Heidi Anderson, with her Nan and brother, has been thinking about life after death.
[O]n the 16th of August this year, my beautiful 96 year-old Nan passed away. Since then, I have rode one hell of a roller-coaster with my emotions all over the shop.
Nan and I always had a pact that if there were something on the other side, that she would come back and tell me about it.
She never believed there was anything else after you die and she would always say to me: “Once you’re dead, you’re dead. That’s it. There is nothing else.”
That is what terrifies me. The thought of “that’s it” petrifies me. I’m seriously scared of dying and for years this has given me anxiety.
I have worked with my psychologist about this fear. Dying is inevitable, but I still find it so hard to comprehend.
I’m not sure any of the sessions have helped, I still think about it a lot.
People constantly say to me: “Why stress about something you have no control of?”
Or, “You won’t know when you’re dead that you’re dead, so chill out.”
Heidi Anderson’s Nan, who passed away in August age 96.
Believe me, if I could switch it off I would but that’s easier said than done. It’s not the thought of how I die that bothers or upsets me, it’s the thought of the unknown. Not knowing what’s next.
This consumes my thoughts far too often and it’s something that I have tried to come to terms with over the past few years with no such luck.
When my Mum told me that Nan was dying and she wouldn’t recover from her fall, I flew straight to her bedside, along with all the family.
Saying goodbye to my Nan was the hardest thing I have ever had to do in my life.
Once Nan knew herself that she was dying and had accepted her fate, she called me into her room to speak. At this stage, she didn’t have much energy but she was putting all her fight into saying goodbye to people individually.
“Heidi, we all die. That’s life,” she said to me. “That’s the one thing are guaranteed in life. We’re born to die.”
Looking back, I think Nan was speaking to herself, as she too was always so afraid of death.
Over the next few days, Nan went downhill and eventually she stopped speaking and just slept.
Family came and went and said their goodbyes, but I stayed around.
I wanted to be with Nan as she exited this world. I wanted to hold her hand as she took her last breath.
Looking back, I think I also wanted to confront my fear of death. If I saw what actually happens, maybe I wouldn’t be so scared.
So I hung around the hospital like a bad smell, rarely leaving Nan’s bedside.
I played her music, told her stories and relived all our good times.
Unfortunately, by that stage she was no longer talking, but she would twitch her lips or flicker her eyes.
I swear she could hear everything, she just couldn’t respond.
In the end, I flew home to Perth. She was holding on and I felt Nan just didn’t want to die in front of any of her grandkids.
12 hours after I got home, Nan took her last breath with her three daughters at her side.
The nurses at the hospital said it was very common for people, when they’re dying, to choose who is with them.
Although I wanted so desperately to be with Nan, I felt she knew it was best that I wasn’t there.
When I arrived home in Bathurst for her funeral, I still felt that I wanted to confront my fear of death and see Nan.
Mum took me to the funeral home the morning of her farewell and I saw Nan for the first time since she passed away.
She was dead and she even looked it. No amount of makeup was hiding the fact that she was gone.
It hit me like a ton of bricks. Nan was dead and she was never coming back.
Thoughts started flooding my brain.
“Where is she? Is there something else out there? Is she with Pop? What happens? Where has she gone?”
Her body was there but that wasn’t my Nan.
My friends asked later if she looked peaceful and I found that hard to explain. She looked like she was gone and that is something I won’t ever really understand.
I’m not sure seeing my Nan in her coffin has helped my fear of dying, but it definitely gave me some kind of closure.
I am still waiting for Nan’s spirit to visit me and let me know if there is anything else out there.
I have had a couple of dreams about her and I talk to her all the time but I am yet to feel her or hear if there is life after death.
In one of the largest and most rigorous clinical investigations of psychedelic drugs to date, researchers at Johns Hopkins University and New York University have found that a single dose of psilocybin—the psychoactive compound in “magic” mushrooms—substantially diminished depression and anxiety in patients with advanced cancer.
Psychedelics were the subject of a flurry of serious medical research in the 1960s, when many scientists believed some of the mind-bending compounds held tremendous therapeutic promise for treating a number of conditions including severe mental health problems and alcohol addiction. But flamboyant Harvard psychology professor Timothy Leary—one of the top scientists involved—started aggressively promoting LSD as a consciousness expansion tool for the masses, and the youth counterculture movement answered the call in a big way. Leary lost his job and eventually became an international fugitive. Virtually all legal research on psychedelics shuddered to a halt when federal drug policies hardened in the 1970s.
The decades-long research blackout ended in 1999 when Roland Griffiths of Johns Hopkins was among the first to initiate a new series of studies on psilocybin. Griffiths has been called the grandfather of the current psychedelics research renaissance, and a 21st-century pioneer in the field—but the soft-spoken investigator is no activist or shaman/showman in the mold of Leary. He’s a scientifically cautious clinical pharmacologist and author of more than 300 studies on mood-altering substances from coffee to ketamine.
Much of Griffiths’ fascination with psychedelics stems from his own mindfulness meditation practice, which he says sparked his interest in altered states of consciousness. When he started administering psilocybin to volunteers for his research, he was stunned that more than two-thirds of the participants rated their psychedelic journey one of the most important experiences of their lives.
Griffiths believes that psychedelics are not just tools for exploring the far reaches of the human mind. He says they show remarkable potential for treating conditions ranging from drug and alcohol dependence to depression and post-traumatic stress disorder.
Clinical pharmacologist Roland Griffiths.
They may also help relieve one of humanity’s cruelest agonies: the angst that stems from facing the inevitability of death. In research conducted collaboratively by Griffiths and Stephen Ross, clinical director of the NYU Langone Center of Excellence on Addiction, 80 patients with life-threatening cancer in Baltimore and New York City were given laboratory-synthesized psilocybin in a carefully monitored setting, and in conjunction with limited psychological counseling. More than three-quarters reported significant relief from depression and anxiety—improvements that remained during a follow-up survey conducted six months after taking the compound, according to the double-blind study published December 1 in The Journal of Psychopharmacology.
“It is simply unprecedented in psychiatry that a single dose of a medicine produces these kinds of dramatic and enduring results,” Ross says. He and Griffiths acknowledge that psychedelics may never be available on the drugstore shelf. But the scientists do envision a promising future for these substances in controlled clinical use. In a wide-ranging interview, Griffiths told Scientific American about the cancer study and his other work with psychedelics—a field that he says could eventually contribute to helping ensure our survival as a species.
[An edited transcript of the interview follows.]
What were your concerns going into the cancer study?
The volunteers came to us often highly stressed and demoralized by their illness and the often-grueling medical treatment. I felt very cautious at first, wondering if this might not re-wound people dealing with the painful questions of death and dying. How do we know that this kind of experience with this disorienting compound wouldn’t exacerbate that? It turns out that it doesn’t. It does just the opposite. The experience appears to be deeply meaningful spiritually and personally, and very healing in the context of people’s understanding of their illness and how they manage that going forward.
Could you describe your procedure?
We spent at least eight hours talking to people about their cancer, their anxiety, their concerns and so on to develop good rapport with them before the trial. During the sessions there was no specific psychological intervention—we were just inviting people to lie on the couch and explore their own inner experience.
What did your research subjects tell you about that experience?
There is something about the core of this experience that opens people up to the great mystery of what it is that we don’t know. It is not that everybody comes out of it and says, ‘Oh, now I believe in life after death.’ That needn’t be the case at all. But the psilocybin experience enables a sense of deeper meaning, and an understanding that in the largest frame everything is fine and that there is nothing to be fearful of. There is a buoyancy that comes of that which is quite remarkable. To see people who are so beaten down by this illness, and they start actually providing reassurance to the people who love them most, telling them ‘it is all okay and there is no need to worry’— when a dying person can provide that type of clarity for their caretakers, even we researchers are left with a sense of wonder.
Was this positive result universal?
We found that the response was dose-specific. The larger dose created a much larger response than the lower dose. We also found that the occurrence of mystical-type experiences is positively correlated with positive outcomes: Those who underwent them were more likely to have enduring, large-magnitude changes in depression and anxiety.
Did any of your volunteers experience difficulties?
There are potential risks associated with these compounds. We can protect against a lot of those risks, it seems, through the screening and preparation procedure in our medical setting. About 30 percent of our people reported some fear or discomfort arising sometime during the experience. If individuals are anxious, then we might say a few words, or hold their hand. It is really just grounding them in consensual reality, reminding them that they have taken psilocybin, that everything is going to be alright. Very often these short-lived experiences of psychological challenge can be cathartic and serve as doorways into personal meaning and transcendence—but not always.
Where do you go from here?
The Heffter Research Institute, which funded our study, has just opened a dialogue with the FDA (Food and Drug Administration) about initiating a phase 3 investigation. A phase 3 clinical trial is the gold standard for determining whether something is clinically efficacious and meets the standards that are necessary for it to be released as a pharmaceutical. Approval would be under very narrow and restrictive conditions initially. The drug might be controlled by a central pharmacy, which sends it to clinics that are authorized to administer psilocybin in this therapeutic context. So this is not writing a prescription and taking it home. The analogy would be more like an anesthetic being dispensed and managed by an anesthesiologist.
You are also currently conducting research on psilocybin and smoking.
We are using psilocybin in conjunction with cognitive behavioral therapy with cigarette smokers to see if these deeply meaningful experiences that can happen with psilocybin can be linked with the intention and commitment to quit smoking, among people who have failed repeatedly to do so. Earlier we ran an uncontrolled pilot study on that in 50 volunteers, in which we had 80 percent abstinence rates at six months. Now we are doing a controlled clinical trial in that population.
How do you account for your remarkable initial results?
People who have taken psilocybin appear to have more confidence in their ability to change their own behavior and to manage their addictions. Prior to this experience, quite often the individual feels that they have no freedom relative to their addiction, that they are hooked and they don’t have the capacity to change. But after an experience of this sort—which is like backing up and seeing the larger picture—they begin to ask themselves ‘Why would I think that I couldn’t stop cigarette smoking? Why would I think that this craving is so compelling that I have to give in to it?’ When the psilocybin is coupled with cognitive behavioral therapy, which is giving smokers tools and a framework to work on this, it appears to be very helpful.
You are also working with meditation practitioners. Are they having similar experiences?
We have done an unpublished study with beginning meditators. We found that psilocybin potentiates their engagement with their spiritual practice, and it appears to boost dispositional characteristics like gratitude, compassion, altruism, sensitivity to others and forgiveness. We were interested in whether the psilocybin used in conjunction with meditation could create sustained changes in people that were of social value. And that appears to be the case.
So it is actually changing personality?
Yes. That is really interesting because personality is considered to be a fixed characteristic; it is generally thought to be locked down in an individual by their early twenties. And yet here we are seeing significant increases in their “openness” and other pro-social dimensions of personality, which are also correlated with creativity, so this is truly surprising.
Do we know what is actually happening in the brain?
We are doing neuro-imaging studies. Dr. Robin Carhart-Harris’s group at Imperial College in London is also doing neuro-imaging studies. So it is an area of very active investigation. The effects are perhaps explained, at least initially, by changes in something [in the brain] called “the default mode network,” which is involved in self-referential processing [and in sustaining our sense of ego]. It turns out that this network is hyperactive in depression. Interestingly, in meditation it becomes quiescent, and also with psilocybin it becomes quiescent. This may correlate with the experience of clarity of coming into the present moment.
That is perhaps an explanation of the acute effects, but the enduring effects are much less clear, and I don’t think that we have a good handle on that at all. Undoubtedly it is going to be much more complex than just the default mode network, because of the vast interconnectedness of brain function.
What are the practical implications of this kind of neurological and therapeutic knowledge of psychedelics?
Ultimately it is not really about psychedelics. Science is going to take it beyond psychedelics when we start understanding the brain mechanisms underlying this and begin harnessing these for the benefit of humankind.
The core mystical experience is one of the interconnectedness of all people and things, the awareness that we are all in this together. It is precisely the lack of this sense of mutual caretaking that puts our species at risk right now, with climate change and the development of weaponry that can destroy life on the planet. So the answer is not that everybody needs to take psychedelics. It is to understand what mechanisms maximize these kinds of experiences, and to learn how to harness them so that we don’t end up annihilating ourselves.
Keely Dowton (right) and her mother who died last year.
[D]uring this time of the year death appears in a guise of make up, costumes and candied treats. Often portrayed by colourful eccentric images, celebrations such as Halloween and the Day of the Dead were traditionally about remembering the dead and the memories of lost loved ones.
But talking about death is not easy if you’re British. When broached, the topic seems to make people feel uncomfortable and can even be judged as a morbid conversation subject. But death is part and parcel of what it means to live. We talk about having the ‘time of our lives’ or ‘living life to the full’ but often try and forget what inevitably follows.
We wanted to talk more about death so asked readers for their experiences of grieving and what death means to them. Here’s what some of them said.
‘Grief is so overpowering – it consumes you’
Having lost my mother 17 months ago the experience of losing her is still very raw for me. Mum went to her doctor with a minor stomach upset and died four weeks later with an aggressive bowel tumour. She had no previous symptoms and wasn’t even unwell. It came as a complete shock with total devastation to her family.
Grief is so overpowering – it consumes you. First the numbness and autopilot mode then the heaviness of despair, then the oceans of tears, then the questions of the pointless, futility of life. Then anger, then deep despair, then numbness and repeat. Repeat. 17 months on and I still question all of it; but I cope by leaning on my loved ones and I cope by using my mum’s strength to spur me on. Ironically, she is the one that gets me out of bed in the mornings.
My life has changed drastically. After mum died I resigned from my job, married my partner of 22 years (we married on mum’s birthday as a gift/gesture to her), I got a dog and am now planning a move with my husband to Sri Lanka for a few years. I see my life in two parts; my old life with mum and my new life; one I didn’t want or choose but one that I’m trying to embrace. I try to live my life as my mum wanted; with gusto and enjoying the little things. I’m trying at least.
Keely Dowton, 44-year-old teacher living in Essex
‘I said ‘Good morning’ to a photo of him each day’
I lost my father seven years ago. It was totally unexpected and at the time I could not deal with it. I said ‘Good morning’ to a photo of him each day as I did in person before. I threw myself into planning the funeral, keeping busy meant not thinking about what had happened.
Just after he passed away, I noticed a robin that would watch me when I was gardening. The robin visited the garden most days and would look towards the house. There are some people who think that symbolises that a loved one who has passed is okay. That brought me some comfort even if I don’t completely believe it. I like seeing robins in the garden, even when they are being fiercely territorial. Seeing them is associated with my dad now. I talked about my dad in the present tense for a long time, maybe a year after he had died. Even now it feels incorrect to talk about him in the past because he lives on in my heart and mind. He always will. That’s love.
Anonymous, 39-year-old teacher living in the Midlands
Joanne and her husband
‘Dealing with death is relatively easy compared to getting on with life without them’
Death means my husband. It is something I’m familiar with now as I have lived through his. I lay with his dead body for half an hour and felt peace. Other people’s death isn’t scary for me anymore but mine is as I fear for my children.
I think it’s more difficult to talk about death if you haven’t had any personal experience of it. A lot of the time it’s very clinical, with the funeral director taking the body away fairly swiftly. There’s not often the chance to spend time with the dead and say goodbye. It’s almost frowned upon. I took some pictures of my husband dead; before and after he was embalmed. It doesn’t feel right sharing that fact with people as I’m worried they’ll think it weird. It didn’t feel weird to me.
Even though my husband suffered with all the indignities of cancer I believe in the end he had a good death. He’d put his affairs in order, planned his funeral, said goodbye to loved ones and ultimately died in my arms. If if wasn’t for the fact that he was only 48 it would have been perfect.
Dealing with the death was relatively easy compared to getting on with life without them. That’s the hardest bit. When the funeral flowers and cards stop coming. When friends no longer bring cooked dishes round. That’s when the shit hits the fan and you see the size of the hole they have left.
Joanne Baker, 47-year-old full-time parent of two children living in Guiseley
‘I gave her a bag of popping corn – she was being cremated and would have loved that!’
The death of my mother last year was like watching a transition from pain to peace. I miss her so much. The horror of the last 12 hours in A&E and hospital side ward as she slipped into unconsciousness will never leave my memory. The nurses were kind but no one could save her from her journey. As she took her last breaths, I told her to go find her mum now and that we would be OK. It was a privilege to share those moments but terrifying.
I’m a Christian. My mother pre-paid for a cardboard coffin, and at her request we pasted all the grandchildren’s art work on it. Her lid was open and we spent an hour talking to her. Her spirit felt close. I placed momentoes in her coffin and a bag of popping corn just for fun in her hand. She was being cremated and would have loved that!
Jayne Gale, 47-year-old nurse
‘I did not cry at the funeral, nor did I go to view his body’
I experienced my dad’s death at the tender age of 13, in June 2003. I did not cry at the funeral, nor did I go to view his body. I couldn’t believe he was gone for good. Many times I dreamt of bumping into him on the street. I thought he would come back, even though I knew and understood that he wouldn’t.
I think most people find it hard to talk about death either due to a trauma or the death of a loved one, and in many African customs it is taboo to do so. Though it’s been 13 years since my dad left I still weep as if he just died. He was my hero. I have been praying over it, and God has helped me to accept the reality, and to stop living in denial.
Grace, 26-year-old living in Nairobi
Mourners attend a vigil for bus driver Manmeet Alisher at a Sikh temple in Brisbane, after he was burned alive when an incendiary device was allegedly thrown at him while he was letting passengers on at Moorooka
‘There is nothing to fear about death’
I lost a little boy who was just two months old – he suddenly passed away one night unexpectedly. I did not understand how this could happen to me – not even as a punishment because I felt I had never done anything that would have deserved such a chastisement.
This was when I started to try to find an answer, so I began reading about what happened after death, the meaning of life and death, why we are here on earth and so on. I got the answer after 30 years of research, so I know now why this happened to me. To me, death means to continue to live in a different form in another dimension where I will be able to meet all my dear ones who died before me and most importantly review all my past life on earth. I will then know if and how I have progressed spiritually. This will be done without judgment, just with love. Then, I will examine and decide what still has to be improved and go back to earth for another experience.
In 2012 my mother died at the age of 84. She suffered a lot and wished she could die as soon as possible “waiting for the angels to take her”. One day she had an accident at home while cooking – she was burnt and taken to hospital where she died two months later. At the very minute she died, I felt filled with an unutterable sensation of happiness which I couldn’t explain at first and I understood when I was told the precise time when she died. I was so happy that she had been freed at last. My sisters got depressed and didn’t understand my reaction at first, but I told them how I felt and they agreed that it was the best way to deal with our mother’s death.
I hope there will be more records similar to mine, so that people grow aware that there is nothing to fear about death – no judgment, no hell, no punishment – only love exists.
Jean Louis, 65-year-old retired teacher living in France
‘Those who talk openly and honestly about death tend to have a more peaceful, meaninful time at the end of their life’
Popular media images of death and dying often portray an image of inevitable suffering, as does frequent media coverage highlighting the inadequacies of health and social services in providing good end of life care and support. As a result, many people live in fear of death and the dying process and ultimately do not have the death they would have preferred.
Problematic issues including misconceptions, unspoken anxiety, lack of control, or the loved ones of a dying person perceiving the dying process as a ‘bad death’ can all contribute towards problematic grief. My own observations of dying people and bereaved relatives are that those who have talked openly and honestly about death and dying – and who have planned for what they would like to happen when the time comes – tend to have a more peaceful, meaningful time at the end of their life.
Katie Shepherd, 43-year-old clinical nurse specialist in palliative care, and permaculture designer living in Spain and Yorkshire
A skull on a turntable.
‘I dealt with the deaths of those close to me quite badly. It’s why I’m an undertaker’
Death has shaped my entire life, literally. I became an undertaker, something for which you need no professional qualifications almost 17 years ago after seeing Nicholas Albery of The Natural Death Centre talk about a different way of approaching funerals, environmentally, socially and religiously. I had a welter of family deaths as a child, most of whose funerals I didn’t go to. Now we do the opposite, encouraging as much family involvement as possible.
It is entirely understandable that people find it difficult to talk about death. The implications of our own extinction and that of the Earth’s are huge, particularly now we are at a stage when even the planet may die. I dealt with the deaths of those close to me quite badly. It’s why I’m an undertaker – do what I say, not what I do.
My father’s death two years ago was sudden and unexpected. The family gathered, and we supported one another. Tears, yes, but plenty of loving laughter – he had an offbeat personality in some ways with a great sense of humour, even around death: he’d always said (in jest) that when he goes he wanted to be stuffed and sat in a chair so he could be glowering at people!
Of course there is the awful reality of his loss in all our lives, the desperate sadness that he’s not here in the physical. He genuinely hadn’t an enemy in the world, and family, friends and colleagues past and present, travelled from far and wide to be at his funeral.
I know that he’s still present though, with countless confirmations of that, so we still go on walks together (a shared love of nature) and we ‘chat’ daily. It’s the next best thing to being in the same physical universe.
Angela, 55-year-old artist and writer living in Ireland
‘It is far easier to grieve among family and friends’
My father died while I was working in Saudi Arabia in the 1980s. My brother sent a telegram, but my employers (who had my passport in a safe) did not pass the telegram to me. I found out a few weeks later via a letter from my mother which started from the premise that I knew already. From this experience I learned that it is far easier to grieve and move on if you do it among family and friends.
Dying is taboo among health and care professionals who sometimes prioritise medical initiatives over individuals and families
Don’t Leave Me Now, a play about early onset dementia, was performed at St Gemma’s hospice in Leeds to an audience of healthcare professionals.
[S]eth Goodburn seemed fit and well until two weeks before he was diagnosed with pancreatic cancer. He died just 33 days after diagnosis, spending much of that short time in hospital. In the emotional whirlwind of coping with the poor prognosis his wife, Lesley, felt their hopes for Seth’s end-of-life care were sidelined by medical professionals trying to do their job.
“The NHS focuses on the medicine and trying to fix people even when that’s not possible,” she says. “A lot of the conversations and decisions that we might have made were overshadowed by dealing with what was the next medical treatment and intervention.”
There is an ongoing conversation in the medical profession about how to care for terminally ill patients, given that the profession’s instinct is to preserve life. The issue is just one of many being address by Brian Daniels, a playwright commissioned by the National Council for Palliative Care (NCPC) to tell stories such as Goodburn’s through plays, and help educate healthcare professionals about patients and families’ experiences of end-of-life care.
Homeward Bound, a play based on a series of letters Lesley Goodburn wrote, in the months after her husband’s death, to medical professionals involved in his care, launched NCPC’s national conference this year to an audience of 300 healthcare workers.
In addition, Daniels’ plays on early onset dementia and palliative care for those with disabilities, have been performed in hospitals, hospices, care homes and to general audiences across the country. Daniels says: “[They] take people out of their professional role for a minute to look at the family and human side of the people they’re dealing with.”
For Goodburn, that human aspect is key. She could not fault the professionalism of those involved in caring for her husband, but says poor communication could leave the couple feeling worse. “There were just so many things where people weren’t cruel or unkind or deliberately unthinking, but just didn’t really think about what it was like to be me and Seth. He went from being well and living a normal life to suddenly being told that he was dying.” She says, for example, a physiotherapist asked Seth to march on the spot as part of an assessment to see if he was able to go home, as he had previously wished, seemingly unaware that his condition had deteriorated and he was dying.
An actor in Don’t Leave Me Now.
Claire Henry, chief executive of the NCPC, says plays such as Homeward Bound are designed to encourage medical professionals to reflect on the people going through this traumatic process. “We obviously work very closely with people who have experience and they tell us their stories. Some are good, some not so good. Healthcare professionals don’t go to work to do a bad job, but sometimes they don’t think of things that affect people in a broader sense.”
What impact does a play have that a lecture, for instance, cannot? Don’t Leave Me Now, another play by Daniels, about early onset dementia, was performed at St Gemma’s hospice in Leeds to an audience including nurses, housekeeping staff and workers from other local hospices. Dr Mike Stockton, its director of medicine and consultant in palliative medicine, says the play enabled them to see some of families’ and patients’ challenges through a different lens. “It’s sometimes hard to have a full understanding … of what people may be going through and the reasons behind their actions or the emotional challenges, adjustments or the resilience that people need.”
Lynn Cawley agrees. There was barely a dry eye at a performance at Morley Arts Festival in October of Bounce Back Boy, the powerful dramatisation of her adopted son, Josh’s, story. Josh was severely disabled following a serious head injury as a baby, and later adopted by Cawley. Despite pioneering medical treatment throughout Josh’s life, Cawley says he was denied admission as an inpatient to a local hospice because his needs were too complex, and died a difficult death at home. She is fighting to end what she describes as end of life discrimination against those with disabilities.
Cawley thinks a play is an effective way of communicating that message, and for getting people to think about palliative care more broadly. She says: “When it’s someone’s real life story, people put themselves in it [and] they might think of a patient that they know. We hope that it will change policy but also people’s attitudes.”
For Stockton, working in a hospice, the wider issue of how treatment is balanced with patient comfort is a daily consideration. He says the two can often be done together: “It is about having early, thorough, open, honest, transparent conversations with people about what they want.”
For Cawley, as a carer and mother who went through the palliative process, those open conversations about dying are key. “We even find it hard to say the word,” she says. “When we’re watching Casualty on a Saturday night and they’re trying to tell a relative that somebody is dying, but they won’t say the word dying or death, we’re just like – say death!”
Traditionally, the “Day of the Dead” is a time when family and friends gather to remember friends and family members who have died. But it’s also a perfect time to think about your own death – if you dare.
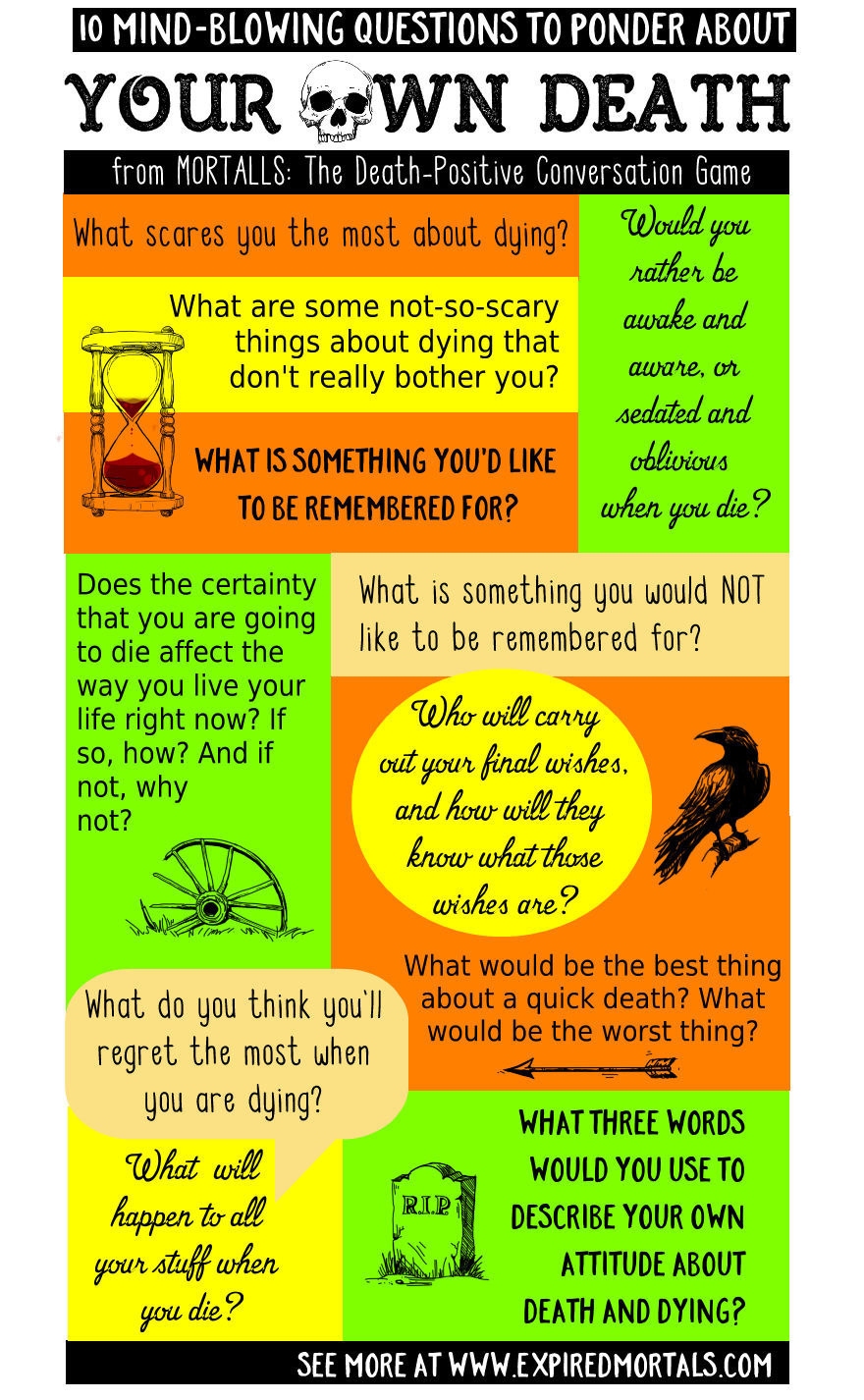
Care to face your own mortality? Here are 10 Mind-Blowing questions to ponder about your own death.
Most people won’t go there because it’s either too scary, too painful, or we just pretend it will never happen to us. But ready or not, there’s a 100% certainty death will eventually get up close and personal with every one of us. Here, from MORTALLS – The Death-Positive Conversation Game, are 10 mind-blowing but worthwhile questions to ponder about your own death… if you are willing to do so:
What scares you the most about dying?
What are some not-so-scary things about dying that don’t really bother you?
When you die, would you rather be awake and aware, or sedated and oblivious? Why?
What would be the best thing about a quick death? The worst thing?
What do you think you will regret the most when you are dying?
What is something you want to be remembered for?
What is something you do not want to be remembered for?
Who will carry out your final wishes when you die? How will they know what those wishes are?
Does the certainty that you are going to die affect the way you live your life right now? If so, how? And if not, why not?
What three words would you use to describe your own attitude about death and dying?
[M]y mother once told me a very sweet story about how I, as a toddler, handled my grandmother’s death. After the funeral, my mom asked me if I knew where Grandma had gone. I told her, as matter-of-factly as a 2-year-old could, that she was in a garden, surrounded by daisies (her favorite flower).
Even at such a young age, I’d developed a sense for the appropriate kinds of euphemisms for death — and I knew that sharing them would bring comfort to my mom. But that didn’t change the fact that my grandmother was dead — like, she was dead and buried and there weren’t any daisies in there with her, though I didn’t quite comprehend that yet.
It was actually much later, when I was 17 and attending another relative’s funeral, that the reality of death truly hit me. My uncle had died after being diagnosed with cancer way too late, and his passing was a real shock to the family. The memorial service was at his house in Virginia and the choir from his church sang some upbeat hymn about going where you were always meant to go. Listening to that, and knowing how he died, I thought, This must be a joke.
I bristled at the idea that dead people were anything other than dead. On one hand, I found it naive to think about death in such rosy terms, inwardly rolling my eyes at those who did. On the other, I believed that death was supposed to be frightening, and by rejecting the idea of an afterlife or deliverance I all but cemented that fear in my mind.
In other words, I gave myself two options: I could scoff at death or fear it wholeheartedly. Multitasker that I am, I decided I could do both.
I found myself viewing death as two very different (and equally problematic) beasts — a hulking, dark thing that we only discuss in whispers and a lurking shadow that simply absorbs the rueful jokes we hurl at it.
Neither of these images get death quite right, but there I remained, with death constantly on the brain. For fear of seeming morbid or like a total downer, I kept most of my thoughts about death and dying to myself. Yet, a question nagged at me — Was I alone in feeling this way?
The urgency of that question has only increased over the course of this year. That’s why, this fall, R29 conducted an informal survey about death, to which more than 300 people, mostly millennial women, responded.
Nearly half of all respondents said they learned about death by the time they were 5 years old, citing such sources as dead pets, 9/11, Mufasa, and, like myself, the death of a loved one. They grew up believing that the deceased ended up in God’s arms, went to heaven, took on another earthly form, or were left to fade into nothingness.
Regardless of their foundational experiences with death, most people still think about it — and in a small, strange way, I found that comforting. “Ever since turning 30, I think about death every couple hours,” one person wrote. “It’s almost the only thing I think about,” wrote another.
The thing is, most people don’t simply fear death or laugh at it. Instead, people describe how they use death to interrogate their religious beliefs, take stock of their health, and motivate themselves to spend time with distant, elderly loved ones.
Many said they hope they’ll die quickly and at an advanced age. Some alluded to suicide attempts (If you’re experiencing suicidal thoughts, please call the National Suicide Prevention Lifeline at 1-800-273-TALK (8255) or the Suicide Crisis Line at 1-800-784-2433.) or an unshakable conviction that they’ll die young. One person qualified their acceptance of death like this: “I deeply fear dying, but don’t fear death.” In total, 71% admitted to having imagined their own death.
I’ve been turning that number, 71%, over and over in mind my since first seeing it. For one thing, it answers my question: I’m anything but not alone in constantly thinking about death. It also makes me regret that we didn’t ask how many of them ever told anyone about imagining their own death. I wonder how much higher or lower that number would be.
Here’s what I want to tell everyone who thinks about death on the daily: You’re not morbid. You’re human. And you don’t have to keep those thoughts to yourself. After all, chances are, most other people are thinking them, too — and death is neither a beast nor a shadow.
It’s something that informs and gives meaning to how we live. As one person put it: “The more I learn about death, the less I fear it.”
Welcome to Death Week, in which we’ll attempt to unpack our feelings, fears, and hang-ups about death, dying, and mourning. We’ll do our best to leave no gravestone unturned.
Never mind assisted-dying, our health care system needs to change the way it deals with the natural end of life
By Mohamed Dhanani
Mohamed Dhanani, left, with his father-in-law Ijaz Ahmad at a wedding last year. “The eight different doctors who treated my father-in-law all had different ideas about what (his wishes not to be life support) meant, and how involved the family should be in making treatment decisions,” writes Mohamed Dhanani. “This inconsistency — the waiting, the arguing, the feeling of powerlessness — was our family’s worst experience with a health care system of which we are so often proud.”
I’ve spent much of my career in the health care field, but it took a very personal experience to drive home just how poorly prepared health care providers are to help us through the one certain life-experience that awaits us all: death.
It happened in a hospital in southern Ontario. My father-in-law, Ijaz Ahmad, who lived with insulin-dependent diabetes for 35 years, went into the hospital for a partial foot amputation due to a bone infection.
Prior to surgery, a routine diagnostic test was performed requiring dye to be inserted into his bloodstream. After the surgery, the dye put him into kidney failure while it was being metabolized. Within a day of the surgery all of his organs started to fail and he was put on life support for what we were told would be two to three days so his organs could rest and strengthen — after which, we were told, “the doctors would bring him back.”
He spent the next 18 days on life support. And what became clear over that long 18-day ordeal is that what had clearly become the end of his life would have been unnecessarily prolonged depending on which of the eight doctors we interacted with was treating him that day.
Like so many families who have had the difficult but essential conversation with an aging parent around their end-of-life wishes, we had spoken with him about his wishes. He was clear he did not want to be on life support.
The eight doctors who treated my father-in-law all had different ideas about what those wishes meant, and how involved the family should be in making treatment decisions. This inconsistency — the waiting, the arguing, the feeling of powerlessness — was our family’s worst experience with a health care system of which we are so often proud.
Some of the doctors acknowledged his wishes but said life support was an essential part of the treatment plan; it was just a temporary measure to aid in his recovery. Others made very little effort to consult with us, and another outright refused! Another doctor assured us he would “bounce back,” though nurses told us this was increasingly unlikely and that the doctor was prone to sugar-coating discussions with families.
Because of this inconsistency, different members of my family were hearing different things — and that made it even more difficult for us to make a decision we all felt comfortable with. Finally, I pulled aside the latest doctor treating my father-in-law and asked him for an absolutely frank and direct discussion. Only then were we able to make an informed decision that respected my father-in-law’s wishes and provided as much comfort as possible to our family.
On my father-in-law’s 18th day on life support, and on what was to be the final day of his life, a new doctor was treating him. This doctor had trained and practiced in the U.K., and had only recently started to work in Ontario. His European training and experience gave him a different perspective on end-of-life care, and one for which we were grateful.
In Europe, the societal conversation on end-of-life care is more advanced than in Canada — they have grappled publicly with these essential issues of decision-making in health care for many years, and physicians have therefore become more comfortable discussing end-of-life decisions with their patients and families.
Not only is this an essential conversation we need to normalize as families and as a society, it is something our health care system must take on as an essential part of its work. All doctors must be trained to discuss end-of-life care in a direct and compassionate way with patients and their families. This will only become more important as people live longer, and as their health issues become more complex as they reach the end of their lives.
Over the last few years, Canadians have engaged in an impassioned debate on assisted death, a debate that culminated in landmark — and controversial — legislation in Parliament. But assisted death is just a small part of the issue.
As my family’s experience illustrates, end-of-life care and the difficult discussions surrounding that care are too inconsistent — inconsistent between institutions and inconsistent between doctors within a single hospital. It is something we can and must fix.
Surrounded by family and friends my father-in-law peacefully passed away within minutes of removing the breathing tube. He was 66 years old. May his soul rest in eternal peace.