Mario Fonovic seated in the palliative care ward of the Queen Elizabeth Hospital.
At 55 years of age Mario Fonovic is in the final stages of terminal lung cancer. He doesn’t expect to see the end of 2016, but he is refusing to go without a smile on his face.
Mr Fonovic joined the program to discuss a topic most people dread — death.
“I’ve arranged my funeral right down to my flowers — but don’t bring tissues, bring a tambourine,” he said.
Mr Fonovic said he was neither sad nor scared of his approaching death, and had decided to share his journey on Facebook.
“I can see what is happening to my body,” he said.
“I feel it, I can see it and eventually I will end up in a coma.
“If I can help one person accept death or dying or cancer [I will].
“Just accept what is happening in your life and get on with it, because life is short.”
Looking back on his life, Mr Fonovic said he wished he had only done one thing differently.
“My one and only regret is that as a gay man I never fought to have a child,” he said.
Mr Fonovic said he was lucky to have legally married his partner Sid in a ceremony in California before legislation there changed.
The two plan to move into a newly purchased home together this week and Mr Fonovic is determined he will not die in a hospital.
Too many hospital visits
Mr Fonovic has spent his fair share of time in and out of hospital since being diagnosed with asthma eight years ago.
Being a long-time smoker only made his condition worse.
“Four years ago I coughed … after having one of my last cigarettes and blew a hole in my left lung,” Mr Fonovic said.
His left lung had deflated and he struggled to breathe.
After a week in hospital being treated he was sent home, but within six hours he was back in the emergency department — his left lung had deflated once more.
After another round of treatment Mr Fonovic’s life began to return to normal.
Eighteen months later Mr Fonovic was back in hospital — this time his right lung had collapsed.
“I ended up looking like the Michelin Man as air was leaking into my body,” he said.
He was placed in intensive care and surgeons removed a third of his right lung.
In December 2015 Mr Fonovic visited a respiratory physician to check whether he would be suitable for a lung transplant.
Mario Fonovic having his chest scanned
During a routine scan the doctor discovered cancer.
“I was so happy the day that I went on the transplant list … because I wanted my life back,” he said.
“In one breath I went, ‘yes’ — and then it was cancer.”
Getting on with it
A burst of stereotactic intense radiotherapy saw Mr Fonovic end up with an infection and he was once more admitted to hospital.
“On the second of May [my doctor] shook my hands and said, ‘you are in remission’,” Mr Fonovic said.
“In the following week I went downhill to the point where I couldn’t walk down my hallway.
“I felt like a semi-trailer had parked on my chest.”
Three weeks later Mr Fonovic admitted himself into hospital for a follow-up scan and found out the cancer had returned.
“The PET scan actually showed how bad it is,” he said.
“Not only had I got the cancer back, but it had taken over the whole lung.”
The lymph nodes on the side of his lungs had stimulated the nerves on his spinal cord and were causing him immense pain.
With the firm belief he would not see his next birthday, Mr Fonovic said he decided all he could do was face death.
“You just put your feet on the side of the bed, pull your trousers on and get on with it,” he said.
The cancer may have wreaked havoc on Mr Fonovic’s body, but mentally he is nowhere near finished with life.
‘Cohen’s economy of words, the syntax of love, his ability to go straight to the only matter that matters – her death, his mortality, their love – is a thing of beauty and wisdom.’
The songwriter’s letter to Marianne Ihlen in her last hours was beautiful, poetic and to the point. Yet so often we deal with death in an inane, mawkish way
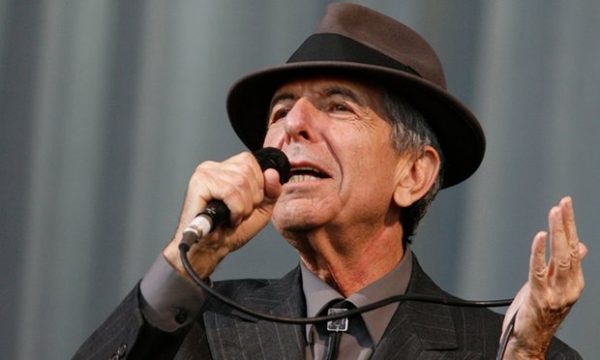
A short goodbye. A few sentences. But words of such clarity, simplicity and beauty. Many of us have by now read Leonard Cohen’s letter to a woman he once loved, Marianne Ihlen, on her deathbed – and those who didn’t know it already have seen that Cohen is a class act, a man you don’t meet every day.
He heard that she was dying and two hours later he wrote to her that he too was old and his body failing. He had, of course, written for her before, with the lyrics of So Long, Marianne and Bird on the Wire. This time he told her: “Know that I am so close behind you that if you stretch out your hand, I think you can reach mine.”
Slipping into unconsciousness, her friend said that Marianne did reach out her hand. Cohen’s letter also stated that he didn’t need to talk about her beauty and her wisdom, “because you know all about that”. The 10 years they were together on and off, their intimacies, their passions, their endings, those – despite the songs – are all a part of their own personal story. Now he wishes her endless love on her journey – to death. It is everyone’s journey, but few speak so directly of it, not even while whispering in the waiting rooms.
Was Marianne his greatest muse? What does it matter? He loved her for a while. He loved his four bottles of wine a day before he took himself off to the Buddhist monastery where he was given the Dharma name of Jikan which means “silence”. But he knows about silence as he also knows about the tower of song.
Death is so often met with silence or with sentiments that are an inane babble to fill a void. The mawkish inscriptions and epitaphs seek to cauterise the grief, to fix it for a while. For how to write of loss? How do you write to a person you will never see again? I have done it, clumsily, inelegantly, with false jauntiness and then a wish for them to rest. Whatever that means.
So Cohen’s economy of words, the syntax of love, his ability to go straight to the only matter that matters – her death, his mortality, their love – is a thing of beauty and wisdom in itself. His ever deepening voice, the self-mockery, to see him now deadpan and dapper is still quite something. But once she held him like a crucifix and he let her go: “I’m cold as a new razor blade,” he sang.
Some think of him as a doom-monger but he is deadly funny and the faith was always there. “I think I was touched as a child by the music and the kind of charged speech I heard in the synagogue, where everything is important,” he said in his eighth decade, adding ironically that he was singing “a lot of Jew-sounding songs in different keys”.
Yet it is the fact that his words are so charged that is the reason they touch us. In my local park, there is an inscription on a bench for a friend who died and the words are taken from So Long, Marianne: “It’s time that we began to laugh and cry and cry and laugh about it all again.”
Cohen once said: “Poetry is just the evidence of your life. If your life is burning well, poetry is just the ash.” What ash though? Warm, sacred, dancing us to the end of love; young passions, old bodies, a rare and gracious farewell. So long, Marianne. Thank you, Mr Cohen.
Veterinarians say that helping suffering animals and stressed-out owners can become grueling.
When I walked dogs at a Chicago animal shelter, I wondered how each one got there. Whether a stitched-up pup shirked from my touch or happily greeted me tongue-first, my eyes would well up with salt. I wanted to keep them all.
People who work in animal shelters or veterinary clinics try to save the animals that come through their doors. But they’re at high risk of compassion fatigue, a sustained stress that takes a toll on a caregiver’s mind and body — and her heart.
It can morph into many forms: Some feel guilt or apathy, others turn to substance abuse. Little data exists, but research suggests veterinarian suicide rates are some of the highest in the medical field, and a 2014 study of about 10,000 veterinarians found twice as much “severe psychological distress” in them than in the general public. One 1 in 6 veterinary school graduates say they have considered suicide.
People in the animal community know this is a risk, and they have stories of people they’ve known who have taken their lives.
Among the biggest strains for animal shelter employees is euthanasia, according to a 2009 study published in the Journal of the American Veterinary Medical Association. Derived from Greek terms that mean “good death,” euthanasia is viewed as a humane way to end an animal’s life by organizations including the American Veterinary Medical Association and PETA.
Though rates of animal euthanasia have sharply dropped in the last few decades, about 3 million cats and dogs are estimated to be put down every year. When faced with alternatives like neglectful owners or living on the street, a peaceful death might be the most merciful option, says Stephany Lawrence, a former shelter intake and adoptions manager in Denver. Shelter life can be scary, even detrimental, especially if the animal is ill or has a behavioral issue.
“Nothing is worse than killing an animal, but it’s a really, really compassionate process,” Lawrence tells Shots. The euthanasia is quick; the employees are tender. But the grief of a life extinguished and the suffering that preceded it can linger. “What I struggled with was how anyone could give up a pet or treat animals as disposable items,” she says. “And I actually think that’s probably something shelter workers have a hard time with, as much, or even more so, than euthanasia.”
Private animal hospitals practice euthanasia, too, but there the patient is often a beloved pet. And veterinarians and staff have to manage both the end of the animal’s life and the humans’ grief.
On some days, the tide of clientele truncates how much time and compassion a doctor can give a dying patient or an owner trying to cope. That’s when the fatigue rears for Krista Magnifico, a veterinarian in Jarrettsville, Md., who writes a behind-the-scenes blog “You feel guilty because you’re not there for them in the capacity that you want to be,” she says.
Veterinarians and rescue workers face another challenge: stressed out and even hostile humans. One reason is cost. Veterinary care can be very expensive, even with insurance, and financial constraints can lead to tense situations. If they escalate, stepping out for a breather or bringing in another staffer can help. Sometimes, conflicts escalate to the point where a clinic has to call the police.
Magnifico won’t turn away clients who love and want to help their pet. But if they’re not empathetic to the animal, or the relationship has fractured and no longer benefits the pet, she’ll suggest alternatives, like seeing another clinic. “I have to be very true to the core of who I am,” she says. “And with that, I know that I’m not a veterinarian for everybody.”
Once someone brought in a dog with a bone tumor in its leg. To relieve the pet’s pain, a staff member at Magnifico’s clinic advised that the limb be amputated. But the owner declined the procedure, tied the dog to a tree in front of the clinic, and left.
Sometimes clients ask for convenience euthanasia. Other times, owners threaten to kill the pet themselves. In those cases, the people at the end of the leash cause the most distress for animal shelter and clinic employees.
“The rhythm of a healthy life is fill up, empty out; fill up, empty out,” says Patricia Smith, founder of the Compassion Fatigue Awareness Project, which aims to help caregivers learn healthy forms of self care. But caregivers tend to spend their empathy on everyone but themselves, and they forget to refuel. “The result of that is we have nothing left to give,” Smith says. “We give from a place of depletion instead of abundance.”
“One of the hallmark signs of [compassion fatigue] is that you cannot undo what you’ve been exposed to, and your worldview is forever changed,” says Elizabeth Strand, founding director of the University of Tennessee’s veterinary social work program. Strand noticed a huge need in the veterinary environment for social work, and Tennessee was the first school in the country to create a specialty in veterinary social work. Michigan and Missouri now offer similar programs.
Veterinary social workers provide support for animal-related professionals who need an extra hand resolving stress or stubborn conflict. They can also gently guide grieving pet owners through heartbreak, or help figure out what to do when an animal is a victim of family violence.
Strand and others say that veterinary professionals are becoming more willing to talk about the mental health stresses of their work, and veterinary schools are addressing mental health and emphasizing communication skills.
To bolster resilience, students at Cornell University’s College of Veterinary Medicine participate at the teaching hospital as early as their first year, so that they’re accustomed to working with very sick animals and distraught owners. Students can also staff the school’s pet loss support hotline after special training.
The veterinary school at University of California, Davis, has one full-time counselor and one part-time counselor just for veterinary students. “As our counselor started getting busier and busier, we thought that we had a problem, and what we realized is that this was not a problem,” says Dr. Sean Owens, associate dean for admissions and student programs at Davis’ School of Veterinary Medicine. “We’re actually doing a better job of destigmatizing talking to mental health professionals, meaning that our students are now more likely to drop in and say, ‘I just spent four hours grieving with a client … How do I process it?’ ”
The Davis program provides yoga, art projects, massage therapists — even a surfing club. Clinical skills labs that use actors who practice common scenarios, though awkward, can lift confidence later. The school was the second veterinary school after Colorado State University to offer a “healer’s art” course, which embraces the emotional aspects of practicing medicine.
“What has really triggered [change] has been the greater publicity of suicides of veterinary students,” says Owens. “You’re not fully complete in this profession unless you’re able to grieve and be a human.”
Leroy Blast Black was a loved man, that we can boldly affirm. We did not know Leroy blast Black, dubbed “Blast,” gone too soon at the tender age of 55, but obviously he was well surrounded during his illness.
Mr. Black died Tuesday at his family home in Atlantic City as the result of lung cancer “due to exposure to fiberglass.”
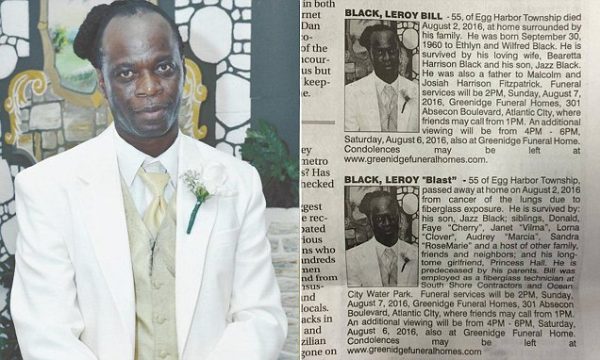
However, the most intriguing fact about the death of Mr Leroy Blast Black is the fact that two obituaries were printed in today’s Press of Atlantic City.
Indeed, it might have looked like a mistake on the obituary page this morning when two identical-looking (at first glance) listings appeared on top of one another, but the two different, but similar, obituaries were placed by his wife and girlfriend, respectively.
The one from the wife reads:
Black, Leroy Bill – 55, of Egg Harbor Township died August 2, 2016, at home surrounded by his family. He was born September 30, 1960 to Ethlyn and Wilfred Black. He is survived by his loving wife, Bearetta Harrison Black and his son, Jazz Black. He was also a father to Malcolm and Josiah Harrison Fitzpatrick…
The one from the girlfriend follows:
Black, Leroy “Blast” – 55 of Egg Harbor Township passed away at home on August 2, 2016 from cancer of the lungs due to fiberglass exposure. He is survived by: Jazz Black; siblings, Donald, Faye “Cherry,” Janet “Vilma,” Lorna “Clover,” Audrey “Marcia,” Sandra “RoseMarie” and a host of other family, friends and neighbors, and his long-tome (sic) girlfriend, Princess Hall…
Our colleagues at Philly Voice called the Greenidge Funeral Home, and the person that answered clarified: “The obituaries were placed separately because “the wife wanted it one way, and the girlfriend wanted it another way.” But he did not anticipate any problems because everybody knew it was happening.”
NBC News tried to reach the wife and the girlfriend but without any success.
Joseph Greenidge Jr., the funeral director at Greenidge Funeral Homes, told KYW Newsradio in Philadelphia it isn’t unheard of for there to be multiple obituaries written from different perspectives. But, he said, they took direction from Leroy’s wife regarding the funeral arrangements.
Although you might feel like you’re going to die if that bartender doesn’t get you a beer right now, this isn’t exactly a dire situation. What is, however, is if you’re faced with a real life or death scenario. In these cases, most people panic, and not hyperbolically.
That’s why we spoke to seasoned ER guru Dr. Ryan Stanton (and spokesperson for the American College of Emergency Physicians), who faces life or death situations every single day he goes to work. He’ll teach you how to keep cool if you ever find yourself in such a predicament.
Prepare for any situation
You can’t possibly prepare yourself for all circumstances, since we’d all be pretty screwed if some Leftovers-type stuff went down, but first aid training goes a long, long way. Hit up your local fire department, American Red Cross, or hospital for a basic first aid class, which will help you help others when it matters most. You’ll learn how to give non-creepy, hands-only, live-saving CPR that doesn’t require you to basically tongue kiss a stranger, plus super useful skills like what to do when someone’s choking, and how to stop major bleeding. And you can also learn how to shock someone’s heart using an AED machine if they go into cardiac arrest.
Know you don’t always have to do something
Even if you’re prepared, know your limitations, because sometimes doing very little is the best possible thing. Let’s say you come across a car wreck, and someone is badly injured. As Dr. Stanton explains, just being there is good enough: “Sometimes the best thing you can do is call 911 and talk to the person,” he said. “Give them comfort.” If the person in the crash is already bleeding badly, any stress on top of that will make them “more likely to have complications.”
And to further hammer home the point that real life is not like being in a hospital drama on TV, you don’t have to be a hero and save everyone. So if you see someone having a seizure, outside of “keeping [the person’s] airway open,” (a technique you learn in basic first aid!), your job is to sit there and wait for EMS to arrive. “People feel like they have to do something,” Dr. Stanton said. “They try to shove stuff in the person’s mouth to keep them from breaking teeth, or put their fingers in their mouth to keep them from swallowing their tongue. And then you just end up with two people hurt instead of one.”
Prioritize, prioritize, prioritize
When someone comes into the ER with a problem, Dr. Stanton asks himself the same question: “What’s going to kill them first?” Probably that hospital food, says every comedian from the ’80s. But if that person is not bleeding to death and is breathing fine, then Dr. S has bought himself enough time to figure out what to do next.
By way of example, let’s go back to our imaginary person in a car crash: Dr. S says some newbie doctors can get distracted by the victim’s nasty-looking sideways ankle and not realize that they’re also not breathing. Prioritizing allows you to focus on what’s critically important at the moment. You can only do one thing at a time.
Know that sometimes there are no solutions
Everyone knows they’re supposed to calm down in a stressful situation, but it’s not just about taking a few deep breaths (though you should also do that). “Panic has never fixed a problem,” Dr. Stanton said. “Fixing a problem involves working through what you know — if it’s not part of what you know, find the people who know it.” If someone else can’t help, perhaps there are no solutions whatsoever to the super stressful, life-threatening situation you find yourself in. “[Sometimes] you can’t change the current situation,” he said. “All you can [affect] is what’s going to happen now and moving forward. Stay calm and think about what you can do [next].”
Gain confidence through education, experience
ER doctors stay calm while saving lives everyday, and they’re able to keep cool by relying on a combination of experience and education. Now, outside of being that guy in Catch Me If You Can and impersonating a doctor to gain some life-saving experience, first aid training will suffice.
Dr. Stanton put said experience to work one Sunday outside of the ER, when someone passed out behind him in church. While other people were freaking out, Dr. Stanton followed his own advice and everything turned out fine.
Other, non-passed out churchgoers were concerned that the unconscious person didn’t have a strong pulse, and that it was imperative to check their sugar. But Dr. S knew the best move in this situation — make sure the victim was breathing and stay there until EMS arrived. And to stay calm. In a hospital, “if the doctor is calm and relaxed, the whole [ER] is calm and relaxed and everyone does their job.” Be the calm one in any life-threatening situation you encounter, and you’ll do just fine.
Craig Phillips has found that his work as a death doula has given him a greater appreciation for life.
Before he enters the room, Craig Phillips pauses for a deep exhale.
“Just to let everything go,” he says. “And to remember that I’m here for them.”
Until he walks in, he won’t know whom, exactly, he’s about to see. Today it’s an elderly woman in a blue hospital gown. Eyes closed. Jaw dropped open. Breathing loud and labored, but regular.
There is a little green circle by her name on the white board in the nurses’ station. Hospice center code for “actively dying.”
“She doesn’t have anyone with her,” a nurse says. So Phillips goes, pulls a chair up to her bed and introduces himself.
“I’m not here to poke or prod you,” he says softly. “I’m just here to be with you. I’m just here to sit with you.”
The work of a death doula — Phillips’s work, now — is primarily about presence. He is there to ease the passage from this world to the next. And he knows that the most valuable thing he can offer anyone taking that most solitary of journeys is his company. So he sits, silently wishing them peace and comfort.
Especially with patients who can no longer speak, Phillips has learned to slip his hand beneath theirs, palm to palm, rather than rest it on top. This way, he says, “you get an understanding of how well wanted you are.” When his grip is returned, he knows that he is welcome.
Phillips operates alone, but he is part of a growing army of volunteers and professionals who call themselves death doulas. (Some, opposed to that term, prefer end-of-life doulas, soul midwives or transition coaches.) And like the childbirth doulas from whom they draw their name, their mandate is to assist and accompany. Their patients’ experience may be quieter, more sorrowful, but it is no less sacred. Or scary.
As the baby boomers move into retirement, fresh consideration is being given to what it means to grow old, which measures to take to treat illness and, ultimately, how we die. There’s a growing recognition among hospice workers and palliative-care givers that pain management is not enough. That the spirit must be attended to as much as the body. And that the soon-to-be-bereaved need help along with the dying.
It’s out of this recognition that death doulas are emerging. Most say they feel almost inexplicably called to the role. And profoundly touched by it.
A good death
On a sunny spring day in Alexandria, Virginia, 30 women and one man sit in a windowless hotel conference room, having traveled from all over the East Coast and paid $600 to learn to serve as death doulas.
“Our role is to walk alongside” the dying “in their journey,” says Henry Fersko-Weiss, president of the International End of Life Doula Association (INELDA), one of several organizations offering certification in the field.
The weekend-long training will cover the best ways to touch a dying person, when to use aromatherapy and guided visualizations, strategies to relieve overburdened family members, how to organize a “legacy project” to help capture the patient’s life, assisting at the moment of death and helping loved ones process their grief in the weeks that follow.
On the first morning, Fersko-Weiss, a social worker who worked with hospice facilities for decades before creating an end-of-life doula program in 2003, asks each of the students to recall a death that affected them. How it smelled and looked and felt. How it shaped their concept of what constitutes a “good death.”
One woman talked about her daughter’s stillborn baby.
“That was the hardest hurt I ever felt,” she said. “I didn’t understand how you could take a baby who was full-term.”
Fersko-Weiss nodded and observed that she may be able to transform her pain into something that could aid dying patients and their families.
“If we can touch that place of angst and anguish and despair,” he said, “it may help us to be more present to other people experiencing it now.”
Later, the prospective doulas talk about their reasons for coming. Several had had negative experiences with the death of a close relative. A few were birth doulas who wanted to assist with the exit from, as well as the entrance into, life. One woman had suffered a brain injury and a near-death experience. All said that they wanted to be of service in a way that would make this final transition somehow better for others.
They will be called upon to fill all kinds of roles, Fersko-Weiss told them. Sometimes patients may need help with physical care; other times, families will need assistance with errands or household chores. In all cases it will be a doula’s job to listen, without judgment, to honor the experience of both the dying person and their loved ones, and to facilitate meaningful interactions between them.
“As a doula, it’s important to encourage people to say everything they need to say,” Fersko-Weiss explains, “so that they don’t look back and really regret it.”
Beautiful souls
Craig Phillips’s path to end-of-life doula work wasn’t straight, but he thinks he was always inching toward it. He grew up in Wilkes-Barre, Pennsylvania, next door to a cemetery that served as his playground. In college, he had a chance meeting with Elizabeth Kubler-Ross, the famed psychiatrist whose groundbreaking work shaped our modern understanding of death. And all through his life, Phillips has had an intense awareness of his own mortality.
At 61, he has the look and presence of a yogi, but he spent most of his adult life in the corporate world. Several years ago, his sister called, saying that her ex-husband was suffering from advanced ALS and living in a facility very close to Phillips’ Baltimore home. So Phillips went to see him. And kept going, two or three times a week, for the last 2 1/2 years of the man’s life.
“I’d bring him flowers,” he recalls. “I’d tell him stories. I’d take oil over and rub his feet, stuff like that. Just devoted myself to him. And it was a beautiful thing.”
A man in Phillips’ running club mentioned volunteering as a death doula, so when he retired last fall, he linked up with Gilchrist Hospice Care, which serves more than 750 patients daily in the Baltimore area and established its own end-of-life doula program in December 2009. It has since grown to more than 150 volunteers.
After 20 hours of training in January, Phillips spent a morning shadowing a mentor doula at Gilchrist’s facility in Towson.
“We walked into a patient’s room, and she said, ‘Isn’t this person beautiful?’ I could see that they were. And she said, ‘Yes, all my patients are beautiful,’ ” he recalls. “You walk into a room and there’s someone there with their mouth open, looking very near death. Perhaps no teeth in their mouth and a three-day beard or whatever. And I look at these souls and they’re beautiful. It’s the oddest thing. Their guard is down. They’re just who they are in their most real, beautiful state.”
Phillips has helped long-term-care patients communicate with a letter board and even washed a dog for one family. On his weekly visits to an elderly man who was still alert, Phillips brought videos of the patient’s favorite big band performances.
But with many patients, Phillips just sits, quietly meditating and sending good wishes. He tells them that they are safe. And that they are not alone. One woman was unable to speak, but when he said goodbye after three hours, “she mouthed the words ‘Thank you’ and held out her hands like I was dear to her,” he says.
The work has also produced an unintended side effect. It has pushed Phillips’ awareness of mortality even further to the forefront of his mind.
And happily so.
“The more immediacy, for me, that I have of this,” he says, “the more appreciation I have for every day, every minute.”
It is illegal to help someone kill themselves in Malta. But what if someone is dying in great pain?
It is illegal to help someone kill themselves in Malta. But what if someone is dying in great pain?
Opioids usually administered in these times are sometimes not enough to stop the agonal stage of death. Agony comes from the Greek word ‘to struggle’. The process of dying, as seen by an observer, is that of a struggle. The stage right before an older person dies is often accompanied by disorientation, struggling to breathe with long pauses in between loud, laboured breaths – called Cheyne-Stokes breathing.
Sometimes a death rattle is heard in the breathing when there is liquid in the lungs. Sometimes the person may start convulsing. This agonal process is eloquently described in the Tibetan Book of the Dead. This is not the way we want to die.
In one study looking at what people said is their ideal way to die, Gilbert Meilaender from Valparaiso University in Indiana suggested a one-word answer: Suddenly! The idea is to live as long as possible at the peak of our vigour and then, when the time has come, to die quickly and painlessly. But this is not the way we die.
With our advancing and encroaching technology, it is more likely that dying will become a more protracted affair despite our wishes. Surprisingly, when we try and hasten the process we, as a society, have responded by punishing those who are trying to help us achieve a painless death.
In the US, one of my neighbours, Sharlotte Hydorn, before her death in 2013, gained a measure of notoriety by offering to mail you, for only $60, a package containing GLADD exit bags – Good Life and Dignified Death. The kit included a plastic bag, medical tubing, two canisters of helium and instructions on how to commit suicide – by placing the bag on your head and filling it with helium, which deprives the body of oxygen. The body does not know it is being denied oxygen since the helium mimics the oxygen molecule. You die peacefully. In the US, more than a quarter of us will likely die in an emergency room, our final departure looking more like a chaotic medical soap opera. Our death will be seen as another medical failure. For the majority of us, this is not what we want or what we deserve.
In Europe and the US, hospice care is gaining ground as the gold standard for end-of-life care. The Malta Hospice Movement is today caring for over 1,000 patients and their families. However, Malta Hospice, as most hospice services, is used by too few people. And when these services are used, they are used too late. The result is that most older adults still experience widespread distress in the final stages of life.
The result is that we deal with dying underhandedly. In hush hush tones we conspire to give the dying person a good death. In Malta, Jurgen Abela from the University of Malta’s department of family medicine conducted a survey of 160 doctors. The results are revealing. One in seven doctors were asked by their patients to help them die. Despite this, nine out of 10 would refuse such requests for moral reasons – since a majority were Catholic and this was important to them – despite half of these same doctors accepting the right of individuals to hasten their death. Such schizophrenic response harbours a sense of bigotry.
The religious fervour to curtail euthanasia has not slowed the growing number of states that have legalised physician assisted death. With four US states and four countries that today openly and legally authorise active assistance in dying of patients, the list of states/countries is growing.
There is nothing absolute in these situations. Physicians cannot determine with infallible certainty that someone is going to die, sometimes the medication used does not work as intended, or is delayed, the process of injecting a person with enough opioids to kill them is not family-friendly and it is killing without consent. These are all valid criticism that pose moral challenges.
If we look at how physicians die, what we find is that a majority of them do not go for invasive treatment if they know that it is unlikely to improve the outcome. They chose quality of life over quantity of life and self-medication is high. It takes a special person to go through with euthanasia.
In the state of Oregon in the US, only a small fraction goes through physician-assisted-suicide. In 2013, a total of 71 people went through physician-assisted-suicide out of nearly four million people in Oregon. In Malta this would translate to less than five people a year. There is no ‘thin end of the wedge’. These people, nearly exclusively white, were educated with a diagnosis of cancer (since we know a lot about the progression of this disease.)
Different older adults need different support. Some end-of-life options may not appeal to you, but the option needs to be made available for others that it might help. Euthanasia is about diversity of needs. Not everyone might want or need it but it should be an option for those very few for whom it might help alleviate the pain of dying.