My great grandma, or Mia, as we knew her, was 100 when she decided she was ready to die. I found this out through a nonchalant conversation with my granny, her daughter, just after Christmas. She was eating a bowl of porridge at the breakfast bar, and said: “Mia wants to go, and that’s legal in Canada.”
Was I shocked? Not really. Although I didn’t actually know that Canada, where she had lived all her life, offered medically assisted dying (MAiD), my family are the type to take things into our own hands.
It’s a weird thing, euthanasia. It’s something you’re taught about in RE lessons at school, debating whether we have a right to ‘play God’. It’s something I agreed with as a faraway idea that I’d never have to consider. Something I thought was good in theory but hadn’t ever put any serious thought into the practice.
When I learned about Mia, I agreed with it still. Everyone I told did too, commenting on how brave her decision was and how amazing it was that she had this ‘opportunity’. They may have been thinking about the procedure itself rather than offering support but that was okay, because this was, overall, A Good Thing.
Meanwhile, with my family, talk swiftly turned to logistics. Timetables detailing who would be where and when were emailed around and the bank split Mia’s estate equally, with cheques ready to be collected by her children on the ride home from the facility. It helped the Canadian side of the family to deal with it Monica Geller-style, working pragmatically through the practical elements of her life.
“We’re more open to things that are predictable,” says Dr Anna Janssen, a psychologist specialising in palliative care. “There’s something safer about it, and that means we can be more flexible in our thinking and more open with ourselves and each other.”
But while they were handling the logistical side, it became very clear that we needed to introduce this flexibility into the emotional side of things, too.
The ‘five stages of grief’ ends with ‘acceptance’. The problem here was that for Mia to go with our blessing, we needed to accept her death before she actually died. That’s an unchartered process; grieving while someone is still alive and well(ish) feels weird. My auntie Penny summarised it perfectly, saying she felt she was going through grief sideways, like a breech birth.
Feeling emotion with a deadline meant we had to sprint through the confusion, the sadness, the relief of it all. If we had been Monica about the logistics, we Chandler-ed around the feelings part somewhat chaotically. But we still all felt weirdly…lucky? “With assisted dying, everyone involved has choice in the death,” explains Judy Tatelbaum, author of The Courage to Grieve. “That makes a great difference. Anticipatory grief is very healthy.”
But I was worried about what the minutes and days after she died would bring, seeing as we had already ‘grieved’. “Maybe the grief afterwards is easier, as some feelings have happened already,” said Dr Janssen. “But eventually there will be something new, because the context has changed, and you can’t feel it until the person has actually died.”
And so the 9th of January came. I asked not to know the exact time she was meeting her doctor, because what do you do in the minutes that someone you love is dying? In the most extreme version of the Schrödinger’s cat experiment, I went into a meeting, curious about whether she’d still be alive when I came out. She wasn’t. But there was an email telling the whole story, including how she had greeted the doctor by asking if he was the nice man who was going to help her.
Yes, my experience introduced a new closeness to my family. But it highlighted a flaw in the current MAiD plan. The message from the guidelines, the ethical debates and the psychologists I’ve spoken to is that assisted dying should be about having autonomy. It should make it easier, because you plan and prepare for the place, time, aftermath and even the feelings. But MAiD is such new territory that there are the same unknowns as with ‘regular’ dying.
Up until now, humans have only ever died after suffering through old age or illness or suddenly and shockingly in an accident. Those five stages of grief have been based on these same experiences over thousands of years. Now, suddenly, we’ve introduced a model where death can be scheduled into our diaries, and we can’t just apply the same rules. There are no history or self-help books to teach us how to navigate a brand-new type of grief that brings up a totally different, sporadic, rushed and uncertain feeling.
While there are articles and research papers discussing ethical, religious and legal boundaries, all the conversations have forgotten the people, families and feelings. And maybe that’s because, as Dr Janssen pointed out to me, it’s easier to discuss facts and figures than it is to discuss emotions.
For my family, MAiD was the first time we all properly discussed dying. Perhaps this is the taboo-breaking policy the world needs? You can’t send out a ‘save the date’ without telling people what for, after all. But to stop the turbulence, there’s still a grief taboo that needs to be broken. “We need to talk about the psychology of death and grief, but also the psychology of living. We talked about the death, but not about how we’re then meant to live well,” said Penny.
For families going through MAiD this year, in five years, or further in the future, when it could be a global policy, the system will benefit if we open up. “At the moment we don’t talk about it enough to know whether that [five stages] model requires more thought,” agrees Dr Janssen. “In my academic brain, I’m thinking we need to ask what MAiD means for people, but really, we’ll simply hear more if we take the time.”
My granny has since told me not to be shocked if she asks for MAiD. Is that a conversation she would have had with me if it wasn’t for Mia taking the plunge? Probably not. And while I haven’t yet applied my newfound skill for discussing death with anyone else, I’ll no longer hold back – especially when talking about my own.
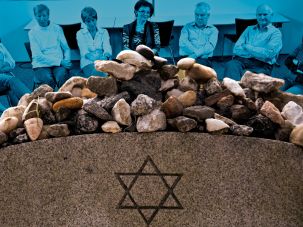
One sunny Thursday evening in June, eight people, ranging from thirty-somethings to senior citizens, sat around a table at the Manhattan Jewish Community Center nibbling on cookies.
In front of them stood Sally Kaplan, one of three facilitators present from the organization What Matters, a New York City-based not-for-profit that facilitates group and individual conversations about advanced care planning. Sally interrupted the snacking to provide the group with a directive: pair off with the person next to you and talk about when you first realized you were mortal.
The participants looked around at each other; a few nervously giggled. There was a moment of uncertain silence. And then, everyone turned to their partner, and a rush of words poured forth. Death, it seems, can be confronted.
The What Matters event is just one example of a surge in Jewish programming focused on end-of-life issues, from speeches to workshops to unstructured discussions reminiscent of Death Cafes, where strangers meet over coffee and cake to talk about any topic related to death they so choose. (I’ve attended and written about death cafes before, although at the earlier ones I attended, participants ate pancakes or Chinese food rather than desserts.) The first “café mortel” was held in Switzerland in 2004. Since then, the movement has spread globally: from living rooms in Cincinnati to (thwarted) plans for a permanent café in London to China, where sickness and mortality remain taboo.
And the death café now has Jewish equivalents: Over the past years, death café-esque events have been held at Jewish community centers, senior homes, synagogues, and even mortuaries. Most recently, a coalition of Westchester County, New York synagogues organized a series[ of “death cafes” (the events were more structured than the traditional café mortel) centered around subjects like Jewish funerals and the afterlife in traditional Jewish thought. In Israel, Rabbis Miriam Berkowitz and Valerie Stessin, who founded the pastoral care initiative Kashouvot, have also hosted death cafes in the past. The Dinner Party, a network of meal-based gatherings for young adults who have experienced loss, currently offers kosher dinners in New York City.
In 2016, Death Over Dinner, an American initiative similar to Death Cafe, partnered up with IKAR, a Los Angeles-based non-denominational Jewish community, and Reboot, a nonprofit Jewish think tank, to launch Death Over Dinner: Jewish Edition.
“We launched [the pilot] on Yom Kippur, because that is the quintessential Jewish moment of facing our mortality,” says Francine Hermelin, the creative director of Reboot. Though Reboot and Ikar have hosted dinners themselves, in addition to having partnered with organizations like Moishe House and the Contemporary Jewish Museum of San Francisco, they also offer an online questionnaire that helps guide a potential host to stage a dinner in his or her own home. They soon plan to add printable cards with verbal prompts, including quotes from psalms, Talmudic wisdom, and food for thought from contemporary rabbis, as an additional resource.
“[This initiative] is to make that personal shift, and ultimately a cultural shift, where talking about death is no longer a conversation we’re afraid of but a conversation that we are embracing,” Hermelin says.
The increased focus on mortality in recent years is likely the result of a combination of factors: an aging population living increasingly longer and facing unprecedented healthcare situations, a greater openness towards talking about historical taboos generally, and a growing consumer interest in wellness, including a concept of “the good death.” And Jewish initiatives focused on death and mourning want to take part in this larger dialogue, using spirituality and Jewish tradition as a foundation. Indeed, a 2017 Pew study found that “geographically and theologically diverse” faith communities were uniquely suited to address concerns around death and mourning, even for those with no prior religious affiliation.
“We [in the Jewish community] seized upon this wave,” says Kaplan, who points to books like Atal Gawande’s On Being Mortal and Paul Kalanithi’s When Breath Becomes Air as examples of the trend. Though What Matters is non-denominational––Kaplan describes it as “value neutral and person-centered”––Kaplan says she sees confronting mortality through discussion as a “very Jewish” enterprise, one she feels is reflected in Jewish texts. “People are surprised that there are so many Talmudic stories that deal with advanced care planning!” For further insight, Kaplan referred me to Rabbi Mychal Springer, Director of the Center for Pastoral Education at the Jewish Theological Seminary, who cites the story of Rabbi Yehudah Ha-Nassi, who was unable to die while his students were incessantly praying for him, until his handmaid dropped a jug from the roof and distracted them. In the moment of silence, Ha-Nassi was able to depart peacefully. ” This is a classic example of the way the rabbis were saying we shouldn’t prolong the dying process,” Rabbi Springer said.
Support doesn’t always come in the form of face-to-face groups: Lab/Shul, a creative Jewish community based in Lower Manhattan, operates an initiative called Kaddish Club, which includes a monthly potluck dinner in New York City, and a 15-minute weekly phone call they’ve dubbed Virtual Mourners’ Kaddish. During the calls, which began in 2014, the far-flung bereaved reflect on their departed loved ones, share some wisdom, and then recite Kaddish together.
“We’ve had folks call in from all over the country and all over the world,” says Sarah Strnad, Lab/Shul’s Director of Operations. “A lot of the traditional options [i.e. daily kaddish in a synagogue setting]… don’t always work in our modern lives.” Strnad says one of the most moving things about the calls is how they end up becoming micro-communities. “Even on the virtual calls, when people might never see each other in person, they remember each other’s stories and they can give each other support week after week.”
Of the current offerings, few are Orthodox in orientation. This might be because those who identify as Orthodox see processes around death as strictly prescribed ––decisions about life support deferred always to the ordained, mourning periods a certain length, prayers predetermined –– and therefore not necessary to hash out.
But Elad Nehorai, founder of Hevria and Forward contributor has imminent plans to hold a death café that will include a more observant audience (though he hopes to provide a space for the observant, he stresses that anyone is welcome). Nehorai, who has attended “secular” death cafes in the past, told me, “It was actually my fascination with death that caused me to choose to be Hasidic after growing up secular. Death has this fascinating power to force us to face what we really believe. Even as believers, we must face our beliefs in a brave way. Death forces us to do that.” (Full disclosure: Elad and I collaborated in organizing this event.)
During the course of my writing this piece, I attended my grandfather’s memorial service, tried to comfort a friend whose loved one was gravely ill, and heard a rabbi speak about ministering to a father grieving for his child as one of his first clerical duties.
Even though I had thought it slight hyperbole when she said it, I realized Francine Hermelin’s assertion that “we’re always experiencing death” was absolutely true. Though we may find it difficult to face our end with courage, as Nehorai hopes we can, we should do our utmost to be as prepared, emotionally, logistically, and spiritually, when the time inevitably comes, for as it says in Genesis, “For you are dust, and dust you shall return.”
Thankfully, there is increasingly more out there to help us do just that.
But we learn early on that despite the fact our lives are universally finite, most people don’t want to talk about it.
We’ll talk sex, we’ll talk drugs, we’ll even talk money—but not death.
That could be changing with the proliferation of so-called Death Cafes, informal get-togethers in cities across America, Europe and Asia, where people eat a little something, drink some coffee maybe and talk about, well, the inevitable.
The mission is to revamp typically depressing and urgent end-of-life discussions to more leisurely “Everything-I-Wanted-To-Know-About-Death-But-Was-Afraid-To-Ask.”
The conversation ranges, and depends on the group of people who’ve gathered: anything from how much a funeral costs to the details of a “green” funeral (think: corpse as compost) to tips on how to talk to your family members about your own funeral.
There’s a range of people who attend, too, from someone who had a death in the family and wants to be better prepared next time, to health care providers who want a different perspective on dealing with death. They range in age from 20-somethings to 90-somethings.
The object: to turn death from a feared end to something that is part of life.
“Death Cafés change the way you live in the most profound and wonderful way,” says Kim Mooney, 67, who runs monthly meetings in Longmont, Colorado.
Mooney even held a few events in a mortuary. “I like to say it’s the only time you will walk in and walk out of one, so you might as well take advantage of it.”
Death café hosts tend to have a sense of humor.
Death on twitter
If you want to confirm the popularity of the death positive movement, just go on social media. There’s The Death Café Facebook group, which lists times and dates of meeting and has more than 50,000 likes and followers.
Advocates say the meetings allow people a low-pressure way to express fears about the Great Unknown; to chat about the way other cultures handle death; and to share practical information, such as learning the nuts and bolts of filling out end-of-life forms.
Talking with strangers, hosts say, is often an easier way to broach the topic before launching a conversation about death with loved ones.
Lizzy Miles is a hospice social worker who hosted America’s first café in 2012 in Westerville, Ohio. She baked cookies in the shape of tombstones with grey icing and “Death Café” where the epitaph normally goes.
She is one of more than a 100 Death Café hosts in this country. She’s still hosting—and still making treats—for nearly a dozen people who show up each month.
Yes, these are the cookies Lizzy makes for her Death Café guests in Ohio.
“No one ever comes to a Death Café already uncomfortable talking about death,” she says. “If you are, you’re not going to come. We have a lot of sandwich generation people, who are taking care of their parents.”
Miles is so committed she even traveled to a Death Café in Hong Kong—“on my own dime!”—to see what it was like.
“It was amazing, people were speaking English and Mandarin and Cantonese,” she says. “And I thought ‘Oh my gosh, all these different languages. This is pretty cool but almost exactly the same.’”
Dos and don’ts
Anyone can be a host, but there are guidelines. The Death Café website has a set of guidelines and Miles herself was a co-author on an article that included a list of dos and don’ts in the Omega Journal of Death and Dying:
Do: Allow a space for folks to share their ideas respectfully and openly.
Do: Offer the opportunity for everyone to speak but allow those who want to remain silent to do so.
Don’t: Charge an admission fee.
Don’t: Sell death-related products.
Don’t: Turn the group into grief support.
Miles and others believe that confronting our mortality will prompt us to the make the sorts of life changes that some folks do only when confronted with a fatal disease. Why wait?
Shellie Balogh, a 61-year-old hospice nurse attended one of Miles’ cafés in Ohio.
“It wasn’t what I expected; it was more upbeat,” she says. “It’s a fun thing to do if I have a free Saturday. You go and meet people you may never see again and just have this conversation, opening up this forbidden area of discussion.”
A midwife for dying
Suzanne O’Brien hosts a New York City group that meets at a public library on the Upper West side. She’s a nurse turned death doula.
Death doulas—part of this burgeoning “death-positive” movement—provide the same sort of bedside care, comfort and companionship that birth doulas offer to pregnant women but at the other end of the life cycle.
O’Brien said monthly conversations tend to fit into five buckets, sometimes all five covered in one 90-minute session:
The physical: How do I make sure I’m comfortable during my dying hours. What do I want to happen to my body?
The financial: What forms do I need to fill out? Or how much money do I want to spend on a funeral versus, say, end-of-life care?
The emotional: How do we deal with potential regrets or forgiveness?
The mental: Reasoning and acceptance
The spiritual: How do beliefs about death inform the way we live.
One woman wanted to know how to donate her body to a medical school anatomy class. She also wanted to make sure her family would not be given the leftovers when the students are done picking her apart, something she had heard can happen.
She told the group: “I’d rather just be flushed.”
Banishing the secrecy
The idea of a group of a random community members chatting about death over refreshments was the brainchild of Swiss sociologist Bernard Crettaz. He launched a “Café Mortel” in 2004 in the lakeside town of Neuchâtel, Switzerland. A dozen mortal members attended.
The point, as he once told a reporter for the Independent, a British newspaper, was to remove death talk from its “tyrannical secrecy.”
The first cafe outside of Switzerland was held by John Underwood, who hosted in his London basement in 2011. He’s given credit for helping the movement go global; he died last year, at the age of 44, from undiagnosed leukemia.
Today, there are death-with-food meetings in about 55 countries—including the U.K., Italy, Hong Kong, Finland, the Netherlands and New Zealand.
Becoming a regular
Those who are regulars say that while the subject matter is death, the meetings are not sad. Hosts emphasize that they are not grief support groups, more death-curious groups.
Jane Geller, a retired schoolteacher in New York City attends the Upper West Side meeting nearly every month.
“It’s a misnomer to think it’s depressing,” she said. “Death Cafés are really about life.”
Shatzi Weisberger, an 88-year-old retired nurse from New York City is a regular, too.
“I was always especially interested in how we come into this world and how we leave it. When I got into my eighties, I got personally interested for my own edification.”
Last fall, she hosted her own “FUN-eral” (pronounced Funn-eral) in the common room of her apartment building. More than 100 attendees came to the event. It sounded like a macrabe-themed birthday but she said it was a death, not a birth, party. And a way to attend her own funeral.
She said she has planned her own green burial. “I’m going to be wrapped in a shroud and buried in the woods upstate and my body will deteriorate and something will grow. I don’t know if it will be grass or flowers or a tree so I feel my dying is bringing life into the world. That’s not depressing at all.”
The answer might seem simple, but in the hands of Lesley Hazleton, the question takes us on a surprisingly humorous and thought-provoking journey into what it would actually mean to live forever. And whether we’d truly want to. A frequent TED.com speaker and ‘Accidental Theologist,’ Hazleton uses wit and wisdom to challenge our ideas not only about death, but about what it is to live well.
Lesley Hazleton has traced the roots of conflict in several books, including compelling ‘flesh-and-blood’ biographies of Muhammad and Mary, and casts “an agnostic eye on politics, religion, and existence” on her blog, AccidentalTheologist.com. Her newest book, Agnostic: A Spirited Manifesto, celebrates the agnostic stance as “rising above the flat two-dimensional line of belief/unbelief, creating new possibilities for how we think about being in the world.” In it, she explores what we mean by the search for meaning, invokes the humbling perspective of infinity and reconsiders what we talk about when we talk about soul.
A UBC professor has determined that people diagnosed with terminal cancer—who have hope, positivity and family support—are able to live well during the advanced stage of the disease.
Carole Robinson, professor emeritus with UBC Okanagan School of Nursing, recently published a paper explaining the process of living well with an awareness of dying.
“While there is a growing body of research focused on select aspects of people’s experiences with advanced cancer, there is little research examining the process of living with advanced cancer across the trajectory towards death,” says Robinson. “Even patients whose prognosis is limited are living longer and want to live well, making this issue a global concern.”
Robinson notes that globally there are 14.1 million new cancer cases diagnosed each year, 8.2 million cancer deaths, and 32.6 million people living with cancer. Historically, researchers have studied the concept of living well with a chronic illness, but not specifically cancer. Robinson says those studies convey the idea it may be possible to live well with advanced cancer, but little is known about how it is done or how to support it.
The study analyzed 22 interviews with Spanish residents involved in previous research that explored their experience of living with advanced cancer. The researchers found the participants engaged in a five-phase iterative process: struggling, accepting, living with advanced cancer, sharing the illness experience and reconstructing life. This process revolved around participants’ awareness of dying, which differed from people living with chronic illness and was a unique aspect of this newresearch.
Each phase was revisited, and as the disease advanced living well got more challenging. Participants talked about strategies for living with advanced cancer, including making life adjustments, maintaining a positive attitude, normalizing and hoping.
Over time, participants realized struggling against the disease created additional difficulties. In fact, they understood it was counterproductive so they made a conscious choice to let go of struggling. Some referred to it as being the only choice they could make while living with the uncertainty of advanced cancer. This enabled accepting their life circumstances at some level and learning to live alongside their illness.
Robinson says that the importance of family love and support cannot be underestimated. For all the participants, she adds, awareness of dying led them to focus on living well. Sharing the experience with loved ones softened suffering remarkably. They were aware they did not have time to lose.
“Although it might happen in moments, participants were able to put advanced cancer behind them and live life rather than living their illness,” she notes. “Living in the moment enabled deep appreciation of everyday things such as the beauty of a flower garden.”
Robinson says the key takeaways to living well encompass a balance between dependence and independence, being able to see the positive and maintaining hope even in the end stages of the disease.
“The participants in this study worked hard to live a life rather than live an illness,” says Robinson. “The implication here is to support the positive. It has been found in previous research that hoping for a cure when cancer is advanced is not lack of awareness—it can be a choice in focusing simply on positive possibilities.”
THE UNWINDING OF THE MIRACLE
A Memoir of Life, Death, and Everything That Comes After
By Julie Yip-Williams
Julie Yip-Williams
By Lori Gottlieb
When we meet Julie Yip-Williams at the beginning of “The Unwinding of the Miracle,” her eloquent, gutting and at times disarmingly funny memoir, she has already died, having succumbed to colon cancer in March 2018 at the age of 42, leaving behind her husband and two young daughters. And so she joins the recent spate of debuts from dead authors, including Paul Kalanithi and Nina Riggs, who also documented their early demises. We might be tempted to assume that these books were written mostly for the writers themselves, as a way to make sense of a frightening diagnosis and uncertain future; or for their families, as a legacy of sorts, in order to be known more fully while alive and kept in mind once they were gone.
By dint of being published, though, they were also written for us — strangers looking in from the outside. From our seemingly safe vantage point, we’re granted the privilege of witnessing a life-altering experience while knowing that we have the luxury of time. We can set the book down and mindlessly scroll through Twitter, defer our dreams for another year or worry about repairing a rift later, because our paths are different.
Except that’s not entirely true. Life has a 100 percent mortality rate; each of us will die, and most of us have no idea when. Therefore, Yip-Williams tells us, she has set out to write an “exhortation” to us in our complacency: “Live while you’re living, friends.”
Before her diagnosis in 2013, Yip-Williams had done more than her share of living. It was, indeed, something of a miracle that she was alive at age 37 when she traveled to a family wedding and ended up in the hospital where she received her cancer diagnosis. Born poor and blind to Chinese parents in postwar Vietnam, she was sentenced to death by her paternal grandmother, who believed that her disability would bring shame to the family and render her an unmarriageable burden. But when her parents brought her to an herbalist and asked him to euthanize her, he refused.
The family would eventually survive a dangerous escape on a sinking boat to Hong Kong, and less than a year later make their way to the United States, where at 4 years old, Yip-Williams had a surgery that granted her some vision, if not enough to drive or read a menu without a magnifying glass.
She would go on to defy her family’s expectations, eventually graduating from Harvard Law School, traveling the world solo and working at a prestigious law firm where she meets Josh, the love of her life. She becomes a mother and, soon after, a cancer patient, and soon after that, because of this unfortunate circumstance, a magnificent writer.
During the five years from her diagnosis to her death, we enter her world in the most intimate way as she cycles through Elisabeth Kübler-Ross’s famous stages of grieving: denial, anger, bargaining, depression and acceptance. Describing the ways in which terminally ill patients cope with their own deaths, these stages weren’t meant to delineate a neat sequential progression but rather the various emotional states a dying person might visit, leave and visit again.
Yip-Williams toggles between optimism and despair, between believing she’ll defy the statistics as she had so many times in her life — “odds are not prophecy” — and trying to persuade her husband to confront their harrowing reality. She makes bargains with God, just as she did as a young girl when, in exchange for her poor vision, she asked for a soul mate one day. (“God accepted my deal!”) She posts pictures of contented normalcy on Facebook — of meals cooked, a car purchased — but rages at her husband, healthy people, the universe and, silently, at the moms at a birthday party who ask how she’s doing. “Oh, fine. Just hanging in there,” she replies, while wanting to scream: “I didn’t deserve this! My children didn’t deserve this!” She frets about the “Slutty Second Wife” her husband will one day marry and the pain her daughters will experience in her absence. And, near the end, she oscillates between being game to try every possible treatment and accepting that nothing will keep her alive.
“Paradoxes abound in life,” Yip-Williams writes in a heart-rending letter to her daughters; she asks us to confront these paradoxes with her head-on. One of the paradoxes of this book is that Yip-Williams writes with such vibrancy and electricity even as she is dying. She moves seamlessly from an incisive description of her mother as “the type of woman who sucks blame and guilt into herself through a giant straw,” to the gallows humor of “Nothing says ‘commitment to living’ quite like taking out a mortgage,” to the keen observation “Health is wasted on the healthy, and life is wasted on the living.” Unlike the woman in her support group who, after being given a terminal prognosis, defiantly declares, “Dying is not an option,” Yip-Williams prepares meticulously for her death while paying close attention to the life she will one day miss: “the simple ritual of loading and unloading the dishwasher. … making Costco runs. … watching TV with Josh. … taking my kids to school.”
This memoir is so many things — a triumphant tale of a blind immigrant, a remarkable philosophical treatise and a call to arms to pay attention to the limited time we have on this earth. But at its core, it’s an exquisitely moving portrait of the daily stuff of life: family secrets and family ties, marriage and its limitlessness and limitations, wild and unbounded parental love and, ultimately, the graceful recognition of what we can’t — and can — control.
“We control the effort we have put into living,” Yip-Williams writes, and the effort she has put into it is palpable. Of all the reasons we’re drawn to these memoirs, perhaps we read them most for this: They remind us to put in our own effort. It would be nearly impossible to read this book and not take her exhortation seriously.
If someone you love has died in a hospital, you may have seen modern death at its worst: overly medicalized, impersonal, and filled with unnecessary suffering. The experience can be a bitter lesson in Buddha’s most basic teaching: the more we try to avoid suffering (including death), the worse we often make it.
Even though roughly half of Americans die in hospitals and other institutions, most of us yearn to die at home, and perhaps to experience our leavetaking as a sacred rite of passage rather than a technological flail. You don’t have to be a saint, or be wealthy, or have a Rolodex of influential names to die well. But you do need to prepare. It helps to be a member of at least one “tribe,” to have someone who cares deeply about you, and to have doctors who tell you necessary truths so that you can decide when to stop aggressive treatment and opt for hospice care. Then those who care for you can arrange the basics: privacy, cleanliness, and quiet, the removal of beeping technologies, and adequate pain control. They can listen and express their love, and provide the hands-on bedside care hospice doesn’t cover.
From then on, a more realistic hope for our caregivers, and for ourselves when we are dying, may not be an idealized “good death” by a well-behaved patient, but a “good enough death,” where we keep the dying as comfortable and pain-free as possible, and leave room for the beautiful and the transcendent—which may or may not occur.
Hospice professionals often warn against high expectations. Things will probably not go as planned, and there comes a point when radical acceptance is far more important than goal-oriented activity. They don’t like the idea, inherent in some notions of the “good death,” of expecting the dying to put on a final ritual performance for the living, one marked by beautiful last words, final reconciliations, philosophical acceptance of the coming of death, lack of fear, and a peaceful letting go.
“In It Together” by Nancy Borowick. Nancy Borowick’s photo series (January 2013 through December 2014) depicts the experiences of Howie and Laurel Borowick, partners for over 30 years, who found their lives consumed by doctor appointments and the shared challenges of chemotherapy.“The Calm before the Storm”“His and Hers”
“I don’t tell families at the outset that their experience can be life-affirming, and leave them with positive feelings and memories,” said hospice nurse Jerry Soucy. “I say instead that we’re going to do all we can to make the best of a difficult situation, because that’s what we confront. The positive feelings sometimes happen in the moment, but are more likely to be of comfort in the days and months after a death.” This is what it took, and how it looked, for the family of John Masterson.
John was an artist and sign painter, the ninth of ten children born to a devout Catholic couple in Davenport, Iowa. His mother died when he was 8, and he and two of his sisters spent nearly a year in an orphanage. He moved to Seattle in his twenties, earned a black belt in karate, started a sign-painting business, and converted to Nichiren Shoshu, the branch of Buddhism whose primary practice is chanting. He never left his house without intoning three times in Japanese Nam Myoho Renge Kyo (“I Honor the Impeccable Teachings of the Lotus Sutra”).
He was 57 and living alone, without health insurance, when he developed multiple myeloma, an incurable blood cancer. He didn’t have much money: he was the kind of person who would spend hours teaching a fellow artist how to apply gold leaf, while falling behind on his paid work. But thanks to his large extended family, his karate practice, and his fierce dedication to his religion, he was part of several tribes. He was devoted to his three children—each the result of a serious relationship with a different woman—and they loved him equally fiercely. His youngest sister, Anne, a nurse who had followed him to Seattle, said he had “an uncanny ability to piss people off but make them love him loyally forever.”
When he first started feeling exhausted and looking gaunt, John tried to cure himself with herbs and chanting. By the time Anne got him to a doctor, he had a tumor the size of a half grapefruit protruding from his breastbone. Myeloma is sometimes called a “smoldering” cancer, because it can lie dormant for years. By the time John’s was diagnosed, his was in flames.
Huge plasma cells were piling up in his bone marrow, while other rogue blood cells dissolved bone and dumped calcium into his bloodstream, damaging his kidneys and brain function. He grew too weak and confused to work or drive. Bills piled up and his house fell into foreclosure. Anne, who worked the evening shift at a local hospital, moved him into her house and drove him to various government offices to apply for food stamps, Social Security Disability, and Medicaid. She would frequently get up early to stand in line outside social services offices with his paperwork in a portable plastic file box.
Medicaid paid for the drug thalidomide, which cleared the calcium from John’s bloodstream and helped his brain and kidneys recover. A blood cancer specialist at the University of Washington Medical Center told him that a bone marrow transplant might buy him time, perhaps even years. But myeloma eventually returns; the transplant doesn’t cure it. The treatment would temporarily destroy his immune system, could kill him, and would require weeks of recovery in sterile isolation. John decided against it, and was equally adamant that he’d never go on dialysis.
After six months on thalidomide, John recovered enough to move into a government-subsidized studio apartment near Pike Place Market. He loved being on his own again and wandered the market making videos of street musicians, which he’d post on Facebook. But Anne now had to drive across town to shop, cook, and clean for him.
The health plateau lasted more than a year. But by the fall of 2010, John could no longer bear one of thalidomide’s most difficult side effects, agonizing neuropathic foot pain. When he stopped taking the drug, he knew that calcium would once again build up in his bloodstream, and that he was turning toward his death.
An older sister and brother flew out from Iowa to help Anne care for him. One sibling would spend the night, and another, or John’s oldest daughter, Keely, a law student, would spend the day.
Christmas came and went. His sister Irene returned to Iowa and was replaced by another Iowa sister, Dottie, a devout Catholic. In early January, John developed a urinary tract infection and became severely constipated and unable to pee. Anne took him to the University of Washington Medical Center for what turned out to be the last time. His kidneys were failing and his bones so eaten away by disease that when he sneezed, he broke several ribs. Before he left the hospital, John met with a hematologist, a blood specialist, who asked Anne to step briefly out of the room.
Anne does not know exactly what was said. But most UW doctors are well trained in difficult conversations, thanks to a morally responsible institutional culture on end-of-life issues. Doctors at UW do not simply present patients with retail options, like items on a menu, and expect them to blindly pick. Its doctors believe they have an obligation to use their clinical experience to act in their patients’ best interests, and they are not afraid of making frank recommendations against futile and painful end-of-life treatments. When the meeting was over, the doctor told Anne that her brother “wanted to let nature take its course.” He would enroll in hospice. Anne drove him home.
John knew he was dying. He told Anne that he wanted to “feel everything” about the process, even the pain. He took what she called “this Buddhist perspective that if he suffered he would wipe out his bad karma. I said, ‘Nah, that’s just bullshit. You’ve done nothing wrong. The idea that we’re sinners or have to suffer is ludicrous.’” She looked her brother in the eye. She knew she was going to be dispensing his medications when he no longer could, and she wasn’t going to let him suffer. She told him, ‘You’re not going to have a choice.’”
The drive to treatment takes half an hour, and Howie and Laurel Borowick take turns, resting and driving, depending on who’s getting treatment that day. “The Drive to Chemo”In Laurel’s final moments, her family assured her that all would be OK. “Last Touch”
Anne said she “set an intention”: not to resist her brother’s dying, but to give him the most gentle death possible and to just let things unfold. On January 15, her birthday, she and John and a gaggle of other family members walked down to Pike Place Market to get a coffee and celebrate. John was barely able to walk: Anne kept close to him so that she could grab him if he fell. It was the last time he left the house.
The next morning, a Sunday, while Anne was sitting with John at his worktable, he looked out the window and asked her, “Do you think I’ll die today?” Anne said, “Well, Sundays are good days to die, but no, I don’t think it’s today.” It was the last fully coherent conversation she had with him.
He spent most of his last nine days in bed, as his kidneys failed and he grew increasingly confused. He didn’t seem afraid, but he was sometimes grumpy. He had increasing difficulty finding words and craved celery, which he called “the green thing.” He would ask Anne to take him to the bathroom, and then forget what he was supposed to do there. His daughter Keely took a leave of absence from law school, and Anne did the same from her job at the hospital. Fellow artists, fellow chanters, former students to whom he’d taught karate, nephews, nieces, and sign-painting clients visited, and Anne would prop him up on pillows to greet them.
Anne managed things, but with a light hand. She didn’t vet visitors, and they came at all hours. If she needed to change his sheets or turn him, she would ask whoever was there to help her, and show them how. That way, she knew that other people were capable of caring for him when she wasn’t there. “The ones that have the hardest time [with death] wring their hands and think they don’t know what to do,” she said. “But we do know what to do. Just think: If it were my body, what would I want? One of the worst things, when we’re grieving, is the sense that I didn’t do enough,” she said. “But if you get in and help, you won’t have that sense of helplessness.”
Each day John ate and spoke less and slept more, until he lost consciousness and stopped speaking entirely. To keep him from developing bedsores, Anne would turn him from one side to the other every two hours, change his diaper if necessary, and clean him, with the help of whoever was in the room. He’d groan when she moved him, so about a half an hour beforehand, she’d crush morphine and Ativan pills, mix them with water as the hospice nurse had showed her, and drip them into John’s mouth.
One morning her distraught brother Steve accused her of “killing” John by giving him too much morphine—a common fear among relatives, who sometimes can’t bear to up the dose as pain gets worse. At that moment, the hospice nurse arrived by chance, and calmly and gently explained to Steve, “Your brother is dying, and this is what dying looks like.”
The death was communal. People flowed in and out, night and day, talking of what they loved about John and things that annoyed them, bringing food, flowers, candles, and photographs until John’s worktable looked like a crowded altar. Buddhists lit incense and chanted. Someone set up a phone tree, someone else made arrangements with a funeral home, and one of the Buddhists planned the memorial service.
Most of the organizing, however, fell to Anne. It may take a village to die well, but it also takes one strong person willing to take ownership—the human equivalent of the central pole holding up a circus tent. In the final two weeks, she was in almost superhuman motion. She leaned in, she said, “into an element of the universe that knows more than I know. I was making it up as I went along. People contributed and it became very rich.
“That’s not to say there weren’t times when it was phenomenally stressful. I was dealing with all the logistics, and with my own mixed emotions about my brother. I was flooded with memories of our very complicated relationship, and at the same time I knew my intention was that he be laid to rest in the most gentle way possible.”
Hospice was a quiet support in the background. Over the two years of his illness, John’s care had perfectly integrated the medical and the practical, shifting seamlessly from prolonging his life and improving his functioning— as thalidomide and the doctors at UW had done—to relieving his suffering and attending his dying, as the hospice nurses and those who loved him had done.
There were no demons under the bed or angels above the headboard. Nor were there beeping monitors and high-tech machines. His dying was labor-intensive, as are most home deaths, and it was not without conflict.
A few days before he died, two siblings beseeched Anne to call a priest to give John last rites in the Catholic church. “It was a point of love for my siblings. They were concerned that John was going to burn in hell,” Anne said. “But John hated priests.” In tears, Anne called the Seattle church that handled such requests, and the priest, after a brief conversation, asked her to put her sister Dottie on the phone. Yes, Dottie acknowledged, John was a Buddhist. No, he hadn’t requested the sacraments. Yes, his children were adamantly opposed. No, the priest told her, under the circumstances he couldn’t come. It wasn’t John’s wish.
Ten days after the family’s last walk through Pike Place Market, the hospice nurse examined John early one morning and said, “He won’t be here tomorrow.” She was seeing incontrovertible physical signs: John’s lips and fingertips were blue and mottled. He hadn’t opened his eyes in days. His breathing was labored and irregular, but still oddly rhythmic, and he looked peaceful. The hospice nurse left. Anne, helped by John’s daughter Keely and his sister Dottie, washed and turned John and gave him his meds. Then they sat by his side. Anne had her hand on his lap.
“It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.
“He just had this one-room apartment with a little half-wall before the kitchen. I walked over to put water on to make coffee, and Keely said, ‘His breathing’s changed.’”Anne stopped, ran over, sat on the bed, and lifted her brother to a sitting position. He was light. She held him close, and during his last three breaths she chanted Nam Myoho Renge Kyo, as her brother had always done, three times, whenever he left his house. “I was really almost mouth-to-mouth chanting, and he died in my arms,” she said. “We just held him, and then my sister Dottie said her prayers over him.”
Anne sat next to her brother and said, “John, I did well.”
“I know he would not have been able to orchestrate it any better than how it unfolded,” she said.
“It was a profound experience for me. I realized what a good death could be.”


 In front of them stood Sally Kaplan, one of three facilitators present from the organization
In front of them stood Sally Kaplan, one of three facilitators present from the organization 
 The object: to turn death from a feared end to something that is part of life.
The object: to turn death from a feared end to something that is part of life.
 Do: Offer the opportunity for everyone to speak but allow those who want to remain silent to do so.
Do: Offer the opportunity for everyone to speak but allow those who want to remain silent to do so.  Death doulas
Death doulas Shatzi Weisberger, an 88-year-old retired nurse from New York City is a regular, too.
Shatzi Weisberger, an 88-year-old retired nurse from New York City is a regular, too. 


 The family would eventually survive a dangerous escape on a sinking boat to Hong Kong, and less than a year later make their way to the United States, where at 4 years old, Yip-Williams had a surgery that granted her some vision, if not enough to drive or read a menu without a magnifying glass.
The family would eventually survive a dangerous escape on a sinking boat to Hong Kong, and less than a year later make their way to the United States, where at 4 years old, Yip-Williams had a surgery that granted her some vision, if not enough to drive or read a menu without a magnifying glass.





 “It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.
“It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.