Policies designed to prevent the misuse of opioids may have the unintended side effect of limiting access to the pain-relieving drugs by terminally ill patients nearing the end of their life, new research led by the Oregon State University College of Pharmacy suggests.
A study of more than 2,500 hospital patients discharged to hospice care over a nine-year period showed a decreasing trend of opioid prescriptions as well as an increase in the prescribing of less powerful, non-opioid analgesics, meaning some of those patients might have been undertreated for their pain compared to similar patients in prior years.
The findings, published in the Journal of Pain and Symptom Management, are an important step toward optimizing pain management and minimizing the suffering of dying patients. Hospice care refers to treatments whose goal is to maximize comfort and quality of life as opposed to prolonging life.
Researchers at OSU, Oregon Health & Science University, the Dana Farber Cancer Institute and Ariadne Labs in Boston, the University of Massachusetts Medical School and the University of Maryland School of Pharmacy used electronic health record data to examine 2,648 discharges of adult patients to hospice care.
The discharges were from an acute care, academic hospital between Jan. 1, 2010, and Dec. 31, 2018. The average patient age was 65, more than half had cancer, and the study sought to determine the year by year frequency of patients receiving opioid prescriptions.
After adjusting for factors that could affect prescription frequency, including age, specific diagnosis and where the patient was to receive hospice care, the results showed a nearly 12% downward trend from the first year (91.2%) to the last (79.3%).
“Pain is a common end-of-life symptom and it’s often debilitating,” said the study’s lead author, Jon Furuno, an associate professor and the interim chair of the Oregon State Department of Pharmacy Practice, who notes that more than 60% of terminal cancer patients report “very distressing pain.”
Opioids, a class of drugs that block pain signals between the body and brain, are an effective pain management tool. But there are barriers, Furuno said, to the optimal prescribing of opioids.
Among the hurdles are timely and accurate pain assessments, patient and caregiver concerns regarding addiction, and caregiver concerns about making mistakes in administering the meds. Additional obstacles are policies and practices aimed at limiting opioid use in response to the opioid epidemic.
Traced to over-prescribing that began in the 1990s, the epidemic claims more than 40,000 American lives annually, according to the U.S. Department of Health and Human Services. Ten million people a year misuse prescription opioids and 2 million suffer from an opioid use disorder. Opioids can be highly addictive and they exist both as prescription painkillers like morphine, hydrocodone, fentanyl and oxycodone and street drugs such as heroin.
Five years ago, the Centers for Disease Control and Prevention produced a guideline for prescribing opioids for chronic pain, and there have been several other federal, state and local efforts over the last 10 years to curb opioid prescribing, Furuno said.
“There are some concerns, however, that indiscriminate adoption or misapplication of these initiatives may be having unintended consequences,” he said. “The CDC Prescribing Guideline and the other initiatives weren’t meant to negatively affect patients at the end of their lives, but few studies have really looked at whether that’s happening. Our results quantify a decrease in opioids among patients who are often in pain and for whom the main goal is comfort and quality of life.”
Furuno adds that the concurrent increase in non-opioid analgesic prescriptions suggests health care providers remained concerned about pain management even as they wrote fewer opioid prescriptions.
“Sometimes non-opioids alone are the best choice, or non-opioids in combination with opioids,” he said. “But it’s important to remember that non-opioids alone are also not without risk and that delaying the start of opioid therapy may be delaying relief from pain.
“Even among patients prescribed opioids during the last 24 hours of their inpatient hospital stay, opioid prescribing upon discharge decreased,” Furuno added. “It seems unlikely that patients would merit an opioid prescription on their last day in the hospital but not on their first day in hospice care, and it’s well documented that interruptions in the continuity of pain treatment on transition to hospice are associated with poor patient outcomes.”
About a month before the coronavirus pandemic engulfed us, my mother understood that she was dying. She had cancer. She had struggled to swallow food and maintain her weight. She was so light that I could lift her like a 12-year-old. On her firm instructions, the ambulance we children had arranged to take her to the oncologist was rerouted to a hospice. There, she received tender and expert end-of-life care. After four days, she died: peacefully, without pain, and with her family around her.
Today, this memory feels weirdly distant. In Italy and Spain — and soon in other countries — patients are dying in opposite conditions to the ones my mother experienced. They go to hospitals hoping for treatment. But, for lack of ventilators, some of them die gradually, alone. Visits from loved ones are often prohibited.
The flood of commentary on the pandemic focuses, correctly, on how to reduce fatalities. But we should also consider how to ease the loneliness and pain of those deaths that are inevitable. No one wants to die slowly in a medical hangar, cut off from family and friends. Rather, most want something as close as possible to what my mother had. They want to choose their own balance between prolonged life and prolonged pain. They hope to have the right to reconsider their choices.
Of course, in the current crisis, the hospices cannot serve everybody, and infectious disease presents risks to caregivers that cancer does not. The imperative is, therefore, to give people the tools to manage death at home, as humanely and safely as possible. Yet this component of our response to the pandemic is missing. We have not grappled with the need to distribute morphine to those who are suffering, even if this is a risky course, as the opioid crisis makes obvious; once we have finally supplied our medical professionals with the masks and other protective gear they need, we need to do the same for family caregivers. But we do not discuss these things, because we are determined to resist death, not dwell on the question of how we might go about dying.
My mother’s last lesson to her children was that this obstinacy is mistaken. While I was vainly learning all I could about her treatment options, she was coming to terms with the reality she could feel around her liver. “No more abracadabra,” she told me fiercely, when I protested that it was too early to give up. She knew she would soon die, and she wanted a good death.
A good death requires lucidity, not magical thinking. Today, this means confronting the reality of overloaded hospitals, and being honest about their inability to help all those who are stricken. In Italy, doctors have had to perform a kind of triage normally seen in wartime: They allocate life-saving ventilators based on age and health status. The same has happened in Madrid, where hundreds queue to be admitted to emergency rooms. Countries such as the United States and Britain will be lucky to escape this fate. New York’s governor, Andrew M. Cuomo, has repeatedly sounded the alarm about the shortage of ventilators. “You’re going to be thousands short. Thousands,” he said on March 15.
Hospitals don’t like to talk about the terms of the triage. Like the rest of us, they prefer to focus on preventing death; they recoil from being explicit about when death might have to be accepted. As a recent article in the New England Journal of Medicine noted, the absence of clear guidelines burdens front-line clinicians, who are forced to make heart-rending choices — doctors in Italy have wept under the pressure. But the absence of clear guidelines also leaves citizens adrift. If you or I fall seriously ill, will we have access to a ventilator?
Last week, two medically connected relatives called me. Being well informed and 70, they both know they fall on the wrong side of any triage. They have therefore resolved that, if their lungs begin to fail, they will avoid going to the hospital. At 70 — even in their 80s — patients still have a good chance of surviving covid-19 at home. But if they do not, my relatives’ definition of a good death is to be together at the end, even at the risk that one will infect the other. All that they ask is access to the palliative drugs that will control the suffering.
Society should think about the millions of people who are not medical insiders, and who should be helped to understand the choices that may potentially confront them. No doubt if governments and hospitals made public their criteria for triage, people would be horrified. But at least they could decide whether to seek help at a hospital or remain in their own beds. And the medical authorities, having leveled with the citizens, could be more forthcoming about the help available at home. To anyone who has witnessed death, it would be a huge relief to know that at least the pain can be managed. Death will be inevitable for each of us, one day. Terrible suffering should not be.
Dr Geoffrey Mitchell, Professor of General Practice and Palliative Care at the University of Queensland, recently wrote an article on the ‘very public’ debate relating to opioid use, and tension between standard end‐of‐life care and voluntary assisted dying, as a ‘perfect storm’ that is impacting GPs and other health professionals.
‘Some are choosing to abandon end-of-life care altogether rather than risk professional ruin should they persist in the use of any opioid therapy,’ Professor Mitchell said.
Professor Mitchell cited previous newsGP articles as evidence doctors are worried. He said he was motivated to write his article in order to help alleviate concerns and prevent a wave of GPs from leaving palliative care.
‘[GPs responding like this was] no surprise to me. I’m aware of the risk-averse nature of a lot of GPs and the fear of litigation is quite high with some of my colleagues,’ he told newsGP.
‘The fear is that the use of medicines to minimise suffering and distress at the very end of life may hasten death and be construed by critics as euthanasia by stealth.
‘The reality is that the person is dying. While treatments such as opioids may theoretically shorten life marginally, it is the disease that causes death, not the treatment.’
In a recent ABC interview, RACGP President Dr Harry Nespolon agreed with this position and reiterated that the college is alarmed about the impact increased scrutiny on opioid prescription is having on doctors providing palliative care.
‘Good palliative care does require the use of high-dose opioids, and that’s what patients deserve,’ he said.
‘They deserve a good death and a painless death. All this is doing is asking doctors to prescribe fewer opioids for patients who really should be getting them.’
According to Professor Mitchell, the increased emphasis on opioid diagnosis, combined with incomingvoluntary assisted dying laws, has emboldened critics of palliative care and led to misinformation that can actually harm patients.
‘If [terminally ill patients] need strong opioid medication and can’t get it because their doctor won’t prescribe it, well then that’s the other side of the coin – the person is going to be suffering unnecessarily in their final days and hours, and that is unacceptable,’ he said.
‘Critics of palliative care think it’s quite often assisted dying under a legal guise, which is not true.
‘It’s just wrong, but it’s out there and so people who might not be feeling particularly confident about what they’re doing will say, “Well, I don’t want a bar of it”.’
However, despite the current climate of fear, Professor Mitchell believes a study he co-authored last year should go some way towards alleviating litigation concerns and help ensure patients receive proper medical care.
‘Of all case law online and all tribunals, all settings, we found 12 cases. Of those, only two had adverse findings recorded, and neither led to criminal proceedings,’ he said.
‘What that says is that if your case is looked at, if you’ve shown due care and attention, the likelihood of getting into trouble is negligible.
‘Many of the cases were … findings which were more to do with system issues, rather than personal issues.
‘Things go wrong, obviously, and they have to be looked at, but because people by and large know how to use opioids or are cautious about their use, when things go wrong it’s usually not the person, it’s something else.’
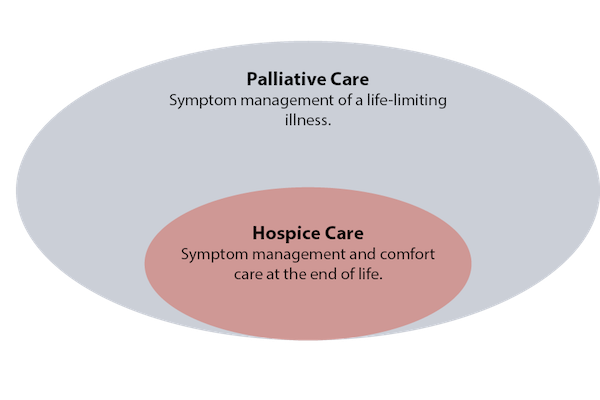
Hospice a word that is synonymous with “end of life” care. Palliative – a little more confusing and often confused with ‘end of life’. The two are very different therapies but Palliative Care is an offshoot of Hospice.
Hospice is a service for patients who are terminally ill and have decided not to take any more medication that might “cure” them (i.e. chemotherapy for a cancer patient). The focus becomes relief from pain and symptoms and not a cure. There are some who say that going into Hospice means you’re giving up or that you will no longer receive the medical care you need. That is not true – you have chosen to focus on your quality of life not the quantity and the medication used is to do just that.
A Hospice team usually includes a doctor, nurse, social worker and chaplain (if you wish). They work together to meet the patients physical, emotional and spiritual needs. This team also cares for the family who can be against the choice to, in their eyes, “give up.” There is counseling, hugs and support from a good Hospice team – my Mother’s team was unbelievable and supported and counseled our entire family through the last three days of her life.
To qualify for Hospice your doctor must state that the patient’s death is expected in 6 months or less. If a patient chooses Hospice then changes his or her mind it isn’t an issue. The patient simply goes back into the curative therapy with their doctor. You can also change your mind again and be readmitted . . . there is no pressure – it’s about what you, the patient want.
Palliative Care (pronounced pal-lee-uh-tiv) is specialized medical care for people with serious illness. This type of care is focused on providing relief from the pain, symptoms and stress of a serious illness for both the patient and family.
Again, it’s a team of specially-trained doctors, nurses and other specialists who work in partnership with the patient’s other doctors to provide an extra layer of support. It can be used at any age and at any stage in a serious illness. The services are offered in tandem with the curative treatment. A good example of Palliative Care use is in Parkinsons or Multiple Sclerosis when there are flare ups.
Both Hospice and Palliative Care are paid for by most insurance companies including Medicare and Medicaid. Both are offered in your home, nursing homes, assisted living centers, hospitals and provide respite care when the caretaker family needs a break.
What these two services offer us are choices in treatment for serious illnesses. We each have our own journey and whilst none of us hope it comes to either of these services, we can make informed decisions for us or our loved ones knowing that they exist. No matter how strong you are physically and emotionally – watching a loved one suffer is often intolerable. There are teams out there to support and comfort. Use them if you need them.
Several years ago, MapQuest directed me on a 10-hour drive to visit my father in a Florida hospital. Complications from diabetes, including blindness, kidney failure, congestive heart failure, and a below-the-knee amputation, had taken their toll. This time my father, 69, was hospitalized for an infection of unknown origin that physicians could not name, despite their many attempts to grow cultures.
I did not know it at the time, but my father was dying.
Once I arrived at the hospital from Durham, North Carolina, I could hear his screams from the nurses’ station. “Never mind. I hear him,” I told the nurse whom I had just asked the location of my father’s room. “I’ll follow the sounds.”
That any patient would be left in so much pain that his screams could be heard down the hall was unacceptable to me. That this patient was my father, a man I had always known as a big, strong former football player – the kind of man other men didn’t dare cross (but who was also loving and gentle) – was difficult for me to process. Yet, here I was, being guided to his hospital room by the sound of his cries. Despite being a trained philosopher with an interest in bioethics, I had not yet begun to think about the ways in which racialized health disparities manifest even at the end of life. My father’s excruciatingly painful process of dying was but one example.
The author with her father, John Wesley Wilson, on Easter Sunday, 1977.
Gaps while living, gaps while dying
It is well documented that African-Americans experience excess mortality, or deaths beyond the expected mortality rate. However, even if disparities in the mortality rate for African-Americans were rectified tomorrow, the fact remains that we will all eventually die. And how we die matters.
According to a 2013 Pew Research survey, 72 percent of American adults have given at least some thought to their end of life wishes, with 37 percent of American adults having given their end of life wishes a “great deal of thought.” Some of these wishes include decisions about pain management, maintaining quality of life, and whether to continue aggressive medical treatment for terminal illness.
Additionally, research shows that people tasked with making treatment decisions for loved ones who cannot express their own wishes sometimes experience distress about watching their loved one suffer. Even months or years later, they wonder whether they made the “right” decision.
Pain ignored
Black patients generally receive worse pain management in primary care environments and emergency rooms. Even black children are not treated for their pain to the extent that white children are. Some attribute this to false beliefs about biological differences between black and white patients, including the belief that black people have “thicker skin” and, therefore, do not experience as much pain as whites. These false beliefs lead to inaccurate pain assessments by physicians evaluating black patients and an unwillingness to take the pain complaints of black patients as seriously.
This disparity in black patients’ pain management continues even as black patients are dying. Families often want to ensure that their loved ones are as comfortable as possible once patients reach the point where death is near. Racialized gaps in pain management lead to a denial of humane comfort care that contributes to unnecessary suffering for black patients and their loved ones.
Symptoms ignored
Pain is ignored more in African Americans patients, and so are symptoms.
Inadequate pain management is but one aspect of the lower quality of care that black patients report in general that affects when and how black patients die. In December 2015, 57 year-old Barbara Dawson was arrested and forcibly removed from Calhoun Liberty Hospital near Tallahassee, Florida, after she refused to leave without further treatment. Although she had been evaluated in the hospital, she was discharged despite her continued complaints of difficulty breathing. Hospital personnel apparently assumed she was faking her symptoms and called police to arrest her for being disruptive. Dawson collapsed before she could be placed in the police cruiser and was returned to the hospital where she died an hour later from an undetected blood clot in her lungs.
Dawson may or may not have been at the end of life when she arrived at the hospital. However, hospital staff allowed her condition to deteriorate by not taking her complaints seriously. She died only feet away from people who could have, at minimum, eased her process of dying. The hospital was later fined US$45,000, and Dawson’s estate settled a lawsuit against the hospital for $200,000 in 2017.
Less interaction
Dawson’s experience is a dramatic and appalling case. Nevertheless, one groundbreaking study revealed that physicians generally interact less – both verbally and nonverbally – with black patients who are dying than with white patients who are dying. At the end of their lives, black patients do not receive the same comfort care, including eye contact and touch, from physicians that white patients do.
The U.S. health care system can improve care for all patients at the end of life. However, this system still denies black patients the kinds of interventions that white patients often take for granted. This denial contributes to more painful, horrific deaths of black patients and compounds the grief of their loved ones.
In my father’s case, even as part of me still hoped for a miracle, the thing I wanted most in the world was for him to be as comfortable as possible. That this did not happen despite my best efforts still haunts me when I think about the end of my father’s life.
If someone you love has died in a hospital, you may have seen modern death at its worst: overly medicalized, impersonal, and filled with unnecessary suffering. The experience can be a bitter lesson in Buddha’s most basic teaching: the more we try to avoid suffering (including death), the worse we often make it.
Even though roughly half of Americans die in hospitals and other institutions, most of us yearn to die at home, and perhaps to experience our leavetaking as a sacred rite of passage rather than a technological flail. You don’t have to be a saint, or be wealthy, or have a Rolodex of influential names to die well. But you do need to prepare. It helps to be a member of at least one “tribe,” to have someone who cares deeply about you, and to have doctors who tell you necessary truths so that you can decide when to stop aggressive treatment and opt for hospice care. Then those who care for you can arrange the basics: privacy, cleanliness, and quiet, the removal of beeping technologies, and adequate pain control. They can listen and express their love, and provide the hands-on bedside care hospice doesn’t cover.
From then on, a more realistic hope for our caregivers, and for ourselves when we are dying, may not be an idealized “good death” by a well-behaved patient, but a “good enough death,” where we keep the dying as comfortable and pain-free as possible, and leave room for the beautiful and the transcendent—which may or may not occur.
Hospice professionals often warn against high expectations. Things will probably not go as planned, and there comes a point when radical acceptance is far more important than goal-oriented activity. They don’t like the idea, inherent in some notions of the “good death,” of expecting the dying to put on a final ritual performance for the living, one marked by beautiful last words, final reconciliations, philosophical acceptance of the coming of death, lack of fear, and a peaceful letting go.
“In It Together” by Nancy Borowick. Nancy Borowick’s photo series (January 2013 through December 2014) depicts the experiences of Howie and Laurel Borowick, partners for over 30 years, who found their lives consumed by doctor appointments and the shared challenges of chemotherapy.“The Calm before the Storm”“His and Hers”
“I don’t tell families at the outset that their experience can be life-affirming, and leave them with positive feelings and memories,” said hospice nurse Jerry Soucy. “I say instead that we’re going to do all we can to make the best of a difficult situation, because that’s what we confront. The positive feelings sometimes happen in the moment, but are more likely to be of comfort in the days and months after a death.” This is what it took, and how it looked, for the family of John Masterson.
John was an artist and sign painter, the ninth of ten children born to a devout Catholic couple in Davenport, Iowa. His mother died when he was 8, and he and two of his sisters spent nearly a year in an orphanage. He moved to Seattle in his twenties, earned a black belt in karate, started a sign-painting business, and converted to Nichiren Shoshu, the branch of Buddhism whose primary practice is chanting. He never left his house without intoning three times in Japanese Nam Myoho Renge Kyo (“I Honor the Impeccable Teachings of the Lotus Sutra”).
He was 57 and living alone, without health insurance, when he developed multiple myeloma, an incurable blood cancer. He didn’t have much money: he was the kind of person who would spend hours teaching a fellow artist how to apply gold leaf, while falling behind on his paid work. But thanks to his large extended family, his karate practice, and his fierce dedication to his religion, he was part of several tribes. He was devoted to his three children—each the result of a serious relationship with a different woman—and they loved him equally fiercely. His youngest sister, Anne, a nurse who had followed him to Seattle, said he had “an uncanny ability to piss people off but make them love him loyally forever.”
When he first started feeling exhausted and looking gaunt, John tried to cure himself with herbs and chanting. By the time Anne got him to a doctor, he had a tumor the size of a half grapefruit protruding from his breastbone. Myeloma is sometimes called a “smoldering” cancer, because it can lie dormant for years. By the time John’s was diagnosed, his was in flames.
Huge plasma cells were piling up in his bone marrow, while other rogue blood cells dissolved bone and dumped calcium into his bloodstream, damaging his kidneys and brain function. He grew too weak and confused to work or drive. Bills piled up and his house fell into foreclosure. Anne, who worked the evening shift at a local hospital, moved him into her house and drove him to various government offices to apply for food stamps, Social Security Disability, and Medicaid. She would frequently get up early to stand in line outside social services offices with his paperwork in a portable plastic file box.
Medicaid paid for the drug thalidomide, which cleared the calcium from John’s bloodstream and helped his brain and kidneys recover. A blood cancer specialist at the University of Washington Medical Center told him that a bone marrow transplant might buy him time, perhaps even years. But myeloma eventually returns; the transplant doesn’t cure it. The treatment would temporarily destroy his immune system, could kill him, and would require weeks of recovery in sterile isolation. John decided against it, and was equally adamant that he’d never go on dialysis.
After six months on thalidomide, John recovered enough to move into a government-subsidized studio apartment near Pike Place Market. He loved being on his own again and wandered the market making videos of street musicians, which he’d post on Facebook. But Anne now had to drive across town to shop, cook, and clean for him.
The health plateau lasted more than a year. But by the fall of 2010, John could no longer bear one of thalidomide’s most difficult side effects, agonizing neuropathic foot pain. When he stopped taking the drug, he knew that calcium would once again build up in his bloodstream, and that he was turning toward his death.
An older sister and brother flew out from Iowa to help Anne care for him. One sibling would spend the night, and another, or John’s oldest daughter, Keely, a law student, would spend the day.
Christmas came and went. His sister Irene returned to Iowa and was replaced by another Iowa sister, Dottie, a devout Catholic. In early January, John developed a urinary tract infection and became severely constipated and unable to pee. Anne took him to the University of Washington Medical Center for what turned out to be the last time. His kidneys were failing and his bones so eaten away by disease that when he sneezed, he broke several ribs. Before he left the hospital, John met with a hematologist, a blood specialist, who asked Anne to step briefly out of the room.
Anne does not know exactly what was said. But most UW doctors are well trained in difficult conversations, thanks to a morally responsible institutional culture on end-of-life issues. Doctors at UW do not simply present patients with retail options, like items on a menu, and expect them to blindly pick. Its doctors believe they have an obligation to use their clinical experience to act in their patients’ best interests, and they are not afraid of making frank recommendations against futile and painful end-of-life treatments. When the meeting was over, the doctor told Anne that her brother “wanted to let nature take its course.” He would enroll in hospice. Anne drove him home.
John knew he was dying. He told Anne that he wanted to “feel everything” about the process, even the pain. He took what she called “this Buddhist perspective that if he suffered he would wipe out his bad karma. I said, ‘Nah, that’s just bullshit. You’ve done nothing wrong. The idea that we’re sinners or have to suffer is ludicrous.’” She looked her brother in the eye. She knew she was going to be dispensing his medications when he no longer could, and she wasn’t going to let him suffer. She told him, ‘You’re not going to have a choice.’”
The drive to treatment takes half an hour, and Howie and Laurel Borowick take turns, resting and driving, depending on who’s getting treatment that day. “The Drive to Chemo”In Laurel’s final moments, her family assured her that all would be OK. “Last Touch”
Anne said she “set an intention”: not to resist her brother’s dying, but to give him the most gentle death possible and to just let things unfold. On January 15, her birthday, she and John and a gaggle of other family members walked down to Pike Place Market to get a coffee and celebrate. John was barely able to walk: Anne kept close to him so that she could grab him if he fell. It was the last time he left the house.
The next morning, a Sunday, while Anne was sitting with John at his worktable, he looked out the window and asked her, “Do you think I’ll die today?” Anne said, “Well, Sundays are good days to die, but no, I don’t think it’s today.” It was the last fully coherent conversation she had with him.
He spent most of his last nine days in bed, as his kidneys failed and he grew increasingly confused. He didn’t seem afraid, but he was sometimes grumpy. He had increasing difficulty finding words and craved celery, which he called “the green thing.” He would ask Anne to take him to the bathroom, and then forget what he was supposed to do there. His daughter Keely took a leave of absence from law school, and Anne did the same from her job at the hospital. Fellow artists, fellow chanters, former students to whom he’d taught karate, nephews, nieces, and sign-painting clients visited, and Anne would prop him up on pillows to greet them.
Anne managed things, but with a light hand. She didn’t vet visitors, and they came at all hours. If she needed to change his sheets or turn him, she would ask whoever was there to help her, and show them how. That way, she knew that other people were capable of caring for him when she wasn’t there. “The ones that have the hardest time [with death] wring their hands and think they don’t know what to do,” she said. “But we do know what to do. Just think: If it were my body, what would I want? One of the worst things, when we’re grieving, is the sense that I didn’t do enough,” she said. “But if you get in and help, you won’t have that sense of helplessness.”
Each day John ate and spoke less and slept more, until he lost consciousness and stopped speaking entirely. To keep him from developing bedsores, Anne would turn him from one side to the other every two hours, change his diaper if necessary, and clean him, with the help of whoever was in the room. He’d groan when she moved him, so about a half an hour beforehand, she’d crush morphine and Ativan pills, mix them with water as the hospice nurse had showed her, and drip them into John’s mouth.
One morning her distraught brother Steve accused her of “killing” John by giving him too much morphine—a common fear among relatives, who sometimes can’t bear to up the dose as pain gets worse. At that moment, the hospice nurse arrived by chance, and calmly and gently explained to Steve, “Your brother is dying, and this is what dying looks like.”
The death was communal. People flowed in and out, night and day, talking of what they loved about John and things that annoyed them, bringing food, flowers, candles, and photographs until John’s worktable looked like a crowded altar. Buddhists lit incense and chanted. Someone set up a phone tree, someone else made arrangements with a funeral home, and one of the Buddhists planned the memorial service.
Most of the organizing, however, fell to Anne. It may take a village to die well, but it also takes one strong person willing to take ownership—the human equivalent of the central pole holding up a circus tent. In the final two weeks, she was in almost superhuman motion. She leaned in, she said, “into an element of the universe that knows more than I know. I was making it up as I went along. People contributed and it became very rich.
“That’s not to say there weren’t times when it was phenomenally stressful. I was dealing with all the logistics, and with my own mixed emotions about my brother. I was flooded with memories of our very complicated relationship, and at the same time I knew my intention was that he be laid to rest in the most gentle way possible.”
Hospice was a quiet support in the background. Over the two years of his illness, John’s care had perfectly integrated the medical and the practical, shifting seamlessly from prolonging his life and improving his functioning— as thalidomide and the doctors at UW had done—to relieving his suffering and attending his dying, as the hospice nurses and those who loved him had done.
There were no demons under the bed or angels above the headboard. Nor were there beeping monitors and high-tech machines. His dying was labor-intensive, as are most home deaths, and it was not without conflict.
A few days before he died, two siblings beseeched Anne to call a priest to give John last rites in the Catholic church. “It was a point of love for my siblings. They were concerned that John was going to burn in hell,” Anne said. “But John hated priests.” In tears, Anne called the Seattle church that handled such requests, and the priest, after a brief conversation, asked her to put her sister Dottie on the phone. Yes, Dottie acknowledged, John was a Buddhist. No, he hadn’t requested the sacraments. Yes, his children were adamantly opposed. No, the priest told her, under the circumstances he couldn’t come. It wasn’t John’s wish.
Ten days after the family’s last walk through Pike Place Market, the hospice nurse examined John early one morning and said, “He won’t be here tomorrow.” She was seeing incontrovertible physical signs: John’s lips and fingertips were blue and mottled. He hadn’t opened his eyes in days. His breathing was labored and irregular, but still oddly rhythmic, and he looked peaceful. The hospice nurse left. Anne, helped by John’s daughter Keely and his sister Dottie, washed and turned John and gave him his meds. Then they sat by his side. Anne had her hand on his lap.
“It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.
“He just had this one-room apartment with a little half-wall before the kitchen. I walked over to put water on to make coffee, and Keely said, ‘His breathing’s changed.’”Anne stopped, ran over, sat on the bed, and lifted her brother to a sitting position. He was light. She held him close, and during his last three breaths she chanted Nam Myoho Renge Kyo, as her brother had always done, three times, whenever he left his house. “I was really almost mouth-to-mouth chanting, and he died in my arms,” she said. “We just held him, and then my sister Dottie said her prayers over him.”
Anne sat next to her brother and said, “John, I did well.”
“I know he would not have been able to orchestrate it any better than how it unfolded,” she said.
“It was a profound experience for me. I realized what a good death could be.”
My story begins eight years ago, when I was approached by my first client requesting that I supervise her in a therapeutic session with a psychedelic medicine.
She had debilitating depression and anxiety brought on by a breast cancer diagnosis. Although she had survived her cancer, she couldn’t shake her terrible emotional distress. She had tried therapists, pills and a residential program. Nothing had worked.
Then she came across stories in the media about research at UCLA using psilocybin (the active ingredient in magic mushrooms) with cancer patients suffering from what was called “end-of-life distress” and how this new treatment was showing really promising results.
She was desperate to try it for herself.
Well, as a licensed therapist and academic, could I help this woman? Reading the research literature, I learned that psychedelic research was becoming well-developed as a treatment for the psycho-spiritual depression and “existential anxiety” that often accompany the diagnosis of a life-threatening illness.
I also found myself in a bind: The science was telling me that psilocybin is the treatment most likely to benefit patients with existential anxiety when other treatments have failed; my ethical code from the B.C. Association of Clinical Counsellors tells me to act to my client’s benefit; federal law forbids me to use this treatment.
This is why, together with colleagues in the Therapeutic Psilocybin for Canadians project, I filed an application with Health Canada in January 2017, seeking a so-called “Section 56 exemption” — to permit us to provide psilocybin-assisted psychotherapy to patients with terminal cancer.
Immediate decrease in death anxiety
Dinah Bazer found relief from cancer anxiety by being treated with a dose of psilocybin administered by a New York University study.
The research indicated it led to immediate, substantial and sustained decreases in depression, death anxiety, cancer-related demoralization and hopelessness.
It resulted in increased quality of life, life meaning and optimism. And these changes had persisted at a six-month follow-up.
Patients attributed improved attitudes about life and death, self, relationships and spirituality to the psilocybin experience, along with better well-being, life satisfaction and mood.
It is heartening to see research moving into Phase 3 clinical trials that will involve many more research participants. However, the foreseeable future for Canadians who need this game-changing therapy is not especially rosy.
At our current rate of progress, it may well still be years before psilocybin successfully completes Phase 3 trials and becomes available as an orthodox medicine.
Therapists risk criminal penalties
In the meantime, many Canadians with terminal cancer are also suffering from end-of-life distress, and are in dire need of relief — now.
They face serious and life-threatening illness. Their condition is terminal, so concerns about long-term effects of psilocybin are not relevant. They suffer from serious end-of-life psychological distress (anxiety and depression) to the point that it interferes with their other medical treatments. And this distress has not successfully responded to other treatments.
Psilocybin is currently a restricted drug, meaning that therapists risk criminal penalties if they aid or abet its possession. That means that we cannot recommend or encourage its use.
My professional Code of Ethics, however, states that our ethical duty is to act in a way that serves our clients’ “best interests.” The service we provide has to be “for the client’s benefit.” We must “take care to maximize benefits and minimize potential harm.”
A compassionate, humanitarian death
I agree with the Canadian medical establishment that, in ordinary circumstances, new medicines should be made available to Canadians only when they have successfully completed Phase 3 clinical trials.
In the New York University study a pill, containing either a placebo or psilocybin, was presented to the subjects in a chalice.
But I contend that the patients described here are not in ordinary circumstances. They have terminal cancer. All other treatments have failed them; they have nothing left to lose. They have the right to die; surely they have the right to try!
These patients deserve access to a still-experimental but promising medicine on compassionate and humanitarian grounds. Because of their extraordinary medical straits, psilocybin now for them represents a reasonable medical choice; it is necessary to them for a medical purpose.
Our application to Health Canada seeking a “Section 56 exemption” will be ruled on very shortly.
We fully expect that it will be denied — for political, not scientific reasons. Justin Trudeau’s Liberal government is likely in no mood to loosen up on psychedelics before the dust from the legalization of cannabis has fully settled. I think the government would like it if someone else made that decision.
Violation of our rights and freedoms
If our application is denied, we intend to file for a judicial review, and if necessary, a lawsuit in Federal Court challenging that denial.
We believe that prohibition of access to psilocybin for a legitimate medical purpose violates a citizen’s Canadian Charter of Rights and Freedoms Section 7 right to “life, liberty and security of person.”
This clause has already been interpreted by the Supreme Court to imply that a citizen has the right to autonomy in making health-care decisions. Charter-based arguments have already led to success in three recent landmark medical cannabis cases.
We argue that what applies to cannabis also applies to psilocybin:
The prohibition of … cannabis “limits the liberty of medical users by foreclosing reasonable medical choices through the threat of criminal prosecution. Similarly, by forcing a person to choose between a legal but inadequate treatment and an illegal but more effective one, the law also infringes on security of person.” Supreme Court of Canada, R. v. Smith, 2015
One thing that unites all of us human beings is that we will die. Imagine if, when our time comes, we could all have the option to die peacefully, with acceptance, without anxiety.












 “It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.
“It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.

