“Why, you may ask, take on this unpleasant, frightening subject? Why stare into the sun?”
— Irvin D. Yalom, Staring at the Sun: Overcoming the Terror of Death

“Are you willing to pretend something for a minute?” asks Greg Lathrop, a local end-of-life activist. “So, let’s pretend this. March 27 will be your last day here. In this game, we know that you’re going to die March 27th. Now, how’s your life? See, it’s a simple perspective shift. Perspective is just a choice. You shift the perspective just that much, and it opens a door. We’re getting somewhere. Now it’s like, ‘I hate my job,’ or ‘I’m in debt up to my eyeballs.’ What would it look like, in these last three months, to live the best three months of your life? It gives us an opportunity. It’s more than a bucket list. What’s your life’s purpose — why are you even here?”
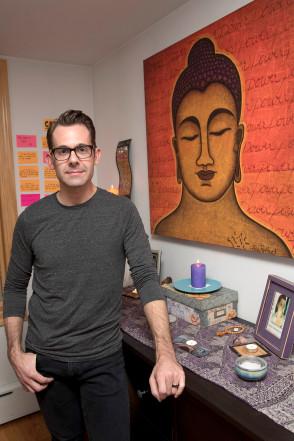
Lathrop, a registered nurse, holds a certification as a Sacred Passage doula — caring for people who are in the process of dying — and is co-founder of Asheville’s Third Messenger, a community of Asheville death-issues activists who have created a forum for conversations about death at the so-called Death Cafe. Lathrop is also part of a growing national community that works in “the death trade” — people dedicated, he notes, to broaching the conversation of death and dying within a culture that prefers to speak about virtually any other subject.
Lathrop first began that conversation on the heels of his own significant loss. Synchronistically, the death of Lathrop’s wife and the passing of Third Messenger co-founder Said Osio’s daughter propelled the two men to join forces in end-of-life activism. To Asheville locals and tourists alike, Third Messenger’s work may be most visible in what has become a landmark Biltmore Avenue structure.
Ministered to for years by Earl Lee “Happy” Gray (before his passing in October 2016), the “Before I Die” wall poses passers-by one simple question: What have you left undone? Not surprisingly, responses range from the mundane to the profound, reflecting our culture’s divisive relationship with the end of life. Yet the wall serves as a catalyst, the beginning of what Third Messenger views as a critical and much-needed conversation. “We cultivate the sacred art of being with dying — we use art to engage the conversation,” says Lathrop.
It is precisely this lack of familiarity with death that engenders the paralyzing fear of the unknown and creates what author and end-of-life activist Stephen Jenkinson, who spoke at Asheville’s Masonic Temple Nov. 6, refers to as a “death-phobic culture.”
Dr. Aditi Seth-Brown, hospice and palliative care physician at CarePartners, agrees: “Many years ago, there were so many intergenerational families and communities, so death was something that young children were around and saw — life happened around death.” As a result of an unfortunate marriage of families living farther apart and a highly individualistic culture, Sethi-Brown now frequently encounters many individuals who have virtually no experience with the process she views as an inextricable part of life.
“People come to us, and oftentimes this is their very first experience with death, and there’s so much fear of the unknown,” says Sethi-Brown, who is also is a local musician, whose work includes playing for people transitioning and at Third Messenger events. “Sometimes, family members come to us and say, ‘We don’t want our loved one to know that they’re dying.’ We don’t practice it. There are some traditions around the world that actually have practices around death, meditations around death — just like if you’re birthing, you go to birth classes, read birth books, but [there’s] nothing to prepare you for death.”

Shining light upon the shadows
“I was 9. That’s the start of it, in my memory.” says Asheville resident Julie Loveless. Beginning in early childhood, Loveless found herself plagued by an inexplicable and inescapable fear of death. One night in particular, Loveless says, “We were at my grandmother’s house. My parents were there, my grandmother, my aunt, and it was time for me to go to bed. I was terrified, because I knew I wasn’t going to wake up the next morning. So I was coming up with all of these tactics to stay up. I had a fever, I had diarrhea, my stomach hurt, I was throwing up, I fell down the stairs — anything I could do to stay up and be the center of attention.” It was as though she needed to be seen in her terror, Loveless says, validated in her very existence. “I needed somebody to know I was alive.”
Loveless’ childhood fear of death is far from uncommon. Recent studies show that children as young as 5 express substantial “death anxiety.” The results of one such study indicated that a mature relationship to dying (understanding death as an inevitable biological event) correlated with a decreased fear of death.
Is it any surprise, when many children are now inoculated from the natural rhythms of life, that they fear, rather than revere, that great unknown? The reality is that “we don’t even have a language for dying,” says Lathrop.
Trish Rux, hospice and palliative care nurse and Sacred Passage doula, agrees. In contrast to her upbringing, she says, the majority of individuals she meets have rarely contemplated death. “I was raised without a death phobia,” Rux says. “I remember my father bringing me to a friend’s funeral when I was pretty young and my not really understanding about the casket, and his explaining it to me. He was just a very practical person. Just knowing that death is a part of life — it was an accepted thing.”
In stark contrast, Rux now regularly witnesses individuals who, in their final days, have scarcely given a thought to the inevitability of their own mortality. “Curiously, I’ve had people that in are in their late 80s, and they’ve not thought about their death. It’s incredible to me — they haven’t thought about what they want, who they want to see. It’s sad for me, and it’s pretty common.”

Dancing with death
Loveless was 30 when she first received a diagnosis of breast cancer and 37 when it returned with a vengeance. After having been in remission from the cancer for seven years, a persistent lymphedema sent her back to the oncologist for a standard biopsy. “I’ve never seen it happen that fast,” Loveless says. “He walked in, did the core needle biopsy and left. I got my clothes back on and am sitting down, and he immediately walked back in and said, ‘It looks like disease.’ The way he was talking about it, he made it clear it had metastasized. I don’t think he said the word, ever — it was just understood.”
Yet Loveless is no longer afraid to fall asleep. Now faced with the stark reality of her worst childhood fears, she finds herself liberated rather than imprisoned. “When I go back to the last time I remember having that really potent fear of death that was crippling, like pulling over to the side of the road and having to breathe into a paper bag, to now — it’s night and day. Before, when something would go wrong and I’d look into the mirror and see a new mark on my skin, I’d think ‘Oh, that might be skin cancer.’ Or, ‘I have a headache — I might have an aneurysm.’ To have those thoughts in my head all the time, to think that way and then to be like ‘Oh my God, I might have cancer — oh wait, I do have cancer.’ I have the worst thing you can have. Nothing else is scary.”
Freed from the fear of dying, Loveless now finds herself preoccupied with living. “[I] wake up in the morning and [think], ‘This may be my last day — how am I going to spend it?’ [Or], this might be my last minute — do I want to spend it brushing my teeth and sitting on the toilet and looking at Facebook? Or, do I want to go make a really yummy smoothie, or do I want to go outside and look at the leaves? So, if you’re thinking that way all the time, you have no idea that it’s even happening until the end of the day and you realize — ‘I didn’t waste my day today.’”
Lathrop questions whether we cheat ourselves of the chance for a more meaningful life if we spend our days running from the inevitability of death. His answer: “Death is my guru. It becomes a real teacher for how to live.” And Sethi-Brown agrees: “The reality is you don’t know when your time is. Don’t be afraid of having the conversation. The fear of the conversation, the discomfort around it — go there, explore that — and you’ll see, it will change your life.”
Complete Article ↪HERE↩!