It’s not quite the peaceful drifting off I’d imagined for my dad.
By Harriet Brown
At age 86, my father had survived both colon cancer and a stroke that left him with aphasia. His mind was sharp, though, and he wasn’t depressed. A crack bridge player with a passion for Italian restaurants, he was popular at his assisted living facility even though he couldn’t speak much. He told me he’d lived a good life and wasn’t afraid of dying, and he didn’t want to go through any more medical trauma. No chemo, no radiation, no surgeries, no treatment.
His advance directive read DNR and DNI — do not resuscitate, do not intubate. No one would break his ribs doing CPR or make bruises bloom along his arms trying to find a vein. As his health-care proxy, I was completely on board. I’d read Sherwin Nuland’s “How We Die,” Atul Gawande’s “Being Mortal,” Elisabeth Kubler-Ross’s “On Death and Dying.” Comfort would be the priority and any pain would be “managed,” which I assumed meant erased.
Up to 80 percent of Americans die in hospitals or nursing homes, and a third spend at least 10 days in an intensive care unit before they die, many of them comatose or on a ventilator. A week after his sudden diagnosis of widespread metastatic disease, my father was lucky enough to get a bed in our town’s only hospice, a homey facility staffed with attentive and experienced caregivers. The alternative would have been a hospital bed in my living room, so it was a relief to know that my father was in the hands of professionals. They would know what to do.
And they did. The nurses and caregivers were gentle as they repositioned my father in bed, explaining each move even when it seemed he couldn’t hear or follow. When he could no longer swallow they squirted morphine into his cheek and rubbed it so the medicine would be absorbed. “This will make you feel better,” they would say, and my father would turn his head and open his chapped lips like a baby bird.
But his death was not the peaceful drifting away I’d always imagined, where you floated into a calm, morphine-induced sleep, your breath came slower and slower and then simply stopped. He vomited blood over and over. A lifelong stoic who never complained of pain — even when he’d broken a hip the year before — he twitched restlessly in bed, eyes closed, his brow furrowed and his skin clammy.
The magical “managing” of pain and nausea I’d anticipated turned out to be more aspirational than real. The hospice nurse prescribed one anti-nausea medication, then another, without success. Eventually, Ativan and Haldol settled the nausea, and morphine helped the pain. My father was lucky it helped; about 25 percent of people die in pain. One caregiver confided to me, “There are people whose pain we never get under control.”
For days we watched my father’s cheeks hollow, watched him pluck at the thin blanket that was all he could bear on his body. His kind brown eyes glazed over, and some trick of the light made them look blue under his half-closed lids. Sometimes he sat up suddenly, reaching forward, and then fell back on the pillows. I knew there was a name for this behavior, terminal restlessness, that it’s common during the dying process. I knew the gurgling sounds he made as he breathed came from his body’s inability to clear secretions, and that — according to hospice — it probably wasn’t uncomfortable for him.
Leaving the hospice facility one night, I told my 81-year-old aunt that I wished I had the nerve to put a pillow over his face. “I’ll stand guard at the door while you do,” she replied. Dying is hard work. And it’s hard to watch.
On the last night, I sat with my father until the summer sky began to darken. Then I gathered my belongings and leaned over the bed where he lay unresponsive, his eyes closed, his mouth half-open. I kissed his stubbled cheek. “Dad, I’m going now,” I told him. “It’s time for you to go too.” He died a few hours later. He was alone, as most people are when they die, so I don’t know if it was peaceful, if he made a sound or opened his eyes or just stopped breathing.
After he died, I was haunted by scenes of his suffering. I remembered looking out a hospital window nearly 30 years earlier with my newborn daughter in my arms, realizing that every one of the people I saw on the street had been born. For every person walking down Seventh Avenue, a woman had borne pain that tore her body open. It was a horrifying thought.
Drugs help with the pain of childbirth, but they can’t take it away completely. It’s the same with dying.
“Suffering is an ineradicable part of life, [like] fate and death,” wrote psychologist Viktor E. Frankl in his bestseller “Man’s Search for Meaning.” He was something of an expert, having survived nearly three years in a variety of Nazi camps.
Of course, my father’s suffering was nothing like the kind Frankl witnessed. But still, death, like birth, is a creaturely process, a force that wrenches us onward without consulting our preferences or respecting our sensibilities.
In the weeks after my father’s death, I began to understand in a deeper way the meaning of a good death. No drugs took away all my father’s physical pain and nausea. But in the care he was given, the morphine, the quiet words, the repositioning and cool cloths on his forehead, his suffering was addressed even if it couldn’t be “managed.”
And that, I think, is what we all want. Not just freedom from beeping machines and needles and the cold lighting of an ICU, though that matters, too. Not just the absence of pain, which isn’t possible for everyone. But the solace of being seen and heard and acknowledged brings comfort even in the face of deep suffering.
I hope it’s something we can remember as we move toward a society where more of us can have a truly good death.
Two brothers are combining palliative care expertise, linguistics and AI to encourage more effective conversations between doctors and people receiving end-of-life care.
Hospitals track infection rates, bed occupancy and many other measures. Why not good conversations, too?
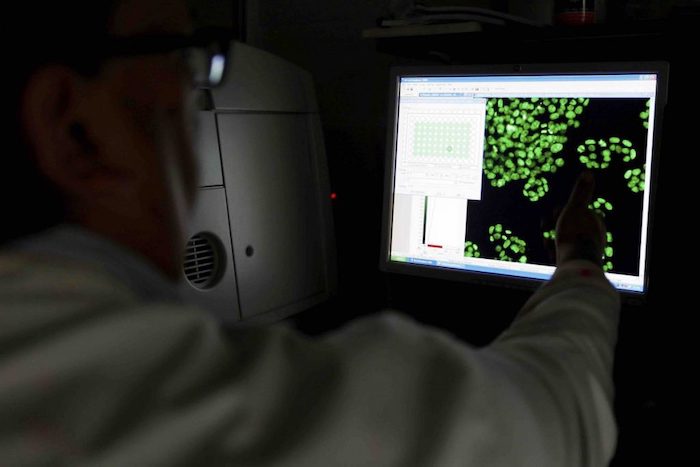
One afternoon in the summer of 2018, Bob Gramling dropped by the small suite that serves as his lab in the basement of the University of Vermont’s medical school. There, in a grey lounge chair, an undergrad research assistant named Brigitte Durieux was doing her summer job, earphones plugged into a laptop. Everything normal, thought Bob.
Then he saw her tears.
Bob doesn’t baulk at tears. As a palliative care doctor, he has been at thousands of bedsides and had thousands of conversations, often wrenchingly difficult ones, about dying. But in 2007, when his father was dying of Alzheimer’s, Bob was struck by his own sensitivity to every word choice of the doctors and nurses, even though he was medically trained.
“If we [doctors] are feeling that vulnerable, and we theoretically have access to all the information we would want, it was a reminder to me of how vulnerable people without those types of resources are,” he says.
He began to do research into how dying patients, family members and doctors talk in these moments about the end of treatment, pain management and imminent death. Six years later, he received over $1 million from the American Cancer Society to undertake what became the most extensive study of palliative care conversations in the US.
The resulting database contains over 12,000 minutes and 1.2 million words of conversation involving 231 patients. This is the basis of the Vermont Conversation Lab, which Bob created to analyse this data and find features of those conversations that make patients and family members feel heard and understood.
Brigitte’s job in the lab that summer was simple: listen to moments of silence and categorise them. The idea was that they could indicate emotionally charged connections between doctor and patient. Once the silences were coded, they would be used to train a machine-learning algorithm to detect them automatically – and, with them, moments of emotional connection.
You might ask what place algorithms could possibly have in this sensitive realm. The reality is that healthcare communication needs help, especially in palliative care, where practitioners seek to bring patients to their deaths as meaningfully and painlessly as possible.
In 2014, the US Institute of Medicine made improving doctor-patient communication a priority in its landmark study, ‘Dying in America’. An analogous publication in the UK, Ambitions for Palliative and End of Life Care, emphasised the need for patients, family and caregivers to have “the opportunity for honest, sensitive and well-informed conversations about dying, death and bereavement”. It reiterated that doctors need to make those conversations possible.
Most of the resulting communications training seems to offer scripts and templates to help doctors deliver bad news and make decisions with patients. But this is not enough. In this context, doctors really need to understand conversations more broadly. They need to appreciate everyone’s role in a conversation. They need to learn the ability to listen and be silent. They need to confidently recover from conversational missteps.
“Oncologists are in general very uncomfortable with this kind of thing. They want to focus on treatment, and they talk eloquently about different protocols and clinical trials,” says Wen-Ying Sylvia Chou, a programme director in the Behavioral Research Program at the US National Cancer Institute. She oversees funding on patient-doctor communication at the end of life. “But sitting in the place of being a listener is not something that clinicians are trained for or necessarily comfortable doing.”
End-of-life medical conversations also often involve language in extremis.
Enter Bob Gramling. Hospitals track infection rates, bed occupancy and many other measures. Why not good conversations, too?
Amiable and serene, wearing a bracelet of Buddhist meditation beads, Bob sees a big role for artificial intelligence (AI) that can detect and measure the features of clinical interactions that matter to patients, then report those measurements to numbers-oriented healthcare systems.
Once such technology is widely available, he says, “we can incentivise our hospitals to build systems to improve those interactions and reward doctors for doing it”.
§
“How are you?” asks the nurse practitioner, who’s just come into the patient’s room.
“Fine,” the patient says. She’s a 55-year-old white woman with stage 4 breast cancer. Neither she nor the nurse practitioner know that she’ll be dead in five days.
“No, you’re not,” the nurse practitioner retorts.
“Oh, a loaded question,” the patient laughs.
“It’s been a long – well? No,” says her spouse.
“No,” says the patient. “It’s a polite question, it’s a polite answer.”
This is a snippet of a conversation in Bob’s database that he played to his brother David, a linguistics professor at the University of Arizona. David recognised the dynamics of this specific moment. The people in that room hadn’t been talking about care or disease, but they had been doing something important in the conversation that would affect the quality of the care.
When the Gramlings’ father died, David flew home from a literature studies fellowship in Berlin. But years earlier, he’d been intimately involved as a caregiver, witnessing a “smörgåsbord of insane, irrational communication failures” with lawyers, nurses, nutritionists and priests.
For a year after their father’s death, the brothers were swallowed by family matters. As they emerged, they began talking about palliative care communication and linguistic research in healthcare settings, and began to collaborate professionally.
The most recent result is a book, Palliative Care Conversations, published in early 2019. It aims to show physicians how conversations work, such as how clinicians and patients often understand words and phrases differently. David looked at the conversations at a granular level, using the tools of a linguistic subfield called conversation analysis. He spent years listening to audio recordings of the conversations, noting moments worth closer analysis.
Meanwhile, Bob provided clinical details about medical culture. In the last few years, he has also hung out with jazz musicians, who are master communicators when they’re improvising, and visited the Stanford Literary Lab to see how digital tools can be applied to massive literary corpuses to understand patterns too diffuse for human readers to catch.
Research on end-of-life communicating and decision-making typically looks at what doctors or nurses say. It rarely takes into account the deeper linguistic and cognitive factors that influence patients’ abilities to communicate in the first place.
As the Gramlings note in the book, the above back-and-forth between patient, spouse and nurse practitioner is remarkable for a first exchange between strangers. They explain that’s because “the clinician is willing to risk conventional rapport-building pathways by contradicting the family member’s self-reported state of mind”. In other words, the physician has opened the door to a looser mode of relating – and it works.
Another conversation doesn’t go as well. It’s a “pragmatic failure”, as David would say.
“When I came in,” says the nurse practitioner, “I saw you were watching Scrubs.”
“Scrubs?” the patient says. He’s a 63-year-old black man with stage 4 kidney cancer, who will live for 135 more days.
“Have you ever seen Scrubs?” asks the nurse practitioner, who is white.
“Yeah,” the patient says. “No, I wasn’t watching Scrubs.”
As the exchange unfurls, it’s clear the patient and clinician won’t connect. The clinician then seems to want to force their way to the task at hand, and forget the small talk where rapport could be built.
“When you study communication in healthcare, you’ll see a lot of monologues from doctors,” Bob says. “I don’t mean that in an insulting way – it could be really good information.” In palliative care, he explains, conversations are different: “It might be just because it’s the nature of palliative care. It’s what we do and what our value is… there is a lot of turn-taking.” That’s another term he learned from his brother. It refers to the back-and-forth of conversation.
“This is not a clean, rational, logical experience that fits on an 8-and-a-half-by-11 piece of paper, it’s a human-engaged relational endeavour,” he adds. “If we’re going to develop metrics for that, we’d better be looking at both the beauty and the science from many angles.”
Research on end-of-life communicating and decision-making typically looks at what doctors or nurses say. It rarely takes into account the deeper linguistic and cognitive factors that influence patients’ abilities to communicate in the first place.
One study, by speech-language pathologists in the late 1990s, showed just how large these language challenges can be. They gave a battery of language comprehension and memory tests to 12 hospice patients: 11 of them couldn’t recall words, had difficulty understanding things and pronouncing words, and had difficulty remembering what was said to them. These symptoms get in the way of normal activities, like having conversations.
Even something as crucial as how well older patients can hear gets overlooked. In a 2016 survey of 510 hospice and palliative care providers across the US, 87% of them said they did not screen for hearing loss, even though 91% of them agreed that patients’ hearing loss impedes conversation and negatively affects the quality of the care they receive. Only 61% said they felt confident nonetheless that they could deal with patients with hearing problems.
The Gramlings pay a remarkable amount of attention to another factor: the pain, shortness of breath, fatigue and medications that can keep patients from communicating normally.
In his research, David has addressed what he calls “language in extremis”: what happens when people’s ideas about language and communication buckle under the strain of circumstances, as in multilingual experiences in Nazi concentration camps, or interpreting in border patrol detention facilities.
End-of-life medical conversations also often involve language in extremis. As cancer brings a person’s life near to its end, they may have lost some of their lifelong communicative powers to the disease or its treatments. They may have less ability to speak subtly and indirectly, which is important for politeness. Shallow breathing shortens utterances, and drugs may block word-finding. All of this reinforces an asymmetry in communication that doctors don’t always grasp.
At the end of a patient’s life, there may not be effective medical treatments, just things to discuss and plans to make.
A physician might encourage a patient to speak openly, and indicate their willingness to listen, but in practical terms, “That gesture doesn’t quite work,” David says, and doctors need to understand why.
At the same time, people still hew to lifelong social conventions about being a user of their language. They might be dying, but “They don’t back away from their interactional responsibilities,” David says. They honour turn-taking; they don’t interrupt. They tell jokes, they use family language, and they create mini-rituals of inclusion and exclusion, often to deal with the communication asymmetries.
“If I were picturing the developmental arc,” says David, “it wouldn’t be coasting down into death. It would be all the way and sometimes heightened. The kind of complex literacy you need to use in a hospital setting in a serious illness, and managing all your oncological terms – it’s almost like the competencies themselves get expanded in this end of life.”
§
In his lab, Bob is examining even more fleeting aspects of conversations, such as pauses. It’s an interesting choice, because pauses might be considered as a sign that a speaker has lost their way or that an interaction is breaking down. On the other hand, pauses are easy to locate in the acoustic signals of recorded conversations. And they might indicate where someone is listening or about to say something important, so they might be a good thing.
Bob’s team used machine learning to identify pauses of 2 seconds or longer in spoken conversations, then human coders like Brigitte Durieux tried to categorise them, looking for ones that were more than just silence.
Because they didn’t have access to what the doctors or patients were actually thinking, they looked for the presence of emotional words and other sounds like sighs or crying on either side of the pause. Did a question about the quality of life, treatment hopes, prognosis or dying precede the pause? If so, the pause may have been because the doctor invited the patient to consider something.
The team found that during some of these pauses, some connection, shift or transformation was occurring. These “connectional silences” were rare. Out of a set of 1,000 clips with pauses, a mere 32 were connectional in nature. They were brief, as well, most lasting less than four seconds. But there’s still power in them.
The dynamics of a conversation change dramatically after such a connectional silence. Suddenly, a patient will be talking more than they did earlier. They’ll be directing the conversation, not the doctor. It’s as if the mutual agreement to pause for two seconds spilled into an agreement to shift roles.
“No, for some reason I guess I just in my head was gonna be on [chemotherapy] for the rest of my life and everything was gonna be hunky dory and…” a patient begins.
A 2.9-second connectional silence follows. The doctor inhales audibly, to signal they will respond, which makes the patient pick back up.
“You know. I knew early on, I mean you told me early on it’s not like and then this will be the rest of my life. Something, you know, might go down.”
The doctor responds. “Something. That can be a very hard thing to think about. That here we found something that’s helping but you can’t stay on it for the rest of your life.”
In other moments, the silence comes after a doctor has said something empathetic.
“It’s rare of me to tell somebody point-blank you’ve got to stop. However, I will say you have my permission to set limits,” the doctor says.
“Okay,” says the patient, then falls silent for nearly seven seconds.
His wife chuckles. “He can’t stand the thought of it. I can tell by his laugh,” then she laughs.
“I know he can’t stand the thought of it,” the doctor says.
“No, that’s okay,” the patient says. “I’ll get used to it.”
Or in another instance, the doctor tells a patient’s spouse, “what you feel is really hard. It’s really hard.” There’s a 2.8-second silence.
“I just wish he had a better quality of life.”
“I know, I know,” says the doctor.
Even though these connectional silences don’t happen often, Bob thinks they’re good linguistic markers of connection exactly because doctors don’t commonly use them. When someone good at monologuing and interrupting falls silent, it may mean they’re allowing something else to happen.
Bob surmises, “More often than not, the conversations that have a lot of space in them are probably going to lead to people feeling more heard and understood.”
§
Judy had a question. Having come to the hospital at the University of Vermont to recover from the flu, this elegant, 83-year-old woman was lying in her bed. Two doctors had come to her room bearing news. It was cancer, not the flu, and it had spread from her liver. She could undertake a course of chemo, or she could have her pain managed as she died.
She turned to her daughter, Kate, sitting beside her. “What should I do?” she asked.
When the doctors had requested this meeting, Kate had dropped everything to be there. It seemed unusually serious. Now she knew why. She wondered why she hadn’t seen the signs of her mother’s cancer. Judy’s skin had started to look yellow, she recalled. But instead of recommending a check-up, she bought her mother some pinker make-up.
In this pivotal conversation, the doctors presented the options but also wanted to know what was important to Judy. They knitted the science together with thoughtfulness and compassion. Kate was struck by their slow, almost languid approach to delivering the news.
Slowly it dawned on her that this was a conversation about her mother’s death. Neither of them had prepared for this. Not now, not so soon.
“It had the nature of a conversation with a clergyperson rather than a doctor,” she remembers. Pastoral kept coming to mind.
At the end of the conversation, one of the doctors gave her his card. It was Bob Gramling. Kate has since seen the bright blue spectrographs showing gaps in conversation – where the pauses occur. She thinks these are important moments as well.
“Where there’s silence, where there are gaps, that’s where the caring shows up,” she says. “I think it’s incredible work to point out to doctors there’s a lot going on in the silences.”
Bob and David have only scratched the surface of how these conversations work. So far they have only studied English speakers, for example; pauses work differently in other cultures, so they need data on those moments, too. And because their data comes from people with cancer, there’s a concern that the analysis may be skewed.
With cancer, says Wen-Ying Sylvia Chou of the National Cancer Institute, most patients have time: “They continue to be themselves and continue to be part of the conversation and any ongoing discussion.” With other diseases, though, there could be more risk that the person would “lose cognitive function or physical function”. In those cases, she says, conversations “would look very different”.
Healthcare’s use of natural language processing – technologies that treat language as data – is expanding, and the chances are good that research like that of the Gramlings will expand to cover conversations with people who have other serious illnesses.
What is a conversation?
Bob isn’t the only researcher exploring the use of artificial intelligence in palliative care. In 2017, James Tulsky, a palliative care physician at Dana-Farber Cancer Institute in Boston and a Harvard professor who studies health communication, stressed that “mass-scale, high-quality automated coding will be required” to give feedback that helps clinicians improve their expressions of empathy.
Tulsky turned to Panayiotis Georgiou, a computer engineer at the University of Southern California, to develop automated detection of emotional connections between doctors and patients. In 2017, a team headed by Georgiou showed that certain acoustic features of the speech of couples in counselling could be used to predict marital outcomes. What if algorithms could do the same for palliative care conversations?
“The technology in theory exists out there to do all this,” Tulsky says. “It’s just a matter of doing enough research, running enough iterative trials, training up the machines to actually get these algorithms trained well enough so you could apply them to more random talk.”
I ask Judy’s daughter Kate what she thinks of using artificial intelligence to enrich human connections. “I wouldn’t worry about the technology,” she says. “The more technology, the more sacred the conversation becomes.”
What does she mean? Anything that enables humans to use their voices more effectively with each other is a good thing, she explains: “It’s because of the increasing technology that the interaction becomes more wonderful.”
§
What is a conversation? It’s a setting where humans interact, often for a purpose but sometimes for none at all. People have to learn how to have conversations but when they become expert in their culture’s conventions, conversing becomes so automatic it feels natural.
Modern healthcare has hijacked conversation and made it a tool by which physicians can achieve their ends.
According to David, “The contemporary hospital still understands ‘conversation’ as ‘making a pre-determined X happen through conversation’.” This is a barrier in serious illness and end-of-life care, where the conversations need to be venues for figuring out what the X might be.
At the end of a patient’s life, there may not be effective medical treatments, just things to discuss and plans to make. This may need a more natural conversation than a medical one, a conversation in which none of the participants may know what the outcome will be.
After all, these conversations aren’t just for doctors; they’re for patients, too. And family members, nursing aides, housekeeping staff. “There are a lot of human beings who have a vested interest in this other human,” Bob says.
There are critics who don’t think artificial intelligence and machine learning have a role to play in palliative care. Bob’s view is that shying away from analysing this kind of conversation in this way means that essential opportunities for improving it will be missed.
“It is helpful, as a discipline that has historically thought of communication as just the art of medicine, to actually think that, no, this is a science,” he says. And understanding that science could help us re-engineer the healthcare system to support more meaningful conversations.
He’s aware of the delicacy in institutionalising and commodifying a human interaction, though. “As a physician,” he says, “I was afraid of being a researcher that was going to oversimplify this kind of sacred experience into something that’s measurable and convenient and essentially meaningless.”
That’s where Brigitte Durieux struggled with her feelings as she listened to thousands of audio clips of pauses. In some conversations, people were laughing, but she was struck by the loneliness in others. She had begun to recognise patients’ voices and wondered what had happened to them.
“Nobody is perfect, but there are times when one realises there’s something that could be said to make this feel less like a loss,” she says. Sometimes she whispered under her breath something the doctors could have offered instead.
After Bob found Brigitte crying, he wrote an ethics proposal to the hospital so that he could introduce a new procedure into his lab. He borrowed an idea from the hospital’s palliative care unit, where staff gather every week to say the names of people who have died, then ring a singing bowl.
Now, at the start of every Vermont Conversation Lab meeting, a researcher reads the name of one of the patients from the database and rings the bowl. So far, they have gone through the list of names twice.
The ceremony helps, says Brigitte, because it reduces the guilt of turning a sensitive moment in someone’s life into a piece of data.
“What it does ultimately,” she says, “is recognise the humanity of things.”
After helping a girlfriend through the messy, tangled finances left in the wake of a parent’s death, John Kerecz had a message for his own mom and dad: Get your paperwork in order.
A few years later, Kerecz’s father passed away unexpectedly. The 52-year-old environmental engineer from Harrisburg, Pennsylvania went to the house and looked where his father and mother used to keep their important documents, but nothing was there. It was pure luck that he went to the computer to look up a phone number and saw a folder on the desktop labeled “DEATH.”
“Sure enough, everything was there in that folder,” Kerecz says.
Armed with a copy of the will, lists of the financial accounts and insurance policies and other paperwork, Kerecz was quickly able to settle his father’s estate and use the funds to take care of his ailing mother, making him extremely grateful.
The difference between having your files organized or not is about more than just stress; leave behind a mess and it can delay inheritors’ access to funds and cost a bundle in legal fees.
“It could be six months or longer if you don’t have the paperwork in order, and … your family is in the dark, not knowing things, jumping through hoops. It’s not a fun existence,” says Howard Krooks, past president of the National Academy of Elder Law Attorneys.
Taking care of the necessary documents is a hallmark of good parenting, he adds, rather bluntly: “More than any kind of monetary legacy, if you really love them, you’d do this.”
HOW TO GET IT DONE
Compile a list of the financial information your heirs will need upon your death: wills, trust information, investment accounts, legal contacts, etc. You can keep this information in an electronic file – in one master document or several attachments – to serve as a road map to find all the physical paperwork.
Or, you can do what some of elder law attorney David Cutner’s clients do, and just pull out a cardboard box and start piling up the papers.
You have to do more than just gather the information, though, cautions Cutner, co-founder of the Lamson & Cutner Elder Law firm in New York. You have to tell your loved ones you have done it and tell them where to find it. You can either hand over the file immediately or keep it in a safe place (away from the prying eyes of caregivers and potential scammers).
A safe deposit box, by the way, is not a good place to keep these papers, says Cutner, because it’s too hard to access when needed.
THE WILL
Top of the list is a copy of your will, hopefully the most recent version, plus contact details for the attorney who drew it up and any executor named. Also important are trust documents, if they exist, estate experts say.
While power of attorney and living will documents are crucial should you become incapacitated, they will not be useful after your death, says Krooks – your heirs will then be using a death certificate to obtain access to accounts.
The real power in assembling all these items is that it forces you to go through the process of specifying your wishes. Without them, your family would have to put your estate into probate, which is when the state determines the distribution of your assets. This can take up to a year and eat up about 5 percent of the estate, says John Sweeney, an executive vice president responsible for Fidelity’s planning and advisory services business.
FINANCIAL ACCOUNTS
Your heirs will need to know all of your account information, down to your utility bills and your tax returns. You can either create a list or include copies of statements in the file, or just directions to where to find them. Also useful is a list of relatives to contact.
Knowing passwords for online accounts is not as important as naming another person on key accounts ahead of time, says Sweeney. This way, if the family needs to make mortgage payments or pay any medical bills, they do not have to wait until the estate is settled.
“Children are often dipping into their own assets to pay for taxes and mortgages when the last surviving parent has passed away,” says Sweeney.
In that same vein, make sure to sign another person up for a key to any safe deposit boxes or home safes, says Krooks. Include clear directions on how to access any other valuables that may be stashed elsewhere, so that it’s not mistakenly thrown out.
SURVIVOR BENEFITS
Pensions and insurance plans have many different payout rules, so you need to leave behind detailed information about policies. Insurance information should extend beyond life insurance to car, home and boat insurance, says Sweeney. It is also critical to include your Social Security benefit information, he adds.
The job of assembling all of this information can be massive, but most people appreciate it in the end.
“At first they curse us out because it’s so much to gather and put in one place. But by the time they come into the office, they’re really glad they did this exercise,” Krooks says.
My father passed away from cancer six weeks ago. The days after his death were characterized by the expected: disbelief, morbid Hallmark cards extending condolences, and dishes of limp lasagna left at the door. But the period following his passing was also colored by the unexpected.
I wasn’t expecting panic or anxiety. Nor was I expecting derailing flashbacks to the last week in the hospital, night after night of insomnia, or the decimation of my formerly robust immune system. In short, I wasn’t expecting grief.
Theoretically, I knew grief happened after a significant loss. I’d just somehow made it to 34 years of age without ever really experiencing it firsthand. In essence, grief is a common emotional response to a distressing situation. But although it’s normal, it can be utterly annihilating. Grief gathers up feelings and experiences—that are challenging enough to deal with on their own—into one giant, messy package that spills out over everything.
A Small Piece of Cannabis-Infused Fudge
Deep down, I knew the grief and pain I was experiencing was something I had to work through. “The cure for the pain is in the pain,” says the poet Rumi. I wasn’t looking for benzodiazepines, antidepressants, or anti-anxiety meds to numb the feelings. But I did feel like I’d benefit from something that would allow me to elevate myself from the depths of the grief swamp, make sense of it, and muddle through the funeral and weeks that followed.
I found it in my refrigerator. One small piece of cannabis-infused fudge forged a small window of space in my head, allowing me to observe what was going on both inside and outside. A sense of peace descended, and I slept four hours that night.
Any grief-stricken person will tell you that grief can place you at the behest of your emotions, causing you to swing wildly between panic, sadness, regret, and anger. Compound this with sleep deprivation, and your ability to reflect and retain a sense of perspective is severely compromised. Ironically, a functioning reflective faculty is one of the things a grieving person misses most.
During the week leading up to the funeral and for a few days after, nuggets of fudge provided not an escape, but elevated respite. Throughout the constant coming-and-going of family, friends, funeral directors, and total randoms who stayed lingering long after they’d worn out their welcome, cannabis was my grief aid, helping me find presence in the moment. Those little nibbles of fudge enabled me to appraise the more challenging events with a sense of equilibrium and calm.
Openness to Insight and Meaning
Mickey Nulf, a cannabis educator and patient consultant, leaned into cannabis after he lost his mother to a drug overdose. For Nulf, cannabis helped him to confront his grief in a healthy way.
“Cannabis kept my mind level as I was being rushed with emotions from the feelings of grief and sadness that I had. It allowed me to feel the feelings, but understand them at the same time,” explains Nulf. “It kept my anxiety down while the grief hit, and encouraged me to actually deal with the grief instead of just burying it.”
Grief is often tinged with moments of profound insight and meaning, and openness to these moments can make testing times easier to weather. Nulf recalls the most impactful moment he experienced was seeing his mom lying in the funeral home. “I hadn’t cried before then but cannabis allowed me to experience those feelings again. I dropped to my knees and cried for my mom. I was sad she was gone; sad that I didn’t get the chance to say ‘I love you,’” he reflects.
Nulf believes cannabis enabled him to access his feelings fully, which was essential to making sense of his mother’s death. “I was able to process the loss, and understand that the picture was greater than the loss,” he recalls. “I could see the tragedy but find happiness through it. It was a first for me in my lifetime.”
An Expert’s Opinion
But what do the experts think? While there are no clinical studies exploring cannabis use and grief, there is plenty of interest. “Currently, there is promising preliminary evidence about the efficacy of medical cannabis in the treatment of these conditions, all of which are hallmark features that characterize the constellation of grief symptoms,” observes Dr. Rahul Khare, MD, an expert on the medical applications of cannabis.
Large-scale clinical trials, however, are needed to draw firmer conclusions. It’s also vital to acknowledge that studies indicate that a grieving individual is more vulnerable to substance abuse, dependency, and addiction. A recent study also suggests that cannabis use among individuals with depression can be problematic and prevent them from seeking proper psychiatric care. Cannabis may straddle a fine line between helpful aid and problematic crutch.
Dr. Khare suggests that the key may be to combine cannabis with appropriate mental healthcare. “Although it is controversial, the current evidence suggests an overall promising relationship in the treatment of grief with medical cannabis, if such treatment is paired with proper psychiatric and mental healthcare by licensed professionals,” he reflects.
Khare is optimistic that cannabis could represent a powerful tool for helping with grief in the future. “In my personal experience treating patients with medical cannabis, I have found a marked decrease in the use of antidepressant medication as well as a reduction in opioid and benzodiazepine use as well,” he states. “I believe with further research, a more definitive link between the efficacious uses of cannabis for grief will be unveiled.”
Since he watched his mother collapse and die, Richard Bridgman’s fear of death has left him emotionally paralyzed.
It was right around Thanksgiving—nearly 45 years ago—and Bridgman was sleeping overnight on his mom’s living room couch.
“In the middle of the night, she walked into the room and said, ‘Richard, I’m dying,’” recalls Bridgman, who tried to reassure his mom that she’d be OK. But his mother, who had a heart condition, was suffering a massive heart attack. “She looked at me and fell over on her head. I didn’t know what to do. She was dead.”
Death haunted much of Bridgman’s early years. His stepfather died when Bridgman was 15. His father, an alcoholic, died when Bridgman was 17. And Bridgman was 26 when his mom died before his eyes. Now, 72, and long retired from the bill collection business he once owned in the Springfield, Illinois, area, he has spent most of his adult years trying to cope with—if not overcome—his immense fear of death.
“Death became an obsession,” he said. “No matter where I went or what I did, death was always in the back of my mind.”
Most people prefer not to think about death, much less plan for it. In a tech-crazed world, where communication is broken into 140 characters and six-second sound bites, our connection with each other is dissected into so many bite-sized morsels that discussion of death would seem an unwieldy topic of conversation.
“Everybody has a fear of death, no matter what culture, religion, or country they come from,” said Kelvin Chin, author of “Overcoming the Fear of Death,” and founder of the Overcoming the Fear of Death Foundation and the nonprofit turningwithin.org. “Fear is simply an emotion caused by the anticipation of unhappiness.”
But wait. What if death isn’t actually unhappy? What if it simply—is? For Bridgman, whose fear of death was overwhelming, that simple question was a critical step in learning to deal with death. That question was posed to him by Chin, whom he discovered via a Google search. Several supportive phone consultations with Chin—combined with a simple meditation process that Chin teaches—have helped to keep Bridgman’s fears under control.
“I spent so much money on psychiatrists and psychotherapists—none of them did any good,” says Bridgman. But Chin steered Bridgman toward meditation. “Meditation is better than medicine,” Bridgman said.
Everyone must figure out their own way to handle the fear of death. One expert, who overcame her own fear through years of attending to the dying, says death is rarely the terrible thing that most folks fret about.
“Death is usually a peaceful process,” explains Donna Authers, a professional caregiver, motivational speaker, and author of the book “A Sacred Walk: Dispelling the Fear of Death and Caring for the Dying.”
“Very few people die screaming. They just go to sleep.”
But it took Authers years to learn the lesson that death need not be frightening. As a child, death haunted her. When she was 2 years old, her father was killed in World War II. Her mother, who had remarried, died on Authers’ fifth birthday. “Instead of a birthday party, I woke up to the worst day of my life,” she said. Her grandfather committed suicide when Authers was 15.
It was Authers’s grandmother—while dying from cancer—who taught her the most critical lesson in accepting death’s inevitability. Authers brought her grandmother home to tend to her during her final days, but her grandmother could sense her granddaughter’s terrible fear.
That’s when her grandmother took her by the hand and, unafraid, reminded Authers, “Death is part of life. You, too, will be where I am someday, and you can’t face death with fear,” she said. That changed everything. Seeing her grandmother bravely face death caused her own fears to dissolve.
“I was no longer afraid of death and dying,” Authers recalls.
Authers ultimately left her job as an IBM marketing executive to become a caregiver. Through the years, she has found that faith is the most important quality among those who face death without fear. “People who have faith in something don’t grieve like those who have no hope,” said Authers.
Increasingly, however, Chin has found that millennials—more than any other demographic—fear death the most.
“It’s the downside of social media,” said Chin. “The bombardment and speed of communication lead to an overload that can trigger a fear of death.”
Perhaps even the world of politics can play a role, suggests Sheldon Solomon, professor of psychology at Skidmore College and author of “The Worm at the Core: On the Role of Death in Life.”
In times of political upheaval—particularly when people are reminded of their mortality—the fear of death increases, even as they tend to be attracted to political figures who promise them more security, said Solomon, who has conducted numerous experiments on this issue.
“When people are reminded of their own mortality, in an effort to bolster faith in their own view of reality, they become more hostile to anyone who is different.”
Even then, says Solomon, perhaps nothing alleviates a dying person’s fear of death more than love.
A terminally ill grandmother he knew was distraught at the prospect of death. No doctor and no medicine could help her. Then, she received a short phone call from her granddaughter, begging her for her cupcake recipe. “No one can make them like you,” her granddaughter said.
“That call did more in five minutes than anything else could have,’” says Solomon. “It reminded the grandmother that she will live on in the memories of the people she loves. That was all she needed to know.”
Michael Micallef had lived with Huntington’s disease for nearly three decades. In July, he chose to die by medically assisted death in the backyard of a close friend in Toronto.
As Michael Micallef’s body began to fail, a thought persisted in his mind — he didn’t want to die slowly, the way his father had.
For nearly three decades, the Toronto man had been living with Huntington’s disease. The hereditary, neurodegenerative illness had taken Micallef’s father about a decade before, and now, it was taking him.
As it progressed, his motor skills, speech, ability to read, and even Micallef’s ability to sleep were all faltering.
“He said he really [regretted] he didn’t have the courage to kill himself,” he said of his father.
That’s one of the reasons why on July 7, at the age of 69, the Toronto man and his wife, Vickie, held a party to celebrate his life before Micallef’s medically assisted death later that evening.
Surrounded by his closest friends and his wife of 48 years, Micallef got to say goodbye on his own terms during a party at his condo building.
Alongside dozens of guests, he enjoyed some of his favourite food — cinnamon buns, mangoes, and Whole Foods rotisserie chicken.
“This can be good for everybody. Not the result, but the process,” Micallef said. “Being able to have choices is extremely important to me. Not to others, but it is to me.”
According to the Office of the Chief Coroner, there were 1,593 medically assisted deaths in Ontario between June 30, 2018, and June 30, 2019.
Since the procedure was legalized in 2016, there have been more than 3,300 medically assisted deaths in the province, statistics show. The coroner’s office says that in Ontario, roughly 1.5 per cent of all deaths are now medically assisted.
It’s something Micallef considered ever since his diagnosis, nearly 30 years ago — but it wasn’t truly a possibility until the procedure became legal.
For Micallef and his wife, his decision to die wasn’t a cause for sorrow. His party was a celebration — of life, love, and memories made. There was a steady parade of hugs from well-wishers, along with hopes for an easy passage.
His brother, sister and cousins came. Friends surrounded Micallef to wish him well.
“I said to him, ‘Do you realize how lovely this is? Michael we are going to have a farewell party … when you go to wherever the next stage is, you’re going to know how people feel about you,'” Vickie said.
“This is a blessing.”
‘Little explosions’ in his brain
Micallef attended St. Michael’s College School through his teen years, where a voracious love of reading took hold, alongside a passion for competitive hockey.
Later in life, his job with furniture company Herman Miller had taken both him and his wife to England, Singapore and Michigan, before landing back in Toronto.
The pair did not have children. They had a large group of friends, extended family and associates all over the world.
In Micallef’s last days, he could barely read, or even sleep. He struggled to speak. His quality of life was plummeting.
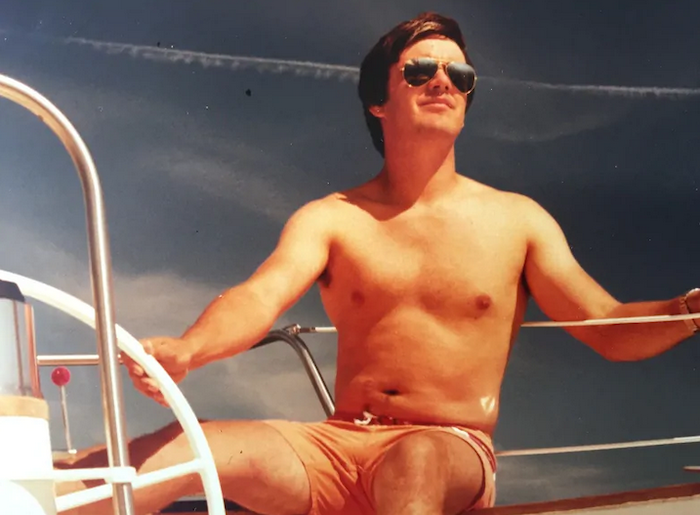
Micallef’s wife, Vickie, said she said goodbye to him 10 years ago because his personality had changed. ‘The man I married hasn’t been with me for a long time,’ she said. The couple, pictured here in 2008, were married for 48 years.
“He told me, ‘My brain is starting to have little explosions in it and my muscles are starting to have little explosions,’ which means he’s going to the next stage,” Vickie said.
Huntington’s disease is an illness that causes certain parts of the brain to die, and results in physical, cognitive and emotional symptoms.
Patients lose weight, have diminished co-ordination, and difficulty walking, talking and swallowing. They can also face symptoms like depression, irritability, and obsessive behaviour.
Saying goodbye
According to the Huntington Society of Canada, people in advanced stages of the disease can no longer manage the activities of daily living, and need professional care.
Micallef wanted none of that.
“I think I said goodbye 10 years ago to Michael because the personality changed, so the man I married hasn’t been with me for a long time,” Vickie said.
Micallef’s family says he had a successful sales and management career. He was diagnosed with Huntington’s disease in his 40s. His father also had the genetic disease. After watching his decline, Micallef didn’t want to go through the same.
Last month, in a friend’s backyard in the city’s Leaside neighbourhood, a nurse injected Micallef with a sedative. Then a doctor administered a substance to end his life.
He died while reclining on a lawn chair, with his wife next to him.
“We had a lovely little chat before he left,” Vickie said.
“I know he’s in a better place. I know his fight — I know his pain — is over with.
“I tell people Michael’s soul is now soaring through the universe, happy to be out of the broken body.”
I knew it was coming; I had known it was coming for years. I had seen my friends go through it, and I had spent many hours thinking deeply about what would happen. Comforted by theories on the nature of consciousness, seduced by feasible rationales for an afterlife, sobered by the practical science of what was really going to happen, I was prepared. And then she died.
My nana had been ill for a long time. Her final diagnosis, chronic obstructive pulmonary disease, came 12 years before she died, although the prognosis was no more than four. She had come close so many times that we had started calling her “the boomerang”. But when she went into hospital for the last time, although in our heads we constructed logical expectations of her coming back to us, in our hearts we knew she wasn’t coming home.
Losing someone close to you is something you can only really talk about once it has happened. All the cliches about grief that I had heard over the years became my reality. Half an hour after she died, my cousin Elliot and I sat in the hospital coffee shop, exhausted, paralysed, silently delirious, while a tiny white butterfly fluttered around our heads, flew a full circle above us and disappeared. Over the next week, the appearance of white butterflies comforted each member of my family at different times in some ineffable way. Despite our wildly varying degrees of faith, that delicate symbol soothed us with an understanding that she was OK: whether she was on a cloud with her brothers and parents, united on an unknown spiritual plane with a greater force as part of a universal consciousness, or just gone, she was no longer in pain.
It was very sad, of course, and that is the best it was ever going to be. The reason I say “the best” is that, if it were not for the acutely careful preparations of us all, including Nana, it could have been far worse.
Palliative care should not be as taboo or scary as it is to many of us. I would go as far as to say that it is the ultimate in wellbeing practices, when a person’s health has failed and all that can be done is care. The word “palliative” comes from the Latin pallium, a cloak, and in many ways this metaphor is apt. In the last days, a “syringe driver” delivered her a steady flow of morphine and anti-anxiety drugs that concealed the worst of her symptoms, shielded her from their effects, protected her from the pain, and even hid her from death for a few more hours or days. If she had not had that, she would have died of hypoxia on the Thursday, gasping violently for breath as she drowned in carbon dioxide that her lungs were too weak to exhale. Instead, she went on until the following Tuesday, my auntie’s birthday, not before she had me write in her card: “Life is worth living because you’re my daughter.” When she finally passed, it was a moment of peace.
(Note to doctors: if it could be called anything other than a “syringe driver”, I think everyone would be much happier. My bampy (grandfather) in particular was unnerved by the name and was initially convinced that it was going to speed up her death.)
On the Saturday, when we all first expected her to go, we played her favourite songs at her bedside: lots of Maria Callas and Ella Fitzgerald, and (who knew?!) Hot Chocolate’s No Doubt About It, a song that recounts Errol Brown’s alien visitation. We were gifted the time to rejoice with her in what made her joyful, emotional and eccentric. As she appeared to slip away, our tear-stained faces fixed around her in uncontainable smiles, sure that the hour had come, she boomeranged back again, just in time for The Chase.
Memories of moments in her final days are precious and I am gratefully aware of how lucky my family and I are to have had them. They exist because of palliative-care specialists. What a mystically unique role: part scientist, part shaman; half doctor, half priest; with careful words held equally as important as the careful drugs. Never hard-heartedly functional, and never “compulsively positive”, it is as if they are of the same station as midwives, just on the other end. I am profoundly moved by this practice. The UK is reportedly the best in the world at end-of-life care, which is cause to be proud, and there are calls from both the International Association of Research in Cancer and the World Health Organization to declare palliative care a human right.
As someone whose first close bereavement was sort-of-sweet-sad but without regret, I support these proposals wholeheartedly. I wish that all people could be treated with such deep compassion and humanity. I sincerely hope that, when it is my time to die, my family and I will be helped to prepare in the same caring, tender way that my grandmother and family were in Llandough on a long weekend in July.