Much of the conversation surrounding end-of-life care has to do with the elderly making decisions based on how they’d like to spend their final days. For them, it’s more about comfort and less about prolonging life, but when children are thrown into the equation — things become a lot more challenging for physicians, patients and parents.
Published in JAMA Oncology, a new report concluded that 68% of young adult cancer patients receive medically intensive care at the end of life. The study’s authors defined “medically intensive care” as “chemotherapy within the last two weeks of life; more than one emergency room visit in the last month of life; intensive care unit care in the last month of life; or hospitalization in the last month of life.”
“This kind of care should be used when it supports the values and goals of patients near the end of life,” said Dr. Jennifer Mack, a pediatric oncologist with the Dana-Farber/Boston Children’s Cancer and Blood Disorders Center. “However, this type of care is often used to prolong life, sometimes at the cost of quality of life, and so it may not fit the goals of all patients, especially those who prioritize quality of life near death.”
Researchers examined the Kaiser Permanente Southern California cancer registry data and electronic health records for 663 adolescents and young adults who died between the ages of 15 and 39. The study analyzed individuals with either stage 1 to stage 3 cancer and evidence of cancer recurrence or stage 4 cancer at diagnosis. The most common cancer diagnosis was gastrointestinal cancer.
The breakdown of the study’s findings is as follows: 11% of patients received chemotherapy within 14 days of death; in the last 30 days of life, 22% of patients were admitted to the intensive care unit; 22 % of patients had more than one emergency department visit; and 62% of patients were hospitalized.
“Older patients who know they are dying often do not want to receive such care, but we do not know if young people feel the same way,” Mack said. “Some may want to receive aggressive measures in hopes of living as long as possible. Physicians who care for adolescent and young adult cancer patients should ensure that young people understand what is ahead, especially if cure is not possible.”
She added that “physicians should open conversations about what is most important to young patients as they approach the end of their lives, so that care supports their wishes.”
Many times patients (and their surrogates) are ill-informed of a physician’s prognosis. To bring everybody up to speed, clinicians can assess care goals with patients. “Understanding what is important to young people at the end of life should be a research priority and a priority in clinical care,” Mack said.
“We should be asking patients what matters most to them as they face the end of their lives, what they are hoping for, and what they are worried about,” she said. “With this information, we can offer care that best fits with the values of individual patients.”
Sesame Street was talking about grief before it was cool. Okay, so talking about death and grief still may not be cool (wait, do people even say “cool” anymore? Am I showing my age?). Let’s just say this: Sesame Street was tackling this topic long before the internet was full of tools and activities for supporting grieving kids. As early as 1983 they were helping kids understand death and grief. 30 years later they are still at it, better than ever.
Then
The first time Sesame Street really tackled death was when Mr. Hooper died in an episode that aired on Thanksgiving Day in 1983. When Will Lee, the actor who played Mr. Hooper, died of a heart attack there were many ways that Sesame Street could have handled it. Rather than shying away from the topic of death and grief, Sesame Street used this as an opportunity to do what they do best – teach. In the “Farewell, Mr. Hooper” episode, Sesame Street used Big Bird to help kids understand death and grief.
Now
In 2010 Sesame Street and Sesame Workshop received grants through a number of defense organizations and Walmart to put together resources for children on grief and loss. Launched with a great TV special, they put together an incredible combination of resources for grieving kids and adults supporting those kids. Many of these resources are available for free viewing and download. Check out a preview of the video here of the special done with Katie Couric, Elmo, and the families of several children who have experienced losses:
Or check out the whole video by going to the PBS website HERE!:
Over the years Sesame Street has kept up this trend of tackling tough topics head on, to help kids in times where they may feel unsafe, unsure, scared or confused. After 9/11 Sesame Street helped kids with fires and emergencies in an episode on a fire at Hooper’s Store.
After Hurricane Katrina Sesame Street tackled this topic through a series of episodes about a hurricane on Sesame Street.
Love Never Dies
In 2004, 21 years after Mr. Hooper’s death on the show, Grover takes Elmo on a walk (cab ride) down memory lane. At the very start of this journey Elmo learned about Mr. Hooper and how Hooper’s Store got his name.
To this day Mr. Hooper’s picture still hangs above Big Bird’s nest and can be seen in the hurricane episodes. Thanks Sesame Street, for facing this tough topic head on. And thanks for reminding kids (and all of us) that those we love and lose remain part of us, even 30 years later.
A simple memorial stone serves as the only visible marker for this shaded gravesite.
There is nothing unusual about these three girls. They are sisters. They have eyes and ears and they will remember this part of their lives forever. Taylor Ann, 9, is the oldest, and determined to speak for the others, even when it gets her in trouble. She is a smiley redhead with freckles and talks without punctuation or taking breath.
Tori is the second-oldest at 7. She is exactingly articulate, pronouncing each syllable in “e-ver-y-thing.” She has light brown hair and a slight lisp, evidence that she is growing as she speaks, her baby teeth falling out and her adult teeth growing in. Her voice is perfectly childish and curious.
Texie, 4, is the baby sister, but not the youngest sibling. That title goes to the girls’ 2-year-old brother, Junior. Texie’s placement on the second-to-bottom sibling rung sets her just high enough to grab her older sisters’ attention, but she is still something of a baby when it comes to conversation. Even so, her sporadic observations are often quite sharp. Of the three girls, Texie has the most recognizable voice when they’re all talking at once. It’s a soft garble she uses in hiccup-like bursts to coo to her stuffed animal or scream “Caaaoooolllerr the feaddderrrs!” at the ruffled bird in her coloring book. She has baby-blue eyes and platinum-blond hair, and she makes her sisters laugh.
The sound of the three of them speaking at once is not unusual. Tori and Taylor Ann bicker over the details of a story about a kitten while Texie boks like a chicken. When I ask about their oldest brother, L.J., Taylor Ann quickly gives an answer she thinks will satisfy me, and then goes back to talking about her cat. “No,” I say, clarifying my question. “How long were you with him at your house after he actually died?”
“Oh, you mean like right after he died?” The other two are quiet now. “Um, just a night. Yeah, just one night.” The distinction is meaningful because, as Taylor Ann had told me earlier, the sisters were with L.J. for a whole year after they knew he was going to die. I look at the younger girls and they’re not interested in talking about it. We’ve talked about it enough over the last three months. Every time they visit Eloise Woods, the natural-burial park where their brother is buried and where I work, they reveal a new angle of their experience of his death. Today’s angle is that they don’t feel like talking about it.
“Let’s go see L.J.,” Tori says.
“Yeah!” the other girls shriek.
We leave the coloring books on the small table between the two sheds where we always meet and walk down Cardinal Trail to visit his grave.
I was wearing hiking boots and jeans with a bloodstain on one of the belt loops when I caught the eye of the lady at the gas station.
“Going to the beach?” she asked coyly.
“No,” I said, giggling. “A cemetery.”
“Ooooooh,” she gasped, her interest piqued.
I didn’t have time to get flirty about death. I swiped my card and rushed back to my car. Just broaching the subject of what I do often turns into a lengthy discussion about the complicated politics and emotions surrounding natural burial. It’s imperative that I engage in these discussions, and most of the time I do. Word of mouth is one of the few ways people learn that they can in fact bury people in Texas without embalming, without a vault, without even a casket. They can even bury on their own land if they meet the requirements of their county and aren ’t concerned with complicating resale of the property. But such conversations are rarely brief, and I had to get to the Woods.
We weren’t sure what time the family would be arriving with L.J., the 11-year-old who had died the night before. Specifics weren’t part of the deal with his family. Though we’d known for close to a year that they would have a home funeral followed by a natural burial, we knew little else. Even the boy’s condition—why he was terminal—was discussed only vaguely by the family. All we knew was that he was in a wheelchair and that he didn’t have long to live.
Home funerals usually lead to natural burials, but not always. Most of our families employ conventional funeral homes, hold a service in a chapel and transport the body to us in the funeral home’s vehicle. We have good relationships with many funeral homes in Austin, even though we can tell their employees feel out of place when their shiny loafers step onto our roads, mulched to prevent erosion. They usually give us a couple of days’ notice before they arrive. The night L.J. died, Ellen MacDonald, my boss, the owner of Eloise Woods, emailed me at 1 a.m. telling me to show up the next morning at 8.
L.J.’s family decorates his casket in preparation for burial.
Every time I drive to Eloise Woods, the sun strobes on my left cheek as it passes between houses and trees. It’s a bright nuisance, just beyond the reach of my visor. I drive along Austin’s eastern edge, and once I’m past the airport and under the toll road, it’s a straight shot to the burial park. I listen to music at a loud volume, usually a certain Warren Zevon live album. I roll down my windows and daydream the rest of the way to the cemetery.
When I park at the Woods 25 minutes later, I remember that I’ve forgotten my hat and will be feeling the full heat of a June day. I complain about it to Ellen as I walk from my car. “I hardly slept last night,” she responds. “I just figured I’d get out here as early as I could to get it set up. The grave still needs to be deeper because I guess they’re bringing him in a casket now.” Under Texas law, a bare body, or one in a permeable encasement such as a shroud, must be buried at least 24 inches deep. An impermeable case, such as a casket, must be covered by at least 18 inches of earth. The first few feet of topsoil is where the most aggressive organic activity takes place, turning whatever has been buried into plant food. We had dug 2.5 feet deep, enough that L.J. in a shroud would be covered with 24 inches of soil. But a family member had offered to build a casket at the last minute, and now we needed to dig at least another foot to ensure that a full 18 inches of soil would cover his little box.
It’s about 50-50 at the Woods when it comes to shrouds vs. caskets. Only one person has been buried without any covering at all—an infant from a Hindu family. Cremation is a custom in that religion, a manner of releasing and purifying the soul, but children are considered already enlightened, and so natural burial with nothing between the body and the earth is traditional. Ellen told me she had laid rose petals on the soil before the baby was placed in the grave, a gesture in line with why someone had offered to construct a casket for L.J. Burying a child in raw dirt isn’t easy.
Ellen wore an apron with a picture of a cat wearing a chef’s hat and the words “The Chef Breathlessly Awaits Your Order” printed beneath.
“I thought it was cute, you know? Kids like cats. Something kind of fun for today,” she explained. Ellen is good at remembering what’s most important and forgetting everything else. Today was all about being there for the kids.
Ellen had no connection to funerals or burials when she bought the Eloise Woods property in 2009. She had completed a doctorate in neuroscience at Stanford University before becoming a stay-at-home mom in Austin. She was so inspired by the show Six Feet Under, where she first learned about natural burial, that she decided to get into the death business herself. She became obsessed with creating a space in Austin where people can bury their dead themselves, a place where the memory of the deceased can continue to grow with the landscape.
Ellen is the reason I got into natural burial. Her accomplishments as an industry outsider signified a shift in my profession and revealed an opportunity largely untouched by traditional industry professionals. In Wisconsin, where I received my funeral director’s license, combining the business of funeral homes and cemeteries is prohibited under the state’s anti-combination law. Due to this 80-year-old statute, I became accustomed to hearing each business condemn the other, usually over outrageously high prices.
When I got to Texas, which allows the two businesses to be combined, it became apparent that such criticisms stemmed from a shared anxiety about the future of the industry as a whole. Cheap, efficient cremations have risen in popularity since the ’90s, eating into the conventional funeral industry’s profits. Families with little interest in embalming or holding a service make it harder for funeral homes to maintain their value.
Even Houston-headquartered Service Corporation International, the nation’s largest funeral corporation, appears to be acknowledging this change of venue. In October 2014, having lost a battle to overturn Wisconsin’s anti-combo law, Service Corporation opted to sell the last of its 16 Wisconsin funeral homes, keeping the five cemeteries it owns in the state. For people in search of a final resting place for their ashes or bones, a cemetery is the only choice. Natural burial parks that are accustomed to working with families without the involvement of a funeral home make that choice easier.
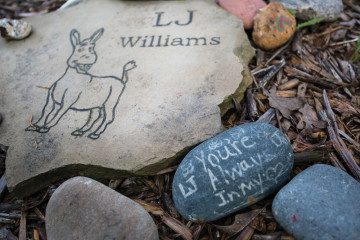
L.J.’s family surrounded his memorial stone with rocks carrying special notes. Owner Ellen MacDonald creates hand-engraved memorial stones for everyone buried at Eloise Woods, like this one featuring Donkey, L.J.’s favorite character from the movie Shrek.
The first burial I worked at Eloise Woods was for a young man in his late 20s. This last summer we buried three kids: one boy of grade-school age and two infants. There are more than 60 occupied plots in the park, a quarter of them for infants and children.
I met L.J.’s family for the first time about a month prior to his death. His three sisters attacked me with questions and whirled with an exuberance that only children seem able to bring to their first experience of death. Having never seen me or even heard my name, they grabbed my hands and Texie crawled into my arms as we set off to explore the graves.
“What happens if you are the last person on earth and everyone else dies?” Tori asked.
“I guess it would be very quiet,” I answered.
“Do you know the month and day you are going to die?” she asked. I said I did not.
“When you die, are you the same age forever?” Taylor Ann asked.
I thought about that carefully before saying “I think so,” though I also told them I was unsure. Then I asked what age they would want to be forever, and we all agreed we’d want to be somewhere in the teenage years, in the bloom of youth.
They picked the wild coreopsis that grows along the paths to put near L.J.’s gravesite. As we came upon the nearby grave of a 26-year-old man, his pensive portrait engraved on his stone, they wondered how he had died. I didn’t know, and that’s what I told them.
“My brother is going to die and come to Eloise Woods,” one of the girls said. At L.J.’s grave, their parents stood with a stroller into which was strapped their littlest brother. Jackie, their mother, looked only slightly overwhelmed and remarkably well put together. She was talking to Ellen about why she’d brought the girls. They’d been confused about L.J.’s future whereabouts, so Jackie thought it would be good for them to see the little 3-by-3-foot hole with the pile of dirt next to it. They laid rocks around the hole, and flowers inside of it.
The girls were fascinated by the wildlife of the park. It looks like a wooded campground, full of bugs, lizards and animals. Hoping to see a bunny, we walked a few more trails while they told me that L.J. slept a lot and no longer got in his wheelchair.
One of them asked me what happens when you die.
“Out here,” I said, pointing to some wildflowers, “you become a plant.”
“What!?” they yelped in confusion.
“Plants are going to grow out of his body?” Tori asked. I realized that I’d have to explain decomposition to complete the puzzle.
“Well, after we die, our bodies break down,” I stammered. I tried again: “They sort of fall apart.” It was no use. Looks of confusion and then boredom crossed their faces.
“Let’s go look for Mom,” said Taylor Ann. They took off, away from me.
They found their parents at the sheds and Ellen presented them with markers and rocks to scribble messages on for L.J. Tori wrote “Get Well Soon” on one. Texie drew a fairly sophisticated cat on another.
The more they colored, the more evident it became that L.J.’s death was an event they were preparing for in much the same way they would prepare for a birthday. To add extra excitement, the date would be a surprise, no matter how ready they thought they were.
Ellen’s cat apron was overshadowed by other sartorial matters once L.J.’s family arrived for his burial. Taylor Ann jumped out of the van barefoot and ran over to me. She had been too distracted to put on shoes before they’d left their house that morning. After parking the van, Jackie opened the door with a mixture of confusion and exhaustion on her face. She caught sight of the bare feet and became annoyed. “Where are your shoes? I told you to put on shoes!” she yelled.
Taylor Ann’s face suddenly reflected the gravity of the day, a collision of sadness and anger at having been yelled at by her mother, who had just lost a child. She burst into tears. Ellen quickly offered some extra sneakers she kept in the shed. Tori and Texie hopped out of the van wearing matching handmade black dresses with white cats on them and pink-and-blue cowboy boots. Taylor Ann stomped down Cardinal Trail toward L.J.’s grave wearing the same cat-pattern dress and borrowed sneakers five sizes too big.
The small group of guests held armfuls of sunflowers and babies. Kids ran wild while their parents alternated between quiet grief and chirping baby talk. The back door of the van remained open and unattended under a bright early-afternoon sun. Inside was a simple pine box about 4 feet long.
Jason, L.J.’s stepfather, and another man got inside the grave with shovels provided by Ellen and finished the digging that we’d been unable to complete that morning. The sisters posed with their sunflowers while I took pictures on my phone, and then they colored pictures to place inside the casket with L.J. After about half an hour, Jackie and Jason went to the van for the casket. Jackie’s face carried a look of powerful intention as they brought it to the grave and set it on the path while we all gathered around. They opened the top and laid it perpendicular across the casket, revealing little L.J. lying on his side, wrapped in a white blanket.
Everyone took turns writing on the top of the casket. The girls laid their pictures next to L.J.
A pastor wearing a rainbow sash covered in peace signs and yin-yang symbols started the ceremony. Taylor Ann, not quite grasping the mood, interrupted with an enthusiastic observation and was reprimanded loudly by Jackie. Still stinging from her earlier scolding, Taylor Ann began to pout until the pastor asked her to stand next to her. Together, they began to read a children’s poem that attempted to explain death.
The girls’ 2-year-old brother, Junior, out of his stroller for the first time I had ever seen, began to stalk the woods. While everyone stood sweating and patient, listening to the poem, Junior squatted outside the circle and began to taste the dirt. Jason alternated between chasing him and standing near Jackie, his expression lightening and darkening between the two situations. When the service was over, everyone said their goodbyes before placing L.J.’s casket into the earth.
It’s hard to explain how it felt to watch the girls embrace their dead brother in his casket. How they kissed his face and stroked his hair then delightedly shoveled dirt onto his grave. If I had to try, I would say it was like hearing a child’s first attempt to pronounce a new word. Ever afterward you hear that word differently, spoken without apprehension and full of love.
The next time I saw them I was measuring and marking plots in an open field. The girls came running at me with arms spread wide like I was someone they loved. I was ripe from working in the sun all day, but Texie clung to me like she had the first day we met. We talked about the other kids who were buried there and walked to one of their graves. Jackie asked questions about him. All the parents do this. They want the story on the kids, looking for similarities that will pull them together. I didn’t know much about the kid’s story, so I asked about L.J.’s.
At the sheds, I gave the girls the coloring books I had brought that day. Junior, red-faced and awake, rolled in the dirt. Jackie gave me the long version of L.J. ’s situation, which started with his being diagnosed with spina bifida, which isn’t a life-threatening condition. The events that led to his death began with him toppling over in his wheelchair. The accident apparently created fissures in his skull, through which cerebrospinal fluid drained. Jackie says his doctors misdiagnosed L.J.’s resulting condition for years before she finally convinced them to perform a 12-hour surgery, but it was too late to save him. He didn’t have to die, she said. She showed me pictures on her phone: L.J. with purple, puffy eyes and a zig-zag incision across the top of his skull. Then she showed me pictures of L.J. when he was healthy, with big brown eyes and a shy smile.
Eloise Woods owner and operator Ellen MacDonald maps the coordinates of a grave in Dunyah Garden, just off Cardinal Trail. Some portions of Eloise Woods are specifically dedicated, like Teva Garden, an exclusively Jewish section, and Sweet Angel Garden, for infants. Rainbow Bridge holds pet remains, but many people interred at Eloise Woods chose to have their pets buried by their side.
They don’t have the energy to file a lawsuit, but they are angry. The constant hospital visits put a huge strain on the family. They were briefly homeless, sleeping in a van in the hospital parking lot.
“That was my favorite because I got to lie down,” Taylor Ann said, smiling and drawing out “liiiiie doooown” and spreading her arms. Jackie gave her an odd smile, unsure if it was safe to laugh at her daughter’s black humor in front of me. I told Taylor Ann that what she’d said was oddly comical, and Jackie broke into a relieved smile. She said that when L.J. died, the family finally had a laugh. Home funerals, like parenting, bring unpredictable joys.
Jackie explained that after L.J. died, as they were washing him, they had pulled out his gastrostomy tube, creating a leak. They scrambled for the Krazy Glue to close the hole. They all laughed as Jackie recounted this, and the girls became giddy as they clamored to offer their favorite silly moments of the death. They told me about how L.J.’s body went floppy after he died and the girls played with his limbs like a doll. Texie had waved his hand, mimicking a lecturing adult. “I’m Dr. George, and you’re not sick,” she mimicked. The sisters burst into giggles again. I could see very clearly how deeply they loved one another, how making their mother smile and laugh was the most important thing in their world.
Jackie, flushed from the laughter, said L.J. would pull at her hair to bring her closer, right until the end. She said the girls all slept with him in the living room the night after his death. Texie told us that now he’s in Eloise Woods in a silly voice that her sisters made her repeat over and over while they laughed.
When I left that day, I cried all the way home. Complete Article HERE!
Tumors had disfigured AshLeigh McHale’s features and spread to her organs. A year ago, AshLeigh, 17, flew from her home in Catoosa, Okla., to the National Institutes of Health in Bethesda, Md., with a thread-thin hope of slowing her melanoma.
One morning a social worker stopped by her hospital room. They began a conversation that would be inconceivable to most teenagers: If death approached and AshLeigh could no longer speak, what would she want those who surrounded her to know?
The social worker showed AshLeigh a new planning guide designed to help critically ill young patients express their preferences for their final days — and afterward.
If visitors arrived when AshLeigh was asleep, did she want to be woken? If they started crying, should they step outside or talk about their feelings with her?
What about life support? Funeral details? Who should inherit her computer? Or Bandit, her dachshund?
AshLeigh grabbed her blue and hot-pink pens, and began scribbling furiously.
When she died in July, she was at home as she had requested. Per her instructions, she was laid out for the funeral in her favorite jeans, cowgirl boots and the white shirt she had gotten for Christmas. Later, the family dined, as AshLeigh had directed, on steak fajitas and corn on the cob.
“I don’t know what I would have done if I’d had to make these decisions during our extreme grief,” said her mother, Ronda McHale. “But she did it all for me. Even though she got to where she couldn’t speak, AshLeigh had her say.”
AshLeigh McHale, center, gave her family detailed instructions about her final wishes, including those concerning her funeral.
A national push to have end-of-life discussions before a patient is too sick to participate has focused largely on older adults. When patients are under 18 and do not have legal decision-making authority, doctors have traditionally asked anguished parents to make advanced-care choices on their behalf.
More recently, providers have begun approaching teenagers and young adults directly, giving them a voice in these difficult decisions, though parents retain legal authority for underage patients.
“Adolescents are competent enough to discuss their end-of-life preferences,” said Pamela S. Hinds, a contributor on pediatrics for “Dying in America,” a 2014 report by the nonprofit Institute of Medicine. “Studies show they prefer to be involved and have not been harmed by any such involvement.”
There are no firm estimates of the number of young patients facing life-threatening diseases at any given time. Cancer, heart disease and congenital deformities together account for an estimated 11 percent of deaths among adolescents, about 1,700 per year. And many thousands live with the uncertainty of grave illness.
“If you are one of the children for whom this matters, or one of their parents, this is a huge opportunity,” Dr. Chris Feudtner, a pediatric palliative care physician and ethicist at the Children’s Hospital of Philadelphia, said of these conversations.
But shifting from hushed talks with parents to conversations that include young patients has met some resistance. Many doctors lack training about how to raise these topics with teenagers. Until recently, most clinical teams believed that adolescents would not understand the implications of end-of-life planning and that they might be psychologically harmed by such talk.
Sometimes when providers do make the attempt, parents or patients may abruptly change the subject, fearful that by joining in, they are signaling that they have abandoned hope.
Yet research shows that avoiding these talks exacerbates the teenage patient’s fear and sense of isolation. In a 2012 survey examining end-of-life attitudes among adolescent patients with H.I.V., 56 percent said that not being able to discuss their preferences was “a fate worse than death.” In a 2013 study, adolescents and parents described such directed family talks as emotionally healing.
Teenage patients can guide, even lead, their medical care, Dr. Feudtner said. But more important, including them in the discussions acknowledges a terrible fact that patient and family members struggle to keep from each other: the likelihood of death.
“Then people can be together, as opposed to alone,” Dr. Feudtner said. The teenage patient feels free to address intimate topics, including “the scariest aspects of the human condition — mortality and pain — but also love, friendship and connection.”
Karly Koch, 20, worshiping in Muncie, Ind. She has a rare genetic immune disorder, and has written about her end-of-life plans.
Creating a Legacy
Karly Koch, a college student from Muncie, Ind., has been treated for many serious illnesses, including Stage 4 lymphoma, all related to a rare genetic immune disorder. Her older sister, Kelsey, died of the condition at 22.
Last spring, Karly, then 19, developed congestive heart failure. Her renal arteries were 90 percent blocked. As Karly lay in intensive care at the National Institutes of Health, a psychotherapist who had worked with the family for years approached her mother, Tammy, with the new planning guide.
“Do we talk about dying?” Mrs. Koch recalled wondering. “Maybe Karly hasn’t thought about it — do we put it in her head?”
“We had already buried a child and had to guess what she wanted,” she continued. “So we wanted Karly to have a voice.”
Karly’s reaction? “She said it wasn’t like we were telling her something she didn’t already know,” Mrs. Koch said.
The guide used by Karly Koch and AshLeigh McHale is called “Voicing My Choices.” While there are end-of-life workbooks for young children and their parents, as well as planning guides for older adults, this is the first guide created for — and largely by — adolescent and young adult patients.
The intention was to create a way for them “to make choices about what nurtures, protects and affirms their remaining life and how they wish to be remembered,” said Lori Wiener, a social worker and principal investigator on the research that led to the planning guide.
Karly Koch with her mother, Tammy.
In the two years since its introduction, more than 20,000 copies have been ordered by families and more than 70 medical centers from Aging With Dignity, the nonprofit that publishes it. “Voicing My Choices” has also been translated into Spanish, Italian, French and Slovak.
In straightforward language, the guide offers young patients check boxes for medical decisions like pain management. Another section asks about comfort. Favorite foods? Music? When visitors arrive, one option could be: “Please dress me, comb my hair and do whatever else is needed to help make me look like myself.”
What gives you strength or joy, the guide asks. What do you wish to be forgiven for? And who do you wish to forgive?
“These are the things that are important to know about me,” one list begins. AshLeigh, who would dance and sing down the aisles of Walmart, wrote: “Fun-loving, courageous, smart, pretty wild and crazy.”
Devastating disease can leave anyone feeling powerless, so a means to assert some control can be therapeutic. For adolescents, who are exploring and defining identity, Dr. Feudtner said, “you can express who you are, what you are and what you care about.”
Karly Koch with her family in Indiana.
By offering young patients opportunities to write farewell letters, donate their bodies to research and create rituals for remembering them, the planning guide allays one of their greatest fears: that they are too young to leave a meaningful legacy.
And so the ability to do it can galvanize them. Lauren Weller Sidorowicz received a diagnosis of metastatic bone cancer at age 18. Determined and outspoken, she joined a focus group of young patients at the N.I.H. whose opinions led to the creation of the planning guide. Days before she died in 2011 at age 26, Ms. Sidorowicz paged Dr. Wiener, frantic to include a final thought in a farewell letter.
To her grandmother, she wrote, “I hope there is potato salad in Heaven as good as yours.”
There are no standards for when and how to introduce a critically ill teenager to end-of-life planning; there are only intuition and experience. Many pediatric cancers have favorable prognoses, Dr. Feudtner said, and raising the topic prematurely may provoke anxiety and fear.
More often, though, doctors postpone the discussion too long, until the patient is too sick to take part. Dr. Maryland Pao, a psychiatrist at the National Institute of Mental Health who helped design the guide, recalled the despair of a mother whose dying son could no longer speak.
“I have no idea what he wants,” the woman told her. “He’s 17, but we never communicated about this.”
Dr. Wiener believes preparation should be done soon after diagnosis, but when the patient is stable. Exploratory talks, she said, become steppingstones, each readying the patient for the next one.
Still, providers encounter problems. “If the family doesn’t want to do it, you’re stuck,” Dr. Pao said. “There’s a lot of magical thinking — that if you talk about it, you’ll help them die.”
And sometimes teenagers themselves put up obstacles to having frank family discussions. Some young patients, for example, did not want Dr. Pao to tell their parents that they were ready to stop treatment. Rather than say as much to their heartbroken relatives, some will pour out their feelings on social media.
Erin Boyle, 25, had been treated for autoimmune disorders since she was 4. Last August, as she prepared for a stem cell transplant for leukemia, N.I.H. researchers asked whether she felt comfortable looking through “Voicing My Choices.”
Ms. Boyle completed most of the guide. At that time, she recalled, “the decisions felt theoretical rather than imminent.”
But shortly after the transplant, she relapsed.
“It was comforting to get my wishes down on paper and free myself to live without worrying about the details of dying,” she said recently.
She died on Wednesday. Her body is going to the N.I.H. for a research autopsy, as she wished, her mother, Ellen, said.
For doctors, end-of-life discussions with adolescent patients can be wrenching. “You have to be self-aware and reflect on your own experiences with grief and loss,” Dr. Pao said. “It’s hard not to be anxious if you have children. You feel helpless. It makes you face your own mortality.”
Ms. Koch on her way to have blood drawn.
On July 25, Karly Koch had an experimental bone marrow transplant. Her family calls that date her “re-birthday.” With 12 medications a day and a surgical mask, she is out and about in Muncie.
Karly takes classes to become a physical therapy assistant. She is a youth leader at her church, where her boyfriend is also a member. She delights in “normal people” activities.
Her parents keep Karly’s copy of “Voicing My Choices” in their bedroom cabinet. “It isn’t gloomy to go through,” Karly said. “It’s kind of fun to get your feelings out there.”
“Now, looking at it,” she continued, “I think I’d like to add some things.”
Sometimes when something unbelievable happens, it’s so outrageous (usually in a good way) that it seems like you’re in a dream.
Life is what you make of it. So if you dare to dream, envision what you want it to be – it becomes your reality. It goes right along with the saying “You can be anything you want to be…”
In dreams anything is possible, impossible becomes possible. In life there are limitations with unseen forces that work along with our motives to confuse us more on the path to fulfillment. Life is but a dream – nothing is so easy as to dream it and make it happen right that moment without obstacles standing in way.
It’s sort of a pot rush, even if the type of weed that will soon be spreading across the state supposedly doesn’t get users high.
The Department of Health’s Office of Compassionate Use this week hurriedly published a revised rule governing everything from stems and seeds to serving the substance to sick kids. The latest version of the rule included tweaks to who can own the five “dispensing organizations” that will eventually get licensed by the state to grow, process and distribute newly-authorized strains of cannabis.
The Legislature, in approving a pot law this spring, required each applicant to have a valid registration from the Department of Agriculture and Consumer Services to cultivate more than 400,000 plants, be operated by a nurseryman as defined by state law and have operated as a registered nursery in the state for at least 30 continuous years. At least 60 nurseries meet the criteria.
A preliminary rule floated by health regulators would have allowed nurseries to have just 25 percent ownership in the entities applying for a license. That option drew a rebuke from the Legislature’s Joint Administrative Procedures Committee, which helps oversee state regulations. The original proposal also neglected to specifically address whether the nursery would be required to have a continued role in running the pot operation.
Under Tuesday’s revised proposal, a nurseryman would have to “serve as the operator,” alleviating some concerns that growers would have little or nothing to do with the grow operation despite lawmakers’ intention that the nascent pot business be controlled by companies with a long agricultural history in Florida. The proposal would require a nursery to have at least 25 percent ownership of the organization that gets a license, but also would offer another alternative that would allow “100 percent of the owners of a nursery” to fulfill that 25 percent requirement.
That ownership change appears aimed at appeasing some nursery owners who expressed concerns about financing the marijuana operations. Because pot is still illegal under federal law, nearly all banks are refusing to lend money to marijuana-related businesses. Converting other areas of operations into cash-only business could pose major problems for growers interested in participating in the medical marijuana start-ups, a lawyer for Costa Farms told the Department of Health at a day-long public hearing last week.
With Scott’s blessing, lawmakers this spring legalized marijuana that contains .8 percent or less of euphoria-inducing tetrahydrocannabinol, or THC, and more than 10 percent cannabidiol, or CBD. Supporters believe the compound, which hasn’t been approved by the feds, can eliminate or drastically reduce life-threatening seizures in children with severe forms of epilepsy. Under the law, doctors can also order the low-THC, high-CBD substance — usually delivered in paste or oil forms — for patients with other spastic disorders or cancer, as long as they have exhausted all other treatments.
Many GOP lawmakers jumped on the “doesn’t get you high” pot bandwagon this spring hoping to thwart Amendment 2, a proposed constitutional change that would legalize “traditional” medical marijuana.
While the state moves toward getting the low-THC, high-CBD regulatory framework in place by Jan. 1, the battle over Amendment 2 — bankrolled heavily by Orlando trial lawyer and Democratic fundraiser John Morgan — is starting to smoke.
The “Vote No on 2” campaign recently nailed down the backing of seven former Florida Supreme Court justices, who joined associations representing Florida sheriffs and police chiefs in opposition. And the amendment’s foes are planning to spend $1.6 million on television ads, slated to start running in October, condemning the proposal. Like all constitutional proposals, at least 60 percent of the voters must approve the amendment for it to pass.
“We want every voter to know the dangers of this amendment and that it is not about the sick, it is about legalizing pot for anyone and for any reason,” spokeswoman Sarah Bascom said.
Polls have shown widespread support for legalizing medical marijuana, but that support is expected to drop in the wake of a full-frontal attack. Las Vegas casino magnate Sheldon Adelson has pledged to double the $2.5 million he’s already dropped on the Drug Free Florida political committee, launched by Tampa Bay developer Mel Sembler. Both are mega-GOP money men.
“When your basic position runs completely counter to public opinion, millions in misleading advertising is the only strategy available. But no amount of advertising can overwhelm the basic facts,” said Ben Pollara, campaign manager at United for Care, a group spearheading the amendment. “Floridians know the benefits of medical marijuana are real, and the people of this state are deeply compassionate. We believe the overwhelming majority will vote to make sure patients no longer have to risk incarceration for listening to their doctors and seeking relief from debilitating diseases and medical conditions.”
“People’s deepest fears about death and dying often spring straight from a traumatic childhood incident or misshapen belief about the end of life that was passed on to them when they were kids.”
In previous postings I’ve talked about how postponing any thoughtful consideration of our death till it’s too late, can have disastrous consequences for us in terms of preparing for the inevitable. I addressed how our death-denying culture provides precious few opportunities for us to deal healthily with our mortality before it comes crashing in on us.
Why is dealing with death so hard for us? Early childhood messages about death sure don’t help. Think spooks, skeletons, things that go bump in the night, and specter of hell and damnation. From a young age, most of us have had it drilled into our heads that we shouldn’t ask questions or even talk about death because it’s either inappropriate, it’ll bring bad luck, or worse, hasten death.
How many times, as a child, did a relative, family friend, or even a beloved family pet simply disappear, never to be heard from or spoken of again? Or perhaps you were told that the absent loved one is now in heaven or asleep with the angels, the “D” word being avoided like Aunt Agnes’s infamous tuna surprise? Or maybe, when you were a kid, you were told that someone you knew had died, but that you wouldn’t be able to go to the funeral because that was no place for kids. And how much of the confusion, bewilderment, and unresolved grief from your childhood are you still carrying around with you today? Is it any wonder that, when faced with the prospect of our own death, we often feel like we’ve been ordered to belt out our swan song without ever having an opportunity to learn the tune.
In the first chapter of my book, The Amateur’s Guide To Death And Dying, I ask my readers to confront head-on the un-golden silence that surrounds the end of life. I invite them to consider the early messages they got about death and dying. I ask; how old were you when you first heard about or witnessed these things? What were the messages you picked up about death and dying from the movies or television? People often report that their deepest fears about death spring straight from a traumatic childhood incident or misshapen belief about the end of life that was passed on to them when they were kids. And, not surprisingly, most people report that they continue to carry these fears with them as adults.
I believe that’s criminal. I also believe that there is a better way to handle this delicate matter with young people than avoiding it, sidestepping it, or perpetuating a misconception. I believe we can break the vicious cycle of our culture’s death phobia by refusing to contaminate another generation with it. It would take a concerted effort, of course, and it would mean that we would have to resolve ourselves of our own fears first, but I believe it’s doable.
A good place to begin this effort is with the stories we read to and tell our children. Stories, both written and recited, become the basis of our children’s understanding of the world. Stories contribute to their language development as well as their critical thinking, and coping skills. Death and grief are particularly thorny subjects to communicate to children, not because our children are incapable of grasping the message, but because we, the adult storytellers, are often unprepared for, or uncomfortable with, the topics ourselves.
To address this problem, I developed a workshop titled: Exploring Death and Grief Through the Medium of the Children’s Story. In this workshop I help adults choose age specific messaging and images for their storytelling. I help them mold the basic concepts about death and bereavement into the arc of their story. And finally, I offer the workshop attendees tips on writing and illustrating their own story with the kids in their life.
By way of example, I share with my audience my latest children’s story, Longfellow And The Deep Hidden Woods. This is the story of Longfellow, the bravest and noblest wiener dog in the world. As my story begins, Longfellow is a puppy learning how to be a good friend to his human companions, old Henry and Henry’s nurse Miss O’weeza Tuffy. By the end of the story, Longfellow has grown old himself, but he is still ready for one final adventure. What happens in between throws a tender light on the difficult truths of loss and longing as well as on our greatest hopes. Curiously enough, all the adults who have read my story say they think it’s actually a book for adults. Maybe so! I can be really subversive like that.
Writing and illustrating a children’s story with your kids can be an amazing bonding experience for both the adult and the child, but this is especially true when the topics are death and bereavement. It’s a project that will open the door to a life-long appreciation for and the affirmation of life, especially it’s final season. The discussion that will be part of your story-writing project will also help you reshape the coming generation’s perceptions about the end of life. It may also help you rethink the early message you received about death and dying when you were a kid.
My workshop ends with one proviso. I caution the adults in my workshop not to wait until there’s a pressing need for the story writing or telling. I encourage them to start now, before grandpa or the beloved family pet is dead. I suggest that they get a jump on this project right away. Because, if they do, it won’t appear to their kids like they are trying to play catch up when death comes calling. I mean think about it; we don’t hold off teaching young people arithmetic till they get their first job making change at the grocery or the fast food counter, right?
Try to imagine how writing a story about death and grief with your kids or grand kids will change the trajectory of their life in terms of their understanding of this fundamental fact of life. Imagine if someone asks your kids or grand kids, twenty or forty years from now, what their earliest memories about death and dying are. Surely they will think back fondly on the time they spent with you as you helped them understand the marvelous cycle of life.
Will this one exercise inoculate your kids or grand kids from all the culturally induced fears, apprehensions and superstitions that abound in our death-phobic society? Probably not! But as the old adage goes, an ounce of prevention is worth a pound of cure.