.”
Dora Goldberg, 90, poses for a portrait at the RoseWood Village assisted living home on Greenbrier Drive after a game of bingo. Goldberg is one of Lee Read’s patients and suffers from dementia, like many of Read’s patients.
Read has a minimum number of required visits for each patient that is based on Medicare requirements, usually ranging from two to four times a week, during which she tracks each patient’s condition and determines what he or she needs. After six months, a patient can recertify if her condition is still declining and their diagnosis is the same, or she can “graduate” if her condition improves. She also works with a team that includes a social worker, a chaplain, certified nursing assistants and supervisors who specialize in different parts of the care process.Once a week, the team meets at the company headquarters to discuss the status of each patient and figure out what needs to be accomplished in the week ahead. Each meeting also includes a moment of silence, after which a ceremonial marble is dropped in a vase for each patient who has died since the last meeting. While it is marbles this time, each year a new symbolic object is chosen.
For Read, hospice was not her first career path. After graduating from William and Mary with a pre-med degree, she pursued a master’s in divinity from Columbia Theological Seminary in Georgia. She then went on to become a chaplain at the University of Virginia and Westminster-Canterbury of the Blue Ridge retirement home in Charlottesville.
But two events changed her perspective and led her back to health care. Her father received hospice care at the end of his life, and her 4-year-old son was diagnosed with cancer within a short span of time. Her son survived the disease, but the experience inspired her to go to nursing school. She also completed the majority of the requirements for a degree in social work, giving her formal education in nearly every function her team at Hospice of the Piedmont performs.
Lee Read holds a patients arm in the common room of the RoseWood Village assisted living home at Hollymead Town Center.
Her interest in helping people resulted in a career defined by “moving to different spots around the bed” of her patients, training her to fulfill both their spiritual and healthcare needs.
For Jeannie Holden, whose mother, Dora, is one of Read’s patients, hospice care came in a time of need.
“I can look back at the emotional part of that [decision] and how difficult it was. My mother was in the hospital, and she had sepsis, and we really didn’t think she was going to pull through,” Holden said. “Up until that point, I didn’t know that I really had any options.”
But after discovering Hospice of the Piedmont, that process became much easier.
“From the get-go, the care, the resources, the on call, the always being there from the social worker to their chaplain, [they] let me know they were there for me as well as my mother,” Holden said. “I always think that there’s more that I can do and I always have to be available, and they’ve helped me to realize that I am doing enough.”
For those who might be in a similar position, Holden said, it’s important to know the reality of hospice.
Lee Read (right) speaks on the phone at the foot of Juanita Burke’s, 97, bed at the RoseWood Village assisted living home at Hollymead Town Center. Burke, who had little strength left, died several days later.
“It’s not synonymous with death being imminent, [but] that it is certainly an end-of-life process,” Holden said. “Hospice can help you maneuver through and help you on the path to accepting that a loved one is at their end of life, [and] they help to make that quality of end of life good, to the best that they can.”
Even after dealing with death personally, professionally, theologically and medically, though, Read is still puzzled by life’s biggest questions.
“I certainly don’t have all the answers, and I’m not even that comfortable when I’m around people that have all the answers, whether it’s a religion or even a company. I like the questions and I like looking for the answers together,” she said. “It’s not my death; it’s not my journey. I am privileged to walk on the ground of the sacred journey of whoever is dying, but it’s their death.”
The families she works with often ask many of those same questions, to which she usually says, “I don’t know, but we’ll be here.”

 CENSUS
CENSUS unique stories, after which they are marked — tattooed — on a rib, proof that they have been tallied. While the census may sound like an Orwellian device, Ball is more concerned with his characters’ emotional lives than with authoritarian foreboding. The father and son move from region to region, entering strangers’ homes, administering the census. With each new encounter a story from the narrator’s life is revealed. The best of these recall him falling in love with his wife, a renowned clown and performance artist who is also one of the novel’s most dynamic characters. In one lovely scene, prompted by his encounter with two eccentric sisters who conjure the Beales of “Grey Gardens,” the narrator remembers a performance in which giant pieces of silverware, a knife and fork, hovered overhead as his wife and other clowns evaded them. In a novel that ruminates so heavily on death, such memories provide a celebratory sense of joy.
unique stories, after which they are marked — tattooed — on a rib, proof that they have been tallied. While the census may sound like an Orwellian device, Ball is more concerned with his characters’ emotional lives than with authoritarian foreboding. The father and son move from region to region, entering strangers’ homes, administering the census. With each new encounter a story from the narrator’s life is revealed. The best of these recall him falling in love with his wife, a renowned clown and performance artist who is also one of the novel’s most dynamic characters. In one lovely scene, prompted by his encounter with two eccentric sisters who conjure the Beales of “Grey Gardens,” the narrator remembers a performance in which giant pieces of silverware, a knife and fork, hovered overhead as his wife and other clowns evaded them. In a novel that ruminates so heavily on death, such memories provide a celebratory sense of joy.