The Lady And The Reaper (La Dama Y La Muerte) de Javier Recio Gracia


The Amateur's Guide To Death & Dying
Enhancing Life Near Death
By George Harrison
[T]HESE are the shocking true stories of the unfortunate people who died whilst having sex.
The tragic stories highlight a dangerous side to everyone’s favourite pastime, so remember to take care next time you get your rocks off.

One man recently met a sticky end after being crushed by a mountain of pornographic magazines.
The Japanese man, named as 50-year-old Joji, was found six months after his six-tonne stash of porn magazines fell on him.
Cleaners tasked with tidying his neglected flat found that the entire apartment was rammed with the explicit magazines.
It is unknown whether the man, a former car-manufacturer, had died from a heart attack and then fell into a stack of pornography, or whether he was crushed to death by his X-rated collection.
In 2007 a couple from Columbia, South Carolina, fell to their deaths after plunging naked from the roof of an office building.
The bodies of Brent Tyler and Chelsea Tumbleston, both 21, were found by a taxi driver in the middle of an otherwise-empty street at 5am.
The couple’s clothes were later found on the roof of a nearby building, where they were believed to have been having a risky outdoor romp before falling from the roof.
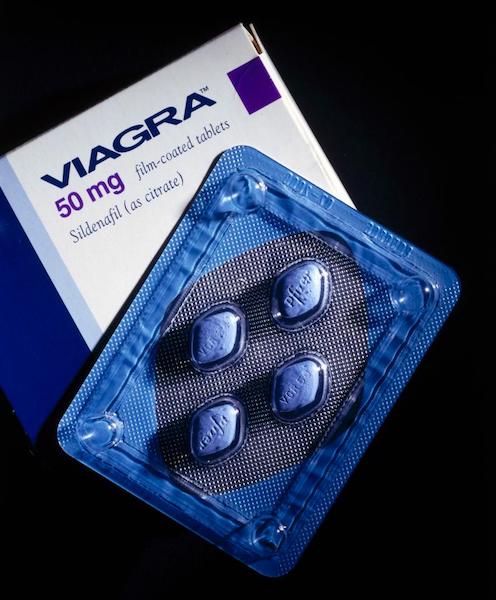
A Russian man died in 2009 after completing a 12-hour orgy with female pals, who had bet him over £3,500 that he couldn’t keep going for half a day.
Minutes after completing the bet, mechanic Sergey Tuganov died of a heart attack, which had been caused by the huge quantity of Viagra he had guzzled to prepare him for the task.

In 2013, a Zimbabwean news website reported that a couple were attacked by a lion after having sex in the bush.
The big cat killed Sharai Mawera after interrupting the couple, although her unidentified lover managed to run away before he could be killed.
After notifying the police, the male lover, who escaped wearing only a condom, found the woman’s mauled body at the scene of the attack.
Donna Lange, 51, smothered her lover to death inside a mobile home.
The intoxicated woman, from Washington, claimed she didn’t know how the man died, although a witness claimed to have seen her crush his face with her chest.

A trainee doctor, Zheng Gang, died of a heart attack in 2011 – after over-exerting himself whilst producing a sample at a sperm bank.
The 23-year-old was pronounced dead at the scene of China’s Wuhan University, where he had spent two hours inside a booth, having already visited four times that week.
A cop died in 2009 when his heart gave out during a threesome – and his wife sued his doctor for not warning him against having sex.
William Martinez, a 31-year-old Atlanta police officer, died whilst having sex with another woman and a male friend.
But his wife won $3 million (£2.4 million) after suing his doctor for not warning him that he had a weak heart, and should avoid strenuous activities.
A sick neo-Nazi roleplaying session ended in tragedy, after 38-year-old Simon Burley died when a sex game with lover Elizabeth Hallam went wrong.
The hanging-enthusiast had a noose fitted around his neck whilst his lover played the part of a Nazi executioner, who hanged him as part of a sex game they were playing.
Unfortunately, the knife she planned to cut him down with was blunt, and the man was left to suffocate to death at his house in Grimsby.
Complete Article HERE!

[T]wo years after an abrupt price hike for a lethal drug used by terminally ill patients to end their lives, doctors in the Northwest are once again rethinking aid-in-dying medications — this time because they’re taking too long to work.
The concerned physicians say they’ve come up with yet another alternative to Seconal, the powerful sedative that was the drug of choice under Death with Dignity laws until prices charged by a Canadian company doubled to more than $3,000 per dose.
It’s the third drug mixture recommended by the doctors whose medication protocols help guide decisions for prescribers in the six U.S. states where aid-in-dying is allowed.
The first Seconal alternative turned out to be too harsh, burning patients’ mouths and throats, causing some to scream in pain. The second drug mix, used 67 times, has led to deaths that stretched out hours in some patients — and up to 31 hours in one case.
“[Twenty percent] of the cases were three hours or more before death, which we think is too long,” said Robert Wood, a retired HIV/AIDS researcher who volunteers with the advocacy group End of Life Washington, in an email. “The longest was 31 hours, the next longest 29 hours, the third longest 16 hours and some eight hours in length.”
Patients and families are told to expect sleep within 10 minutes and death within four hours. When it takes far longer, family members get worried, even distressed, said Dr. Carol Parrot, a retired anesthesiologist who has prescribed drugs for dozens of aid-in-dying patients in Washington.
The doctors say this can be addressed with larger doses of the three drugs they have been using — diazepam, often used to treat anxiety; digoxin, used to treat heart issues; and morphine, a narcotic pain reliever — plus another heart medication, propranolol, in a four-drug cocktail aimed at quickly inducing death, Wood said.
Parrot and Wood are part of a seven-member group of doctors in the Northwest who came up with the three-drug protocol after Valeant Pharmaceuticals Inc. acquired the rights to secobarbital, known as Seconal, in 2015 and raised the price sharply.
“We wanted the new drug regime to be safe, reliable and effective — and cost $500 or less,” said Parrot.
Since 1997, when Oregon’s Death with Dignity law became the first in the nation, doctors had relied on fast-acting, relatively inexpensive barbiturates — either secobarbital or pentobarbital — for patients with terminal diagnoses who sought aid in dying in Oregon, Washington, California, Colorado, Montana and Vermont. The practice also has been approved in Washington, D.C., but is being reviewed by Congress.
Pentobarbital became unavailable after drugmakers blocked its use in U.S. death-penalty executions.
Concerns about the overly long deaths surfaced last summer, Parrot said. Nearly all of the problems occurred in patients already taking high doses of opiates.
“We run into patients who are so tolerant or dependent on narcotics that even the astronomically high doses of oral narcotics in our prescription do not stop them from breathing,” she said.
If patients have diseases that slow or alter normal organ function, it can affect the speed and amount of drugs absorbed in the small intestine, metabolized in the liver and sent to the rest of the body. Very large patients, too, may require larger doses.
Deaths aren’t required to be supervised, and no doctor was present with the unidentified patient who took 31 hours to die, so doctors would only be speculating about the reason, Parrot said.
Not all patients — or doctors — experienced overly long deaths with the previous drug mixture. Dr. Lonny Shavelson, a Berkeley, California, physician who has supervised two dozen aid-in-dying deaths under California’s new law, said it worked fine.
“My personal experience is, I haven’t had long deaths with it,” Shavelson said.
And not all doctors think long deaths are a problem. In Oregon, even with fast-acting barbiturates, time to death has ranged from one minute to 104 hours during the 20 years the law has been in effect, state records show.
“I’ve heard stories where it took quite a number of hours to die, and it was fine,” said Dr. David Grube, an Oregon-based medical director for the advocacy group Compassion & Choices.
Scott and Amy Kreiter, of Wenatchee, didn’t know what to expect when Scott’s mother, Patricia Hansen, 69, decided to take the lethal drugs on Dec. 26, 2016. Hansen, a lively woman who once ran a gourmet ice-cream business, had endured frequent hospitalizations for end-stage kidney failure, congestive heart failure and other ailments.
“She said, ‘I want to listen to Willie Nelson, I want to play a game of Scrabble, I want to drink a Rob Roy or two, and then I want to be done,’ ” said Scott Kreiter, 47.
Hansen proceeded to “kick our butts” at Scrabble, her son said — including fulfilling a goal of getting a triple-word score with a dirty word. Then she mixed the drugs with scotch and drank the solution.
“She didn’t complain. She just took it,” her son recalled. “She said, ‘You thought I’d chicken out, didn’t you?’ ”
Within two minutes of downing the mixture, Hansen was asleep. Within 20 minutes, her breathing had stopped.
“We thought it would take one to two hours,” Amy Kreiter said. “It if had gone on for hours, we would have thought we did it wrong.”
Critics of aid-in-dying say growing reports of overly long deaths underscore their objections. Dr. David Stevens, CEO of Christian Medical & Dental Associations, which has tried to halt or reverse laws, said coming up with new drug protocols could eventually be a step toward Holland’s practice of allowing euthanasia by lethal injection “so the patient could be killed ‘humanely.’ ”
“We are heading down that same path,” Stevens said in an email.
But Parrot and other frequent prescribers of aid-in-dying drugs say they are looking for the best way to honor the wishes of patients in states where the practice is allowed. Doctors recently began using the newest drug mixture and will gather data about its effectiveness.
“We’re not experimenting,” Parrot said. “We are working with available drugs to provide dying patients a comfortable, peaceful death that is reliable and safe for them and comforting for their families as well.”
Complete Article HERE!

[O]bese people in the U.S. may not receive the same kind of care at the end of their lives as people who are thin or normal weight, suggests a new study.
Before they died, obese patients were less likely to enroll in hospice care, spent less time in hospice and were less likely to die at home than thinner people, researchers found.
End-of-life care was also more costly for obese people.
“People with obesity deserve high-quality care, but may not be receiving it at the end of life,” said lead author Dr. John Harris, of the University of Pittsburgh School of Medicine in Pennsylvania.
More than a third of U.S. adults are obese, according to the U.S. Centers for Disease Control and Prevention.
Harris and his colleagues note in the Annals of Internal Medicine that aside from health risks, obesity may present technical and logistical challenges during physical examinations and certain medical procedures.
Previous research also shows that stigma about weight affects how doctors and patients behave, they write.
To see how body weight is linked to healthcare at the end of life, the researchers used data collected between 1998 and 2012 from 5,677 people on Medicare, the U.S. government’s health insurance program for the elderly and disabled.
None of the participants were living in nursing homes or other institutions. The data were drawn from the last six months of their lives.
Based on body mass index (BMI), a measure of weight in relation to height, 7 percent of participants were underweight with a BMI of 18.5 or below, 44 percent were normal weight with a BMI of 18.5 to 24.9, 31 percent were overweight with a BMI of 25 to 29.9 and the rest were obese or morbidly obese with a BMI of at least 30.
A 5-foot-5-inch person weighing 120 pounds would have a BMI of 20, in the normal range. A person of the same height who weighed 240 pounds would be morbidly obese, with a BMI of about 40. The National Heart, Lung and Blood Institute provides a BMI calculator online (bit.ly/2lHXqP2).
The researchers found a 38 percent probability that people with a BMI of 20 would enter hospice care toward the end of life, compared to about 23 percent among people with a BMI of 40.
Hospice care, which can be provided in home or at a facility, provides physical support, including pain control, and emotional support for patients and families dealing with terminal illnesses.
When people with a BMI of 40 did receive hospice care, it was typically for a shorter time than normal-weight people.
“It’s looks like people weren’t getting enrolled, and they got there later if they were enrolled,” Harris told Reuters Health.
The researchers also found that obese people had lower odds of dying at home, which is a typically a wish for people at the end of life. Their likelihood of dying at home was 55 percent, compared to 61 percent for normal-weight patients.
Gaps in care generally rose as BMI increased, the researchers found.
“It seems like people with obesity are getting lower quality of care at the end of life,” said Harris.
The cost of care was also higher when BMI was higher, they found.
The study can’t say why these gaps exist, but the researchers suggest it may have to do with obese people looking less gaunt toward the end of life and not being referred for hospice. Or, they may be unable to find a hospice program that can accommodate their healthcare and family’s needs.
The healthcare systems needs to make sure it’s offering everyone the same level of care, said Harris.
His overarching goal, Harris said, is to improve the quality of care for people with obesity.
Complete Article HERE!
[T]he psychiatrist William Breitbart lives at the edge of life and death. As chairman of the Department of Psychiatry and Behavioral Sciences at Memorial Sloan Kettering Cancer Center in New York, Breitbart specializes in end-of-life care for terminally ill cancer patients. For many of his patients, the most pressing question isn’t when they’ll die or how painful death will be. Rather, it’s what makes life meaningful. They are in search of a meaning that cannot be destroyed by death.
Is there one?
Breitbart has spent the better part of his career trying to answer that question. His ground-breaking research shows that while the specter of death often leads people to conclude that their lives are meaningless, it can also be a catalyst for them to work out, as they never have before, the meaning of their lives.
When people believe their lives are meaningful, according to psychologists, it’s because three conditions have been satisfied: They feel their existence is valued by others; they are driven by a sense of purpose, or important life goals; and they understand their lives as coherent and integrated. Psychologists and philosophers say that the path to meaning lies in connecting and contributing to something that is bigger than the self, like family, country, or God.
Meaning and death, Breitbart believes, are the two sides of the same coin—the fundamental problems of the human condition. How should a human being live a finite life? How can we face death with dignity and not despair? What redeems the fact that we will die? These questions roll around Breitbart’s mind every day as he works with patients facing life’s end.
Breitbart’s interest in meaning took root in his childhood. Born in 1951, Breitbart grew up on the Lower East Side of Manhattan. His parents, Jews from eastern Poland, narrowly avoided Hitler’s death camps. When they moved to America, they carried their memories of the war years with them. Breitbart’s childhood was steeped in that tragic past. Every morning, his mother would ask him at the breakfast table, “Why am I here?” Why, she wondered, did she live when so many others had died?
“I grew up with a sense of responsibility to justify my parents’ survival and to create something in the world that would be significant enough to make my life worthwhile. It’s no coincidence,” he laughed, “that I ended up at Sloan Kettering.”
Breitbart began working at the hospital in 1984 during the height of the AIDS epidemic. Young men his age were dying all around him. As he tended to them, “They were constantly asking me to help them die,” he said. He was also working with terminal cancer patients. “When I walked in the room, they would say, ‘I only have three months to live. If that’s all I have, I see no value or purpose to living.’” They told him, “If you want to help me, kill me.”
If death means non-existence, Breitbart’s patients reasoned, then what meaning could life possibly have? And if life has no meaning, there’s no point of suffering through cancer.
By the ’90s, physician-assisted suicide was a hot topic in Breitbart’s circles and beyond. The doctor Jack Kevorkian had helped his first patient end her life in 1990. As the United States debated the ethics of assisted suicide, other countries were taking steps toward normalizing the practice. In 2000, the Netherlands became the first nation to make physician-assisted suicide legal. Today the practice is legal in the United States in California, Vermont, Montana, Washington, and Oregon.
As Breitbart heard more stories of assisted suicide, he began to wonder what specifically was driving the terminally ill to give up on life. At the time, he was doing research studies on pain and fatigue at the end of life, so he tacked onto those studies some questions that asked his subjects whether they felt a desire for a hastened death. What he discovered surprised him.
They no longer wanted to die. Their spiritual wellbeing improved. They reported a higher quality of life.
The assumption had been that the ill chose to end their lives because they were in terrible pain. But Breitbart and his colleagues found that wasn’t always the case. Instead, those who desired a hastened death reported feelings of meaninglessness, depression, and hopelessness. When Breitbart asked patients why they wanted a prescription for assisted suicide, many said it was because they had lost meaning in life. Unlike clinical depression, which has a specific set of diagnosable symptoms, meaninglessness was more of an “existential concern,” Breitbart said—a belief that one’s life has little value or purpose and is, therefore, not worth living.
Breitbart knew he could treat depression—there were medicines and well-developed psychotherapies for that—but he was stumped when it came to treating meaninglessness. Then, in 1995, he began to see a way forward. He was invited to join the Project on Death in America, which aimed to improve the experience of dying. Breitbart and his colleagues on the project—including philosophers, a monk, and other physicians—had long conversations about death and the meaning of life, “peppered with references to people like Nietzsche and Kierkegaard and Schopenhauer,” Breitbart said. “What I suddenly discovered,” he explained, was that “the search for meaning, the need to create meaning, the ability to experience meaning was a basic motivating force of human behavior. We were not taught this stuff at medical school!”
Breitbart became convinced that if he could help patients build meaning, he could decrease their suicidal thoughts and make their lives worth living even to the very end.
He developed an eight-session group therapy program where six to eight cancer patients come together in a counseling workshop. Each session, in one way or another, helps build meaning. In the first session, for example, the patients are asked to reflect on “one or two experiences or moments when life has felt particularly meaningful to you.” In the second session, patients respond to the question “Who am I?” to tap into the identities that give them the most meaning. One woman responded saying, “I’m somebody who can be very private … [and] have been working on accepting love and affection and other gifts from other people.” In subsequent sessions, they share their life story with the group and think about the role that love, beauty, and humor played in their lives.
In the final session, the patients reflect on the part of them that will go on living even after they are dead—their legacy. That could be their soul, or it could be something they helped to create that will continue to exist—their children, a work of art, or an organization. They present a “legacy project” to the group, generally something they do or create that represents how they want to be remembered. One man brought in a woodcut of a heart sculpted into a Celtic Trinity. “This is what I will teach my children,” he said, “that there is eternal love, and that I will be there for them, far beyond my passing.”
Breitbart performed three randomized, controlled experiments on the meaning-centered psychotherapy. When he analyzed the results with his colleagues, Breitbart saw the therapy had been transformative. By the end of the eight sessions, the patients’ attitudes toward life and death had changed. They were less hopeless and anxious about the prospect of death than they were before they began the program. They no longer wanted to die. Their spiritual wellbeing improved. They reported a higher quality of life. And, of course, they found life to be more meaningful. These effects not only persisted over time—they actually got stronger. When Breitbart followed up with one group of patients two months later, he found that their reports of meaning and spiritual wellbeing had increased, while their feelings of anxiety, hopelessness, and desire for death had decreased.
The time between diagnosis and death, Breitbart has found, presents an opportunity for “extraordinary growth.” One woman, for example, was initially devastated by her diagnosis of colon cancer—but after enrolling in the therapy program, she realized, “I didn’t have to work so hard to find the meaning of life. It was being handed to me everywhere I looked.” And that realization ultimately brought her—and Breitbart’s other patients—some measure of peace and consolation as they faced life’s final challenge.
Complete Article HERE!

By Dr. Henri Bianucci and Dr. Perry Jameson
It is hard not to take my (Perry Jameson) personal experiences and apply them to my work as a veterinarian. One of the most difficult times in my life was when my mom was diagnosed with metastatic renal cell carcinoma.
She was a healthy woman in her 50s who was still teaching third-graders and playing tennis. Mom developed a mild persistent cough and soreness in her hip. At first, they thought she had bronchitis and pulled a muscle playing tennis. When her symptoms did not resolve as expected, the doctors started looking further and, unfortunately, found she had a kidney tumor that had spread to her hip bones, lungs and spine.
At the time there was no effective therapy for this cancer and she progressively worsened over the next eight months. I would drive home every other weekend to help my sister and Dad, who were caring for her. As we struggled with her end-of-life care, I kept asking myself that certainly we were not the first family to face this and there must be someone out there to guide us.
Finally when her oncologist realized she was going to die soon, he recommended we get in touch with hospice. They came in and immediately were able to make her more comfortable and teach us how to do the same. Unfortunately, this was only during the final two weeks of her life.
In my practice, we deal weekly with patients who have cancer, heart failure, renal failure and other terminal illnesses. We do our best to help guide pets and their parents through this end-of-life stage. Last year, the American Animal Hospital Association, along with the International Association for Animal Hospice and Palliative Care, released guidelines to help veterinarians with end-of-life care for pets.
These guidelines were a collaboration of ideas and experiences from multiple university and private practice hospitals. As with my experience with my mom, it was a realization that we were not the only animal hospital dealing with this and we could learn from others how to help with this stage of a pet’s life.
Their first focus was to recognize that the end of life is, in fact, a stage of life. Just as juvenile, adult and senior are recognized stages, so is this final life stage. The importance of this is by recognizing earlier when a pet reaches this stage we can institute animal hospice sooner.
The authors developed the Animal Hospice Care Pyramid (http://bit.ly/2lwl55K) to display the different needs of a pet during the final stage of life. At the base are the physical needs of the patient. The middle section stresses the social needs, while the top emphasizes the emotional needs. All three areas must be considered when trying to bring quality to the end of a pet’s life.
The physical needs always seem obvious, but it is good to have a list to make sure we do not miss anything that may help them be more comfortable. These needs are pain management, control of any clinical signs (e.g. nausea), hygiene, nutrition, mobility and providing a safe environment.
Pets are social; they want to be around other family members, especially when they are not feeling well. This portion of the pyramid reminds us to ensure the pet is able to interact with its family, including other pets, and has some form of mental stimulation. When our Lab, Ariel, was near the end of her life and had difficulty walking, we put her bed in the middle of the den. This way she could watch all that was going on and we could easily interact with her.
The top of the pyramid stresses the importance of the pet’s emotional well-being. By supporting the social and physical needs most of their emotional needs will be met. Preserve their dignity by minimizing and cleaning up any house soiling as soon as possible. Pets are most comfortable with the same routine, so by keeping the same patterns you did before their illness, you will reduce their stress. Most pets are there to be our companion, so by keeping them as part of the family, you will encourage their will to live.
This guide also helps with when we make a decision about ending our pet’s life. If we can no longer meet their physical needs (comfort, they stop eating), and they withdraw from the family, then they are no longer enjoying life.
The goal is to make this final stage of our pet’s life the best it can be, but to also aid us when to say goodbye. Our pets do not live as long as we do so everyone pet parent will need these guidelines sooner or later.
Complete Article HERE!
The End-of-Life Doula Approach
Dying from a terminal illness takes months, often years. As a dying person’s functional ability declines, the demands on caregivers increase. So, by the time the dying person’s body starts its final process of breaking down, the family is likely to be exhausted emotionally and physically. Yet, at this point, family feels called on to be even more present, because they recognize the end is near. They could use increased support, but professional medical help is only sporadically available—and often not there in the critical moments, when a new symptom appears or one worsens in a way the family wasn’t prepared for. If the dying person is at home on hospice care, a nurse, social worker, or chaplain will call at a crisis moment and even try to visit. But, due to the number of other patients they serve and the time it takes to get from one location to another, they often can’t respond quickly enough or actually get there when it matters most. The structure and logistics of hospice care just don’t allow for the best care at the very end of life.
The same is true if a person is dying in a hospital or other facility. While professionals may have easier access to a dying person—because they don’t have to travel to get from one patient to another—they are still limited by their shift schedules and the number of other patients they have to serve. On weekends and at night, when there are far fewer staff members, the problem gets even worse.
So, for the last hours to days of life, a dying person and the family may feel the full weight of the dying process on their shoulders and have minimal assistance. They can feel abandoned, alone, and ill-prepared. Their focus narrows to basic physical care, they stuff down their emotions as best they can, and they move through the experience in a disconnected daze. I have seen this over and over again in the families of dying people, and I experienced it in my own family when my father was actively dying fifteen years ago.
Even though my mother had hired an aide to help with my dad’s care in the last couple of months, she was hardly sleeping at night and on edge during the day as she saw to all my dad’s needs. My dad was ninety years old, and my mom was seventy-seven at the time. Until the last week or so, she maintained the household and went to work every day, managing a forty-story commercial building in the middle of Manhattan. My sister lived across town and helped out many days during the week. I lived an hour and a half away, so I could only get down once a week or, on occasion, two times in a week.
On the days I could be there during the last few weeks, I slept in a bed right next to my dad. I made my mom sleep on the couch in the living room, so she wouldn’t be disturbed during the night by every sound my father made or his slightest movement. But even with all this help, my mother was beyond exhausted.
Although my father went through his dying process years before I formulated the end-of-life doula approach, I was at that time a hospice social worker. Still, we as a family cared for my father and lived our daily lives behind a heavy drape of denial that kept out the truth of his dying. For a time, my sister clung to the idea that a new pinpoint radiation technology might cure him. For a long time, we all held on to the belief that we might hold death at bay and have more time with him. There were times when his decline seemed to pause. Although his functional deterioration was profound, in those times he seemed to hold his own against further descent toward death—and we would believe in our denial again. But then the process would continue, and the truth of his dying would break through our denial.
Four days before he died, we knew that death was close. He had stopped eating weeks earlier. Now he was “sleeping” all the time. It was painfully obvious that his body had entered the final process of breaking down; all his systems were failing. In those last days, my father’s dying process weighed on all of us considerably. We didn’t talk much about the feelings we were experiencing, but I could see it on my mother’s and sister’s faces, and I’m sure they could see it on mine. At least I knew enough about the process to inform my mother and sister about some of the signs and symptoms we witnessed. But I also remember wishing that a dispassionate outsider, one with more knowledge than I had, could be there to help us read the signs more clearly and to support us emotionally. Of course we supported each other the best we could, but it wasn’t really enough. I remember feeling very alone. And, during the last several days, I don’t remember the hospice nurse coming more than once—and then only for perhaps an hour.
I spent the entire night before my father died in the bed next to him. I remember that a lamp on the night table cast a pale yellow light across half the bed, leaving the rest of the room mostly dark. My father was a little restless, and the slightest movement or sound he made kept me from falling asleep. I didn’t know that night how close he was to dying, but it was clear that his death wasn’t far off, and thoughts of what life would be like without him kept swirling around in my head. All my life, my dad had been a gentle, sweet presence. Somehow I couldn’t imagine the world without him.
At 6:00 a.m. I left to go back home. It was a Thursday, and there was an event in my older son’s class that morning that I wanted to attend. But as soon as I arrived home, my wife told me that my mom had called to say that I should go back because my dad had taken a sudden turn for the worse. I kissed my kids and left without even washing my face or brushing my teeth.
When I reentered my father’s bedroom I saw that his limbs looked very stiff, and he didn’t move at all. The only motion in his body was the shallow rise and fall of his chest as he breathed—and each time he exhaled, his chest remained motionless for a long pause before the next inhalation. I settled into watching him, perched on the side of the twin bed just a foot from where he lay. For the next three hours his breath continued to slow, with longer and longer periods of apnea. In the late morning, the aide arrived and came to sit in the bedroom as well. My mother and sister came in at points and spent time sitting near him. Finally, my legs and back stiff from sitting, I decided to walk to the kitchen to stretch and get a drink of water. My sister and the aide were sitting off to the side near the windows, talking to each other. I was out of the room for at most three minutes.
As I stepped back into the bedroom, I saw that my father wasn’t breathing. I stopped in the entrance to the room, frozen by his stillness, waiting to see if the next in-breath would come before I went back to sitting at his bedside. After a minute of waiting, I realized that he wasn’t going to breathe again. My sister and the aide, who hadn’t been looking over at my dad, realized that I wasn’t coming farther into the room and asked me if he was gone. By now almost another minute had passed.
“I think so,” I said, then went to get my mom. We all huddled together on one side of the bed, holding each other and watching for several more minutes before we called the hospice nurse to let her know that my father had died. The nurse hadn’t visited him for the past three days.
Looking back, I don’t remember immediately feeling guilty about going to the kitchen and missing his last breath. My father had never talked about wanting us to be with him when he died. In fact, knowing my father, he would have only wanted his death to be as easy as possible for all of us. He would have said we should do whatever was best for us. But, as the fact that he had actually died became more real and we made preparations for his funeral, that feeling of guilt wormed its way into my thoughts, and I realized that unconsciously this had been important to me.
He was buried three days later, on a Sunday, with swirling flakes of snow like bits of paper falling from the sky. It was bitter cold for early April, chilling us as we stood around his open grave. I remember my wife clutching me as we huddled together with my mother and sister. The rabbi read prayers I didn’t understand, yet their rhythmic, melancholy sound was so familiar. There is something in Jewish prayer that always sounds to me like a cry from the heart, a cry of deep, unfulfilled yearning. I could feel that cry in my heart as I watched the flecks of snow starting to coat the top of the huge pile of orange-brown dirt at the side of the grave. I stopped hearing the prayers and turned inward, silently apologizing to my father for not staying next to him and holding his hand as he took his last breath.
In the days that followed, I found myself apologizing over and over again but not being able to let go of the guilt. When those thoughts came up, I would berate myself for going to the kitchen at just the time when he was dying. It felt as if I had abandoned him just as he needed someone who loved him to be at his side. Many months later, I finally arrived at a rationale that began to ease my guilt. I started to weigh those last moments of not being there against all the hours of caring for him in the seven months of his illness. I added into that equation the many times I had told him I loved and admired him.
Even though I came to accept that my not being present for my father’s last breath was okay, I still would rather have been present. In the years that followed my father’s death, I came to know the dying process a lot better. Now I can read the signs of imminent death. If my father were dying today, I would not leave his bedside when those signs were present. And now I teach those signs to other people so they won’t have to struggle with months of guilt as I did.
Not being present at the end of a loved one’s life is only one way a death can cause unnecessary anguish. Sometimes people end up going to the hospital, even though they didn’t want to die there; sometimes relationships that could be healed, or at least improved, are left hanging, because death is never discussed; sometimes the spiritual distress of the person dying goes unrecognized or unattended. All these failures, and many others, result in deaths with extra layers of suffering that could have been avoided.
It isn’t just the negative events and circumstances that make many deaths so unfortunate; there are missed opportunities for deeper meaning and greater comfort that most people don’t even realize can be part of the experience. Over the last one hundred or more years, as a result of the rise in hospitals and health-care technology, death and dying have become highly medicalized. There have been a number of regrettable side effects from this development. For one thing, people don’t attend to the internal impulse to explore the meaning of their life. For another, advances in technology and medicines extend life in a state of dramatically diminished quality, which only increases physical and emotional suffering for the dying person—and, by extension, for the family.
As a hospice social worker, I encountered these negative aspects of dying every day. They are what propelled me to contemplate a different approach to death and dying, which resulted in my formulating the end-of-life doula approach with its emphases on meaning, legacy work, planning, attention to the sacred nature of dying, alternative interventions for symptom management, intense involvement in the last days of life, reprocessing the experiences with loved ones after the death, and, finally, active involvement in early grief. This model has stayed fundamentally the same over the last thirteen years. Nonetheless, some aspects of it have evolved and become much more important as the movement it spawned has grown. I expect that it will continue to evolve as other developments in the field of death and dying are incorporated into the model.
The end-of-life doula approach encompasses three different areas of activity. The first of these involves the dying person reflecting on their life and planning for how they envision the last days of life to unfold. The second area centers on holding the space for the plan of those last days, when the body is finally breaking down. The last part of the program begins shortly after the person dies, as family and friends process their experiences of the dying time and begin their work on grief.
Reflection
According to developmental psychologist Erik Erickson, the impulse to reflect on one’s life is an inborn imperative that naturally occurs as a person  reaches the last stage of life: old age. Erickson saw different chronological periods of life presenting developmental challenges that led to either greater personality wholeness and a sense of well-being or poorer adaptation to the world and a contracted sense of self. He named each developmental stage with the words that defined the crisis at the center of its psychosocial challenge. He called the last stage of the lifespan “Ego Integrity vs. Despair.” At the heart of the conflict between ego integrity and despair are two questions: “Has my life had meaning?” and “Has my life been satisfying?” How a person answers these questions leads in the direction of either ego integrity or despair.
reaches the last stage of life: old age. Erickson saw different chronological periods of life presenting developmental challenges that led to either greater personality wholeness and a sense of well-being or poorer adaptation to the world and a contracted sense of self. He named each developmental stage with the words that defined the crisis at the center of its psychosocial challenge. He called the last stage of the lifespan “Ego Integrity vs. Despair.” At the heart of the conflict between ego integrity and despair are two questions: “Has my life had meaning?” and “Has my life been satisfying?” How a person answers these questions leads in the direction of either ego integrity or despair.
As a person faces a terminal diagnosis, I believe that they are automatically plunged into Erikson’s final developmental stage—no matter how old they happen to be at the time. I have seen dying people in their late twenties and earlier thirties wrestle with these questions as actively as people in their eighties and nineties.
If a dying person is able to attain ego integrity in the process of reflecting on their life, they come to feel proud of their accomplishments, understand the meaning contained in their life, and achieve a positive sense of completion. Further, they recognize the legacies they will leave behind. If a person fails at this developmental challenge, then they end up believing that their life was wasted; they settle into feelings of regret, bitterness, and despair.
The path to engaging the questions at the heart of this developmental stage involves introspection, journaling, reminiscence, life review, and, at times, deep exploration with other people. To do this work in a meaningful way, the person needs to approach it with a serious, structured examination. They have to look at both the accomplishments and things learned over the course of their life, as well as the failures, discarded beliefs, and unfinished business.
As the process unfolds, the dying person will naturally review the most important events in their life. They will examine how they felt about those events at the time, how they understand the impact of those events on their life, and what if anything they still may need to do in response to those events. Other areas of exploration involve themes that a person sees woven across the fabric of their experience, values that have become important to them, and things they learned—from either success or failure. All of this is fertile ground for understanding a person’s life.
The exploration into meaning can happen in dialog with a doula or family member; in moments of inner reflection, when the dying person is alone; in the effort to crystallize the meaning into a concrete legacy that can be passed on to others; and in discussion with family and friends, who can contribute a perspective the dying person may not fully recognize. Too often, this work of exploring meaning is left undone. If the dying person and the family are not openly discussing dying, or they are trying to maintain an air of normalcy, then reminiscence or life review tends to happen only in fleeting moments when the dying person is alone. Real examination of a person’s life needs structure to arrive at meaning. Without structure, despair is too often the outcome.
As a person explores the meaning of their life, it is natural to consider how that meaning might be expressed in a concrete way that the person finds satisfying; in a way that loved ones will find informative or inspiring. This expression of meaning is referred to as a legacy project. It can take the form of a memory book or an illustrated box that contains objects and/or cards with messages from family and friends. It can be an audio or video interview that focuses in a deep way on one or more aspects of a person’s life. It can be a life scroll that illustrates important moments or recurring themes. Or it might be a series of letters to current or future family members, expressing thoughts and wishes for them when they reach important milestones in their lives. The kinds of legacy projects people create are limited only by the imagination and creativity of those involved. Over time, these legacies become deeply valued family treasures, because they allow people to reconnect with the person after they have died and reengage with the meaning they identified.
A legacy project does more than express meaning. It preserves personal and, therefore, family history. It also gives a dying person the opportunity to exercise more control over how they spend their time in the last months or weeks of life. Loss of control over many aspects of life is a common complaint in severe illness and approaching death. Any way you can return some measure of control is therefore very helpful to the emotional state of the dying person and improves the quality of their life.
Too often, a dying person is treated as if they have already died. Their opinions, ideas, or advice about family events or issues is no longer solicited; they are left out of everyday decisions or ones that involve planning for the future. Creating a legacy project gives back to a dying person the power of who they are and returns their relevance to those around them. After they die, the legacy continues to speak for them, to tell their story, express their values, to convey their hopes for those who survive them or who may be born long afterward.
Complete Article HERE!