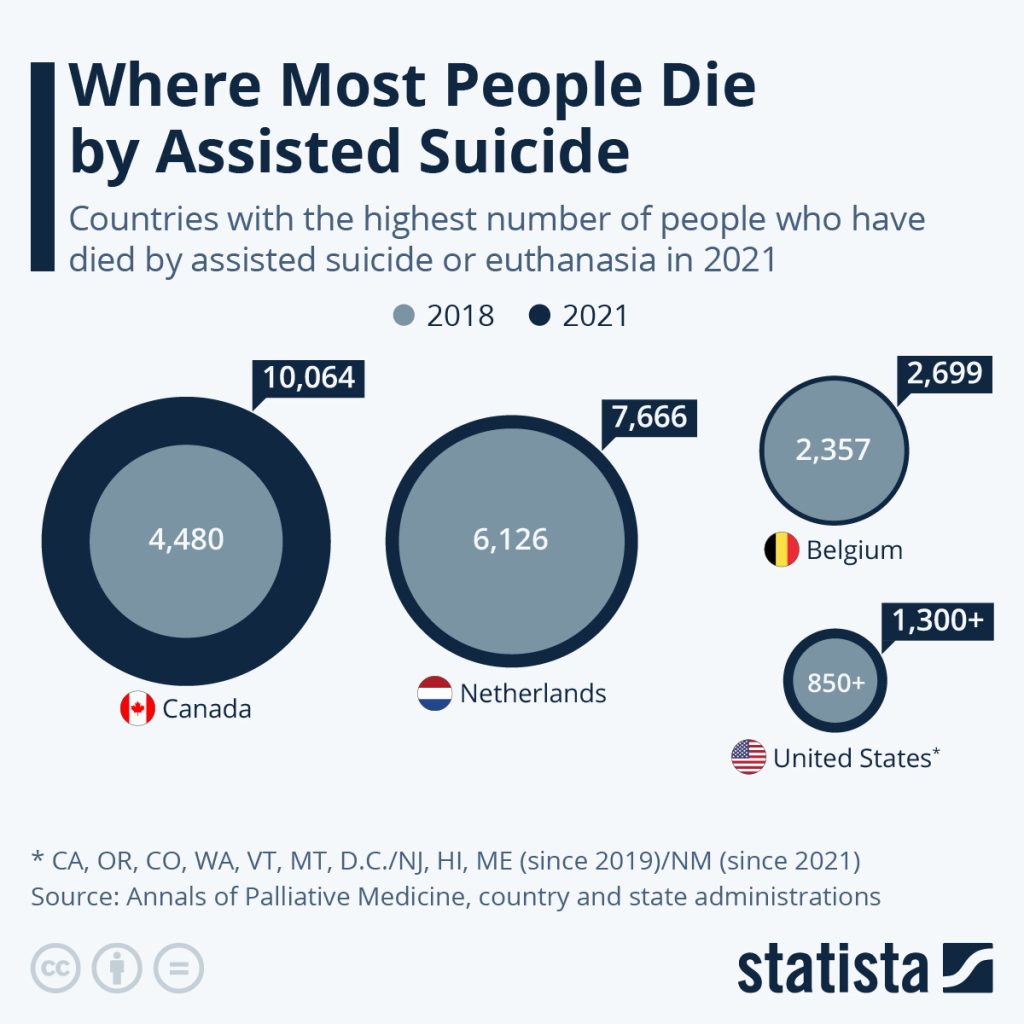
The Netherlands and Belgium which, like Canada, allow both have seen numbers rise more slowly. Assisted dying has been legal there since the early 2000s, however, while Canada legalized it in 2015 and has considered those who p have a disability but are not terminally ill for assisted dying since early 2021.
In 2021, assisted dying accounted for 3.3 percent of all deaths in Canada.
The United States also saw a faster rise in those dying by self-administered physician-assisted suicide over the past four years (euthanasia is not legal in the U.S.). This was also aided by the fact that four states – New Jersey, Hawaii, Maine and New Mexico – legalized it between 2018 and 2021, while two more populous ones, Colorado and California, started the practice in 2016.
Switzerland is another practitioner of physician-assisted suicide, but not euthanasia. 1,196 people died with assistance in the country in 2019, the latest year on record. Assisted dying is also legal or will become so soon in Luxembourg, Colombia, Spain, Austria, New Zealand and most Australian states.
The practice of both self-administered medication-assisted suicide and euthanasia – where a doctor administered deadly drugs upon request – have been legal in the Netherlands, Belgium and Luxembourg since the 2000s and has been practiced in Switzerland, which only allows the former, since the 1980s.
Colombia legalized euthanasia in 2015 and assisted suicide this year and both types also became legal in Canada in 2015.
In the past two years, Spain, Austria and New Zealand have made euthanasia and assisted suicide legal.
Similar laws also came into effect in several Australian states, starting with Victoria in 2019 and Western Australia in 2021. The remaining states in the country except for the Northern Territory will roll out these laws throughout the rest of 2022 and into 2023.
In the United States, the first states to legalize assisted suicide were Oregon in 1994, Washington in 2008, Montana in 2009 (via a state Supreme Court decision) and Vermont in 2013. The number of states who adopted the practice has risen recently, when it was legalized in California and Colorado in 2016, Hawaii, New Jersey and Maine in 2019 and New Mexico in 2021. Active euthanasia remains illegal in the country.
In Italy and Germany, national parliaments are currently grappling with legislating assisted dying after high court cases were decided in favor of proponents of the practice.
Creators of the services say their goal of providing easily accessible and organized help for people in distress has never been more necessary
By Sophia Laurenzi
What do you do after someone dies? Most people expect to deal with intense grief, but they might not realize how many logistical details arise after a death. Those tasks can feel overwhelming: deciding who to call, learning where to get death certificates, planning memorials and navigating finances.
“It’s so daunting … to figure out where to even start,” grief therapist and author Claire Bidwell Smith says. Bidwell Smith’s mother died when she was 18, and her father when she was 25.
Shortly before his death, he helped her make a checklist of all the things she would have to do: call the mortuary, Social Security and the bank; order this many death certificates; plan for what to do with his things. “I sat there with tears dripping down, being like, I don’t want to do this,” Bidwell Smith says. “But the minute he died, I was so grateful to have that list.”<
Now, new apps and websites with names such as Cake, Lantern and Empathy exist to help people navigate the tumult and confusion after a loss, offering tools that range from organized checklists for the early days of funeral planning to resources for later concerns such as closing a deceased person’s credit card account or finding a home for the deceased person’s pet.
The creators of these apps and websites say their goal of providing easily accessible and organized help for people in distress has never been more necessary. “The pandemic has increased people’s understanding of why this is important, as well as the actual need” for services, says Suelin Chen, who co-founded Cake in 2017.
Cake, which says 40 million people a year visit its website, provides a list of what tasks people need help with and then creates a checklist, along with offering guides to tasks like making an online memorial page for a loved one. The website hosts a library of thousands of articles related to death, including how to express condolences to a friend and how to plan an eco-friendly burial service. Cake, which is free to users, also provides help with other end-of-life needs, such as advice for talking to elderly parents or how to create a will.
The website Lantern, founded in 2018, and Empathy, founded in 2021, likewise provide guides on what tasks must be tackled after a death, with information about options at each step and timing.
Lantern, whose co-founder Liz Eddy was inspired to create the website after her grandmother died and ended up Googling what to do next, aims to be a one-stop resources for mourners. Among other things, it provides information about how to write a eulogy and “do an ash scattering ceremony,” and offers a list of “best funeral songs,” with traditional/religious, somber and joyful possibilities. Empathy’s “Obituary Writer” function, meanwhile, promises it “can craft a publication-ready tribute based on your answers to a few questions.” For a fee, it also offers one-on-one support from a professional after-loss consultant who essentially acts as a concierge for after-loss tasks.
“We connect people with services and give them tools, but a lot of it is really an education platform,” Eddy says.
Other companies are working to move beyond just providing information to creating tools that will handle some of the post-death logistical burden.
EstateGrid is working on building a service that will automate much of the bureaucratic aftermath of death. It starts with automated discovery of assets, liabilities and accounts, using the deceased person’s identity and death certificate to generate a list of what needs to be done. The platform will offer tiered levels of services, such as free tools and paid options, for the automation processes.
“Every life leaves a mess,” the website says, which also offers help in selling a house, finding investment accounts, appraising valuables and finding a new home for a pet.
The mobile app Empathy, which also features an easy-to-navigate checklist, offers premium services such as an obituary writer that promises to create a polished obituary based on the mourner answering a few questions. The paid option, which costs $8.99 for one month or $64.99 for a year, also includes tools that automate closing the deceased person’s accounts, memberships and subscriptions. The app uses software to pre-fill forms and streamline processes that usually take dozens of separate phone calls.
The companies are not just about logistics, however. They also include grief resources as part of their tools.
Experts say that makes sense. It’s hard to separate out logistics following a death and the grief people must deal with. The logistics “can be so overwhelming and terrifying, and actually sometimes get in the way of the grieving process,” psychologist Jordana Jacobs says. When the tasks that follow a death take up so much time and energy, it can shift focus away from grief, at least temporarily. As psychotherapist Megan Devine says, “Logistical support doesn’t change grief, but it reduces suffering.”
>Empathy provides grief meditations, journaling and chat support (which is another premium feature). Empathy co-founder Ron Gura says his company has focused on helping people dealing with both issues. “We don’t think you can decouple them,” he says.
The text-based company Grief Coach focuses on the emotions that follow a death, using advice from grief experts to send personalized texts to your phone. These messages — which range from describing breathing techniques to use when feeling overwhelmed to reminders that grief is not a linear process — are designed to provide extra help that family and friends often want to but don’t know how to give.
Founder Emma Payne created Grief Coach after her husband died by suicide and she stopped hearing from many friends and families. Ten years later, she went to a friend’s funeral and learned how devastated many of her people were to have lost touch: They just didn’t know what to say. Grief Coach costs $99 a year, which includes adding up to four friends and family members who also receive texts with suggestions on how they can support the grieving person, such as reminders of the deceased’s birthday.
Grief Coach does not replace human support; instead, it teaches grievers how to find and ask for support and helps their loved ones show up in meaningful ways. Experts say that logistical support from technology can be helpful as a stand-alone, but that digital grief support is best used as a supplement to personal support or therapy that is often needed to process and move forward from profound loss.
“My hesitation around technology is that we just have to make sure we don’t lose the intimacy inherent in what is healing about connection through grief,” Jacobs says. “We have to make sure we still make these technological products very human, because it is through that humanity … that we actually heal the most from loss.
Bidwell Smith, whose father made her that critical checklist, says she believes that even though technology cannot replace those healing connections, it can enable people to connect with each other.
“Grief is so lonely, and it can be very isolating,” she says, but she is encouraged to see people with similar experiences find each other in online communities like social media and new after-loss websites and apps. “I think anything where someone can feel more connected and less alone in what they’re going through is a good thing.”
There is no easy way to deal with what happens when a loved one dies. But by helping demystify essential tasks and offering resources for both logistics and grief, these digital services leaders say they hope they can help lift some of the burden off mourners, giving them a little more space to heal and connect with the support they need.
Alice Matthews helps palliative patients write their life story, sometimes with a “children’s book” version for their kids.
By Justine Toh
When we think of how we’ll be remembered after death, it may seem that simple words and basic descriptions don’t do us justice.
But for parents with a terminal illness and those on their deathbed, plain language is sometimes best.
“Dad was an artist. He painted the world that he saw. People loved his drawings.”
How else do you tell your life story — or explain death — to a young child?
Alice Matthews knows something of the challenge of putting a life into a story.
Since 2017, the SBS and ABC journalist has volunteered as a biographer with the Sacred Heart Community Palliative Care Biography Service based at St Vincent’s Hospital in Sydney.
The work involved sitting by the bedsides of the dying and, over a series of sessions, recording their stories.
For Alice, bearing witness to people’s lives, crying along with them, helping them grieve, reflect, and consider their legacy was an enormous privilege.
“We talk a lot in the service about holding space for someone,” she told RN’s Soul Search.
“There is an incredible spirituality in doing that, sitting with somebody, being with them and not really having to say or do anything except that.”
Death: the storybook version
Alice mostly saw elderly clients, part of a group often “shunted and pushed aside” by the wider world.
“What better way to return value to them than to sit and talk about their life and the value of their life which hadn’t disappeared,” she said.
Such clients often met their deaths with acceptance or comfort in their various religious and spiritual beliefs.
Others died “before their time”, as we would say.
If they had young children, Alice would put together a “storybook” version of their dying parent’s longer biography.
Some of the best-loved children’s books feature themes of loss and death.
For one client, a dad with a young daughter, Alice worked with the family to come up with a child-friendly “circle of life” explanation of death.
“I remember sitting in the room with them as the wife read it to her husband. That was one of the moments where we all sat there in tears,” Alice said.
“I didn’t know how he would react. He wasn’t verbal at that point.
“We waited a moment and then saw that he’d typed: ‘That was beautiful.’
“That was one of those moments where you feel the entire weight of the heartbreak — but also the relief.”
Once upon a time
Another writer who understands this struggle to give language to death is author Chloe Hooper.
Chloe’s partner Don Watson, the historian, author, and speechwriter, was diagnosed with an aggressive form of leukaemia in 2018. Things looked grim.
Then there was the uncertainty: how to explain his possible demise to their young sons — Tobias, then six, and Gabriel, three at the time.
Writing offered some comfort in the face of grief for author Chloe Hooper.
Few age-appropriate titles on the shelf seemed right. So, Chloe embarked on a quest to find the perfect book.
“The right story can help us find a path through the forest. It can help us take our straw and weave it into gold,” she said.
“Quite quickly, I realised that storytelling and perhaps re-storying this situation would be a way to help us through.
“The electricity and potential of ‘Once upon a time’ might be a way for us to light the dark.”
Chloe’s search for the best words to explain death — recounted in her book Bedtime Story — turned up the innumerable ways in which adults have explained death to children.
Grief and enchantment
Along the way, she made a surprising discovery: beloved children’s authors had suffered significant bereavement in their lives.
Roald Dahl, for one, described himself as “limp with despair” as he began writing Charlie and the Chocolate Factory after losing his seven-year-old daughter.
Dahl wasn’t alone. The Brothers Grimm, Hans Christian Andersen, J R R Tolkien, Frances Hodgson Burnett, C S Lewis, J K Rowling — death had touched them all.
Writer Roald Dahl was familiar with death, both in his personal life and in his children’s books.
Writing couldn’t overcome death, but it seemed a comfort in the face of it.
“It made me realise that an ingredient of enchantment is grief,” Chloe told me, referring to the often magical settings of the stories penned by those writers.
What she was looking for — the perfect story to tell her children about death — “was embedded in all of the stories that surround us.”
Mythic narratives similarly stalked the border between life and death, Chloe noticed.
Descent and return narratives saw characters like the Greek hero Odysseus — and even religious figures like Jesus Christ — descend to the dead before returning to the land of the living.
These stories, and their authors, couldn’t help but stray into spiritual territory.
For Tolkien, fairy tales were ultimately about escaping death. C S Lewis, author of the Narnia series, found himself a Christian after becoming convinced that the story of Jesus Christ’s death and resurrection was what Tolkien called a “true myth”: the fairy tale that came true.
‘Everything will be alright’
Plenty of people — including Chloe Hooper — are agnostic about that.
But every parent knows it’s their job to protect their kids. According to the late sociologist and theologian Peter Berger, “to become a parent is to take on the role of world-builder and world-protector”.
For Berger, this makes parents practically godlike.
Parents represent “the underlying order of the universe that it makes sense to trust,” he writes in A Rumor of Angels: Modern Society and the Rediscovery of the Supernatural.
Take the most basic parenting move: hushing a crying child in the dead of night. For Berger, when a mother rocks her bub, murmuring “Everything will be alright,” she relates to her child the way we imagine a god should relate to their creation.
Even the most ardent skeptic gets that a god’s job is to guarantee order and safety and beat back the encroaching darkness.
This casts new light on the stories we spin about death: from fairy tales to storybook versions of the “circle of life”.
What are these if not our attempts to love those we must eventually leave? Our efforts to weave out of the world’s sadness a life-giving spell?
Perhaps we’d rather not read the stories of our lives that get written on our deathbeds.
But even if such stories are prompted by the most decisive of endings, they pulse with love and concern for the living left behind.
Death doesn’t exactly get the last word because these stories are, in the end, about life.
Being honest and facing mixed emotions about a loved one’s death can help with healing
“All people are fallible humans, in life and in death, too. We disagree with one another and we don’t always get along. But there is always a possibility to get it right when both people are alive. We lose that opportunity when someone dies. We lose the chance for closure.”
Jacalyn Wetzel, a writer and therapist from Mississippi, recently lost her father. Wetzel describes her relationship with her father as complicated, so it is not surprising that her emotions surrounding his passing are complicated, too.
Wetzel explains, “Growing up, I had a lot of resentment towards him. My dad made many missteps in his own life and his choices hurt me. When I was an adult, things started to turn around, especially in the last two years. He showed more often than not that he was trying to fill the cracks he had left from years before.”
“Grief is even more complicated when everything between you wasn’t rainbows and sunshine.”
Losing a loved one is always hard. It doesn’t matter if the relationship was good, difficult or a combination. Rebecca Soffer, who runs the website Modern Loss (and wrote a book of the same name), explains, “All people are fallible humans, in life and in death, too. We disagree with one another, we argue, and we don’t always get along. But there is always a possibility to get it right when both people are alive. We lose that opportunity when someone dies. We lose the chance for closure.”
Adds Wetzel, “Grief is even more complicated when everything between you wasn’t rainbows and sunshine. It’s still grief, just the same.”
As a point of clarification, the term “complicated grief” is used to describe a disorder where a person experiences long-standing grief where feelings of grief do not dissipate over time and are debilitating. This article focuses on grief when the relationship itself is complicated.
Fear of Honest Reflection
Psychiatrist Gail Saltz, associate professor of psychiatry at the New York-Presbyterian Hospital Weill-Cornell School of Medicine and host of the “How Can I Help?” podcast, explains, “Funerals are for paying respect to someone. These rituals are about giving comfort and support to the mourners.”
People rarely delve into the complexities of a relationship, especially when speaking publicly about a deceased loved one. We have been taught not to speak ill of the dead, so in general, eulogies are focused on discussing the deceased’s best qualities and sharing stories that put them in a good light.
Saltz says, “What is said at a memorial is not going to give a clear picture of the total person.”
But most relationships are not all good but rather multi-dimensional, especially between family members. Some relationships are fraught or even toxic. Because of the differences in situations, so, too, may be a person’s reaction to the loss.
No Rules for Grief
“Different circumstances can lead to different emotions surrounding death,” explains Saltz. “Many people think grief is just about being sad. But you can also feel a range of other emotions including guilty, perturbed, lonely or ambivalent.”
“The idea that there are five stages of grief that happen consecutively and for a specific amount of time is misguided,” says Soffer. “Grief isn’t organized; it’s a mess and a natural human experience. There is no ‘normal’ way to grieve.”
The idea that there is a correct way to grieve can impede the healing process. Well-meaning friends and family can make people feel judged about how they are grieving or comment on how a person “should” feel rather than listening to the person’s feelings.
“Many people have a picture in their mind of what a mother/daughter or sister relationship should look like,” explains Saltz. “But all relationships are individual. If a person had conflicted feelings about a person when they were alive, they will probably continue to have mixed feelings when they are gone.”
“Whether tears fall or not, it doesn’t mean there wasn’t love there. Love is just as complicated as grief and people aren’t perfect.”
Wetzel recalls that when her stepfather passed away several years ago, some people commented, “Well, he is only your stepfather” or “You are lucky you still have your real father.” The comments stung.
Wetzel says, “My stepfather raised me from the time I was a little kid. In many ways he was more of a father to me than my biological father had been. Although people didn’t mean it, these types of comments upset me.”
Conversely, Wetzel has been made to feel she isn’t grieving enough for her biological dad, especially by his extended family. She herself says she has been waiting for the “dam to break” and is starting to wonder if it ever will.
“I try not to judge myself, “says Wetzel. “Whether tears fall or not, it doesn’t mean there wasn’t love there. Love is just as complicated as grief and people aren’t perfect.”
Safe Space to Grieve
Soffer believes people do themselves a disservice when they don’t allow themselves to fully face all of their mixed emotions about the person and what has been lost.
“It can be lonely when you hide your true feelings or are afraid to speak openly for fear of being judged. Honest reflection can help us learn, build and move forward healthily,” she says.
Well-meaning family and friends can be helpful, but they may also be biased. “People who know you or knew the deceased may have pre-existing beliefs about the relationship or the person,” says Soffer. “If they aren’t able to offer you space where you can speak honestly without judgment, it may be better to seek grief support elsewhere.”
Finding a safe space to share your feelings is key to healing. Peer-to-peer grief support groups (in-person and online) and professional grief counselors are great options. “With a grief counselor, the grief discussed is ‘yours only,’ and you don’t have to worry about another person’s feelings,” explains Soffer. “It may take a few tries to find the right grief counselor, a person you are comfortable talking to about the tough stuff.”
For Wetzel, telling her story on social media proved cathartic. “I have always tried to be real and honest with my followers,” she says. “I needed to explain my absence, so I shared that my father had passed. But then I was getting a lot of condolences which made me feel the need to be transparent about our relationship and my conflicted feelings of grief.”
Wetzel found most people appreciated her candor and many expressed having been in similar situations. “At the time, I was feeling guilty and alone. It was helpful to know others had gone through the same type of experience,” she says.
“We are happy and sad to see you again. You looked after Dad years ago.”
I kick myself for not registering the connection, although I only met him during a brief and disastrous stint in hospital.
The complications of cancer treatment had kept mounting until his wife was forced to admit her 85-year-old husband to hospital despite his protestations. His memory had faded and his moods turned volatile. He died in hospital, captious and discontent. I now recall the exhaustion of the family and their guilt-ridden attempts to reconcile with his end.
Some of my work involves seeing cancer patients in their 80s and 90s. The mission of a “geriatric oncology” service is to treat the cancer in the context of the whole patient; while it can be said that all cancer care ought to share this mission, elderly patients are a particularly vulnerable group, with little margin for misadventure. Since two in five people will receive a cancer diagnosis by the age of 85, there have been several occasions when I have treated both husband and wife.
Here are three things that I have learnt from looking after my most elderly patients.
1. Their goals differ
While younger patients compare their treatment to what someone else is having or bring in an overseas recommendation, and (understandably) want to leave no stone unturned, even at the cost of significant toxicity, my oldest patients often have a different goal – to preserve quality of life and maintain independence, even at the cost of survival.
This is especially true when a person is both patient and caregiver.
Co-dependant elders can get by happily in their own home but the moment one stumbles, both are in jeopardy. I frequently meet people who base decisions on combined harm rather than individual good. Interestingly, the people who sometimes struggle to comprehend this are their doctors who are taught to focus on cure.
Many patients who have accompanied a spouse through cancer and end-of-life care have used the opportunity to reflect on their own choices.
I met an octogenarian who declined chemotherapy after caring for his wife who endured recurrent hospitalisation before dying. The same day an elderly woman insisted she would rather “die on the table” than live a life of regrets, as her husband did after he rejected surgery.
One of my most memorable patients was a 90-year-old man who refused an operation because the resulting diarrhoea would involve him negotiating a steep staircase to use the bathroom more frequently. Given the choice of moving out of his beloved home and living longer, he didn’t think twice. I have seldom seen a happier man exit the hospital without a cure.
I also meet overwhelmed patients who relinquish decisions to professionals but, when given the chance (more on this later), most patients will explicitly state what matters to them and make concordant decisions. A long life, necessarily including experiences of sadness and mortality but also inspiration and hope, has given them fortitude, equanimity and perspective. Not everyone wants to live forever, especially if the life is messy.
2. It’s hard on the children
Elderly patients have middle-aged children in the prime of their careers or out of the workforce for important reasons. Apart from tackling a mortgage, navigating workplace tensions and looking after themselves, they are juggling dependent children and vulnerable parents. They are carers, cooks, interpreters and drivers. In a multicultural community the “blessings and curses of filial piety” are on full display, and I worry that I am rarely useful.
Often, there is sibling conflict, usually because one sibling is doing “all the work”. Then there are the expectations of the carer that are hard to meet.
Can I see their parent on their day off? No, the system is inflexible. Can I organise transport? No, there is no funding. Can I avoid issuing last-minute appointments? No, it’s out of my control. Can I expedite aged care services? No, they must join the queue.
I wish the system understood the toll that illness exacts on the whole family.
One of the hardest things is to witness children seeing one parent succumb to cancer, only to repeat the experience. The despair of anticipatory loss is palpable but, if there is one glimmer of hope, it is the benefit of hindsight.
Families who insisted on intensive care at the end of life acknowledge its futility, those who doubted palliative care recall its worth. There is irony in the hope that the next time will be “better”.
3. We must do better
When illness is regarded as an anomaly, the emphasis is on fixing the problem, averting loss and restoring normality.
Every patient deserves optimal care but, when the conversation begins and ends with response rates and survival curves, it is a missed opportunity to respect the whole person, honour their wisdom, longevity and contribution to society and let them contemplate a twilight that contains dignity and comfort.
The power imbalance between doctors and elderly patients is especially pronounced.
I find it confronting to hear these patients lament that they are undertaking onerous surgery or toxic chemotherapy because they don’t have a choice. Some are confounded to learn that they always have a choice, even if doctor and patient agree to disagree. For many people of their generation, advocating for their right to be heard is unthinkable. For those who come from culturally and linguistically diverse backgrounds, this feels impossible.
No doctor who recommends an intervention in good faith wants to hear that a patient feels coerced, so we must choose language that opens the door to shared decision-making and correct the dismal lack of research on the needs of elderly patients. It is an indictment of medicine if the patient who really wants to say no ends up saying yes.
My elderly patient decides against treatment but requests periodic consultation to allow her to change her mind. All things considered, she says her work on Earth is done and she greatly misses her husband. At this, the daughter sheds a tear, but I can already see that this deliberate decision-making is better than what went before.
We won’t cure the patient but we will have honoured the person. A victory for the patient is a victory for medicine.
Study finds most people over 95 are simply grateful for every day
People well into their 90s are often willing to talk about death, but they’re rarely asked about it, a new British study finds.
“Despite the dramatic rise in the number of people living into very old age, there is far too little discussion about what the ‘oldest old’ feel about the end of their lives,” said study leader Jane Fleming. “We know very little, too, about the difficult decisions concerning their end-of-life care.”
Fleming is with the University of Cambridge’s public health and primary care department.
The researchers interviewed several dozen people over 95 years old — or their relatives or caregivers if they were too frail — about their attitudes on death and end-of-life care.
According to the study, published April 5 in PLOS ONE, most had outlived their peers. Many felt they were living on “borrowed time.” They also felt grateful for each passing day, and didn’t worry too much about the future.
“It is only day-from-day when you get to 97,” said one participant.
The researchers noted that most of the older people interviewed felt prepared to die. “I’m ready to go,” said one woman. “I just say I’m the lady-in-waiting, waiting to go.”
In some cases, the participants felt as if they had become a burden on others or were anxious to finally reach the end of their long lives.
Many were more concerned about how they died than when. They hoped they would “slip away quietly” in their sleep and that their death would be painless. “I’d be quite happy if I went suddenly like that,” said one.
Few participants said they would want to be hospitalized if they became sick.
When asked if they would prefer lifesaving medical care or treatment to help them remain comfortable, most opted for comfort. Most were also not afraid of dying. For some, witnessing the peaceful death of others helped them manage their fears.
One woman recalled her parents’ deaths, saying, “They were alive, then they were dead, but it all went off as usual. Nothing really dramatic or anything. Why should it be any different for me?”
Funeral planning among the very old is more common than open discussions about death, the researchers found. Some had even made arrangements for themselves in advance.
“Death is clearly a part of life for people who have lived to such an old age, so the older people we interviewed were usually willing to discuss dying, a topic often avoided,” Fleming said in a university news release. To best support men and women dying at increasingly older ages, she said, “we need to understand their priorities as they near the end of life.”
Most participants had had end-of-life discussions with their doctor. But, rarely did these conversations take place among family members, said Fleming and her co-author Morag Farquhar, a senior research associate in the public health and primary care department at Cambridge.
“Having these conversations before it is too late can help ensure that an individual’s wishes, rather than going unspoken, can be heard,” Farquhar said in the news release.
A quarter of the participants in a long-term study of older people experiencing homelessness in Oakland died within a few years of being enrolled, UC San Francisco researchers found.
The study, funded by the National Institute on Aging, recruited people who were 50 and older and homeless, and followed them for a median of 4.5 years. By interviewing people every six months about their health and housing status, researchers were able to examine how things like regaining housing, using drugs, and having various chronic conditions, such as diabetes, affected their risk of dying.
They found that people who first became homeless at age 50 or later were about 60 percent more likely to die than those who had become homeless earlier in life. But homelessness was a risk for everyone, and those who remained homeless were about 80 percent more likely to die than those who were able to return to housing.
Becoming homeless late in life is a major shock to the system.
The median age of death was 64.6 years old, and the most common causes of death for people in the study were heart disease (14.5 percent), cancer (14.5 percent), and drug overdose (12 percent).
“These untimely deaths highlight the critical need to prevent older adults from becoming homeless – and of intervening and rehousing those that do, quickly,” she said.
The study is unique for its prospective design. Previous studies of mortality in homeless populations were retrospective and drew information from medical records. By contrast, the current study – Health Outcomes of People Experiencing Homelessness in Older Middle agE (HOPE HOME) – followed a group of people, whether or not they received health care.
Many study participants had serious conditions that went untreated.
“We looked at how frequently people reported diagnosis of heart disease or cancer before dying of these diseases. It was really low,” said Rebecca Brown, MD, affiliated assistant professor of medicine in the Division of Geriatrics at UCSF. “We think this represents a lack of access to care and delayed diagnosis. Often, we didn’t even know people were ill because they didn’t report it in their six-month interviews. But we found it on their death certificates.”
Researchers went to great lengths to track down what happened to the people in the study when they missed check-ins and couldn’t otherwise be accounted for, including looking at photos of unidentified deaths at the coroner’s office, reviewing California state death records to match their participants’ names and dates of birth, querying emergency contacts, searching social media, and reading online obituaries.
They found that as of Dec. 31, 2021, 117 of the 450 people had died since the study began enrolling in 2013. Nearly 40 percent (45) occurred after the pandemic started in March of 2020, but just three of those deaths were from COVID-19. Participants entered the study in two waves, with 350 enrolled in 2013-14 and another 100 enrolled in 2017-18; 101 of the deaths were from the first wave, and 16 were from the second.
Mortality rates were high compared to the general Oakland population. The risk of dying was 3 times higher for men and 5 times higher for women, compared to people of the same age and sex in Oakland. The median age for participants entering the study was 58, and 80 percent were black; 76 percent were male, and 24 percent were female.
The study also contained detailed information about people’s use of drugs and alcohol, as well as their mental health. But drug and alcohol use itself was not independently associated with death.
“The streets are just no place to live,” said Johná Wilcoxen, 72, who spent more than a decade living in his car when he lost Section 8 housing because his children moved out. Through his ordeal he continued working as a plumber, which gave him a place to go during the day and money for food. “The more people as we can get off the street, the better,” he said.