I don’t mean right this moment and I don’t mean that I invite it. I mean that it is inevitable. Echoing in my mind ever louder is the old adage, “the only thing guaranteed in life is death.”
Most of my life – until the very end of it, for many of us – we simply deny death. We forget or don’t hear or don’t heed the echo. But I’m doing the opposite. Like the famous commentator Norman Cousins I’ve decided to embrace dying. Cousins said, “Death is not the greatest loss in life. The greatest loss is what dies inside us while we live.”
First, let me explain what seems like a morbid focus on my mortality. You can skip the next few paragraphs if you’re easily grossed out, and for a long time I didn’t tell anyone because it’s pretty disgusting. A couple of years ago, I developed life-threatening diarrhea. Imagine that dreaded clean-out prep you have to undergo for a colonoscopy. Except that it doesn’t just go on for a day; it goes on for days without end. Just keeping myself hydrated was a constant challenge. I laid on the couch pretty much unable to get up. Fortunately, my gastroenterologist made a diagnosis of an autoimmune disease like lupus – except that my immune cells seem to particularly love munching on my colon.
Also, fortunately, modern medicine has developed a special steroid that for me was a cure that helped me to be, thankfully, (mostly) symptom-free. Then I went to South Africa and all hell broke loose. My colitis symptom – eliminating huge quantities of brown water as often as every 15 minutes – recurred full blast. Again, a raft of tests revealed the diagnosis and a treatment. It was none other than traveler’s diarrhea – three types of E. coli were all partying in my bowels and a blast of antibiotics took them out.
Out of the woods again – whew – except I wasn’t. About a week later I got yet another series of bouts. This time my stool tests were clean. So what was going on? Just as I faced another colonoscopy I remembered the miracle steroid. I had tried it after South Africa and it did nothing. But that was when I’d been loaded with bacteria. Maybe the bugs had triggered a recurrence of the underlying disease? So I started myself back on the steroid and I seem to be OK again. But coming to terms with the fact that I will live the rest of my life with this autoimmune condition has forced me to acknowledge my own mortality.
As my friends age, each is confronting death. Those with chronic diseases are dealing with this reality more actively. But even in those who remain entirely healthy and robust, I see signs – mostly signs of denial.
Don’t get me wrong. Denial is a terrifically adaptive defense mechanism. But is it the best way to avoid dying while we still live? What does it look like for me to not just deny but actually welcome my lifetime limit? It looks like the Tim McGraw song:
“I went skydiving. I went Rocky Mountain climbing. I went 2.7 seconds on a bull named Fumanchu. And I loved deeper. And I spoke sweeter. And I gave forgiveness I’d been denying. And he said, ‘Someday I hope you get the chance to live like you were dying.’ ”
I’m not so sure about the bull riding and the skydiving, but other than that I’m living by McGraw’s recipe. I’ve taken up Ecstatic dancing. I’ve become a regular at ad lib storytelling events – although so far just as an audience member. I’ve been traveling more and to more exotic places. I’ve gone to my first rock ‘n’ roll concert. I’m even going (only because my 20-something children invited and are going with me) to Burning Man – a kaleidoscopic art and music happening in the Nevada desert. And, yes, I know that temperatures there range from 110 degrees during the day to 30 degrees at night, and I know I’ll need to truck in all my own provisions including tent, water and a face mask for the sandstorms.
Most importantly, I’ve been giving/asking for forgiveness. And I’ve become incredibly committed to loving more deeply. So yes, I’m dying. But inside I’m more alive than I’ve ever been.
Puzzlingly, the older and more “seasoned” I become, the more this bit of Amish wisdom is true. Especially when it comes to reading. I don’t have time to read. So, I was surprised when I found myself reading a recent publication from the National Quality Forum. However, as serendipity would have it, I am so glad I did. This publication, “Strategies for Change: A Collaborative Journey to Transform Advanced Illness Care“ had me hooked with the introduction. They had the beautiful audacity to suggest that physicians can and do have the ability to engage in conversation about the taboo (their term) subjects of death and mortality. As I read further, I was rewarded with a section devoted to “peaceful death and dying.”
There has been debate about whether we truly live in a death denying culture. I believe that we do. Strongly so. Ernest Becker, in his Pulitzer prize winning book The Denial of Death, makes a compelling case that western societies are THE most death-denying in all of history. I see the results of this everyday. Our mortality, the inevitable finality of this life, is routinely disregarded as an essential contribution to the plan of care. The result is a series of squandered opportunities for healing and even transformation at the end of life. Very sick patients are referred to hospice without a prior discussion of goals of care and resuscitation status. Very sick patients travel from hospital to hospice house, often dying on route. But even more common is a never-ending procession of the dying patients and their loved ones who come to the end of life totally unprepared.
The poet W.H. Auden described death as “the rumble of distant thunder at a picnic.” It’s a brilliant metaphor. In my mind, in that scenario, we have 3 choices. The first choice is to totally ignore the thunder and hope that the storm blows north, but when the storm does hit, we will be totally unprepared and will be in some danger. The second choice is to recognize that the storm is coming, and to feel dread that it will totally ruin the remainder of the picnic, and yet do nothing to prepare for it. The third option is to recognize the threat that the thunder represents, to reorganize priorities and enjoy the good weather while you can, and then be packed and ready to seek shelter when the storm hits. I believe these metaphorical choices are similar to our society’s attitude toward death. Most of us choose the first 2 options in regards to our own mortality.
The medicalization of death and dying, increasingly prevalent following World War II, has placed physicians in a difficult situation. Advancements in medical technology, the rise of consumerism, and the strengthening voice of patient autonomy have encouraged society to give us the responsibility of managing death, but for the most part we are poorly trained and generally not inclined to do so. We have, however, made significant progress in helping patients and their families negotiate the myriad of decisions and break points they encounter as their health fails and they traverse the healthcare system. This progress, through many variations of advance directives, follows the thread of “quality of life.” I picture the patient as Indiana Jones, running through the jungle, dodging spears and traps, tumbling and rolling, and finally seeing the clearing in the trees. With the screen focused squarely on their face, I see the expression go from anticipation and relief to dread as they look down into the 10,000 foot abyss. Advanced Directives and Goals of Care discussions may get them through the jungle, but when it comes time to die, they are horribly unprepared. Very little time, they realize, was spent considering the quality of their death. It is time to die, and they haven’t imagined themselves on this death bed.
Dying patients and their loved ones today enter a space totally unfamiliar. One hundred years ago, most Americans grew up in household where death occurred and dying was more accepted as a part of daily life. Today, many of us live on the surface of life, existing from Tweet to Tweet. Richard Groves calls this “the demon of busyness.” Our attention span has been measured in seconds. Dying, and being with the dying, often requires sitting with uncertainty for long periods of time. We are very uncomfortable being there. It often does not sound, look or smell nice. Dying is the ultimate time of transition for those involved in the loving and caring for the dying. Without experience, and with difficulty accepting uncertainty, many patients and families come to the dying time unaware of what to expect, and worse, how to prepare.
We need to work much harder at preparing our patients for end-of-life. This is not our responsibility alone, however. There seems to be a grassroots movement developing that encourages open discussion about death and dying. Social media is exploding with new and increasingly innovative ways to initiate and encourage this dialogue. The demon of busyness is being met head on by card games, like “GoWish”, and interactive art such as the “Before I Die “ walls. These social instruments allow our society to begin the uneasy discussion about what has been taboo. In medieval times, the practice of “ memento mori,” a constant gentle reminder of their own mortality, served the purpose of improving the quality of their life, But it also improved the quality of their death. They heard the thunder, they prepared for it, and they enjoyed the picnic.
We can, and should, be part of the discussion. We should initiate it and foster it. Consider hosting a Death Cafe or buy and distribute GoWish card games. Volunteer at a local hospice doing bedside vigils, and write about what you learn. We can become more comfortable in talking about quality of death. We can improve the quality of our patients lives by helping them consider the quality of their dying. It will require that we prepare ourselves by facing our own mortality. We can and should be living and breathing versions of memento mori. We should not run and hide. Our death denying culture needs leaders to help our very sick and dying face the abyss. If not us, then who…?
Two employees from Alive Hospice take on acting roles as a terminally ill patient and a family member as part of a training simulation to help a doctor learn to speak openly about end-of-life care.
[T]he doctor pulls up a chair next to his patient, a 74-year-old woman with lung cancer. He tells her she doesn’t need more chemotherapy. Her eyes perk up; has she beaten her cancer? As it turns out, no. Her cancer has metastasized. She only has six months to live, at most. But her doctor is unable to find the right words.
“My cancer’s not gone? I thought it was getting better,” the patient says, bewildered.
“That’s the tough part …” the doctor replies.
“So, no further treatment?”
“I think we need to focus on quality [of life] over quantity.”
“Are you saying I’m dying?”
From the other side of a two-way mirror, Anna-Gene O’Neal listens closely. She’s set up this simulation — the prognosis is part of a script; the patient is an actor; the physician is being recorded — to improve the way he broaches the topic of death with real patients. O’Neal hears the mock patient all but pleading with the doctor to give her a direct answer. He struggles to do so. After a few minutes, she opens the door to end the simulation.
O’Neal, who runs Alive Hospice here in Tennessee, launched the SHARE simulation lab last year. Participants run through four scenarios. The actors playing patients reply with all the emotions — confusion, denial, anger, grief — that doctors might encounter in real exam rooms. Afterwards, O’Neal sits with the doctors as they watch tape of these interactions on a big-screen TV.
Faced with the uncomfortable task of discussing death, doctors often avoid the topic. Only 17 percent of Medicare patients surveyed in a 2015 Kaiser Family Foundation study said they had discussed end-of-life care — though most wanted to do so. Since that study, Medicare has begun reimbursing providers for having these conversations. Yet still, just a fraction of Medicare recipients at the end of life have those talks with their doctors.
In response, advocates for improving end-of-life care have launched training sessions for doctors around the country.
In California, Stanford’s palliative medicine department has trained dozens of hospice nurses using exercises similar to those carried out here by Alive. In New York, oncologists at the University of Rochester Medical Center observe their peers having conversations with real patients facing terminal illness. In Arizona, the administrators of Phoenix-based Hospice of the West hold regular training sessions, complete with small group discussions, at staff meetings.
Simulators with live actors have intuitive appeal, especially since doctors rarely get hands-on experience with these tough conversations in medical school. But Dr. Scott Halpern, director of the University of Pennsylvania’s Palliative and Advanced Illness Research Center, said there’s little evidence that simulators are any more effective than any other clinical training to improve end-of-life counseling. They show a “tremendous amount of face validity,” he said, but they must be held “to a standard of showing benefits for patients, not a standard of an appealing anecdote.”
O’Neal, 50, agrees more evidence is needed. But she’s also so gung-ho about her simulator that she’s pushing to expand it across the country. Four health organizations — including faith-based Ascension Health — have agreed to let Alive train their clinicians. Later this year, O’Neal plans to work with medical students at one school in Tennessee. Down the road, she hopes to get some independent practice associations to require their members to undergo her training.
“It’s about doing the right thing,” O’Neal said. “I feel strongly that if you do the right thing by people, they’re going to make different decisions.” That shift could lead to more of what she calls “good deaths,” with patients fully aware of their prognosis and able to choose whether they want aggressive, long-shot treatments or would prefer to simply have their pain managed while they spend their final days with friends and family.
Alive Hospice CEO Anna-Gene O’Neal chats with a doctor who went through a simulated scenario about how he can improve his communication with patients.
The little things that can make a big difference
Two of O’Neal’s closest friends died young from breast cancer. Seeing their hospice nurses bring light to the darkness of death prompted O’Neal to think back on her own professional experiences caring for babies as a neonatal nurse and for the elderly as a health care executive. What stood out: the power of clear, concise communication between clinician and patient.
O’Neal came to believe health providers in all specialties should be trained to have such direct conversations. In 2012, she was hired as CEO of Alive Hospice, a nonprofit chain of hospice care facilities serving more than 3,500 patients and families a year in central Tennessee. She soon realized that many Americans lived in “a crisis of denial of our own mortality,” in part because “medical institutions encourage us to never give up.”
So she launched the SHARE simulator. Clinicians pay to participate — $350 to work through four scenarios and then watch the videos and get feedback from O’Neal or her staffers. (To give doctors more privacy, Alive deletes the footage after each session, handing them the only copy so they can review it later if they’d like.)
The work unfolds in a low-slung brick building near Nashville’s Music Row, in a room that looks like a typical hospice or hospital room, set up with a bed, a couch, a box of tissues, and a stack of travel magazines. Tiny microphones dangle from the ceiling to record audio without intruding on the intimacy of conversations. Video cameras shaped like domes are mounted on the walls.
So far, O’Neal has trained 12 doctors and 65 other clinicians, including nurses and social workers. O’Neal said some have already tweaked their communication style: Maybe they’re more comfortable with long pauses after breaking hard news to patients, or more aware of body language that may come off as too stern.
“Watching yourself, you get a feel for your posture, whether you’re using specific phrases, looking a person in the eye, or keeping focus on them,” said pulmonologist Dr. Richard Fremont. “It was helpful seeing what I thought I was doing.”
Dr. Robert Taylor, a nephrologist based in Nashville, initially found the cameras in the training room unnerving. But the actors quickly pulled him into the scenario.
“It’s awkward to see yourself,” he said, describing the experience of watching the footage later. But he noticed little things, like his posture and the inflection in his voice. When he saw the mock patients’ reactions, he realized that little shifts in his own approach could change their perception of the conversation.
Taylor said he’s been committed to frank discussions with patients ever since he recognized, early in his career, that dialysis patients rarely got a full picture of their options. Their doctors were often focused on keeping them alive. But the disease and the treatments often make them “so fatigued that it’s not the quality of life they desire,” he said. Ever since, Taylor said he’s taken pains to better communicate all options to his patients; he wanted to go through the simulator to hone that delicate art. “It can alter what you do,” he said, “but also confirm your answers.”
O’Neal said the simulator challenged other doctors’ views that a patient’s death must inevitably be viewed as a failure.
“Once you get doctors into the training, you create an opportunity for them to be vulnerable and see themselves differently,” O’Neal said. “Whether they admit to change or not, they will change.”
A political divide over end-of-life conversations
When the idea of paying doctors to talk about dying was first debated – during the early, bitter fights over the Affordable Care Act in 2009 – conservatives warned that such conversations could be a pretext for pushing the frail and elderly to give up on treatment. Former Alaska Gov. Sarah Palin said funding of end-of-life counseling amounted to a “death panel.” Iowa Sen. Chuck Grassley said it could enable “pulling the plug on grandma.”
The debate still rages: Earlier this year Iowa Rep. Steve King introduced the Protecting Life Until Natural Death Act, which would end federal reimbursements for end-of-life discussions. King has described such conversations as “intolerable to those who respect the dignity of human life.”
But despite such efforts, O’Neal sees growing support for her approach on Capitol Hill. Last month, a bipartisan group of lawmakers — including Democratic Sen. Mark Warner of Virginia and Republican Sen. Johnny Isakson of Georgia — filed a bill that would provide $50 million to fund access, education, and training related to end-of-life treatment for terminally ill patients.
“Encouraging patients and their families to have these conversations with their physician helps provide peace of mind and undoubtedly increases the likelihood a patient’s care will be consistent with their wishes,” Tennessee Congressman Phil Roe, one of the bill’s sponsors, said in a statement.
O’Neal concurs: Such conversations, she said, empower patients to embrace death on their own terms — and can make those final days “the most meaningful part of the human experience.”
“If somebody’s faith is such that as long as there’s a beating heart, you keep doing everything, we’re 100 percent behind that,” she said. “But if someone says, ‘if I can’t walk to play 18 holes of golf, I’m done,’ we have to respect that as well.”
A doctor, sitting inside Alive’s training room, watches footage of his interaction with a patient and her daughter.
A second chance
O’Neal asks one of her staffers to turn on the big-screen TV in the simulator room so the doctor can review his performance with the 74-year-old patient. As the footage rolls, the doctor grips one of the arms of his chair, bearing a slight grin of discomfort as he watches his fumbling attempts to tell the mock patient she’s dying. Soon, he’s critiquing himself:
“I think I would have been much less polite if I wasn’t on camera …”
“I would’ve been more blunt …”
“That could’ve been done faster …”
After he’s finished, she chimes with nuggets of advice: Don’t let her chase answers. Communicate like it’s a conversation. Honesty is a form of compassion.
“It’s intimidating,” O’Neal reassures him.
The second scenario goes far better. In it, the same patient returns two weeks later with a slew of strange treatment suggestions a relative found on the internet, including a raw beet diet and blood transfusion at a clinic in Juarez, Mexico. The doctor listens intently, careful to let her finish, mindful of his body language.
After she’s done, he leans forward and steers the conversation in another direction. He makes eye contact.
Then, he says in a calm empathetic tone: “We need to start thinking ahead.”
After Morgan’s second surgery he couldn’t remember Fiona’s name, but when asked who she was he answered “the love of my life”.
Who is the best person to care for someone who has died? Sometimes, a person who loved them when they were living. Dr Fiona Reid shares her experience caring for her husband Morgan throughout his illness and in the days after his death.
My husband Morgan was a kind, active and talented man. I felt tremendously lucky when I met him and continued to do so throughout our years together.
Morgan was remarkably fit, working as a stuntman internationally. He trained every day and could perform feats of acrobatics and skill. So it came as a shock when he called me at work one day to tell me he was having difficulty spelling. My heart fluttered and my stomach turned over. I felt an intense sense of dread but tried to convince myself that I was overreacting.
I told him to stay at home and that I would be there shortly. I drove home and held Morgan in my arms. We both knew something was very wrong. Despite this, I was totally unprepared for what happened next; for the utter horror of watching his scan and seeing the large tumour in his brain. My legs wobbled. I wasn’t supposed to be in the CT room because today I was a patient’s wife and not a doctor, but no-one thought to stop me. I still think that was one of the worst moments – the moment the world ended.
“Are there any gremlins in my brain?” he asked. “Yes darling, there is a gremlin”.
Like most people, we had a lot of hope. Morgan was young, he was strong, I was a doctor. Surely the 14-month prognosis was not for him.
He endured two operations on his brain, chemotherapy, radiation therapy, three experimental treatments and more chemotherapy before finally in January 2016 we decided to stop most treatments and concentrate on what little time we had left.
By this time my gorgeous husband was struggling. He had lost half his vision, he couldn’t use the right side of his body, his face was swollen from steroids and he was very tired. It never occurred to me that I wouldn’t look after him. I began to prepare for caring for him at home.
I was lucky to have some knowledge of what caring for someone who is dying might entail, but whatever I knew as a doctor was a fraction of the real experience. I prepared though. I read blogs written by other women who had cared for their husbands through brain cancer. I researched the timeline, what might happen, how his death might be, what symptoms may occur. I tried to predict.
I learned that we continue to hope, even when things are deteriorating. So even if we only get a “good hour” we hope for another later or tomorrow. We learn to reduce our expectations, such that a smile or a squeeze of the hand seems like a victory and the promise of recovery. Therefore in order to prepare, you must force yourself to remember what happened yesterday and last week. When there are more bad days or bad hours than good ones, you know it’s time to make arrangements.
The hardest thing was doing this whilst still trying to keep up Morgan’s spirits (not that he needed much help; he was extremely positive right until the end). I tried to be open with him, but he looked a little hurt when I had the hospital bed delivered. I felt I had let him down a little, but he was struggling to sit up and I was finding it difficult to lift him.
The bed came just in time. A few days later he was unconscious and although he woke up, he never spoke or left his bed again until after his death three weeks later.
You need equipment if you are to care for someone at home. I needed a bed, a wheelchair, a commode, a bath board and later continence aids, pads, eucalyptus oil, face-washers, medications, liquid thickeners and bed shampoo caps. Most things were rented. I bought consumables from disability companies and the palliative care nurses provided some.
Mostly I needed strength, love and support from family and friends – they believed I could do it and the thought of giving him up to someone else’s care frightened me more than caring for him myself.
I decided early that as much as I loved Morgan he didn’t belong to me, and he deserved to be surrounded by love as often as possible. So I declared an open house. I told everyone that they were welcome to visit at any time and without notice, but I also warned them that I would not be providing food or drink and that if the house was full or it was a bad time they may be asked politely to leave.
I also asked for two hours each day to be alone with Morgan. I put on nice music, burned a candle, bathed him, cuddled him and had some quiet time with him. This was precious time for me. Usually, he would smile at me, then fall asleep as I washed him. I put eucalyptus oil in hot water to freshen the air and massaged lavender oil into his temples to soothe him.
It was during this three weeks that I began to think about “after”. His death had now become a real inevitability; he had stopped talking, eating and swallowing, and he slept more often than not. It felt awfully disloyal to start planning his funeral before his death but I was desperate to do something that honoured him and I knew that every funeral I had been to so far would fall short of his expectations. I had little to go on. He did not want to talk about it. He did not want to be cremated, he wanted to be buried somewhere “with trees” – not a manicured cemetery, and without religion.
I knew I wanted to care for him until the last minute – I never wanted to let him go – but I had no idea what was possible. My experience of death so far had been as a doctor working in a hospital and try as we might it is a cold environment, people are rushed through the death of a loved one and bodies are moved quickly to morgues.
I stumbled on home death care. I was looking at local funeral directors and I felt empty – they all seemed so cold, so scripted, the coffin so pointless. I had no idea what to do. By chance, I found a wicker coffin on an Australian site and I thought it looked beautiful, natural, easily degradable and strangely, comfortable. I looked for the local retailer and found Natural Grace holistic funeral directors. It was as if Natural Grace was made for us.
I watched an interview with managing director Libby Moloney and instantly felt that she was special. Libby specialised in home death care and I knew I wanted to keep Morgan’s body at home. She knew a natural burial site which was 10 minutes away from where we were married. It seemed perfect.
I called Libby, speaking softly and feeling awful guilt as I sat in the same room as my sleeping and alive husband. She was incredibly compassionate. She seemed to understand my hesitation and confusion. She was supportive and never pushed.
I crawled into bed with Morgan on the night of Easter Sunday. I knew this was it. I put my arms around him and a few hours later he took a final breath. It broke my heart.
Libby told me that when he died I should feel free to spend some time with him before calling her. I cuddled him and cried. I called his family and they came we spent a few hours together until 4 am, toasting him with single malt whisky and sobbing together. I called Libby and the palliative care nurses in the morning but asked everyone to leave me alone with him until noon. I wanted to wash and dress him and I wanted to do this alone.
Libby came to the house. It was the first time we had met and she was wonderful. The first thing she said was how beautiful Morgan was and then she asked if she could touch him. I was so grateful for that.
She showed me how to set up the cooling blanket then she talked me through what to expect and watch for. She was honest and very frank which I appreciated. We talked about fluids and smell and flies and all those horrible things that could potentially occur but didn’t. Then she suggested I take some locks of his hair.
She offered to do all these things for or with me but was sensitive to the fact I wanted to do it myself. I knew I had made the right decision; had an undertaker come to take Morgan away from me at that moment I think I would have screamed. The pain of his loss was unbearable and I needed a little more time.
I decided that the first day would be for family only, the following for friends and family. I made and received various calls. I warned everyone “Morgan is still here, he looks peaceful”. I told them not to come for my sake but that if they wanted to come and say goodbye they would be most welcome.
I had warned his family that I intended to keep him at home. They were very supportive but understandably surprised. They all visited and sat with us, and I think they appreciated it. On the second day, his brother decided it was time for him to say goodbye. “I won’t be back tomorrow,” he said.
Friends were varied in their response. I found that women wanted to come, but men were less sure. Most people seemed glad for the opportunity to say goodbye. Some wanted a few minutes alone with him (this was hard for me but I did it). Some tried to ignore his presence and just talked to me. I continued to sleep on the sofa beside him.
On the third day, I realised I had to let him go. I had sat by his side for a month. I hadn’t stepped outside or seen the sun, I had barely eaten and barely slept. I needed to visit the cemetery, pick out a burial site and organise the funeral. I needed to leave the house but I couldn’t leave his side.
Now when I looked at Morgan I could see he wasn’t there anymore; whatever he had been had left. I called Libby. She came, I helped, and everything was done with the tenderest care. I had arranged a wedding photo, an autumn leaf and a teddy on his chest in his hands and she asked about them so she could recreate it perfectly in the sanctuary at Natural Grace. It was terribly hard but I was glad I felt able to trust Libby to look after him.
I went to the cemetery to pick a site with Morgan’s sister. We didn’t speak about it but we both picked exactly the same spot, under a beautiful Candlebark tree. We went back to Natural Grace and I checked on Morgan. He was there in the sanctuary, looking just as undisturbed and peaceful, the items arranged just so. Then we discussed the funeral and Libby was open to everything we wanted or suggested. I asked if we could bring him to the funeral ourselves in his 1974 Bedford van (the Beast); “A wonderful idea!” she giggled. She recommended a celebrant. We wanted mulled wine served – “No problem”. I wanted guests to be able to tie messages and flowers into the casket – “Easy”. We would like Morgan’s father to play his pipes – “Lovely”.
On 1st April 2016, we buried my beautiful husband. We met at Natural Grace and I spent the morning sitting with him, holding his hand. I had picked flowers to place in the coffin with him. His family and I placed him gently into his wicker basket coffin. We arranged flowers around him. We placed him in his van. We said goodbye.
We held the service at the cemetery with 300 mourners. Libby looked after me, making sure someone gave me food and drink, and guiding me through the funeral, sometimes physically. She did not rush me, even though the service went much longer than anyone anticipated. Afterwards, at the wake, there must have been 100 people who told me how beautiful it was, and how “Morgan” it was. No-one had been to a similar funeral and they were amazed.
The decision to care for my husband at home before, during and after his death was simple for me but would have been all the harder, perhaps impossible, without the kind, attentive, professional support of Libby, and the loving acceptance of my and Morgan’s family. They allowed me to make these decisions and held my hand throughout this most devastating time. For this, I am eternally grateful to them.
A palliative care specialist reveals what she’s learnt
[W]ith two decades of experience in helping people approach their final days in the best way possible, Adrienne Betteley shares her most touching and disturbing moments
First as a nurse, and then working with Macmillan Cancer Support, I have spent nearly 20 years helping people during the final months of their lives – and making sure that as many as possible have a “good” death is a great privilege.
If my experience of end-of-life care has taught me anything, it’s that there is indeed such a thing as dying “well”. Of course, the way we die varies depending on the cause of death, as well as the individual needs of the person, but there is also a tragic variation in the care and choice that people have as they approach their end.
At Macmillan, we believe the first step in achieving a “good” death is talking about it more – as we set out in our recent report, No Regrets. We looked at the taboo around discussing death, and how planning ahead can help people to die in a place of their choice and to have more control over their treatment.
So, in the spirit of talking more, and being honest, I’m sharing some of my experiences. I hope that it inspires others to do the same.
Dennis’ late wife, with her son (Adrienne’s husband) and grandchildren.
Closure is important
The first time I encountered death was when I was seven years old and living in Australia in the 1970s. My best friend, Stephen, died of leukaemia at the age of 11. He was the son of some close friends of my parents and was like a big brother to me. He was so kind-hearted, and I really looked up to him.
Death wasn’t seen as something children should know about, so I never visited him at hospital or went to his funeral. No one talked about Stephen dying, and I had recurring nightmares about it. I feel that I never had closure, and still think about it now sometimes.
Adrienne Betteley
Don’t let fear stop you
When I was 25, and living in Cheshire, my maternal grandmother Eileen was diagnosed with oesophageal cancer. Her reaction to finding out she was dying was calm; she began talking about her memories and writing them down.
I was pregnant and my granny “held on” until my daughter, Jasmine, was born. I took my daughter to hospital to meet her great-grandmother, a few weeks before she was moved to a hospice.
The experience with Stephen had scarred me, and I didn’t visit her in the hospice. I was too afraid. I thought it would be like a Victorian sanatorium, with people wailing and crying out.
Years later, while I was a student nurse, I realised a hospice can be a place of joy and peace – somewhere to treasure the end of life, rather than focus on death.
I regretted that I had let fear stop me saying goodbye to someone I loved dearly.
Adrienne Betteley couldn’t face visiting her grandmother in a hospice
Trust a professional
My first career was in architectural stained glass, but I also had a part-time job at a nursing home. One of the nurses asked me to help her lay out a woman who had just died. I was very nervous, but it turned out to be an amazing experience.
I had never seen anyone treat another person with such gentleness and respect. As the nurse washed her and did her hair as though she were still alive, I was in awe. She made her look lovely, in her favourite clothes and make-up.
I understood the huge value that this nurse placed on another person’s life. It was this moment that helped me choose my own future in caring for people at the end of their lives.
Focus on pain relief
While waiting for my nursing training to start, I worked in a different nursing home, where I had an awful experience.
I was looking after an elderly woman who was dying of uterine cancer and had become bedbound. One day, the nursing sister on duty told me to get her out of bed to use the commode. I went to do as I was told, but as soon I touched the woman she dug her nails into me and screamed out in pain. I had never witnessed such agony.
Filled with rage, I went straight to the nurse and shouted at her that nobody in this day and age should be allowed to experience such pain. Why were we moving her when it was clear she needed to be catheterised?
She listened to me and sorted out a catheter and a syringe driver for the pain. But it made me determined that no one should have to experience pain like that.
Communication is key
My father-in-law Dennis had been employed on the Crewe railway works, and after years of exposure to asbestos he was diagnosed with terminal lung cancer.
It was the poor communication we encountered that was really upsetting. He was never told his prognosis by a medical professional; in fact a hospital doctor, knowing my nursing background, asked me to tell him instead. I couldn’t believe they would put that kind of pressure on me. But I went ahead and did it; I felt that at least I would do a better job than this doctor.
Adrienne Betteley’s late father-in-law, Dennis
As soon as I’d told my father-in-law, I felt like the grim reaper. The whole experience blurred the boundaries between my professional life and my private relationship with him – it was damaging and I felt a mixture of guilt and anger.
Dennis was encouraged to have palliative chemotherapy, without being warned of the side effects. Any extra time the chemo bought him was overshadowed by painful mouth ulcers, nausea and fatigue. The treatment destroyed any quality of life, and barely extended it: he died within six months.
If he had been given an informed choice about treatment, I’m sure things could have been different.
Say goodbye the right way
A few years ago, my mother died of oesophageal cancer, like her own mum. My dad and I were at her side, and I’d spent the last week in a camp bed next to her, mopping her forehead as we shared memories.
On the night she died, she put her arm around me and said: “Adrienne, I have to thank you for being the most wonderful daughter.” What a privilege to be able to use my knowledge and experience to support my mum and make her death easier.
Adrienne Betteley’s late mother
A Macmillan occupational therapist had transformed mum’s quality of life, making it possible to fulfil her wish of dying at home. As a nurse, I could advocate for her, and demand the right pain relief – but it really brought home how hard it would be for people without my professional background.
Knowing I’d done everything possible to fulfil her wishes made the grieving process easier, but I still had frustrations about what could have been better – especially the lack of support available at the very end. It sounds clichéd to say “dying is inevitable” or “death is the only certainty” – of course we all die, everyone knows that. But all too often, it feels like we are hiding from it. The fact that it will affect every one of us should galvanise us into action, so we demand a “good” death that is pain-free and meets our preferences about treatment and location – for ourselves and those we care about.
[E]lena Wertheimer still remembers the panic she felt last year after her terminally ill father, Vincent Battista, was released from the hospital to spend his last days at his Wyckoff, N.J., home. She didn’t know how to prepare. She wasn’t sure how to care for him—or herself. “It’s hard to think straight,” she says. “You’re under extreme stress.”
On the advice of friends, Wertheimer sought help from an end-of-life doula, a new type of caregiver for dying patients and their families. Also known as death doulas, they offer support through all the stages of dying, similar to the roles that birth doulas play during pregnancy and delivery. Doulas discuss a dying person’s wishes and concerns, and they create memory books for the family. They organize vigils and coach relatives on the signs of dying. Some run errands, organize paperwork or even plan home funerals.
Wertheimer, 49, was very close to her father, and her doula, Janie Rakow, helped her overcome her fear of watching him die. Rakow encouraged her to sit with him and hold his hand. Rakow gently guided her to his bedside after he passed, and Wertheimer and other family members spent four hours there, crying, laughing and telling stories. Rakow ensured they weren’t interrupted. “It was very, very special,” Wertheimer says. “I saw him finally not suffering. My last vision of him was peaceful. It made all the difference in the world.”
Doulas are gaining in popularity amid a growing effort to improve the end-of-life experience for patients and families, particularly when someone dies at home. Doulas cover “a huge gap” in time and resources that busy hospices can’t always provide, Rakow says. A hospice team advises families on medical care for the dying; doulas guide the dying and their loved ones through the end-of-life process, offering mostly emotional and other nonmedical support.
Finding a Doula
If you’re thinking of using a doula, you may find the search confusing. There are death midwives, mourning doulas, death coaches and more. Some are volunteers; others charge hourly rates of $25 to $100 or offer “Vigil Packages” costing $1,000 and up. There is no regulatory oversight or standard licensing, training or certification. “It’s still kind of the Wild West out there,” says Patti Urban, a doula in Guilford, Conn.
Insurance typically doesn’t cover costs for a doula. Before hiring one, check whether your local hospital or hospice has a volunteer doula program. But be sure the doula can provide all the hours you want.
The International End of Life Doula Association (www.inelda.org) is compiling an online state-by-state directory of doulas it has trained. The nonprofit has provided the training for hospitals and hospices in California, Indiana, New Jersey and New York, and it will train aspiring doulas in 12 cities this year, says Rakow, the association’s president. Doulas will also work with you in hospices, hospitals, assisted-living facilities and nursing homes.
Decide what you want from a doula. Do you need someone to organize end-of-life documents? Or to provide a 24-hour presence at the bedside? Set up a consultation, advises Merilynne Rush, co-founder of the Lifespan Doula Association, in Ann Arbor, Mich. Be sure your doula’s personality is a good fit. You might prefer a take-charge attitude or a soothing presence.
Most doulas charge an hourly rate. Start out with a few hours before making a larger commitment, Rush says. Ask for a contract spelling out services and fees.
Review a doula’s qualifications and training, including criminal background checks and previous experience. Some attend weekend seminars, while others serve a minimum number of vigil hours and pass exams to become certified.
Other groups that train doulas include MourningDoula.com and the Lifespan Doula Association, which details standards of practice at www.lifespandoulas.com. Doulagivers.com offers a free webinar to learn the basics of caring for a dying loved one.
Rabbi Laura Geller addresses a room of participants at Temple Emanuel’s conference, “The Next Stage: Looking Backwards and Ahead,” on November 9, 2014.
[C]onfronting sickness and death is part of a faith leader’s job description. Members of the clergy sit with congregants during chemotherapy treatments and pray with them in the midst of pain.
Pastors prepare for this work at seminary, spending a semester working as a hospital chaplain or volunteering at a nursing home. However, some still enter professional ministry unprepared to sit at someone’s bedside and offer advice, according to recent research on religion and end-of-life care.
Many faith leaders are uncertain of when aggressive treatments should be traded for hospice care and confused about what palliative treatments consist of, reports a study in the April issue of the Journal of Palliative Medicine.
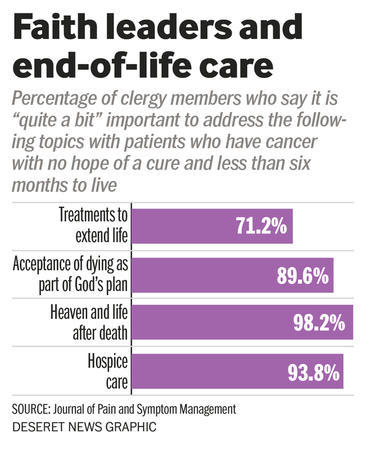
Seven in 10 clergy members say it is “somewhat” or “quite a bit” important for them to encourage ongoing treatment for a cancer patient, even when a doctor says there is no hope for a cure, notes a new study in the Journal of Pain and Symptom Management.
“Poor knowledge of end-of-life care may lead clergy to passively enable congregants with serious illness to pursue … treatments that are associated with increased suffering,” wrote researchers in the Journal of Palliative Medicine.
The National Clergy Project is part of Harvard University’s Initiative on Health, Religion and Spirituality. Program leaders are working on a free end-of-life care curriculum to empower faith leaders, highlighting the important role religion often plays at the end of people’s lives.
“What clergy say — and what they do not say — can make a major difference in whether believers experience a ‘good death,'” the Association of Religion Data Archives reported in its overview of recent research.
Increasingly, palliative care, which focuses on providing pain relief rather than a cure, is seen as a key part of dying well, yet many people, including pastors, find it difficult to give up on intense or invasive treatments.
Accepting that a cure isn’t possible “may be perceived as a decision that undermines one’s faith in a God who may intervene with a miracle through medical treatment,” wrote researchers in the Journal of Pain and Symptom Management.
These researchers and other experts at The National Clergy Project on End-of-Life Care don’t want to undermine religious beliefs. But they do want to ensure that faith leaders are informed about medical options before they influence a patient’s decisions.
“Our goal is for patients and families facing difficult medical decisions to receive better spiritual and medical care,” the project website notes.
Around 3 in 4 faith leaders are open to training on end-of-life care, recent research showed.
In addition to seeking out insights from medical professionals, members of the clergy may benefit from organizing conversations about death and dying within their communities. Rabbi Laura Geller, rabbi emeritus at Temple Emanuel of Beverly Hills, has done this as part of a broader effort to understand what people at her synagogue fear as they near retirement.
“The conversations were so rich and powerful that nobody wanted them to end,” she told the Deseret News last year.
Initial small-group discussions on life after retirement grew into a communitywide effort to better serve the needs of older synagogue members. People thought through how to emotionally and spiritually grow even as their bodies aged and illnesses loomed, Rabbi Geller said.
“How do you make meaning in the face of the fact that you’re going to die? That’s what faith communities are supposed to be teaching people,” she said.