“Everyone knows loss in one way or another. This song is about that,” Marcus Mumford says of Delta track
A young boy watches over his dying mother and fantasizes about better times with her in the video for Mumford and Sons’ new Delta single “Beloved.” The son and mother, who’s still wearing a hospital gown, run around, go shoplifting and ride horses on a beach. “Before you leave, you must know you are beloved,” Marcus Mumford sings against a serene backdrop of synths and guitars, “and before you leave, remember I was with you.” It all builds to an emotional finale.
“Everyone knows loss in one way or another,” Marcus Mumford said in a statement. “This song is about that. I’d never sat with anyone as they died before, and it had an effect on me. As it does everyone I know who has experienced it. But there’s wildness and beauty in it as well, and a deep honoring, that became the beginnings of this song that we worked up called ‘Beloved.’ I feel determined for people to take whatever they want from it, and not to be emotionally prescriptive.”
It’s hard to know what to do or say when someone you know loses a person who was close to them. Grief is a scary and amorphous thing, and if you haven’t experienced it, reaching out can feel like overstepping a boundary or reminding someone of something they’re trying to forget.
But grief is as isolating as it is painful, and it is important to let bereaved friends and acquaintances know you are thinking of them and their loved one, no matter how awkward it feels. This is true if you knew the person they’ve lost; this is also true if you didn’t.
“Most grieving people, whether they’re aware of it or not, one of their biggest fears is that the person who has been lost will be forgotten,” Jennifer Soos, a licensed marriage and family therapist in San Antonio, Texas, says. “Anytime someone remembers them, acknowledges them, speaks about them, conjures them in any way, it’s like a balm to that fear.”
So, though it might seem like ignoring a loss makes it easier for the person in mourning to move on, it’s actually the worst thing you can do. And though it may seem trite to tell someone, “I’m sorry for your loss,” at the very least, acknowledging both that the lost person existed and that now they do not will make your grieving friend feel heard and validated. “I don’t think it can happen too often,” Soos says.
Here’s how to do it.
Send a card—or any kind of message
Or an email, or a text message, depending on what generation the person in mourning belongs to, and how well you know them. “If you are a millennial and it’s a peer, a text message is fine,” Soos says. “An email is better than a text message, because you had to actually sit at a computer to do it. I’m firmly and squarely in Generation X, so I prefer a handwritten note, but I recognize that is a generational preference.”
Basically, doing something is better than doing nothing, but everyone likes a card. (It’s also noteworthy that a text can get lost in the post-death deluge, which is something to keep in mind.)
It’s okay not to know what to say (but here are a few things you might want to)
No one really knows what to say to someone in mourning, particularly if the death of their loved one was unexpected. It’s perfectly fine to admit that in your letter. “The ‘right’ thing to say, in my opinion, is just the truth,” Soos says. “That is what we hear over and over and over again from bereaved people in therapy and support groups and in research. What they say is, ‘I wish people would just say, ‘I don’t know what to say but I’m sorry.’ ‘I don’t know what to say but I’m sad for you.’ ‘I don’t know what to say, but I care for you.’”
You want to let the person know that you’re thinking of them, and you’re there for them, and you’re available to listen. You are not expected to make them feel better, because when you are grieving, nothing will make you feel better. But you do not want to feel ignored or alone. “It seems very vulnerable to say, ‘I don’t know what to say,’” Soos says. “We worry it will be awkward or offensive or upsetting to a person. But the truthful thing is, we don’t know what to say. There are no words that are going to make it better, unless you have a magical spell to bring the dead back to life.”
So, feel free to stick to platitudes, as long as they’re truthful. “One of the things people can say is, ‘I don’t know what to say, but I love you and I’m here for you,’” Dr. Marilyn Mendoza, a psychologist in New Orleans, says. “Or, ‘I’m thinking about you and sending you love.’ Or, ‘No words can describe how sorry I am for your loss. My heart goes out to you.’”
As Soos puts it, “What you are really trying to communicate is, ‘I am here for you. I witness what you are going through, I acknowledge it, I’m not ignoring it, I do not need to have perfect words to help you. You are seen and you’re heard and I’m sharing in the burden of this pain with you just simply by acknowledging it.”
Don’t talk about yourself
This should be obvious, but a condolence note is not the time to broadcast your own life updates. “The note should be for the bereaved,” Mendoza says. “Don’t include stuff about yourself, like I just got a new job or here’s my new address.” Similarly…
Don’t say, ‘I know how you feel’
It’s tempting to empathize with someone in mourning, especially if you’ve experienced loss yourself. But grief manifests differently for everyone, and it can be invalidating to have someone claim to know your specific feelings when they do not. “Don’t say, ‘I know how you feel,’ because even if you’ve lost your mother, you don’t really know how that other person feels. You know how you felt about it,” Mendoza says.
It’s also not helpful to offer advice. “Nobody really wants advice,” Soos says. “It makes some subtle judgment that there’s a right or wrong way to grieve.”
And if you were thinking of using the words “at least” at any point, don’t. “I always tell people, if you’re going to say the words ‘at least,’ you should stop,” Soos says. “You’re about to justify why it shouldn’t be painful, which is invalidating.”
Don’t presume to know the relationship between the person in mourning and the person they lost
It’s common to include a message in a condolence card commenting on how special the deceased was to the bereaved. But if you didn’t know the person who died or much about their relationship with the person you’re writing to, you might want to avoid making any assumptions.
“If you don’t know the person, commenting about them might not be the best thing,” Mendoza says. “Sometimes it’s not a very special relationship.” Of course, if you did know for a fact that this person was very close to your friend, feel free to say so. You also might want to include the deceased’s name. “When you’re the bereaved, people often won’t use the person’s name, but it means a lot to them,” Mendoza says. “So you can say something like, ‘I know David was a special person for you.’”
Offer concrete help, if any
A thing people often say in times of strife is, “Let me know if there’s anything I can do.” It’s not that this is necessarily a bad thing to say, but someone in mourning isn’t going to do the work to take you up on it. Instead of offering vague assistance, “Offer them something specific, and let them tell you whether it will be helpful or not,” Soos says. Ask them if you can bring them dinner, or feed their cat, or babysit their kids, or take them for a drink and lend an ear.
And if you know them well enough (and know that it wouldn’t be an intrusion), feel free to do something without being asked. “I have a really good friend and one of her closest friends died recently,” Soos said. “I didn’t ask, I just showed up at her house and brought dinner.”
Reach out a second time after the immediate mourning period has ended
Most people reach out to the bereaved right upon hearing the news, which is certainly the right thing to do. But immediately after someone dies, everything feels like a blur, and while it’s very nice to be flooded with texts and emails and lovely cards, it’s hard to appreciate the heartfelt messages in the moment. Soos recommends reaching out to those in grieving a second time, after the initial mourning period has ostensibly ended.
“The truth of the matter is that people in those first days or weeks [after a death], they don’t really remember much, quite frankly,” Soos says. “When you hear the news, do an initial reach out, but then immediately mark on your calendar, 4-16 weeks out. That’s the time that most people need more support and encouragement.”
Soos says that after a few months, most people who weren’t close to the deceased move on, but for those who are grieving, the pain hasn’t subsided. “The horrible thing about timing and grief is that the period where the shock starts wearing off coincides with the time everyone else is moving on. And that’s when you’re really settling into, ‘Oh my goodness, this is my real life and this sucks,’” Soos says. “Those messages and notes and texts that come at the 3-month, 4-month mark and on can be more meaningful than the initial reach out.”
So, after a few months, send a text, take your friend to dinner, go to their house with a bottle of wine and a good movie, and let them tell you about the person they loved. Don’t feel like you’re forcing someone to rehash unpleasantness, or reminding them of something they want to forget. What they really want, is not to be forgotten.
Being part of the disability community means constantly losing friends and allies. I don’t expect that to change.
By Robyn Powell
“Kristen has passed away.” I’ll never forget learning that my best friend died. I was only 11 years old. We lived in the same town and attended school together. She had spina bifida as well as problems with her kidneys. After years of dialysis, it was kidney failure that ultimately killed Kristen.
Now, at 37, I have lost count of the number of loved ones who have died. I do know that it is well over 20. Friends have died. Colleagues have died. Romantic partners have died. Even my first love died a few years ago. Each year I lose at least a few people I care about, and I don’t expect that to change. The deaths of people close to me are something I have come to accept.
Just last month, my friend Carrie Ann Lucas died after her health insurer refused to cover the medication she needed. Yes, she had a progressive disability but its symptoms were exacerbated because she did not receive adequate health care.
Other pioneers in the disability community, whom I looked up to, also died recently. Dr. Anita Silvers, a professor of philosophy at San Francisco State, died after complications from pneumonia. Professor Mike Oliver from the University of Greenwich in England died after a short illness. Oliver is known for developing the social model of disability.
I was born with arthrogryposis, a disability that affects my muscles and joints. I use a power wheelchair and have limited use of my arms and legs. Being disabled is normal for me. Indeed, it is all I know. It is also something I am incredibly proud of.
But each time a disabled friend dies I find myself questioning many things in my life. And one recurring question is this: How I can I maintain my disability pride when I am always surrounded by death? It is not always easy. In fact, at times it can feel insurmountable. While some of my friends have died because of their disabilities, others have died because of broken systems that devalue the lives of disabled people.
Some disabilities are associated with shorter life expectancies, but many are not. And, because of advances in technology and treatment, people with disabilities once considered terminal are living longer. Stephen Hawking, who lived for decades with A.L.S. proved that. Nevertheless, being part of the disability community means being surrounded not just by the life and support, but by death.
Research shows that people with disabilities die younger than nondisabled peers. Sometimes our life spans are shortened because of our disabilities, but that is not always the case. In one study, researchers found that disabled people are more likely than nondisabled people to die from heart disease, cancer, stroke, respiratory disease, accidents suicides and assaults. And while physical and circumstantial factors are at play, it is often the way we are treated that contributes to early death.
I have been around disabled people my entire life. The disability community is where I feel the most comfortable to be myself. They understand my experiences — both good and bad — and offer great insights without trying to fix me or my disability. They don’t see our disabilities as tragedies or something to be ashamed of. They appreciate how much it sucks when an airline breaks my wheelchair or a personal care assistant doesn’t show up, but they also recognize how important disability pride is.
Being a part of the disability community has made me who I am — and I don’t just mean in the physical sense. I have had beautiful and rich experiences, not in spite of, but because I am disabled. I have met truly amazing people whom I would never know if I weren’t disabled. Having a disability has also informed my life’s work. First as a social worker and now as an attorney and researcher, I have committed myself to fight for disability rights. My disability and the experiences I have had make me better at my work. I likely wouldn’t be in this field if I weren’t disabled, but I am thankful that I get to do this work.
Not everyone understands disability pride, which is apparent when a disabled person dies and nondisabled people nearly always repeat the same ableist remarks: “They are no longer suffering.” “She is now free to run.” “He is finally cured and now dancing among the angels.” I can’t say hearing these things doesn’t get to me; it does. These comments diminish the lives both of the dead and the living. Most of us are fine not running; we are not suffering, and we do not want to be cured.
During difficult times, I sometimes find myself wondering why I allow myself to continue to be surrounded by death. Having disabled friends means frequent loss. Death and disability are uncomfortable bedfellows. But to avoid this constant grieving would mean to rid myself of a community that I love.
In some ways, I believe that being surrounded by death has allowed me to live a more fulfilling life. I try to cherish my time with loved ones, intensely aware that it could be the last time I see them. I also strive to live in the moment, appreciating the little things in life. Because I have experienced so much loss, I know the importance of celebrating the good times.
Death is unavoidable. But as a disabled person, I am all too aware that death and disability are inextricably linked. Because of my disability, I have an enriched life. I have also experienced tremendous heartbreak. In the end, I have come to understand that I will love, and I will grieve. There’s something almost freeing about accepting that harsh reality.
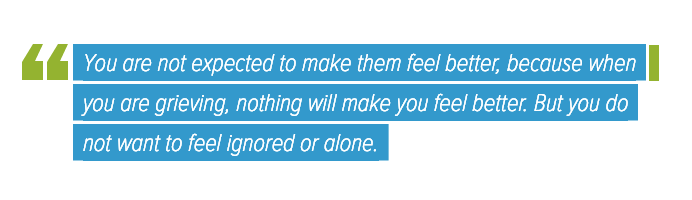
Few people have enchanted the popular imagination with science more powerfully and lastingly than physicist Richard Feynman (May 11, 1918–February 15, 1988) — the “Great Explainer” with the uncommon gift for bridging the essence of science with the most human and humane dimensions of life.
“My heart stopped,” Gleick tells me. “I have never had an experience like that as a biographer, before or since.”
In a mass of unread papers sent to him by Feynman’s widow, Gweneth, Gleick found a letter that discomposed his most central understanding of Feynman’s character. A generation after computing pioneer Alan Turing tussled with the binary code of body and spirit in the wake of loss, Feynman — a scientist perhaps uncommonly romantic yet resolutely rational and unsentimental in his reverence for the indomitable laws of physics that tend toward decay — penned a remarkable letter to a physical nonentity that was, for the future Nobel-winning physicist, the locus of an irrepressible metaphysical reality.
Richard Feynman as a young man
In high school, the teenage Richard spent summers at the beach in his native Far Rockaway. There, he grew besotted with a striking girl named Arline — a girl he knew he would marry. Both complement and counterpoint to his own nature, Arline met Richard’s inclination for science with ardor for philosophy and art. (The art class he took just to be near her would lay the foundation for his little-known, lifelong passion for drawing.) By his junior year, Richard proposed. Arline accepted. With the eyes of young love, they peered into a shared future of infinite possibility for bliss.
But they were abruptly grounded when a mysterious malady began afflicting Arline with inexplicable symptoms — a lump would appear and disappear on her neck, fevers would roil over her with no apparent cause. Eventually, she was hospitalized for what was believed to be typhoid.
Gleick writes:
Feynman began to glimpse the special powerlessness that medical uncertainty can inflict on a scientific person. He had come to believe that the scientific way of thinking brought a measure of calmness and control in difficult situations — but not now.
Just as Feynman began bombarding the doctors with questions that steered them toward a closer approximation of the scientific method, Arline began to recover just as mysteriously and unpredictably as she had fallen ill. But the respite was only temporary. The symptoms returned, still shorn of a concrete explanation but now unambiguously pointing toward the terminal — a prognosis Arline’s doctors kept from her. Richard refused to go along with the deception — he and Arline had promised each other to face life with unremitting truthfulness — but he was forced to calibrate his commitment to circumstance.
Gleick writes:
His parents, Arline’s parents, and the doctors all urged him not to be so cruel as to tell a young woman she was dying. His sister, Joan, sobbing, told him he was stubborn and heartless. He broke down and bowed to tradition. In her room at Farmingdale Hospital, with her parents at her side, he confirmed that she had glandular fever. Meanwhile, he started carrying around a letter — a “goodbye love letter,” as he called it — that he planned to give her when she discovered the truth. He was sure she would never forgive the unforgivable lie.
He did not have long to wait. Soon after Arline returned home from the hospital she crept to the top of the stairs and overheard her mother weeping with a neighbor down in the kitchen. When she confronted Richard — his letter snug in his pocket — he told her the truth, handed her the letter, and asked her to marry him.
Marriage, however, proved to be a towering practical problem — Princeton, where Feynman was now pursuing a Ph.D., threatened to withdraw the fellowships funding his graduate studies if he were to wed, for the university considered the emotional and pragmatic responsibilities of marriage a grave threat to academic discipline.
Just as Feynman began considering leaving Princeton, a diagnosis detonated the situation — Arline had contracted a rare form of tuberculosis, most likely from unpasteurized milk.
At first, Feynman was relieved that the grim alternative options of Hodgkin’s disease and incurable cancers like lymphoma had been ruled out. But he was underestimating, or perhaps misunderstanding, the gravity of tuberculosis — the very disease which had taken the love of Alan Turing’s life and which, during its two-century heyday, had claimed more lives around the globe than any other malady and all wars combined. At the time of Arline’s diagnosis in 1941, immunology was in its infancy, the antibiotic treatment of bacterial infections practically nonexistent, and the first successful medical application of penicillin a year away. Tuberculosis was a death sentence, even if it was a slow death with intervals of remission — a fact Richard and Arline faced with an ambivalent mix of brave lucidity and hope against hope.
Meanwhile, Richard’s parents met the prospect of his marriage with bristling dread. His mother, who believed he was marrying Arline out of pity rather than love, admonished him that he would be putting his health and his very life in danger, and coldly worried about how the stigma attached to tuberculosis would impact her brilliant young son’s reputation. “I was surprised to learn such a marriage is not unlawful,” she scoffed unfeelingly. “It ought to be.”
But Richard was buoyed by love — a love so large and luminous that he found himself singing aloud one day as he was arranging Arline’s transfer to a sanatorium. Determined to go through with the wedding, he wrote to his beloved:
I guess maybe it is like rolling off of a log — my heart is filled again & I’m choked with emotions — and love is so good & powerful — it’s worth preserving — I know nothing can separate us — we’ve stood the tests of time and our love is as glorious now as the day it was born — dearest riches have never made people great but love does it every day — we’re not little people — we’re giants … I know we both have a future ahead of us — with a world of happiness — now & forever.
On June 29, 1942, they promised each other eternity.
Wedding Day
Gleick writes:
He borrowed a station wagon from a Princeton friend, outfitted it with mattresses for the journey, and picked up Arline in Cedarhurst. She walked down her father’s hand-poured concrete driveway wearing a white dress. They crossed New York Harbor on the Staten Island ferry — their honeymoon ship. They married in a city office on Staten Island, in the presence of neither family nor friends, their only witnesses two strangers called in from the next room. Fearful of contagion, Richard did not kiss her on the lips. After the ceremony he helped her slowly down the stairs, and onward they drove to Arline’s new home, a charity hospital in Browns Mills, New Jersey.
Meanwhile, WWII was reaching its crescendo of destruction, dragging America into the belly of death with the attack on Pearl Harbor. Now one of the nation’s most promising physicists, Feynman was recruited to work on what would become the Manhattan Project and soon joined the secret laboratory in Los Alamos.
Los Alamos badge
Arline entered the nearby Albuquerque sanatorium, from where she wrote him letters in code — for the sheer fun of it, because she knew how he cherished puzzles, but the correspondence alarmed the military censors at the laboratory’s Intelligence Office. Tasked with abating any breaches to the secrecy of the operation, they cautioned Feynman that coded messages were against the rules and demanded that his wife include a key in each letter to help them decipher it. This only amplified Arline’s sense of fun — she began cutting holes into her letters, covering passages with ink, and even mail-ordered a jigsaw puzzle kit with which to cut up the pages and completely confound the agents.
But the levity masked the underlying darkness which Richard and Arline tried so desperately to evade — Arline was dying. As her body failed, he steadied himself to her spirit:
You are a strong and beautiful woman. You are not always as strong as other times but it rises & falls like the flow of a mountain stream. I feel I am a reservoir for your strength — without you I would be empty and weak… I find it much harder these days to write these things to you.
In every single letter, he told her that he loved her. “I have a serious affliction: loving you forever,” he wrote.
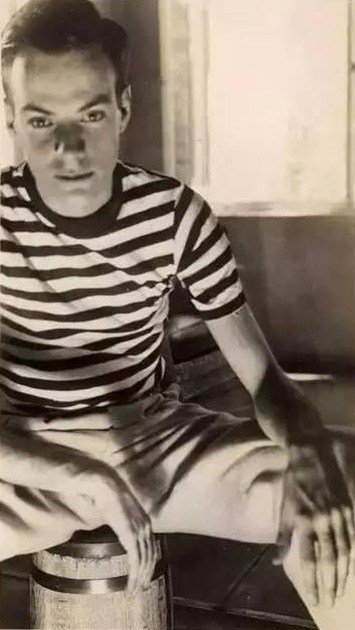
at the Albuquerque sanatorium
In early 1945, two and a half years into their marriage, Richard and Arline made love for the first time. He had been too afraid of harming her frail health somehow, she too afraid of infecting him with the deadly bacterium consuming her. But Arline insisted that this pent up desire could no longer be contained and assured Richard that this would only bring them closer — to each other, and to the life they had so lovingly dreamt up for themselves:
I’ll always be your sweetheart & first love — besides a devoted wife — we’ll be proud parents too… I am proud of you always Richard –[you are] a good husband, and lover, & well, coach, I’ll show you what I mean Sunday.
But heightened as their hopes were by this new dimension of shared experience, Arline’s health continued to plummet. Her weight dropped to eighty-four pounds. Exasperated by the helplessness of medicine, which Feynman had come to see not as a manifestation but as a mutilation of the scientific method, he invested all hope in an experimental drug made of mold growths. “Keep hanging on,” he exhorted Arline. “Nothing is certain. We lead a charmed life.” She began spitting blood.
At twenty-seven, on the precipice of a brilliant scientific career, he was terminally in love.
On June 16, 1945, while working at the computing room at Los Alamos, Feynman received a call from the sanatorium that Arline was dying. He borrowed a colleague’s car and sped to the hospital, where he found her immobile, her eyes barely tracing his movement. Early in his scientific career, he had been animated by the nature of time. Now, hours stretched and contracted as he sat at her deathbed, until one last small breath tolled the end at 9:21PM.
The wake of loss has a way of tranquilizing grief with the pressing demands of practical arrangements — a tranquilizer we take willingly, almost gratefully. The following morning, Feynman arranged for his beloved’s cremation, methodically collected her personal belongings, and on the final page of the small spiral notebook in which she recorded her symptoms he wrote with scientific remove: “June 16 — Death.”
And so we arrive at Gleick’s improbable discovery in that box of letters — improbable because of the extreme rationality with which Feynman hedged against even the slightest intimation of metaphysical conjectures untestable by science and unprovable by reason. During his courtship of Arline, he had been vexed by her enthusiasm for Descartes, whose “proof” of God’s perfection he found intellectually lazy and unbefitting of Descartes’s reputation as a champion of reason. He had impishly countered Arline’s insistence that there are two sides to everything by cutting a piece of paper and half-twisting it into a Möbius strip, the ends pasted together to render a surface with just one side.
Everything that appeared mystical, Feynman believed, was simply an insufficiently explained mystery with a physical answer not yet found. Even Arline’s dying hour had offered testing ground for conviction. Puzzlingly, the clock in the room had stopped at exactly 9:21PM — the time of death. Aware of how this bizarre occurrence could foment the mystical imagination in unscientific minds, Feynman reasoned for an explanation. Remembering that he had repaired the clock multiple times over the course of Arline’s stay at the sanatorium, he realized that the instrument’s unwieldy mechanism must have choked when the nurse picked it up in the low evening light to see and record the time.
How astonishing and how touchingly human, then, that Feynman penned the letter Gleick found in the box forty-two years later — a letter he wrote to Arline in October of 1946, 488 days after her death:
D’Arline,
I adore you, sweetheart.
I know how much you like to hear that — but I don’t only write it because you like it — I write it because it makes me warm all over inside to write it to you.
It is such a terribly long time since I last wrote to you — almost two years but I know you’ll excuse me because you understand how I am, stubborn and realistic; and I thought there was no sense to writing.
But now I know my darling wife that it is right to do what I have delayed in doing, and that I have done so much in the past. I want to tell you I love you. I want to love you. I always will love you.
I find it hard to understand in my mind what it means to love you after you are dead — but I still want to comfort and take care of you — and I want you to love me and care for me. I want to have problems to discuss with you — I want to do little projects with you. I never thought until just now that we can do that. What should we do. We started to learn to make clothes together — or learn Chinese — or getting a movie projector. Can’t I do something now? No. I am alone without you and you were the “idea-woman” and general instigator of all our wild adventures.
When you were sick you worried because you could not give me something that you wanted to and thought I needed. You needn’t have worried. Just as I told you then there was no real need because I loved you in so many ways so much. And now it is clearly even more true — you can give me nothing now yet I love you so that you stand in my way of loving anyone else — but I want you to stand there. You, dead, are so much better than anyone else alive.
I know you will assure me that I am foolish and that you want me to have full happiness and don’t want to be in my way. I’ll bet you are surprised that I don’t even have a girlfriend (except you, sweetheart) after two years. But you can’t help it, darling, nor can I — I don’t understand it, for I have met many girls and very nice ones and I don’t want to remain alone — but in two or three meetings they all seem ashes. You only are left to me. You are real.
My darling wife, I do adore you.
I love my wife. My wife is dead.
Rich.
And then, with the sole defibrillator for heartache we have — humor — Feynman adds:
PS Please excuse my not mailing this — but I don’t know your new address.
If we have the capacity to love, then we have to face grief as well, along with how it manifests in our lives—particularly through sleep.
BY Lisa Smalls
Losing a loved one is one of the most painful life events we endure, where grieving is a natural and recurrent phase of life for us all. If we have the capacity to love, then we have to face grief as well, along with how it manifests in our lives—particularly through sleep. Poor sleep can go hand in hand with grieving in a downwards spiral, where physical and emotional symptoms of grief can intensify when sleep issues are not addressed. Grief can be momentary or become complicated grief over time, where advanced symptoms of grief can be emotional, physical, as well as cognitive.
Emotional Wellness
Grief alone can wreak havoc on your emotional wellbeing, causing depression and anxiety that makes it hard to sleep. Sleep is a fundamental part of the grieving process that helps heal your emotions, so a lack of sleep is particularly dangerous. Specific emotions are encountered at every stage of the grieving process, where quality sleep helps you process and navigate these feelings. So grieving makes sleeping hard, but you still need sleep to recover from grieving!
Physical Wellbeing
The physical symptoms of grief are less discussed but are highly significant, where proper sleep helps your body mend faster. In addition to poor sleep, symptoms include a weakened immune system, heart problems, alcohol and substance abuse and depression. Your physical symptoms of grief can cause sleep deprivation but will also worsen without sufficient sleep. If you are experiencing advanced symptoms of grief that must be addressed and healed by better sleep, take the steps within your power to improve sleep. For example, create an ideal sleep space. Eliminate noise and light pollution, invest in your sleeping structure, and stick to a regular bedtime. The quality of your waking life depends on how you invest in your sleep life.
Cognitive Ability
Grieving can cause you to experience hazy thinking as part of temporary cognitive impairment. Your mind and body are actually protecting you from experiencing too much at once, particularly when the loss of a loved one is sudden. In this state of mind, you can make snap decisions or act out in ways that are not like you. Sleep helps you restore a clear mind and act like yourself again.
Grieving doesn’t always mean you will experience insomnia or sleep deprivation though. Sometimes excessive sleeping is common as well. Every person faces their grief in different ways; however, the amount and quality of your sleep is commonly affected and is symptomatic of grief. Some people actually sleep more, where people who are facing overwhelming emotions are often reluctant to get out of bed and face the realities of everyday life. Retreating to bed can be an escape when you are working through so many exhausting emotions, but often in these cases, the quality of sleep is still low. Nightmares and dreams of your loved one can also be difficult to handle or process. When many of those grieving see their loved ones in their dreams or nightmares, it can be mostly unsettling where such dreams do not provide closure.
We even sometimes prepare for grief when someone we love is fighting cancer, which is a process that can be emotionally overwhelming and cause sleep issues as well. Thought leaders on grief are starting to recognize grief as both a process and a disease, where studies show that grieving can cause poor sleep that can become a chronic disturbance. Know when to ask for professional help in order to protect yourself and properly heal your mind, body and soul.
Bereavement is an old-fashioned term, harking back to an era when family members who lost a loved one dressed in black, literally wearing their grief for all to see.
Today, mourning a death has few rules, traditions or identifiers. But research indicates that a significant loss is deadly serious, putting the grieving at higher risk for serious health problems, and even their own premature death.
For more than a decade, Dr. Toni Miles has studied the impact of bereavement. A physician with a Ph.D. in public health, Miles is a professor of epidemiology at the University of Georgia and director of its Institute of Gerontology.
As the boomer population ages and more individuals live with grief, Miles believes the time is right to look at bereavement care as a public health issue that can buffer the negative impact of loss. Her research also identifies effective strategies to support the bereaved.
In this interview, Miles explains how bereavement affects people’s health and mortality and what we can do to better help those who are grieving.
Kevyn Burger: What toll is taken by the loss of a close family member?
Dr. Toni Miles: Critical losses are destabilizing and accumulate over time. The death of a significant loved one — by that I mean a parent, spouse, sibling or child — increases your own risk of dying.
I’m not talking about the anecdotal story of an older couple that dies within twenty-four hours of each other. I’m using a large data set of people fifty and older, studying people who report they’ve lost someone close in the last twenty-four months. At a population level, those people are two times more likely to die over the course of a lifetime than someone without that loss.
What else does the data show?
The rates for premature death are highest in the first two years after the loss. The research also shows that the younger you are when you lose someone important to you, the worse it is for your health. The elevated mortality risk for children who lose a parent goes up fivefold. In our models, losing a child, even an adult child, statistically carries a high risk of morbidity.
It sounds like time, in fact, does not heal these wounds.
That’s true. The risk never goes away; it does not return to the expected level of the general population that has not experienced such a loss. Even when you adjust for age, the risk stays higher. When we measure this at a population level, we believe that five percent of the deaths that happen in a year are attributable to a loss; by that I mean, they might not have died if they didn’t have this loss in their background.
What’s the physical toll of grief?
Bereavement is this feeling of profound loss; it’s having a giant hole in your soul. You are living with this feeling that you didn’t have before this event. Your physiology is perturbed. People gain or lose weight, their sleep is disturbed. They take up smoking again. Grief sends people to the doctor and the hospital.
And, sooner or later, everybody loses a significant loved one.
If people started turning purple with each loss, we would be able to see it in front of us. Some people are lavender, others are like an eggplant.
After studying the risks and outcomes of elevated mortality from a public health perspective, I say we are in the midst of a hidden epidemic.
What can be done to help?
We need bereavement care for the grief-stricken. We need to take care of the people around the deathbed, not just the person in it. Bereavement care is a therapeutic strategy that can build resilience. There are things you can do that are non-pharmacological that counter the negative effects of loss. (People) need permission to grieve and help processing what they’re experiencing, from professionals or from people who care.
Do we collectively do a good job caring for bereaved people?
Not at all, but we could. I want this research to influence policy. I’m looking for ways to interject bereavement care into our society. We can use this knowledge to lower that known elevated risk. For example, the literature shows us that the loss of a family member significantly increases stress hormones in pregnant women. Knowing that can be huge for practitioners. It can change how a mother-to-be is cared for.
What are other risk factors that impact the health of survivors?
A death can mean a financial loss to the household. In the statistical model, we found that people who were getting money support from the deceased and take a financial hit are more likely to get sick and die. We often overlook that.
From a practical standpoint, what can we do to help a friend or neighbor who is mourning the loss of a significant loved one?
Encourage physical activity. I say, walk the bereaved. This is something a friend or neighbor can offer after a loss. Show up and say, ‘Let’s take a stroll.’ Movement cuts the risk of negative outcomes in half in our (research) models in people over fifty. The data showed a benefit derived from any type of physical activity. Activity also decreases the instances of insomnia, and if you can sleep, you can heal.
What about the gesture of bringing food after a funeral?
A lot of comfort food is fatty and salty. Every recipe in Georgia starts with, ‘Fry a pound of bacon.’ When my bother-in-law died, I thought, ‘These people are trying to kill us.’ Don’t bring the casserole with the cream sauce. Bring a nice bowl of fresh fruit.
Any ‘don’ts’ to keep in mind when expressing sympathy?
To a person, those who are bereaved say, ‘Don’t tell me you know how I feel.’ Even if you think you do, they won’t buy it. It will only anger them.
Be prepared to listen, but not everyone wants to talk. In the movie First Man, the Neil Armstrong character lost his young daughter. Five years later, her death comes up in a group setting. It brings her back to him and he has to leave. He goes home and is looking at the moon when a friend shows up and asks, ‘Do you want to talk about it?’ Armstrong replies, ‘No, that’s why I came here.’ That moment is very illustrative. He needed his friend to just sit quietly and be a presence for him. Sometimes that’s good enough.
What do we feel when a loved one is in the very last stage of their lives? What do people who are dying feel when they realize that their time here is nearly over? That process – emotional grief is what we refer to as anticipatory grief. It is the anticipation and grief reaction to understanding that someone or yourself are about to die. Not specifically in the next few moments, but in the months to come. In this post, we discuss anticipatory grief and the grieving process.
What is Anticipatory Grief?
Anticipatory grief is the emotional response to the pending death of a loved one. It is a very powerful form of grief and occurs both in the loved ones of someone who has a terminal illness and in the person who is suffering that illness.
This is a response to the realization that that person or yourself is going to die and that the hope of being cured has diminished. Anticipatory grief is not always about the actual loss of life. It can accompany a major change in peoples lives such as having to have a limb amputated or when a woman must have a mastectomy and feels that her femininity is dying.
What Are the Signs and Symptoms of Anticipatory Grief?
There are five stages of grief and those include:
Denial – Sometimes when faced with death, we deny that the situation is as serious as it is. We cannot accept that death is a possibility or that someone who is dying will eventually die. Instead, we might push them to try harder or resent them silently for not trying harder or resent those around them for not trying harder. “If only” statements are common. If only, I had done more… If only I had taken the time… If only I had talked to the doctor…
Anger – Anger can be uncontrollable and rage-like. It can be directed at the person who is dying or at the people caring for that person – doctor, caregivers, etc. The response is after an accusation and can be violent – physical or emotional – outbursts.
Bargaining – There is the thought that you can make a deal in exchange for something more. ” I can give you more money if you give me better medication – strong chemo, etc. The idea of death is not solidified at this point. There is still the desperate clinging to hope for things that have not yet been identified or discovered – A new drug, a new procedure, a new chance.
Depression – We understand now and the regrets of what we have said, the time we have wasted, the little things that mean nothing are now a weight that pulls us downwards. For those who are about to lose a loved one, this depression may cause us to not want to see the person, or to take the blame for their loss upon ourselves. These are darker emotions.
and Acceptance – We have accepted the fact that nobody is to blame, that there is nothing left to bargain for, and that despite our sadness we or our loved one is going to die. It is a calming of the angst that we have felt. It is often a recognizable and reconciliation period we discuss forgiveness or give permission to someone we love so that they can die. It is about dignity and hope and while sad, is an uplifting from the depressed period through which we have passed. It is a coming to terms with death and the loss and sometimes it is a deeper understanding of what death is – a part of life.
Coping with Anticipatory Grief
One of the first things to understand about anticipatory grief is that it is a very normal process. You have not done anything wrong. The fact that you are grieving means that you care.
Be willing to talk with other people about what you are feeling. In Hospice, the idea is to treat the entire family because anticipatory grief is very powerful. If hospice is not available, talk to your clergy or begin to see a therapist. There are support groups that can help and many are free of charge.
Talking is a release and grief is very much like a deep pressure that we contain until we explode. Talking relieves that pressure and helps us to see grief for what it is and to recognize why we feel what we do. Talking is good for the entire family and for the patient.
It is important to acknowledge that this is a loss for everyone involved. This is not specifically about giving up the fight, but a reorganization of your options and the tools available to preserve the quality of life and the dignity of the person who is dying. It is a way to make good use of the time that is left and to focus on being good to yourself and to your loved ones.
If you are facing a terminal illness, be sure to set up a support system for the people around you. As you move closer to death it is these people who will help you to handle the pressure and the stress. It is also wise to set up a support system that cares for the people around you. Many will carry the burden of death silently so as not to burden the person who is ill with their grief. Knowing that now, enables you to build a team that cares for all of you.
Grief is a natural part of being ill and facing a terminal illness. It can be devastating and paralyzing, but by recognizing what it is and how it works empowers you to handle it.