
The Mexican holiday has nothing to do with Halloween, but lots to do with normalizing death.

[T]his summer, it seemed like death was everywhere. In the course of a few short weeks I had a miscarriage and watched my dog be struck and killed as we walked down our dead-end road. Two weeks later, my aunt unexpectedly passed away in her sleep.This trio of tragedies would have left anyone reeling, but I realized that I was hurting deeply in part because I didn’t have an adequate vocabulary to talk about death. This was especially evident when I tried to answer questions posed by my 3-year-old daughter, who kept inquiring about our dog and her great aunt for months. I wanted her to understand that death was normal and even expected, but I was having a hard time remembering that myself. (Here are 5 reasons you should talk about death, even if you don’t want to.)
And then, by chance, I stumbled upon information about Dia de Los Muertos—Day of the Dead—and I was captivated. Day of the Dead is most commonly celebrated in Mexico, although other South American countries celebrate as well. It’s believed that spirits arrive on October 31 and leave on November 2. November 1, however, is the main day of celebration, and the day most commonly referred to as Day of the Dead.
Most Americans, if they have even heard of the holiday, associate it with Halloween and colorfully painted skulls. But despite the coincidental timing, it’s really a fun-filled but complex acknowledgement of death as part of life, and it combines the Catholic All Saint’s Day with indigenous traditions and beliefs.
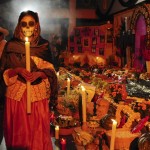
People who celebrate it believe that, on and around November 1, spirits can easily pass between our world and the afterlife. Families might set extra places at the table, exchange stories, and prepare gifts for their deceased loved ones. But mostly the day is about fun, since many people believe spirits would be insulted if they came back to find everyone in mourning.
This seemed vastly different from how many Americans view life, death, and grieving, so I wanted to learn more. It turns out there’s a whole lot that we could all learn from Dia de Los Muertos about the grief process.
Death is a part of life.
I’ve always thought of life and death as opposites. However, Day of the Dead celebrates death as a part of life, rather than the end of it. And recognizing that life and death go hand-in-hand can ease the grieving process, says Kriss Kevorkian, PhD, an expert on grief.
“Day of the Dead connects life and death in a way that, generally speaking, Americans don’t often do,” says Kevorkian. People who celebrate it realize that their loved ones are still present in their lives, even if they aren’t physically there. “You’re not taught to believe that once your loved one dies that’s it.” By normalizing death, the grieving process also becomes normalized and less of something to fear.
A relationship doesn’t end just because someone has died.
“The first chapter of grieving is really recognizing that someone is gone from this world, and your relationship with them is changing” rather than ending, says Tracee Dunblazier, a spiritual empath and grief counselor based in Los Angeles. Whether you believe like Dunblazier does that it’s possible to communicate with the dead, or you merely believe in keeping them alive through memories, recognizing that some sort of relationship can be maintained can be very healing.
“When you think of death as final, you’re looking from a specific sliver of a perspective that does not show the whole story,” Dunblazier says.
Grief doesn’t follow a strict timeline.
When someone you love dies, everyone expects you to struggle—but only for a little while. The problem, of course, is that people don’t heal on schedule, and sometimes it takes months or even years to “move on,” especially after someone passes unexpectedly. This idea is known as complicated grief, and Western cultures usually view it as something to treat (perhaps with therapy and/or antidepressants).
Cultures that celebrate Day of the Dead, however, don’t try to force a sense of closure. Having a holiday that acknowledges the presence of the dead can make complicated grief easier to address, particularly on November 1, when the spirits are thought to be nearby. Believing that your loved ones can hear and understand you on this holiday means that you have the chance to say anything that was left unsaid before they died, says Merrie Haskins, a counselor and psychotherapist based in Minnesota.
Funerals (or at least memorials) can be fun.
In America, death is a very somber event. We wear black to funerals and talk in hushed tones. However, anyone who has ever listened to a lovingly-delivered eulogy knows that smiles and laughter are an important part of the grieving process. Although South American cultures have sad funerals as well, they incorporate happiness and fun into Day of the Dead to honor their loved ones in a more spirited way. That’s something that’s not common in American culture. (See how these 3 alternative therapies can help heal your grief, according to Prevention Premium.)
“We don’t usually have a celebration with levity, happiness, song, and dance,” says Shoshana Ungerleider, MD, chair of the End Well Symposium, an organization that focuses on quality end-of-life care. “People who celebrate the Day of the Dead take this lightness very seriously, due to the belief that spirits who come to visit would be insulted if they found everyone in mourning.”
Haskins suggests adopting that focus on fun as a way to celebrate your loved ones. For example, each year she attends an Academy Award viewing party given in honor of a particular deceased family member who used to love watching the awards show. “That makes it fun for us to remember her and for new people to get to hear about how wonderful she was,” she says.
Stop fearing death, and your own death will be better.
Everyone dies, but many people are too terrified to think about it—to their detriment. “In America, we often shy away from talking about death, loss, and grief. As a physician, I see many gravely sick people in the hospital who have never considered what they want at the end of life,” Ungerleider says. As a result, their final days can be stressful for them as well as their families, because everyone is struggling to make decisions that align with their beliefs while simultaneously dealing with the grief of imminent loss.
A celebration like Day of the Dead can make people think about their own death and plan for what they want at the end of their lives. “By accepting and discussing openly that death is a part of life, you make sure you receive the care you want.”
Complete Article ↪HERE↩!


















{kind=link}