Preparing for the death of a loved one is difficult no matter the circumstances.
But Annalisia Wilharm said she never expected a doctor would deliver the bad news about her grandfather via a video screen on a robot.
Wilharm was sitting by her grandfather’s bedside in the ICU of the Kaiser Permanente Medical Center in Fremont, California, last Monday night when the machine rolled into their room and a doctor, appearing via live video link, offered his grim prognosis. Her grandfather Ernest Quintana, 78, died the next day.
“I think they should have had more dignity and treated him better than they did,” Wilharm told CNN. “No granddaughter, no family member should have to go through what I just did with him.”
Wilharm told CNN her family knew that her grandfather would die soon. But they’re angered by the way the situation was handled and how the news was delivered. She said she and her family hope no one else receives the same treatment.
Ernest Quintana died after being told by a doctor who visited him via robot that there were no more treatment options left.
“I was so scared for him and disappointed with the delivery,” Wilharm said, choking up. “And I could tell by the look on his face what that did to him.”
A spokeswoman for the hospital offered “sincere condolences to the family” in a statement sent to CNN.
“We take this very seriously and have reached out to the family to discuss their concerns,” said Michelle Gaskill-Hames, a senior vice president and area manager of Kaiser Permanente Greater Southern Alameda County.
“Our physicians and nurses were in regular, in-person communication with the patient and family about his condition from the moment he entered our hospital,” she added. “The evening video tele-visit was a follow-up to earlier physician visits — it did not replace previous conversations with patient and family members and was not used in the delivery of the initial diagnosis.”
For years, Quintana had lived with chronic obstructive pulmonary disease, a progressive lung disease that make makes it hard to breathe. It includes emphysema and chronic bronchitis.
Last Monday, doctors at the hospital conducted tests to assess the state of Quintana’s lungs. That evening, Wilharm told her mother and grandmother — Quintana’s wife of 58 years — that the pair should go home and get some rest.
Soon after a robot with a video screen came into the room, accompanied by a nurse who remained silent. A doctor on the screen began speaking to them.
Wilharm said she had no idea who the doctor was or where he was located.
She filmed the interaction on her phone as the doctor relayed the results of her grandfather’s tests.
In the footage viewed by CNN, the doctor on the screen tells Quintana, “Unfortunately there’s nothing we can treat very effectively.”
The doctor explains they can give Quintana morphine to make him more comfortable, but that would make breathing more difficult.
Wilharm then tells her grandfather the doctor is recommending hospice care at home.
“You know, I don’t know if he’s going to get home,” the doctor says, adding that the best treatment plan at that point was to begin focusing on Quintana’s comfort.
Wilharm told CNN that at that point she had to call her mother and grandmother so they could get back to the hospital.
“It didn’t matter (to the hospital) that his wife of 58 years wasn’t there for that,” she said.
Wilharm told CNN that her family was under no illusions about her grandfather’s condition.
“We knew that we were going to lose him,” Wilharm told CNN in a phone interview Saturday. “Our point is the delivery (of the news). There was no compassion.”
When her grandmother returned to the hospital, she asked the nurses about the robot. According to Wilharm, they explained the hospital was small and the robot was used to make rounds at night.
Gaskill-Hames, the hospital spokeswoman, said the health care provider is “continuously learning how best to integrate technology into patient interactions.”
“In every aspect of our care, and especially when communicating difficult information, we do so with compassion in a personal manner,” she said, adding that the term “robot” is “inaccurate and inappropriate.”
“This secure video technology is a live conversation with a physician using tele-video technology, and always with a nurse or other physician in the room to explain the purpose and function of the technology,” Gaskill-Hames added. It “allows a small hospital to have additional specialists such as a board-certified critical care physician available 24/7, enhancing the care provided and bringing additional consultative expertise to the bedside.”
Wilharm told CNN that a doctor had visited Quintana in person earlier in the day.
Wilharm said the in-person doctor was “very sweet” and held her grandfather’s hand as she spoke with him about hospice care and his options.
Gaskill-Hames said the hospital does not encourage the use of technology to replace personal interactions between patients and health care workers.
“We understand how important this is for all concerned, and regret that we fell short of the family’s expectations,” she said.
Wilharm agrees.
“That was one of the worst days of my life,” she said.
After her 52-year-old husband died of the flu in 2014, Susan Capurso from Long Island, New York was left feeling helpless, angry and unsupported.
“We weren’t prepared at all,” says Capurso, who had been married for 25 years. “We didn’t have hospice, as my husband’s illness was not a long-term one. At the end, there was no one standing next to me saying ‘this is what is happening now. He’s going to pass within hours and this is what to expect.’ I’m detail-oriented, I wanted to know.”
Interested in offering non-medical, holistic and emotional support to the dying and their families, Capurso began to research the work of an end-of-life doula. Traditionally, a doula is a layperson who aids a woman in childbirth and newborn aftercare alongside medical staff. In the same way, end-of-life doulas are supportive to hospice; they do not take the place of it.
To further her interest in this growing field, Capurso began volunteering for a hospice and enrolled in the certificate-bearing Doulagivers training school of New York City (DoulaGivers.com), a school started by Suzanne O’Brien, formerly a hospice and oncology nurse.
O’Brien was inspired when, on a trip to Zimbabwe in 2012, she saw how local people were trained to sit with a person who was dying and “guide” them through their journey. While the country lacks basic needs and medicinal care, “they did have neighbors sitting with a family member who is dying — holding that space for them,” says O’Brien. “The power of presence might be the most powerful medicine we have, but we’ve lost that in our health care system. We’re all in this together. We should support each other however we can.”
On O’Brien’s course, “training is individualized,” says Capurso. “Weekends are spent with [O’Brien] and everything else is done online through a series of live webinars and modules.”
The three-pronged curriculum covers end of life phases from diagnosis to stabilization, transition and disease process. Elder care assistance and advanced directive (when a patient determines their end of life wishes while they are still able to do so) is also covered.
“This covers the important papers you really need to button up, such as health care proxy, living will, do not resuscitate,” says Capurso.
Practical help is also part of a doula’s workload.
“We come into homes, prepping meals for the week, doing laundry and going through each room to ensure it’s safe,” says Capurso.
Beyond these basics, Capurso extends her healing work to include the creation of a legacy book with patients.
“It’s something we work on together. We go through your life, adding personal stories, photographs and memories,” says Capurso. “It’s not just something you’re leaving for family and friends, it really is therapeutic — bringing light, love and closure.”
Helping patients to compose letters to loved ones and assisting families with writing memorials and eulogies are also customary tasks.
Having your “funeral” before you die is another trend that doulas can help with.
“Why not have a memorial before you go?” says Capurso. “Let’s laugh, say our goodbyes and be happy. It doesn’t have to be scary. A celebration with the dying person there shapes the person’s life and offers closure.”
Carrying out a dying person’s wishes is also a top priority for Capurso.
“I can help find a way for the last days to meet a dying person’s desires. Maybe starting to contact family members to come in for a final visit, asking them to write a memory down on a card and placing it in to a basket, incorporating nice music, candles or aromatherapy,” says Capurso.
This line of work is especially well-suited for hospice volunteers who want to do deeper work, as well as healers, reiki practitioners, massage therapists and acupuncturists. It’s also beneficial to have a genuine interest in educating the community on the resources available for them.
“You don’t go looking for this career, it calls out to you,” she says.
The demand for such caregivers is overwhelming. By 2020, an estimated 117 million Americans will need some caregiver assistance.
“Doulas fit in to the personal companion model, which is a billion-dollar industry serving our elder population,” says Deanna Cochran, RN. Cochran is the founder and CEO of Quality of Life Care, LLC, in San Marcos, Texas, an end-of-life training and certification agency. She’s also the first chair of the End of Life Doula Council within the National Hospice and Palliative Care Organization.
“The dying have specific needs and fears that need addressing,” she says. “As we evolve, the field is ripe for training people to be skillful at this — it’s a movement that’s growing. There’s plenty of room for every single hospice in this country to have at least one part-time doula. Within the next 10 to 15 years, opportunities will also become prevalent at nursing homes and assisted living centers.”
Fortunately, training is more prevalent now.
“There are over 10 certification programs, ranging in price from $700 to $2,500,” says Cochran, who offers a fast-track, 16-week program. “You can learn the skills, but you need to do the work by volunteering through hospice, nursing homes, hospitals. There’s an art to it.”
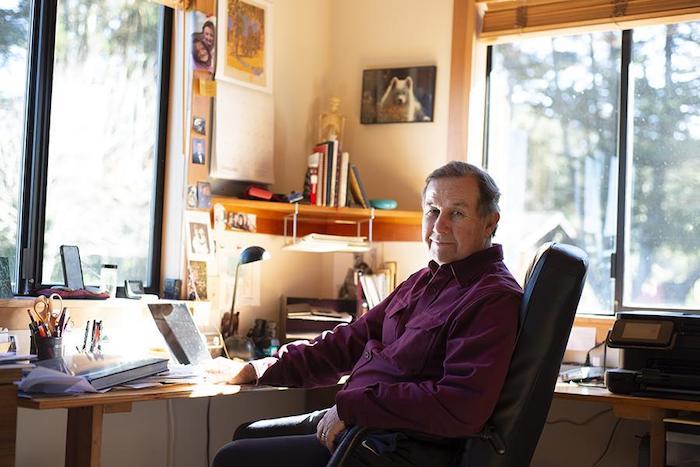
Dr. Steve Hadland learned over time to appreciate the “majesty and mystery” of death.
By Ellen Shehadeh
Dr. Steve Hadland began his medical career as an emergency room physician, fixing people and saving lives at all costs. These days he treasures his work as a hospice physician associated with Hospice of Petaluma, tending to the terminally ill and allowing them to die in comfort. Two extremes, one might say, but understandable given the intervening events in his life.
Steve’s practice melds a deep belief in social justice, reverence for life in all forms and enduring, self-described conservative views about end-of-life practices. His youthful face and genial manner, combined with an easy laugh and a soothing voice, belie the depth of his thinking, intellect and perceptions. He is informed not only by medical writings but also by psychology, literature, philosophy and classical music. One feels both calm and welcome in his presence.
Steve was the youngest in a conservative family growing up in Chicago. He attended university in Iowa City, studying astrophysics as a stepping stone to an astronaut program, and later majored in neuroscience. “University was a political and social awakening, as well as an intellectual one,” he says. He participated in marches and protests against the Vietnam War and for civil rights.
He longed to break out even further from his roots, however, and what better place than California, where “legend loomed for surfing and blondes.” He never quite managed the surfing thing, but wasted no time marrying his first wife, a blonde, during the summer of love, which coincided with his first year at Stanford Medical School. Their marriage of seven years included major involvements in the civil rights, anti-war and human potential movements.
All along, he had thoughts and profound feelings about end-of-life experiences, in part influenced by a Tolstoy novella, “The Death of Ivan Ilyich,” which he read in a death and dying course at Stanford. “It inspired me then, and continues to inspire me, year after year,” he says of the book, which he recommends “to anyone who really wants to know about what it’s like to die.”
Steve’s first job out of medical school, in 1972, was in a Kaiser emergency room. The nurses recognized his empathic nature and would steer the most difficult patients his way. Yet he recoiled at the Herculean efforts by staff to revive a dying patient, “all the excitement, the IVs,” and how quickly and “disrespectfully” staff abandoned a corpse when resuscitation efforts failed. At the time, there was no such thing as “do not resuscitate” or hospice.
Steve sought a different kind of medical experience and, in the fall of 1974, he arranged an interview with Dr. Michael Whitt in Point Reyes Station. He remembered the area from a drive many years before; “It cast a spell on me,” he says. Dr. Whitt’s liberal medical practice included home births, which at the time were popular in alternative communities, but Steve was stunned that he would deliver babies without liability insurance.
Steve’s conservative orientation and lack of maturity led him to decline a job offer by Dr. Whitt but, many years later, he would run a small integrative medical practice and pain management clinic out of his Point Reyes Station home. Ironically, he never secured liability insurance. “The influence of West Marin,” he quips.
Newly divorced in 1978, Steve encountered a single mother of three from Holland who was working as a Kaiser receptionist to pay her way through nursing school. They married two years later and, after 38 years, “it looks like it’s going the distance,” he says, laughing. Anneke van der Veen became an emergency room nurse, but they never worked together professionally, realizing the potential pitfalls of mixing business with pleasure.
Steve had traveled to England in 1978 to visit the first modern hospice. Although he was impressed with the approach, “I could tell I wasn’t ready for it,” he says. It was 12 years later that he helped start a hospice in Santa Clara, which he ran for five years along with an oncologist friend. He explains: “The world said, ‘You seem to be ready.’”
As society’s views about death and dying dramatically changed over the years, so clearly have Steve’s. Fifty years ago, death was a taboo subject and doctors rarely broached it with their terminal patients or even gave them an honest diagnosis. Now people take advantage of many choices, like refusing to eat and drink or using lethal medications now sanctioned by law. In California, the End of Life Option Act allows a patient to self-administer a lethal cocktail, but only after being judged by two physicians to be of sound mind and six months from death.
Some people object to the strictness of this law, which does not allow someone to assist in a patient’s suicide if the patient is physically or mentally unable to self-administer, even if it had been the patient’s expressed wish. In some states such assistance could be considered euthanasia or even murder.
Steve agrees with this self-described conservative view. “I don’t think it’s a bad thing; we don’t know what’s going on [inside their head]” or what kind of life these patients, some with Alzheimer’s and dementia, might have that we cannot fathom, he says. Surprisingly for a hospice worker, he was still opposed to the law when it was passed in July 2017, because “it’s a slippery slope.” How slippery? He cites a law in the Netherlands that now allows not only terminally ill patients but also depressed people to legally receive the fatal cocktail.
Steve explained that under California law, doctors may not legally list the cause of death as suicide when a patient has taken his or her own life. But the law “does allow a reference to the use of aid-in-dying meds as a contributing factor in the death, including the underlying fatal illness.” Steve, as a personal practice, does not include aid-in-dying medicines on the death certificate “to protect the patient from any backlash involving the choice of an induced death.”
Today Steve appreciates what he calls the “majesty and mystery” of death. Along with survivors, he participates in ancient rituals—“beautiful ceremonies” like washing and dressing the body—and finds it deeply humbling.
Steve is a spiritual man. He is influenced by the teachings of Jean Klein, a European who had an awakening in India. Although it is difficult to summarize Klein’s ideas, one important teaching is, “I am not identical with my thought process.” Steve believes that most of what one knows can be understood through other means, “coming from the heart and a sense of pure being.” This understanding has given him confidence to communicate with a dying person without words. “There is something in me that I know will make a difference. I am not anxious or worried, and am not in my head,” he explains.
About society’s recent openness to discussing death and dying, Steve cannot be more positive. It used to be, “If I don’t talk about it, it won’t happen.” The effect of the hospice movement has been to “lift the lid about frank, open discussions about death and dying. It helps people plan and frees them from living in a false reality, or a web of lies,” he says.
Naturally, one so intimate with death has opinions and thoughts about what awaits us all in the end. And what is the best death, to go quickly or to linger for a while? Not surprisingly, Steve believes that for himself, the ideal death would be when you know it is coming. “You get to finish your life, and say your goodbyes,” he says.
Steve also believes in a “continuity of consciousness.” This idea came to him intuitively years ago, after the death of his beloved dog, Misha, whose picture is prominently displayed on his office wall among other family photos. He tells this story, choking back tears.
“As I stood over the grave, I called out loud, ‘Where have you gone?’
A small voice inside asked, ‘Did you love me?’
‘Yes.’ ‘Do you still love me?’
‘Yes.’
‘Then that’s where I am.’”
Steve says, “My co-workers, patients and families living with the experience of dying have taught me much of what I know about love. Not the romantic love, of course, but something more encompassing, a feeling of compassion and connection with others that grows into this deep feeling of commonality and love.”
Meaghan Jackson has a surprising amount of insight into death and love for a 36-year-old.
“Working here, it’s changed me,” Jackson said from a wood-panelled room at the North Shore Hospice, where she has worked as a music therapist for four years.
“It’s completely changed the trajectory of my life.”
Meaghan Jackson is a music therapist at the North Shore Hospice. Jackson says working in palliative care has changed her life.
Jackson guides the residents at the hospice through their final days. She helps them write songs for their loved ones, and plays music for them as they take their last breaths.
Jackson has worked in “death and dying” since she was 22. She says her experiences prompted her to have children early in life, and focus on the present, no matter how difficult.
“I practice the art of being present when that present isn’t pleasant,” she said.
Health practitioners like Jackson say their experiences working with dying patients offer insights into love, relationships and how to focus on what matters.
A room at the B.C. Cancer Centre in Vancouver. Health practitioners say patients facing death tend to prioritize their relationships.
Each of the four practitioners interviewed for this story — a doctor, a social worker, a nurse and a music therapist — say dying patients tend to focus their energy and attention on the people they love.
Dr. Pippa Hawley, a palliative care doctor at the B.C. Cancer Centre, says she has seen couples and families reconcile after decades apart. She’s also seen several of her dying patients get married in the palliative care unit, sometimes in their beds.
Hawley says dying patients don’t have time to take loved ones for granted.
“All of that stuff that we bother with on a day-to-day basis just fades into irrelevancy,” she says.
Dying patients face many challenges with their partners, even when they prioritize love.
Melanie McDonald, a social worker who also works in palliative care at the B.C. Cancer Centre, says every couple she helps deals with death differently.
Couples who thrive during difficult moments are often those who can balance sadness with joy and love, she says.
Social worker Melanie McDonald says couples face many challenges when faced with death.
Nurse Jane Webley, who leads Vancouver Coastal Health’s palliative care unit, says the strongest couples are best at honestly communicating their needs, feelings and end-of-life plans.
Webley says patients who find it too difficult to discuss those matters are often the same ones who push loved ones away and face death alone.
“I think that’s a protection mechanism,” she said. “I would say 90 per cent of the time, it’s fear — and that fear is brought about by lack of communication.”
Dr. Hawley says some of her patients are never able to communicate their feelings and needs. Often, she says, that’s been a long-standing issue for them.
“People tend to die as they have lived,” she said.
Talking about death and end-of-life plans is often easier for older couples who are often more in touch with mortality. But Webley says it’s never too soon to have those difficult conversations.
Another challenge couples face when one is dying is learning to give or receive help, health practitioners say.
Social worker McDonald says people who aren’t used to being caregivers, typically men, often struggle when they’re suddenly thrust into that position. But most people learn to take on that role, she says.
Health practitioners say that learning to ask for help can be a steep learning curve for some patients.
Dr. Hawley says patients can face problems as they lose their independence. But she says it’s important for people to let their partners care for them.
“Don’t feel like you’re a burden,” she said. “It’s actually a wonderful gift to be allowed to care for somebody, to show them that you love them.”
All four of the health care practitioners say love at the end of life can take many shapes.
“Love looks differently in different situations,” says social worker McDonald. “Love shows up in the end of life in friendship and in families and pets and faith traditions and all sorts of different ways.”
Dr. Susan MacDonald reflects on ‘Leo’ and whether she should have told him about assisted death
Dr. Susan MacDonald, a palliative care doctor in St. John’s, wonders if more could have been done for her patient ‘Leo.’
By Ariana Kelland
Susan MacDonald can’t quite pick one reason why Leo sticks with her, pushing her to put pen to paper to tell the story of her patient, and how she feels she failed him.
Asked what sets Leo — a pseudonym — apart from the rest, the palliative-care doctor shakes her head and sets her gaze away, “About Leo … I think, for one, I really liked him. I just really liked him.”
The second fact, MacDonald said, is that his death — suicide by taking his own opioids for insufferable pain — was not his only option.
Medically assisted death would have allowed Leo to die without having health-care professionals standing over him in a fruitless attempt at reversing his overdose, she said.
“He was such an intensely private person and his death was so public, and it didn’t need to be that way,” MacDonald said. “There were options. It just really struck me and made me think.”
MacDonald, an associate professor of medicine and family medicine at Memorial University of Newfoundland, reflected on her patient and what she could have done differently, in an article in the Canadian Medical Association Journal, titled Leo Died The Other Day.
The patient died within the last couple of years, MacDonald said, unable to comment further due to physician–patient confidentially.
To raise — or not to raise — the option of assisted dying
For five months, she and Leo worked hard to control his intense nerve pain. But Leo’s death was inevitable. He had cancer, and by MacDonald’s estimation, had only weeks — maybe months — to live.
Whether it was the physical pain that became too unbearable or the emotional struggle of his impending death, MacDonald doesn’t know why he took his own life.
“It was a very distressing clinical case for me because I felt, at the end of the day, I hadn’t done the best I could for this particular patient,” MacDonald said.
“It was a reflective exercise for me to look back and say, ‘What could I have done better? Where are the problems? And what do we need to do about it?'”
MacDonald said she never raised medically assisted death as an option for Leo. Neither did he. But she wonders if some patients want to bring it up but can’t.
Medically assisted death in Canada is legal. However, MacDonald said, there are no strict guidelines on how a doctor should broach the topic with a patient.
Changing the way she does things
Until Leo’s death, MacDonald would wait for the patient to bring it up, but the manner in which he died has her pausing for second thought.
“There may be people like Leo, who could avail of that option if they knew about it or if it was offered to them,” she said.
“On the other hand, you have the potential to do harm by raising that question,” she said, adding doctors run the risk of offending patients by even mentioning assisted dying as a option.
Medically assisted death is legal in Canada. However, there are no strict rules guiding how physicians should broach the topic with patients.
“I’ve been doing this for 25 years now, and I still haven’t figured out always the right thing to say and the right thing to do for people.”
MacDonald hasn’t gotten many more inquires about medically assisted death since it was legalized, she said. “Not nearly as many as you’d think.”
Now, as she continues caring for those whose deaths are inescapable, she has Leo to think about.
In 2016, a small group of doctors gathered in a Seattle conference room to find a better way to help people die. They included physicians at the forefront of medical aid in dying—the practice of providing terminal patients with a way to end their own life. And they were there because the aid-in-dying movement had recently run into a problem. The two lethal medications used by most patients for decades had suddenly become either unavailable or prohibitively expensive. When doctors briefly tried a substitute, some patients had rare but troubling experiences.
The Seattle group hoped to discover a different drug. But the practicalities of aid in dying, a controversial policy still illegal in most of the United States, are not like those in other medical fields. “There’s lots of data on stuff that helps people live longer, but there’s very little data on how to kill people,” says Terry Law, a participant at the meeting and one of the most frequently used aid-in-dying doctors in the U.S.
Seven states—including Hawaii, where a law took effect on January 1—and the District of Columbia now allow doctors to write lethal prescriptions for qualifying, mentally capable adults who have a terminal illness. And support for the practice has gained new national momentum after the widely publicized death of Brittany Maynard, a young cancer patient who moved to Oregon in 2014 to take advantage of that state’s aid-in-dying law.
But the public remains deeply conflicted about the laws—as does the medical community itself. No medical association oversees aid in dying, and no government committee helps fund the research. In states where the practice is legal, state governments provide guidance about which patients qualify, but say nothing about which drugs to prescribe. “Nowhere in the laws is there any sort of guidance for how to do it. There is no oversight to make sure that it’s happening in a safe way, apart from annual reports and kind of a face-value annual hearing,” says Laura Petrillo, a palliative-care physician who opposes legalized aid in dying.
The meeting of the 2016 group set in motion research that would lead the recipe for one of the most widely used aid-in-dying drugs in the United States. But the doctors’ work has taken place on the margins of traditional science. Despite their principled intentions, it’s a part of medicine that’s still practiced in the shadows.
On the surface, figuring out protocols for hastening death doesn’t seem complicated. Lonny Shavelson, a California physician who specializes in aid in dying, says that when he explains to patients it might take an hour or more for them to die, they’re often shocked. They tell him, “When I put down my dog, it took 10 minutes,” he says.
But veterinarians can use lethal injections on pets. In the U.S., aid-in-dying drugs must be ingested by the patient. The first proposed aid-in-dying law in Washington State would have allowed physicians to inject medications, but that legislation failed to pass. In 2008, a modified law was voted in, with an added requirement that patients self-ingest to help protect them from the possibility of family coercion.
For years, the two barbiturates widely considered the best drugs for hastening death in terminally ill patients were secobarbital and pentobarbital. These medications were painless, fast-acting, and relatively affordable. But since 2015, they’ve been largely unavailable. U.S. pharmacies stopped carrying pentobarbital approved for human use, and the price of secobarbital doubled from an already historic high after Valeant Pharmaceuticals (today known as Bausch Health) bought the manufacturing rights. A few years ago, a lethal dose cost about $200 or $300; now it can cost $3,500 or more.
To help patients who could no longer afford the drug, aid-in-dying groups sought a fix. In Washington, an advocacy organization called End of Life Washington briefly advised prescribing a drug mixture with the sedative chloral hydrate to about 70 patients. “We know this is going to put you to sleep, and we’re pretty sure it’s going to kill you,” Robert Wood, a medical director at the organization, says they told the patients. It worked, but with a tragic catch: In a few cases, the chloral hydrate burned people’s throats, causing severe pain just at the time they expected relief.
The End of Life gathering was born out of the need for a better solution. Wood enlisted three others affiliated with End of Life Washington: Law, its president; Tom Preston, a former medical director; and Carol Parrot, a retired anesthesiologist who, like Law, is one of the most experienced aid-in-dying doctors in the U.S. Others joined that meeting or later ones by telephone: a toxicologist in Iowa, a veterinarian, a pharmacologist, another anesthesiologist. The group had three main criteria, Parrot says: They wanted “a drug that would: number one, put a patient to sleep and keep them asleep; and, number two, make sure there was no pain involved; and number three, ensure that they would die, and, hopefully, die relatively quickly.” Plus, it had to be cheap. They aimed for $500 a dose.
The doctors considered a malaria medicine known to be lethal in large doses, but read that it caused severe muscle spasms in some patients. They discussed the synthetic opioid fentanyl, but were deterred by the drug’s newness and dangerous reputation. So the group decided to use a combination of medications, and eventually settled on high doses of three: morphine, diazepam—also known by its early brand name, Valium—and propranolol, a beta-blocker that slows the heart. They called the mixture DMP.
Next, the group had to test the drug. But they still didn’t have a way to follow standard procedure: There would be no government-approved clinical drug trial, and no Institutional Review Board oversight when they prescribed the concoction to patients. The doctors took what precautions they could. Patients could opt in or out, and for the first 10 deaths, either Parrot or Law would stay by the bedside and record patients’ and families’ responses.
The first two deaths went smoothly. But the third patient, an 81-year-old with prostate cancer, took 18 hours to die, Parrot says. In Oregon, where aid in dying has been legal for 20 years, the median time from taking the medication until death is 25 minutes. Patients themselves typically become unconscious in five or 10 minutes, so they are not affected by protracted times, Parrot, Wood, and Law all emphasize. But longer waiting periods can be nerve-racking for families and other caregivers, especially in the exceptional cases where these have persisted for a day or more.
Parrot and Law halted the DMP trial. The informal research group met again, this time by teleconference, and Law dug through the literature and found an article about people who purposely overdosed on digoxin, a cardiac drug. The group added it to the prescription, and the drug became DDMP.
At first, Parrot gave patients latitude in how they took this new drug combination. “One guy chugged a half a cup of Bailey’s Irish Cream, his favorite thing, after he had his medicine,” she says. “He probably took five or six hours to die.” She suspects that the fat particles in the Bailey’s slowed his gastric emptying. So the researchers checked in with each other again, and decided to increase the doses to what Parrot calls “blue-whale-sized doses.” They dubbed the modified formula DDMP2.
The drug is not a perfect aid-in-dying solution. Secobarbital is faster-acting and remains the drug of choice when patients can afford it, Wood says. Just as in the case of the barbiturates, a few outlier patients on DDMP2 take hours longer to die. And the mixture tastes extremely bitter. “Imagine taking two bottles of aspirin, crushing it up, and mixing it in less than half a cup of water or juice,” Parrot says.
Still, DDMP2 has become the low-cost solution the Seattle group set out to discover. In 2017, secobarbital was still the most commonly prescribed drug in Washington and Oregon, but in Colorado, DDMP2 was more commonly prescribed. The drug consistently accomplishes its purpose in hastening death, Parrot says: “It always works. It always, always works.”
Parrot and Wood keep track of patient data, and they continue to make discoveries. By examining medical histories of the patients who took longer to die, they’ve learned about certain risk factors for longer deaths: being on extremely high doses of painkillers such as fentanyl or morphine; being very athletic; having a compromised digestive tract. For patients who are especially risky, Parrot or Wood will sometimes offer the choice of chloral hydrate, the drug that burned some patients’ throats, although they say they carefully discuss potential problems with patients and families.
Together, Parrot and Law have written perhaps 300 lethal prescriptions over the years and observed the effects of medications on numerous patients. Neither set out to be an aid-in-dying advocate; they turned to End of Life Washington after witnessing the suffering of some dying patients. About eight years ago, Law says she was asked to prescribe lethal medications for a dying woman whose regular doctors had refused. She agreed to see the woman, and realized how difficult it was for some aid-in-dying patients to find doctors. Parrot says she was profoundly affected by the deaths of two close friends who asked her to help hasten their dying, but who lived in states where the practice was illegal. She was unable to help them, and began volunteering as an aid-in-dying doctor soon after she retired.
Most medical professionals don’t participate in aid in dying. Some physicians are concerned that their Hippocratic oath prohibits intentionally helping someone die, or that aid-in-dying requests originate from treatable pain or depression. Some worry about the broader repercussions for a society that accepts medically aiding the deaths of the terminally ill. The American Medical Association remains officially opposed.
Without the support of the rest of the profession and much of society, aid-in-dying research methods don’t fit the model of good medical research, says Matthew Wynia, the director of the Center for Bioethics and Humanities at the University of Colorado. There’s no standard protocol, no standardized data collection or independent group that monitors data and safety—all of which are intended to protect patients and help ensure the quality of the research.
The Belmont Report, which guides federal recommendations for research on human subjects, recognizes that sometimes, no satisfactory options exist for some patients, Wynia points out. In those rare cases, a doctor may want to try an innovative treatment, something for which there’s no approved research protocol. While that’s legal, clinicians are supposed to avoid turning that innovation into established practice, or doing unapproved research on numerous patients, according to Wynia. Some of the same issues exist with medical marijuana, which is legal in several states but still illegal federally. “There’s no way to fix this at the individual level,” Wynia says. “There’s no immediate answer.”
That leaves researchers like Law and Parrot in a bind. They don’t have good ways to do research and communicate what they learn. But they’ve witnessed the suffering some dying people experience, and contrast that with many peaceful deaths of patients who choose aid in dying. “These are not hard deaths,” argues Shavelson, the California physician. “These are lovely deaths.”
Shavelson says he tries to be at the bedside on the day of his aid-in-dying patients’ death. “It’s a lighter atmosphere than you think,” he says. The patient takes the first drug, which Shavelson separates out from the rest of the mixture, and then Shavelson sits down at the bedside and reads aloud questions from the state’s required report. After about 30 minutes, he asks: “Are you ready to take the medications?” He mixes the drug cocktail and the patient drinks it.
“Usually, they go silent after taking the medication,” he says. “They’ve said what they’re going to say by that time.” For a few minutes, patients usually continue to sit silently, their eyes open. “And then, very, very slowly, they’ll close their eyes.”
Shavelson asks intermittently, “Are you still there?” At first, patients usually say yes, or nod. Within five or 10 minutes, they stop responding to the question. Then Shavelson will gently touch their eyelids. “When people aren’t deeply unconscious, they’ll sort of have a twitching response,” he explains. Within 10 or 15 minutes, the twitching response disappears, and patients enter a deep coma.
Using a heart monitor, Shavelson tells caregivers as a patient’s pulse slows and oxygen levels drop. “We wait a little while, and then I say, ‘Ah, the patient’s now dead.’”
This is the first generation of patients who have consciously hastened their death with medications in this way, Shavelson says. He tells them they’re pioneers. “What a different thing, to be able to say, ‘This is the day I die,’” he says.
Nursing requires hands-on training. But research has found that university curriculum often goes light on one of life’s universal experiences — dying. So some colleges have gone to new lengths to make the training more meaningful.
There’s a sound near the end — the death rattle. People stop swallowing. The lungs fill up. There can be involuntary moaning.
“So you get all that noise. And that’s really distressing for family members,” Professor Sara Camp of Nashville’s Belmont University says.
Camp and other nursing instructors at Belmont wear headsets and watch video monitors in a dark closet. The sounds they make emerge from realistic robots lying in hospital beds on the other side of the wall. The instructors also control the stats for the robots’ breathing, pulse and blood pressure.
Other than administering morphine, there’s no exact prescription for students to follow. A review of nursing textbooks found many make no mention of this standard part of the job. And studies of professional nurses find that many feel unprepared.
Belmont adjunct nursing instructor Morgan Bryant mimics the “death rattle” in her headset, also controlling the pulse, breathing and blood pressure of the simulated patients in the lab.
“They’re really comfortable in their skills, like putting in IVs and giving medications,” Camps says. “In this one, they have to focus on communication, when there’s not that much to do. It challenges them.”
There are family dynamics to navigate, like explaining to grown children how their mother signed a do-not-resuscitate order. They have to balance caring for the dying patient and attending to the patient’s family.
In response to surveys showing anxiety about death among young nurses, Belmont started hiring actors to make these end-of-life interactions as realistic as possible.
“That old cancer … didn’t want it to come back,” says Vickie Bailey, who has embraced her role as a grieving daughter.
The student, senior Sara Lindsay, sits on the bedside and puts a hand on Bailey, warning that the end is near.
“Now would be a good time if you have prayers or anything you want to say,” she tells Bailey.
“I’ve been praying all morning,” Bailey responds, in character.
The monitors stop beeping. Everyone sits in silence.
Once the simulation ends, Lindsay marvels at how real the moment felt.
Half a dozen beds are going at the same time in this simulation lab. And all the students gather to debrief afterward. Senior Zacnite Vargas volunteers that she second-guessed herself.
“Should I say she’s dying? She’s dead? She’s passed?” she asks. “I don’t know how to be straight-forward with it.”
Camp tells the class to be cautious, especially about predicting when a patient will die, but also show compassion.
“They may not remember what you say, but they’ll remember how they feel when you were there, because you were there.”
It’s such important work, Camp says, that more students should get the chance to rehearse.