Chad Lewis charges $20 to $25 an hour to assist the gravely ill and their families.
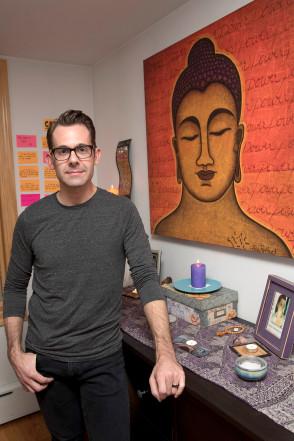
[W]hen Chad Lewis’ mother passed away seven years ago from complications from diabetes, he couldn’t stop thinking about her death. “It wasn’t loving and sweet,” he says. “It was chaotic and angry and scary.”
So Lewis, a 39-year-old who lives in Astoria, set out to find a better way to process the end of life, ultimately making a career shift from Broadway stage manager to death doula.
Doulas who aid women in giving birth have been trendy for years, but now a different type of support person is helping people navigate life’s other major passage. Dying people and their loved ones are hiring death doulas to help them coordinate end-of-life care and vigils, plan funerals and provide a sympathetic but unattached ear.
The profession first came into being in the early aughts and is growing increasingly popular. In 2014, Suzanne O’Brien launched the New York City-based Doulagivers, an online training program for death doulas.
“I can hardly keep up with demand,” says O’Brien, who also holds monthly seminars at an Upper West Side branch of the New York Public Library.
The process usually starts with a patient deciding how they want to die and outlining that with the doulas.
“It’s similar to a birthing plan … Where [do] you want to die? What kind of room you want to die in? What [do] you want to be looking at? What [do] you want it to smell like?” says Shelby Kirillin, 41, a Richmond, Va.-based death doula. She charges between $1,000 and $3,000 as a retainer fee, and asks for payment upfront to avoid chasing down money posthumously. She’ll also work pro bono if a situation merits it.
The “scary” death of Chad Lewis’ mother led him to become a doula.
“I had one young girl say she wanted to die in a yurt,” says Kirillin of a client who’s currently planning her own death. The girl’s cancer condition makes a yurt too impractical, so Kirillin is getting creative. “We decided on mosquito netting over her bed, and twinkle lights to look like stars.” After she takes her last breath, her loved ones will put wildflowers in her hair.
Death doulas also help out after someone passes. Lewis, who charges $20 to $25 per hour, likes to create a basic plan to take care of issues such as child care, grocery shopping and bill payment, to clear up mental space for grieving families.
And more than anything, the professionals help patients process what they’re going through.
“Families buffer pain — you hate to see people you love in pain. And doulas aren’t buffers,” says Kirillin. “Instead of saying, ‘OK, let’s see if we can give you meds,’ I’ll say, yeah, ‘I bet you are in pain. Tell me about it — what does it feel like?’”
When Richmond resident Mel Titus’ best friend of 31 years, Kim, was entering the final stages of her battle with cervical and breast cancers last year, they were introduced to Kirillin.
They were skeptical at first, but Kim (whose last name is being withheld for personal reasons) decided on a death doula so she could manage her death the way she did her life. “She was a processor,” says Titus. “She really liked that she could come up with a plan and do things a certain way.”
And for Titus, Kirillin provided emotional support during an impossible time. “I would have tough days, and I’d call Shelby, and she’d walk me through it,” she says.
Kirillin helped the duo plan Kim’s visitor schedule, and what music they’d play and books they’d read in the final days. Taking care of logistics freed them up to reminisce about Kim’s life, and even laugh about how things were going. “We actually had some funny moments, believe it or not,” says Titus. “It’s sad, but it can be a happy thing, too.”
[I]n the hospital one afternoon, after unsuccessful surgery to remove her tumor, my mother drifted in and out of sleep. I sat on a sofa in her room with light from the window streaming in as I read email. My mother began talking to someone. I looked up.
My mother was an attorney. She dealt in realities. For most of my life, I knew her as a woman with few illusions. She did not kid herself, and she did not let me kid myself. She told my sister and me, when we complained about a situation, “Life isn’t fair.” So when she was diagnosed with pancreatic cancer, my mother approached it matter-of-factly because it was a matter of fact no one disputed. She researched pancreatic cancer online, came to terms with her odds and spent the next seven months maintaining as much control as she could.
Yet illusions sometimes came to her in those months. In that hospital room, she wasn’t talking to me but to people standing on the other side of her hospital bed, people invisible to me. They weren’t there, but she saw them. I couldn’t make out my mother’s words, only that there existed a pleasant back-and-forth going on. I was the first witness to her illusions.
I knew that, as a child, my mother had spent many days in the hospital for surgeries to correct bilateral club foot so she could walk. Her memories of that time included an imaginary friend whom she named after the model of hospital bed in which she had lain. As I watched her that day, I wondered whether John Standard had returned to her after all those years.
A few minutes later, my mother turned to me, fully alert. I asked whether she remembered the conversation she’d just had. Friends she hadn’t seen in a long time, she said, without going into detail. Then she tilted her head and added, “But they weren’t really here, were they?” I admitted that, no, they hadn’t been here. She said, “Well, it was a good conversation.”
My mother’s illusions were not delusions. She was not misled. The word “illusion” comes from the Latin “ludere” meaning “to play.” The word has longstanding negative connotations, as in a deception. But my mother’s illusions were her mind at play.
How different that was from my father’s delusions years earlier, when he was in the hospital undergoing cancer treatment. His gift balloon had become a spaceship, and he described to my mother a terrible war around him. He was caught up in it, afraid. One of the medications he’d been prescribed caused the delusions, and they subsided once it was stopped. But he said the scene had been so real that he couldn’t not believe it at the time. It still felt real after he knew it wasn’t. My mother could deal with anything in the physical world but couldn’t imagine how she would manage if my father lost his mind. By that, she meant his mind losing touch with reality. And she meant that his physical deterioration was enough for her to bear.
Later in her illness, at home, my mother began seeing medieval people on a hillside in her own bedroom. She enjoyed watching them, robed in their dresses and breeches, and she especially enjoyed the music they played. Flutes and mandolins. They even brushed large ostrich feathers and long veils over her skin. She didn’t know when these musicians would show up, but she welcomed them whenever it happened. She knew no one else saw these people or heard this music, and she didn’t care that it wasn’t real. I had some concerns but didn’t know what to do with them. I didn’t talk about these illusions in my book “Tumor” because I didn’t yet know how. There are so many concerns when someone is dying of cancer.
My mother and I talked with her oncologist about this new development, wondering whether such a thing was common in patients with cancer, perhaps the result of wasting or dehydration, two serious physical concerns at that point, or perhaps a side effect of one of the medications or chemo drugs. The oncologist asked several questions.
“No,” my mother said. “I’m not afraid of them. No, they don’t try to harm me. No, they don’t make me do things.”
The midsummer-night’s-dream people never talked to her and she never talked to them. She explained this arrangement as if such conversation would be crazy. Then, she said, “The music makes me happy.”
The three of us — my mother, her oncologist and I — decided this illusion was the least of our worries, that, in fact, medieval singers on a hillside were no worry at all. She had nothing to lose by listening, as long as she could hear the rest of us too. I was surprisingly relieved the oncologist did not want to treat this cognitive symptom because often physicians want to correct what deviates from the norm. He considered the larger context, the limited time, and told my mother to let him know if she stopped enjoying these visions.
This illusion, of course, might be considered a hallucination. The word “hallucination” comes from the Latin meaning “to wander in the mind,” originally akin to dreaming or allowing one’s thoughts to ramble. Hallucinations are now considered deceptions, not merely stray thoughts or daydreaming. To be sure, they can result from serious illness such as schizophrenia, dementia, epilepsy, Parkinson’s disease or migraines and make it difficult to function day to day. So hallucinations also came to be defined medically as distortions of sensory perceptions that the person experiencing them takes as real experiences. My mother, then, wasn’t really hallucinating because, though she accepted her experiences as real in her mind, she knew the people she saw and heard were not real in the world. She liked the touch of ostrich feather on her skin but didn’t think it existed in the world beyond her imagination.
Here was a woman who’d always shopped for a new outfit by picking what was paired on the rack because she was unable to imagine original combinations on her own. When my mother’s body weakened, when her body betrayed her, her mind said, “Let loose and enjoy the music.”
Even in that first observation of my mother’s conversation with friends who were not there, I was not upset that my mother was losing touch with reality or becoming less herself because she seemed at ease. Though they were unexpected and out of the ordinary, I became grateful for the odd joy my mother’s illusions gave her. What a practical thing for her mind to have done. I wish I knew how she did it. Any of us may someday face a similar illness. How fortunate my mother was able to conjure up happiness all on her own without denying the harsh reality of her condition. May we each find or conjure some music in our minds when we need most to hear it.
Anna Benton, of Milwaukee, left, Georgette Paxton, of Madison, center, and Jennifer Snow, of Waunakee, look over Heather Ockler, of Monona, who is playing the role of a dying person wrapped in a shroud during a home funeral demonstration. It was part of a death midwife class taught last month by Sharon Stewart, who helped aspiring death midwives practice skills such as washing and shrouding a body. Death midwives, sometimes called death doulas, are increasingly helping families prepare for and navigate the death of loved ones, in addition to or instead of hospice care and funeral homes.
[B]efore Valli Warren’s husband died last year after a long illness, the Stoughton couple knew they wanted a home funeral and green burial.
But they weren’t sure how to make those things happen. They turned to Sharon Stewart, who delivered ice packs to preserve the body, shared videos about how to wrap it in a shroud and taught pallbearers how to carry it out of the house on a board.
Stewart also helped Warren file paperwork, including a permit letting her transport her husband to Circle Cemetery, near Barneveld, where he was laid to rest without being embalmed or using a casket or vault.
“She walked me through every phase,” Warren said.
Stewart is a death midwife, a new kind of occupation that provides emotional, spiritual and practical support to families before and after death — in addition to, or instead of, hospice care and funeral homes.
The service, which has emerged around the country over the past decade, is analogous to what birth midwives do compared to obstetricians. Some who offer the assistance call themselves death doulas or end-of-life midwives.
‘Back to their roots’
Whatever the title, the providers say they help people “take back” the death process from hospitals and funeral homes. Services include leading family discussions about death planning, sitting vigil with people as they die, helping family and friends wash the body afterward and aiding in tasks such as selecting memorial cards, sending obituaries to newspapers and closing social media accounts. It often involves home funerals or green burials.
“We’re taking families back to their roots, the tradition of when we were born and when we died in our own homes,” said Stewart, a former detective who lives near Brooklyn, south of Madison. “We laid in honor in our parlors, and the community came together to provide care for the family.”
Liz Humphries, a former birth midwife and hospice nurse who recently added an end-of-life doula service to Seasons of Life, her senior care company in Middleton, said, “It’s about reclaiming a really sacred and beautiful human experience.”
Mary Paulauskis, a former hospice nurse from Madison, has added what she calls end-of-life transitions counseling to her business, Mindful Awakenings, through which she teaches meditation.
Paulauskis focuses on helping people think about who and what they want around them as they die. She also coaches loved ones on what to say to a dying person and how to interact — letting them know it’s OK to lie next to the person if they want to, for example.
“It’s creating a space of whatever the patient said they want,” Paulauskis said.
Many people don’t realize that there are several ways to dispose of bodies without embalming, including new, greener types of cremation, said Angie Buchanan, a death midwife in Waukesha who trains death midwives around the country. She informs clients of the options and guides them through their choice.
“We’re the water that runs between the rocks of the medical profession and the funeral industry,” Buchanan said.
Dr. Toby Campbell, chief of UW Health’s palliative care program and a board member of Agrace Hospice and Palliative Care in Fitchburg, said he understands why death midwives are catching on. He said hospice care typically includes two or three visits a week from a nurse or social worker, and an occasional call from a doctor.
“That leaves about 99 percent of the time you and your family are on your own,” Campbell said. “That’s a big space. There are giant gaps between the health care system and death, even including hospice.”
Jim Olson, president-elect of the Wisconsin Funeral Directors Association, said caring for a body after death and managing a funeral are big jobs. Most people will continue to seek help from funeral directors, he said.
Death midwifery is “another alternative for families, which we think is great,” said Olson, who owns Olson Funeral Home and Cremation Service in Sheboygan. “Am I afraid it’s going to affect my business? No, absolutely not.”
There is no licensure or government certification for death midwives. Experienced practitioners, such as Stewart and Buchanan, offer training, as does the New Jersey-based International End of Life Doula Association, which held a session in Madison last year.
Many training programs offer their own certification. The burgeoning field is in a similar situation to massage therapy in the 1990s, before doctors pushed for its regulation, Buchanan said. In Wisconsin, certification for massage therapists started in 2003, with licensure beginning in 2010.
Fees for death midwives vary. Buchanan said she charges $100 for a consultation and up to $2,000 for services covering the whole death process. Stewart has accepted donations of $100 or $200 from some clients, but she doesn’t plan to establish rates until she retires from her day job, at the state public defender’s office, and devotes more time to death midwife duties.
Paulauskis said she plans to charge $25 to $50 for a counseling session and negotiate rates for other services but let people pay what they can. An academic adviser at the UW-Madison School of Social Work, she plans to continue making her living in other ways.
Humphries, who started her end-of-life doula service last month, said she might charge $40 to $100 an hour but offer a sliding-fee scale for people with low incomes.
Humphries is also an organizer of Walking Each Other Home Madison, a group that started in 2014 to help people carry out home funerals and green burials. People can rent the group’s home funeral kit, which includes a body board, ice packs, soap, lotion, diapers, latex gloves and small bags of rice to place over the dead person’s eyes to keep them closed.
‘The personal touch’
Stewart, who has long volunteered at Monroe Clinic’s hospice program, said she saw the need for a more personal death service after her brother died in a car crash at age 19. She was 21.
Police came to the house in the middle of the night, told her mother her son was dead and left. Stewart wanted to see her brother’s body before he was embalmed, but the funeral director wouldn’t let her, she said.
“There had to be a better way,” she said.
Later, as a detective for the Lafayette County Sheriff’s Department in Darlington, Stewart tried to deliver death notifications with more sensitivity. But she wasn’t able to do all she wanted to help grieving families. After a shoulder injury forced her to retire, she discovered death midwifery.
“I thought, ‘This is it. This is the personal touch. This is the attention that families need,’ ” she said.
At a death midwife class she taught last month, Stewart told students to help dying people reconcile with others if they ask, separate arguing family members at the bedside if necessary and encourage loved ones to say goodbye and leave the room if the dying person wants to die alone.
“Your job as a death midwife is to be an advocate for that dying person,” she said.
When Laurie Larson’s husband, Dennis Presser, died suddenly from a heart attack at age 54 four years ago, Stewart helped Larson and her two teenage children navigate the chaos.
Stewart joined Larson when she met with a funeral director to plan the funeral, which took place at the funeral home.
She organized an intimate gathering for family and close friends at the crematorium, with candles, incense and music. As Presser’s body lay inside an open cardboard cremation box, people read poems, told stories and colored the box. Then they placed him in the chamber, and Larson hit the ignition switch.
“I would never have had the energy to create that beautiful ritual,” said Larson, of Madison. “Sharon helped me in so many ways that I never would have thought I needed to be helped.”
Warren’s husband, Spencer, died at 64 from amyotrophic lateral sclerosis, or ALS, also known as Lou Gehrig’s disease.
Stewart helped the couple carry out their wishes. His body remained at home for three days, instead of being whisked off to a funeral home. “I had time to be with him; it was very healing,” Warren said.
As family and friends came for the home funeral, volunteers changed ice packs beside his body as he lay on their bed for viewing. Warren drove him to Circle Cemetery, where gatherers sang and played guitar before shoveling dirt over his shrouded body.
“It was the most natural thing I’ve ever experienced,” Warren said.
[N]essa Coyle calls it “the existential slap”—that moment when a dying person first comprehends, on a gut level, that death is close. For many, the realization comes suddenly: “The usual habit of allowing thoughts of death to remain in the background is now impossible,” Coyle, a nurse and palliative-care pioneer, has written. “Death can no longer be denied.”
I don’t know exactly when my mother, who eventually died of metastatic breast cancer, encountered her existential crisis. But I have a guess: My parents waited a day after her initial diagnosis before calling my brother, my sister, and me. They reached me first. My father is not a terribly calm man, but he said, very calmly, something to this effect: “Your mother has been diagnosed with breast cancer.”
There was a pause, and then a noise I can best describe as not quite a sob or a yell, but feral. It was so uncharacteristic that I didn’t know then, and I still don’t know, whether the sound came from my father or my mother.
For many patients with terminal diseases, Coyle has observed, this awareness precipitates a personal crisis. Researchers have given it other names: the crisis of knowledge of death; an existential turning point, or existential plight; ego chill. It usually happens as it did with my mother, close to when doctors break the news. Doctors focus on events in the body: You have an incurable disease; your heart has weakened; your lungs are giving out. But the immediate effect is psychological. Gary Rodin, a palliative-care specialist who was trained in both internal medicine and psychiatry, calls this the “first trauma”: the emotional and social effects of the disease.
The roots of this trauma may be, in part, cultural. Most people recognize at an intellectual level that death is inevitable, says Virginia Lee, a nurse who works with cancer patients. But “at least in Western culture, we think we’re going to live forever.” Lee’s advanced-cancer patients often tell her they had thought of death as something that happened to other people—until they received their diagnosis. “I’ve heard from cancer patients that your life changes instantly, the moment the doctor or the oncologist says it’s confirmed that it is cancer,” she says.
The shock of confronting your own mortality need not happen at that instant, Coyle notes. Maybe you look at yourself in the mirror and suddenly realize how skinny you are, or notice your clothes no longer fit well. “It’s not necessarily verbal; it’s not necessarily what other people are telling you,” Coyle says. “Your soul may be telling you, or other people’s eyes may be telling you.”
E. Mansell Pattison, one of the early psychiatrists to write about the emotions and reactions of dying people, explains in The Experience of Dying why this realization marks a radical change in how people think about themselves: “All of us live with the potential for death at any moment. All of us project ahead a trajectory of our life. That is, we anticipate a certain life span within which we arrange our activities and plan our lives. And then abruptly we may be confronted with a crisis … Whether by illness or accident, our potential trajectory is suddenly changed.”
In this crisis, some people feel depression or despair or anger, or all three. They grieve. They grapple with a loss of meaning. A person’s whole belief system may be called into question because “virtually every aspect of their life will be threatened by changes imposed by the [disease] and its management,” Lee has written. In a small 2011 Danish study, patients with an incurable esophageal cancer reported that after their diagnosis, their lives seemed to spin out of control. Some wondered why they had received a fatal diagnosis, and fell into despair and hopelessness. “I didn’t care about anything,” one patient said. “I had just about given up.”
In the 1970s, two Harvard researchers, Avery Weisman and J. William Worden, did a foundational study on this existential plight. Newly diagnosed cancer patients who had a prognosis of at least three months were interviewed at several different points. At first, for almost all the patients in the study, existential concerns were more important than dealing with the physical impacts of disease. The researchers found that the reckoning was jarring, but still relatively brief and uncomplicated, lasting about two to three months. For a few patients, the crisis triggered or created lasting psychological problems. A few others seemed to face the crisis, then return to a state of denial, and then double back to the crisis—perhaps more than once. In the study, the researchers describe a patient who was told her diagnosis, only to report to interviewers that she didn’t know what it was—and then make it clear she wasn’t interested in receiving a diagnosis in the near future.
Palliative-care doctors used to think that a patient was either in a state of denial or a state of acceptance, period, Rodin says. But now he and his colleagues believe people are more likely to move back and forth. “You have to live with awareness of dying, and at the same time balance it against staying engaged in life,” he says. “It’s being able to hold that duality—which we call double awareness—that we think is a fundamental task.”
Whether or not people are able to find that balance, the existential crisis doesn’t last; patients can’t remain long in a state of acute anxiety. Coyle has found in her work that later peaks of distress are not usually as severe as that first wave. “Once you’ve faced [death] like that once, it’s not new knowledge in your consciousness anymore,” she says.
The existential slap doesn’t always entail mental suffering, and medical professionals who work with the dying say there are rare cases in which patients seem to skip this phase altogether, or at least experience it in a much less painful way. “People can gradually come to the realization,” Coyle says. “No one has to go through the sudden shock of awareness.”
But for most, figuring out how to adapt to living with a life-threatening disease is a difficult but necessary cognitive process, according to Lee. When patients do emerge on the other side of the existential crisis, she finds that many are better off because of it. These patients are more likely to have a deeper compassion for others and a greater appreciation for the life that remains.
To arrive there, they have to squarely face the fact that they’re going to die. “If you’re an avoidant person, and you don’t like to think about these things, that works better when life is going well,” Rodin says. “It just doesn’t work well in this situation because reality doesn’t allow it. It’s like trying to pretend you don’t need an umbrella or something, or it’s not raining, when it’s pouring. You can do that when it’s drizzling, but eventually, you have to live with the rain.”
[G]eraldine was warmly opinionated and, along with her husband, she’d raised her four daughters to be the same.
When work settled and time allowed, she melted into the couch next to any of her children who were home and turned on the Hallmark channel. If a movie showed people who couldn’t care for themselves, she would remark, “I don’t want to live like that,” or “if that’s me, don’t bother doing all that.”
On May 25, a clot blocked a blood vessel in Geraldine’s heart. Her husband performed CPR. She was whisked to the hospital, where her heart survived, but lack of oxygen launched her brain into uncontrollable seizures. At age 56, her melodic Irish accent was silenced.
Her lips sagged around a breathing tube when I met her three weeks later. Her limbs lay wherever we put them. Kinked gray hair stood in all directions from her scalp, pushed aside by electrodes that recorded brain activity.
In the small conference room in our neuro intensive care unit, we discussed Geraldine’s prognosis with her family.
“We can place a long-term breathing tube in her neck and a feeding tube in her stomach,” I said, “but there are no cases in the medical literature of someone like her living independently again. The best we could hope for is a life of near-complete dependence.”
“When we first came to the hospital, doctors told us my mom might be brain-dead,” one of Geraldine’s daughters countered. “Now, she takes breaths on her own sometimes. She’s already improving.”
Just as Geraldine was stubborn and exceptional in life, her family believed she would be exceptional in beating her prognosis.
“It might be different if my mom was 70 or 80,” her daughter went on, “but she’s only 56.”
For Geraldine’s family, the immediate fear of watching her die outweighed the unfamiliar pain of sustaining her on machines and watching her disappear in a long-term care facility.
Our medical team had seen hundreds of people like Geraldine, most of whom returned to the hospital month after month to manage complications of immobility. Sparse cases of recoveries were overwhelmed by painful, expensive, drawn-out deaths, ones we would never wish for ourselves or our own families.
But for Geraldine’s family, every decision was new. For them, nobody was like Geraldine.
In every other part of medicine, doctors make recommendations for medications, lifestyle changes and surgeries. We don’t offer cancer patients six different chemotherapy regimens and ask them to weigh the pros and cons. Yet when it comes to end-of-life decisions, doctors are terrified of violating patient autonomy. We are scared of our own medical opinions.
Instead of saying, “I recommend…,” we often offer a platter of life-prolonging measures, most of which are unlikely to improve a patient’s quality of life, but which offer the possibility of hope. The patient’s heart will still beat. Her personality will be gone, but her chest will still rise and collapse. Families see an opportunity for loss to be delayed, perhaps even dodged. Then we are surprised when they take us up on the offer to prolong dying.
“I think she would want more time to try and recover,” Geraldine’s daughter said.
So we kept Geraldine alive. A plastic breathing tube sprouted from her neck and a feeding tube with peach-colored formula buried itself in her stomach.
In the hospital, Geraldine’s family learned the common complications of immobility: infection, blood clots and bedsores.
When the infection started, a fever sounded the alarm. We counted the possible causes. Geraldine had a breathing tube in her windpipe, a feeding tube in her stomach and an IV line in her neck, each an access road for bacteria. Lying in bed put her at risk for pneumonia and urinary tract infections. Like mosquitoes in standing water, infections proliferate when the body is still.
Geraldine’s blood clots weren’t a surprise. Medical students are inculcated with the famous triad of conditions that predispose patients to clots, and Geraldine had all of them. Her body was inflamed and torn from the heart attack, infections and procedures that caused her blood vessels to release molecules that helped blood to clot. Lying in a hospital bed, not moving anything unless it was moved, her circulation slowed. Pools of static blood dried into a thick paste in her blood vessels.
Thanks to aggressive nursing care, when Geraldine developed a bedsore it was managed at an early stage. But the term “bedsore” is an understated euphemism. It recalls the annoyance of a cold sore or the tenderness of muscles after the gym. The grotesque image of bone pressing through skin is hidden.
In people who are immobilized, bedsores develop under bony prominences like the heels and the skull. At first, the skin becomes red. If the bedsore progresses, the skin’s outer layer, then the inner layer, breaks down. Finally, in the most severe stage, bone, muscles and tendons are exposed. The entire process can happen in just a few days.
Sixty days after her heart attack, Geraldine was stable enough to leave the I.C.U. She was in a persistent vegetative state — unresponsive to external stimuli. She opened her eyes, as if she were about to say something, but nothing ever came out. Her gaze roved around the room. An ambulance took her to a long term care facility, where she was dependent on machines and people.
“When you first hear someone you love is sick, you think it’s a short term thing,” her daughter told me over the phone a month later. “It’s adjusting to the long term aspect that’s hard.” Geraldine’s daughter woke up at 5 a.m. every day to spend time with her mom before work.
“I think it’s more of a disappointment for my dad,” she said. “He told us that if he ever gets sick, he doesn’t want any of this.”
Geraldine’s family lived between hope and guilt, with the weight of each side in flux. “If my mom knew what we were doing right now, she’d probably be mad at us,” her daughter reflected a few weeks ago.
Yet in the same breath, her voice rose and she said: “My mom’s a fighter, so I think she would be happy with us giving her a shot. We’re hoping for this miraculous turnaround.”
It did not come. Geraldine died of sepsis earlier this month, after more than four months of care.
“People don’t know what they’re in for,” Geraldine’s daughter reflected after the funeral. “It hurt all of us to see her like that.”
In the final days of Geraldine’s life, a doctor asked if the family of another patient in the I.C.U. could visit Geraldine to see what prolonged dying looked like. Geraldine’s family was kind enough to agree.
The visiting family chose to transition their loved one to hospice care.
[T]here’s been an unexpected, and excellent, consequence to California’s new medical aid-in-dying law. For many terminally ill patients, immersion in the process of securing lethal drugs ultimately renders them unnecessary. How did this come about?
Passed by the California legislature in late 2015, the End of Life Option Act allows physicians to prescribe a lethal concoction of drugs to some patients with terminal illnesses who meet certain criteria. The law, commonly described as providing “medical aid in dying,” took effect on June 9, 2016. It stipulates only that the requesting patient be considered terminal (less than six months away from death), possess full decision-making capacity, and be physically able to self-administer the life-limiting drugs. Although the physician is obligated by law to inform the patient of alternative care options, such as psychological counseling or symptom management with palliative care services, there is no direct requirement that the physician arrange or provide them. In its barest form, the option can serve as a dispensary for life-ending medications.
California’s medical community was taken by surprise by the rapid passing of the law in late 2015. It came on the heels of the dramatic case of Brittany Maynard, a young woman with terminal brain cancer who elected to move from California to Oregon to access medical aid in dying under that state’s Death with Dignity Act. Hospital systems and physicians in California suddenly found themselves with an urgent need to rapidly formulate policies around this new right of patients. Some, such as the Catholic Health Systems, opted out on religious grounds. Others scrambled to put basic policies in place for patients who met inclusion criteria. And some institutions decided to put significant time and resources into supporting this new legal reality in the most comprehensive way possible.
One standout example is the University of California, Los Angeles (UCLA) Health Centers. After literally thousands of hours of discussion, the working group determined that the intake process for patients requesting medical aid in dying should be conducted by trained psychotherapists (psychologists and clinical social workers) instead of physicians. Dr. Neil Wenger, director of the UCLA Health Ethics Center, led the effort to create processes and infrastructure to respond to this law. “We wanted to be able to offer a service that doctors tend to gloss over,” he said, when asked why they chose to lead with talk therapy. The intake consisted of an extensive set of questionnaires designed to assess all possible sources of distress. Any patient with physical or psychiatric needs was referred on to the appropriate services. But as the UCLA committee expected, most of what patients needed was to discuss their feelings about their approaching death and process their grief and sense of loss. This mirrors data from the entire state of California as well as Oregon, which suggest that the distress prompting patients to request these lethal medications primarily stems from their fear over losing control at the end of life. It is not, as many may think, due primarily to physical suffering.
The intake questions explored goals of care, quality of life, and patients’ emotions around their impending deaths: Were they ready? What scared them? What made them anxious? Did they feel their lives were complete? What did they feel makes life meaningful? What decrements in quality of life are too great? What haven’t they said and to whom? Anne Coscarelli, psychologist and founding director of the Simms/Mann–UCLA Center for Integrative Oncology, described the conversations that came from this intake process as revelatory and comforting for the patients. Several patients ultimately completed legacy projects, such as video or written messages and stories, for their children and grandchildren. This invitation to talk, which opens up a discussion that most of us are taught to avoid, turned out to be a game-changer.
Only a quarter of the patients ultimately went on to ingest the lethal drugs they came requesting. The actual data is more complex: Some who requested this service did not meet the basic requirements to receive it. Others died before they had a chance to ingest the medications. But the staff from UCLA reported case after case in which patients’ goals shifted from wanting to hasten their deaths to deciding to live out the remainder of their lives.
Ours is a culture that does not talk about death, even when it should be impossible to ignore. Despite the fact that 89 percent of people think that it is a doctor’s responsibility to discuss end-of-life care with their patients, in reality, only 17 percent of patients report having had such a conversation, according to a 2015 survey from the Henry J. Kaiser Family Foundation. As a doctor who practices both critical care and palliative care medicine, I have presided over thousands of deaths. Most of my patients have suffered with chronic illnesses for years: metastatic cancers, failing lungs, and progressive debilitation from dementia. And yet almost none of them have discussed their own death with their doctors, or even their families. Most have no idea that they are actually dying. In this culture that operates on a fantasy of immortality, with unrealistic promises made by television shows and advertisements, doctors see themselves as failures if they are unable to cure their patients. We physicians are trained to lead patients into battle after battle, into the next procedure or intervention, banking always on that magic pill or miracle cure.
This broad cultural unwillingness to acknowledge death results in a phenomenon I call the “End-of-Life Conveyor Belt,” where high-tech treatments are automatically attached to bodies as they progress through the stages of dying. As the baby boomers age and our treatment options blossom, more are being exposed to the suffering brought about by these protocols. The tremendous anxiety we see over loss of control is understandable. It is no wonder that people in many states have asked for, and finally won, the right to take back that control with a pill.
The effort by UCLA Health seems to be working. Placing highly trained psychologists and clinical social workers in the critical role of “first responder” to a patient’s request to hasten death has rendered many of these requests obsolete. In choosing this approach, UCLA is effectively “de-medicalizing” the experience of dying by prioritizing the need for deep reflection. In this way, the program provides patients with an option that doctors are not primarily trained for.
Patients requesting support to hasten their deaths are only a small subset of the population of the dying. They are in some ways canaries in a coal mine, their request for medical aid in dying is alerting us to the unmet needs of the wider population of dying patients. And what I am seeing is that our new legal responsibility to steward these patients responsibly through this rocky terrain will build practices and skills that will help all of those at the end of life.
Where goes California, thus goes the nation. California was the fourth state to legalize medical aid in dying and has since been followed by two more. And UCLA’s approach, with trained psychologists guiding patients through this tricky terrain, shows us the way. Let’s take advantage of this wave to take better care of all our seriously ill patients. And let’s make sure we give patients what they really need and hope that lethal drugs are always the last tool in the toolbox.