Things are not necessarily as they appear. In Michael Cruz Kayne’s “Sorry for Your Loss,” a comedy show about grief, that is a prominent theme.
When the producer Kate Navin caught the show last year at Caveat, a comedy theater on the Lower East Side in New York, she knew the instant he displayed a photo of himself with his wife and two children what he wasn’t telling the audience: that this wasn’t the full picture of his family, that it couldn’t be, because one of his three children had died.
“In that moment I felt — I don’t want to use the word ‘seen’ because it can be cliché, but that’s the best word,” Navin said recently at a cafe in Greenwich Village.
Her own family photos work the same way. Her first son, Jack, was 2 years and nine months old when he died in a fire with his grandmother, Navin’s mother-in-law, 10 years ago this August. Ask Navin what Jack was like and she’ll tell you he loved the movie “Cars,” prized raspberries above all foods and was remarkably kind — unusual for a toddler, she knows, having had two more.
“You’d give him a bowl of raspberries and he’d hand them out to everybody in the room first before he’d start eating,” she said. “That was Jack. He was unbelievable.”
Navin was deliberately not going to produce shows about grief when she joined the audio entertainment company Audible in 2017 to head its theater division.
But when Daniel Goldstein, a writer-director who is a mutual friend of Navin and Kayne, took her to see “Sorry for Your Loss,” thinking that she might have a professional interest in it, he was correct. She thought the embrace of its humor could help other “lost parents,” as she calls them.
Michael Cruz Kayne, pictured with his family in “Sorry for Your Loss,” a comedy show about reckoning with the death of his son.
The show, running through June 10 at the Minetta Lane Theater, Audible Theater’s Greenwich Village base, is the latest iteration of “Sorry for Your Loss,” with shinier production values than Kayne, a staff writer on “The Late Show With Stephen Colbert,” is accustomed to having at comedy clubs. Here he ponders the mysteries of permanent absence and lingering presence, and pokes at the culture’s deep discomfort with the inevitability of death and loss.
Kayne, who hosts the podcast “A Good Cry,” first performed “Sorry for Your Loss” not long after a tweet he sent in November 2019, marking the 10th anniversary of the death of his son Fisher, from sepsis at 34 days old.
Kayne had grown tired of not talking about that central fact of his life, which he said in a separate interview had become “the elephant in the room of my whole brain.” After the tweet went viral, he took that conversation to the stage, making a funny autobiographical show that allows sadness in.
“I’m still at a point with it where I am happy to be identified with the story of my son,” Kayne said. “If that means that for a while, or forever, I am Grief Boy, things could be worse. This subject isn’t the only thing I want to contribute to the universe. But if it stopped here, I would feel like I got to say the thing I really wanted to say most of all.”
These were not, by the way, maudlin interviews. But Navin did tear up when she recounted how terrified she had been of grocery shopping after Jack died, because she wouldn’t know what to say if she ran into one of his friends and they asked where he was.
In the experience that Kayne articulates in the show, she recognized her own surreal isolation.
She wants no one’s pity. But mention a child who died to someone who didn’t know, she said, and the conversation may not recover, because no matter how long ago it happened, people react as if your grief is fresh, and as if you are broken.
“The mood shifts,” she said. “And it’s hard to be the person who caused the mood shift.”
Kayne and Navin would like people to be less awkward about grief, which would let those who need to talk about it stop keeping it to themselves. “Sorry for Your Loss” provides one space for that.
When I asked Kayne if he believes that art can heal, he quoted the W.H. Auden line “poetry makes nothing happen,” which he said he thinks about a lot.
“I do think it’s possible for art to at least make you feel like you are not alone,” he allowed. “It’s so much to know that I’m not the only person who feels this way. If that is healing, which I think it is a little, then yes, I think art can heal people.”
Navin, for her part, is certain that Kayne has changed her in a way that feels good, making her “less sheepish” about telling people that she has three children, and less worried about people’s reaction.
“That’s a huge gift,” she said. “And he just makes me feel less damaged. Truly I feel less damaged than I did a year ago.”
The thought of our dogs dying is something that we pet parents have a lot of difficulty with. But the reality is that, unlike your children or anyone else you’ve helped raise and take care of, your dog will probably not outlive you. At some point, it will be time to say goodbye to your dog.
Even more sobering, you may end up facing a difficult decision about when to end the life of this precious friend and family member. Some dogs do pass peacefully on their own, but in many cases, the will to survive keeps a dog going long past the point of experiencing good quality of life.
While recent advances in veterinary medicine are nothing short of amazing, remember that just because you can prolong your pet’s life doesn’t mean it’s in your dog’s best interest to do so.
Most of the factors around aging and death are beyond our control, but the one thing you are able to do for your dog is alleviate undue pain and suffering. Arguably, no other decision you make about your dog will be as difficult as the one to euthanize, but in so many cases, it’s the only humane option.
If there’s ever a time to put your dog’s welfare ahead of your own needs, this is it. While the idea of living without your beloved pet can be devastating, the thought of them suffering should feel even worse.
So in considering what to do, ask yourself the following questions:
Does your dog have a terminal illness? Ask your vet what to expect at the next stage. Then ask whether you’re prepared to go there.
Is your dog in the kind of pain that cannot be alleviated by medication?
Will more treatment improve your dog’s quality of life, or simply maintain a poor quality of life?
Can you afford treatment? End-of-life care can run into thousands of dollars. Unfortunately, people can end up prolonging their grieving while paying off credit cards.
Has your dog lost the ability to maintain most bodily functions? If they can no longer stand up, get down stairs, defecate, and urinate on their own, the quality of their life is pretty poor.
Do they still want to eat? Once a dog loses their appetite, they may be signaling that they’re close to the end.
Are their gums pink? When gums aren’t a normal pink, your dog isn’t getting enough oxygen.
Is it in their best interest to extend their life, or are you doing so for yourself? This last point is the most difficult one for most of us to sort out, but it may well be the most relevant.
Other Things to Consider
You may find that everyone feels free to tell you what to do, but the responsibility for this choice is yours. This can be more difficult if you have a significant other who’s also attached to your dog, and you disagree about the next steps. However, it can still weigh heavily on a single person.
People often say, “You’ll know when it’s time.” In many cases that’s true, but not always. But remember that no matter what people tell you, choosing euthanasia is not “playing God” any more than providing medical treatment to save a life is.
Your veterinarian is trained to save lives. That’s what they do, and that’s why you go to them. But all they can do is delay, not prevent. No vet should make you feel guilty for choosing not to pursue treatment, even if you can afford it.
If your vet is advising euthanasia and you’re reluctant, closely examine your own motives and see if they’re for your benefit or the dog’s. Most people believe it’s better to euthanize your dog a day too early rather than a day too late.
Euthanasia ensures that you’ll be able to be with your dog at the moment they pass, so they’re not alone. While you don’t have to be present, dogs turn to their beloved humans most when they’re fearful. It may be quite traumatic for your furry friend if you’re not with them.
That said, it may be best for kids or those who cannot remain calm to not stick around. Otherwise, they may make a stressful situation even worse for a frightened dog and other humans who are present.
Make a List or Two
Before your dog gets to the point where euthanasia is a consideration, and you’re still fairly calm, write a list of what gives them a good quality of life. Decide how many of those points they can be without in old age and still enjoy their life.
Eating. Will they still be able to enjoy food, or even eat on their own?
Walks. Will they be able to enjoy fresh air or any form of exercise?
Petting and affection. Can they still enjoy pets from you or from strangers? Do they recognize people, or do they act fearful?
Going outside. Can they go potty on their own when and where it’s appropriate? Or are they unable to control their bodily functions at all?
Being social. Does your dog still like to be in groups of people and dogs? Or do they easily feel exhausted and defensive?
Car rides. Can your dog still get in the car and stay comfortable on a ride? Can they stick their nose out the window?
How many points do you think your dog needs to enjoy life, even if they’re not in pain?
If you believe they can maintain quality of life with four of those seven, then you know it may be time to consider euthanasia if they lose the ability to keep three of those points.
Promise yourself that you’ll consider other factors, such as pain, the kind of senility that causes fear, and a lack of bodily function and control that may cancel out any items on the list.
Next, decide how much money you can afford to spend on veterinary care. Make a decision, write it down, and stick to your plan when your emotions are off the chart.
If your dog is suffering, then they’ve already lost most of the joy that comes from being a dog.
The emotions surrounding this decision are mixed and complicated. To do what’s best for your dogs, you need to realistically assess the criteria without allowing emotion to overwhelm the decision-making process.
Have you ever decided when to end your dog’s suffering? How did you make your decision? Let us know in the comments below.
— Death isn’t an easy subject, but Tufts University School of Medicine has developed effective exercises for teaching empathy to medical students
“Family doctors always talk about preventive care, like cancer screenings, nutrition, and vaccination. There’s a whole host of preventive issues we routinely bring up. And end-of-life wishes should be one of them,” says Amy Lee, M02, associate professor of family medicine at Tufts University School of Medicine.
By Christina Frank
No one likes to talk about dying—not even doctors, even though confronting death is a non-negotiable requirement of the job.
“Doctors in general are not very good at talking about end-of-life issues with patients,” says Amy Lee, M02, associate professor of family medicine at Tufts University School of Medicine. “Part of that is just our general cultural discomfort with talking about dying, but part of it is lack of education and training about how to do it well.”
Back in 2010, to address what they considered a significant gap in medical education, the Department of Family Medicine decided to require every medical student to participate in an experiential learning exercise about end-of-life decisions as part of their six-week family medicine clerkship in their third year. Earlier this year, Lee and Deborah Erlich, M07, associate professor of family medicine and family medicine clerkship director, published a paper in the journal Family Medicine evaluating three years of student reflections on the exercise. Students reported increased empathy for patients facing end-of-life decisions, and an intention to improve the way they support patients at the end of life.
Erlich points out that most clinical education on this topic was previously “opportunistic,” meaning that a student may have the chance to address end-of-life wishes with a patient as part of a hospital rotation, but not necessarily. “In the hospital there’s no systematic planning of which patient a student will see,” she says. “So, if they have a meaningful meeting with a dying patient in the hospital by happenstance, then maybe one student will have that experience around discussing a patient’s or family’s wishes at the end of life. But if they happen not to, they’ll miss that part of the education. We decided all students should receive training on this topic and graduate prepared to have these conversations.”
Using a booklet from the nonprofit organization Aging with Dignity called “Five Wishes,” each student is asked to privately fill out an advance directive for themselves. The idea is that by going through the process of thinking about what they would want at the end of their own lives, they develop a stronger sense of empathy toward patients. The wishes address practical concerns, such as who they’d want as a healthcare proxy, as well as medical and emotional concerns. They can specify under which conditions they’d want to discontinue treatment, if they’d like someone to be with them when they die (if possible), and what they’d like their legacy to be.
“In this case, students are not roleplaying having a real conversation with a patient—which is also critically important— but they are putting themselves in the position of walking in the patient’s shoes,” says Erlich. “That’s one of the things that defines empathy.”
The “Five Wishes” exercise is now one of many components in the medical school’s curriculum that address end-of-life care. Students in the preclinical years learn about caring for dying patients as part of a mandatory course called “Threads.” Other courses include patient interviews where patients and their family members talk about coping with illness, death, and dying. Clerkships for students in their clinical years hope to offer more opportunities for students to address end-of-life issues.
As family medicine physicians, Lee and Erlich think primary care physicians, especially, should begin discussing a patient’s end-of-life wishes long before they are known to be dying. “We’re family doctors, so we take care of patients throughout their lifespan,” says Lee. “We have long-term relationships with our patients and their families. It’s even more important in that trusting environment to be able to have these difficult conversations.”
To kick off a conversation with the students about this, Lee and Erlich informally ask the group if they think an 80-year-old should discuss this topic with their family doctor at their annual visit, to which everyone answers yes. “Then we say how about a 70-year-old, a 60-year-old, and continue down the lifespan by decade,” Erlich explains. We get down to people in their 20s and 30s and almost all of the students agree that end-of-life wishes should be discussed at annual visits for all adults.”
Lee says the early days of the COVID-19 pandemic made younger people more aware of how important it is to talk about end-of-life wishes, and that it is an issue that affects people of all ages.
“The pandemic resulted in the deaths of younger, relatively healthy people. I think our students recognized that it would be a good idea to at least think about a healthcare proxy, for example, who would make decisions for you if you were incapacitated,” Lee says. “Family doctors always talk about preventive care, like cancer screenings, nutrition, and vaccination. There’s a whole host of preventive issues we routinely bring up. And end-of-life wishes should be one of them. Unfortunately, all human beings inevitably will die, and better to have a death that is prepared for and incorporates what the patient wants.”
The Student Perspective
These innovations in the School of Medicine’s curriculum means that future physicians will be able to better empathize with and support patients and their families as they make end-of-life decisions.
Christianne Gonzalez Davidson, M24, is finishing up her third year in medical school and is planning to go into family medicine. She says she found the “Five Wishes” exercise initially disconcerting, but ultimately empowering.
“On the one hand, it shook me a bit to reflect on the hypothetical situations presented—such as myself in a coma without hope of recovery or being on life support. Having seen patients in these conditions with their loved ones and imagining myself and my family in their shoes was a very humbling experience. But then I realized that this exercise made me feel not only empathy for patients in this position, but also a sense of autonomy, and that’s something I hope to be able to offer my future patients as well.”
— A new paradigm to enhance senior living. Embrace aging as a gift.
By John Ritchie
Conscious Aging: to experience senior aging as more a gift and less a burden, and many burdens as also gifts.
Senior living, with retirement or part-time work, may bring more free time, less work stress and more choices for what you want to do. It can also at times feel lonely, or leave one feeling depressed or anxious because of the loss of work and work community, diminished physical abilities and social contacts, and decreasing accomplishments, recognition, usefulness and felt importance. I see Conscious Aging as a special combination of mutually enhancing experiences and practices uniquely relevant and available to seniors.
Conscious, in this context, means to intentionally be more mindful and present, to enhance our awareness and connections, or open our mind and heart. “Inner Work” is the primary practice and relationships become more important than accomplishments. Through increased exploration, self-reflection and compassion, we can experience a shift in our interests, values and needs, and greater acceptance, appreciation and enjoyment of senior living. Conscious Aging is focused not on what we should believe or externally do, but how to be and experience life.
I am suggesting that our present “successful” aging and “positive” aging models or guidelines for senior living support a paradigm that primarily focuses on external criteria and goals. It is common for seniors to talk about, and identify with, their travels, recreation, fun activities, entertainment interests, past accomplishments and children/grandchildren activities. Focusing on external-based goals, possessions and activities tends to not find fulfillment or happiness beyond short-term pleasure; and avoids directly exploring and finding “positives” from our “negative” senior sufferings, losses and limitations. Successful models were more important and helpful for us when we were young adults and middle age (e.g. finding a good job, spouse and career; and creating a successful family, comfortable home, active social life). These external-based models now tend not to align with our internal senior shifts in interests, values and needs; nor satisfy our increased senior yearnings or utilize natural aging experiences.
I am advocating for what I’m calling “Enhancing Awareness and Connections” as a quality or process of how to focus our attention and effort, to be applied to all components of Conscious Aging. All of senior aging is our curriculum. Conscious Aging has been applied to various components, or “what” to focus our attention and effort on. Some of these components include 1) conscious eldering, 2) bringing closure to life, 3) preparing for dying and death, 4) conscious senior service, 5) Conscious Villages or co-living, and 6) living life’s purpose and meaning.
I. For those of you who are already seniors, see if you resonate with some of the listed common shifts from middle age to senior age in interests, values, needs or roles. These are often due to, or facilitate, “inner work” and increased awareness and connections, that come with senior aging. “Living more from the ‘inside out’ rather than from the ‘outside in’.” “It’s not what happens to us, but our relationship to what happens.”
Doing to Being … Staying Busy to Slowing down … Intensity to Intimacy
Holding On to Letting Go … Past/Future to Present … Seeking Pleasure to Appreciation
Outcomes to Relationships … Competition to Cooperation … Self-Centered to Selflessness
Learning to Understanding … Criticalness to Empathy … Distractions to Presence
Head to Heart … Fairness to Compassion … Accomplishments to Contributions
II. See if you resonate with some of these increased senior “yearnings” as you become more aware of what “pulls” you rather than responding to what has “pushed” you in the past. Yearnings support “inner work” or enhanced understanding and relationships, and Conscious Aging. “We want to know our essential nature or essence, or to go from self to soul to spirit.”—Kathleen Dowling Singh. “The second half of life is about restoring wholeness.”
Find Life’s Meaning … Clarify My Purpose … Understand Spirituality … Know Thy True Self
Become Comfortable With Dying … Want Deeper Relationships … Connect to Everything/Divine
III. See if you resonate with some of these natural senior aging experiences, which support and enhance inner work or greater awareness/understanding and connections/relationships, and thereby Conscious Aging. “Senior aging is not a problem we need to solve, but a stage of life to be fully experienced.”
Slowing Down … Solitude … Silence … Letting Go … Patience … Acceptance
Being in the Present … Calm … Forgiveness … Simplifying … Humility … Vulnerability
IV. As you will notice, the following intentional “inner work and internal practices” overlap with natural senior aging experiences and what seniors commonly experience as middle-age to senior-age shifts in interests, values, and needs, to further enhance Conscious Aging. “We can’t choose or control the circumstances of our age, but we can choose the quality of awareness we bring to those circumstances.” “Your compassion may or may not change others, but it will certainly change you.” “When life is short, make it broader and deeper.”
Calm, Curious, and Compassionate … Being in the Present … Slowing Down … Silence … Solitude
V. We can apply inner work and internal practices to common senior aging negative experiences to access and experience positive thoughts, feelings, and experiences. Our struggles become portals for understanding, growth and healing. “There are some things you can only learn in a storm.” “Until we suffer, we won’t look deeply for something more to learn.”
For example, if you are feeling sad and lonely, frustrated and stuck, or very ill and tired, direct your attention inward and internally slow down in silence to become calm, curious and compassionate. Direct your attention to the present, which will help you let go of future and past attachments or distractions. You will then notice how you can see broader and deeper with greater presence, understanding and loving kindness. This will help you notice what moves you or brings you joy and what you appreciate in the moment or about others and yourself. For example, you’re stuck in bed, and you shift your attention from what you can’t do, to what you can do, enjoy or appreciate, such as sight (notice beauty, watch movie), sound (listen to music, birds outside), or touch (pet your dog, give self a massage). You can shift attention to relationships and initiate or schedule more frequent and closer connections- longer talks, phone calls, Zoom meetings, texting, Facebook, or invitations to visit you. It’s now more about connections, harmony and wholeness, than about individual accomplishments and success.
— The battle over how science defines the end of life
The concept of brain death is facing its greatest challenge in the United States in decades.
Ideological differences threaten to muddy the definition of death in the United States — with potentially negative consequences for clinicians and people awaiting organ transplants.
Dead in California but alive in New Jersey: that was the status of 13-year-old Jahi McMath after physicians in Oakland, California, declared her brain dead in 2013, after complications from a tonsillectomy. Unhappy with the care that their daughter received and unwilling to remove life support, McMath’s family moved with her to New Jersey, where the law allowed them to lodge a religious objection to the declaration of brain death and keep McMath connected to life-support systems for another four and a half years.
Prompted by such legal discrepancies and a growing number of lawsuits around the United States, a group of neurologists, physicians, lawyers and bioethicists is attempting to harmonize state laws surrounding the determination of death. They say that imprecise language in existing laws — as well as research done since the laws were passed — threatens to undermine public confidence in how death is defined worldwide.
“It doesn’t really make a lot of sense,” says Ariane Lewis, a neurocritical care clinician at NYU Langone Health in New York City. “Death is something that should be a set, finite thing. It shouldn’t be something that’s left up to interpretation.”
Since 2021, a committee in the Uniform Law Commission (ULC), a non-profit organization in Chicago, Illinois, that drafts model legislation for states to adopt, has been revising its recommendation for the legal determination of death. The drafting committee hopes to clarify the definition of brain death, determine whether consent is required to test for it, specify how to handle family objections and provide guidance on how to incorporate future changes to medical standards. The broader membership of the ULC will offer feedback on the first draft of the revised law at a meeting on 26 July. After members vote on it, the text could be ready for state legislatures to consider by the middle of next year.
But as the ULC revision process has progressed, clinicians who were once eager to address these issues have become increasingly worried.
Fuelling their fears is a rising tide of political polarization and mistrust of scientific expertise. Some clinicians following the ULC discussions say that the idea of brain death itself is facing its greatest challenge since its conception in the 1960s. The outcome could have serious implications for intensive care units (ICUs) across the United States and might affect the availability of vital organs for transplant. And although few expect the ULC’s recommendations to erase the idea of brain death, some observers fear that the doubts and narratives sown throughout the process could have a lasting effect on state laws and on public perception.
“I thought this would be an upgrade, and it’s completely fallen apart from that perspective,” says Robert Truog, a bioethicist and paediatrician at Harvard Medical School in Boston, Massachusetts, who is not a voting member of the ULC committee, but has watched its progress closely. “As soon as we talk about the deeper issues, the profound disagreement of some members of the committee become apparent, and you reach a standstill.”
Redefining death
Current legal definitions around the world generally allow for two types of death: when heart and respiratory function stop irreversibly, or when crucial functions of the brain are lost. Historically, these two have been closely entwined: stop the heart, and the brain is dead in minutes. Stop the entire brain functioning, and the heart stops beating. But medical advances in the 1950s, such as modern ventilators, meant that the two types of death could be separated.
Such technologies, along with improved methods of measuring brain function, prompted the formation of a committee at Harvard University in Cambridge, Massachusetts, in 1968. The members developed a definition of irreversible coma or brain death that was controversial at the time.
In 1981, prompted by a presidential commission on the topic, the ULC codified this form of death into a model law called the Uniform Determination of Death Act (UDDA), stating that a person can be considered dead when there is an irreversible cessation of circulatory and respiratory function or of all functions of the entire brain, including the brainstem. The Harvard committee and the UDDA proved influential: most countries in the world followed suit with their own laws adopting brain death.
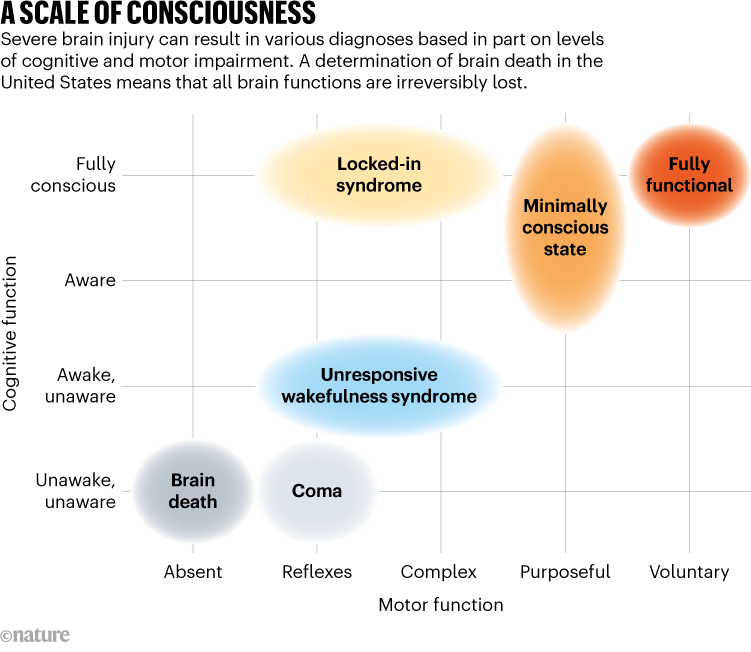
People who are in a coma, or who have unresponsive wakefulness syndrome, or locked-in syndrome are not brain dead. Not all functions of their brains have stopped, and some might be able to breathe without the assistance of a ventilator, show signs of wakefulness or have intact reflexes (see ‘A scale of consciousness’).
Source: J. L. Bernat Annu. Rev. Med. 60, 381–392 (2009)
Today, although brain death makes up just 2% of adult deaths and 5% of childhood deaths in hospitals in the United States, it tends to garner outsized attention from the media and in the law. Erin Paquette, a paediatrician and bioethicist at Northwestern University in Evanston, Illinois, says that’s because the physical appearance of a person who is brain dead often doesn’t line up with people’s concept of death. Hooked up to a ventilator, a person who is brain dead might look like any other individual in an ICU.
This can make it difficult for clinicians to communicate with family members about brain death, especially when the law lags behind scientific understanding. This happened in McMath’s case. Although she never definitively regained consciousness or the ability to breathe on her own, she began puberty and had her first menstrual period — a sign that a small region of her brain called the anterior hypothalamus, which helps to control the body’s hormones, might have been active.
This realization prompted her mother to sue the state of California in a bid to erase the death certificate there because not “all functions of the entire brain” had ceased as the UDDA dictates. Using a strict interpretation of the law, McMath’s mother might have been right, says James Bernat, a neurologist at the Dartmouth Geisel School of Medicine in Hanover, New Hampshire, even though it wasn’t a sign that the girl would recover. The anterior hypothalamus, Bernat says, receives blood through a different supply from the rest of the brain, so some function might be preserved in a small subset of people who have been declared brain dead. (McMath’s heart stopped in June 2018, at which point she was issued a second death certificate; her mother withdrew the lawsuit shortly afterwards.)
Language tweaks
Clinicians have called for changes to the language of the UDDA, hoping to clarify which brain areas are relevant to recovery. Other countries, such as the United Kingdom and India, define brain death much more narrowly than the United States, focusing not on the entire brain, but on the brain stem, which is necessary for essential functions such as breathing, swallowing and maintaining a heartbeat. The United Kingdom goes one step further by not separating the ways that death happens: all deaths happen when brainstem function is lost.
Truog supports this simplified system, which Canada adopted in May. But Bernat says it’s unlikely that the United States will adopt this standard: “If the ULC is going to do anything to the UDDA, they want to just tweak it,” he says. Nevertheless, he hopes that the revised law will address how to interpret residual activity in areas of the brain that are not linked to consciousness or breathing.
Nailah Winkfield appears at a news conference in 2018 to discuss the death of her daughter, Jahi McMath.
Other language changes are more subtle. Some clinicians have been calling to amend the law so that it refers to a ‘permanent’ loss of brain and heart function instead of an ‘irreversible’ one. The argument is that current tests for death do not evaluate reversibility, but rather permanence. Irreversibility, clinicians say, is a much higher standard to meet, and would require them to wait for hours to prove that they cannot restart heart or brain function. And even if it were possible to restore some functionality, some have said it might not be wise or even ethical to do so.
The need to address the language about irreversibility has been made more urgent thanks to research by Nenad Sestan, a neuroscientist at Yale University in New Haven, Connecticut. He and his colleagues pumped a blood substitute through the bodies of pigs and restored cellular function in some organs1, including the brain2, hours after the animals were slaughtered. They were careful to note that although cells might be metabolically active, this does not translate to organ function. “We might one day be able to reverse things we used to say were irreversible, and ultimately what we care about is permanence,” says Alex Capron, a medical ethicist and specialist in health policy at the University of Southern California in Los Angeles, who helped to direct national efforts to define death in the 1980s.
These language discrepancies mean that guidelines put out by organizations such as the American Academy of Neurology (AAN), in Minneapolis, Minnesota, outlining what physicians should test for when declaring brain death don’t line up with the UDDA.
Individual hospitals, too, have their own determination-of-death policies and procedures that might differ from those put out by the AAN. Currently, the UDDA states that physicians ought to use “accepted medical guidelines” as the basis of their determination, but that leaves room for them to use different medical organizations’ guidelines, and ones that are outdated.
In 2016, David Greer, a neurologist at Boston Medical Center, and his colleagues were surprised to find substantial differences when they analysed nearly 500 hospitals’ policies to see whether they adhered to the AAN’s guidelines3. They found that most clinics did not require someone with neurology experience to determine brain death, and more than one-quarter didn’t require physicians to test for conditions that can mimic brain death, such as abnormally low blood pressure or hypothermia.
New AAN guidelines are coming later this year, says Greer, who co-authored them. The revision will standardize death determination between adults and children to make the concept easier for people to understand, he says. Greer and others are calling for the UDDA to specify which medical guidelines to rely on and a process by which states can incorporate newer standards into practice.
Added tensions
But some are afraid that the time is not right to update the UDDA. Lainie Ross, a paediatrician and bioethicist at the University of Rochester in New York, says that when she heard this process was opening up, she felt uneasy. “It’s not that I think what we have is perfect,” she says, “but sometimes, perfect is the enemy of the good.”
Ross says her fears have been borne out — and many other medical professionals who spoke to Nature agree that the ULC discussions so far have not been as productive as they would have liked.
One concern is a lack of scientific expertise. The ULC committee that will ultimately decide on the final text of the revised UDDA consists of 15 voting members, all of whom are attorneys, and none of whom has direct experience treating people with severe brain injury.
One of the commissioners is James Bopp Jr, who serves as the general counsel for the anti-abortion organization the National Right to Life Committee in Washington DC. He says that he publicly supported the UDDA in the 1980s, but has changed his mind in the past few years and no longer thinks that brain death constitutes biological death. He now argues that even if a person has no chance of recovery, they still have rights.
So far, Bopp’s efforts to remove brain death from the UDDA have not succeeded. But although the concept of brain death will probably remain in the United States, the ULC might approve bracketed text, which serves as an optional recommendation for state legislatures as they consider revising their laws. This bracketed text could include a clause similar to New Jersey’s current law, allowing people to object to a diagnosis of brain death for reasons such as religious beliefs.
Many agree that it’s important to include language to handle objections and accommodations, but allowing for such opt-out clauses in the UDDA has split researchers. Truog is in favour of them, adding that they are the only sure-fire way to stop the deluge of lawsuits that threatens to undermine public acceptance of brain death. But Ross says that consistency is paramount, so she would prefer that either no states have an opt-out clause, or every state has one — to avoid the situation in which someone is considered alive in one state but dead in another.
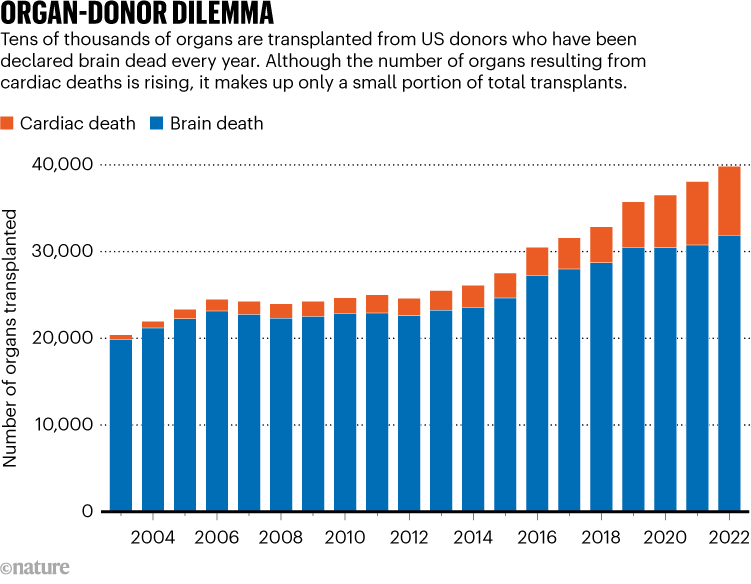
To add to the tension, people who are brain dead represent most deceased organ donors in the United States (see ‘Organ-donor dilemma’), meaning that any changes to how death is determined will also have knock-on effects on the organ waiting list — which currently stands at more than 100,000 people. The worry is that with more people refusing to accept a determination of brain death, the waiting list could grow substantially, and ICUs could be filled with people who will never recover.
Source: Organ Procurement and Transplantation Network (OPTN)
Truog says that New Jersey has had its opt-out clause for years, and it has neither massive organ shortages nor ICUs filled with people who are brain dead. But Capron cautions that expanding opt-outs for religious reasons to many states would be venturing into uncharted territory. And signalling that brain death isn’t universally accepted could “have an effect on people who would not have gone into it having any doubts”, he says. The logistics of organ transplantation also become sticky in this scenario: organ-transplant registries have become more national. Higher opt-out rates could pose an obstacle if one state’s population is providing fewer organs to the registry but still requires the same number, Ross says.
Exploring other options
The outcome of the UDDA revision process is still largely unknown. The ULC could recommend leaving the 1981 UDDA intact. In that scenario, individual state legislatures could still vote to revise their laws in any way that they see fit, but it would be without an explicit recommendation from the ULC. If drafting continues as planned, the full ULC will vote on the revised UDDA at its summer 2024 meeting.
Beyond revising the UDDA, there are other, more systemic, ways to build public trust in the concept of brain death, Paquette says. One example is more uniform and robust medical training: because brain-death determinations are relatively infrequent, many neurology residents in the United States finish their training without witnessing a single brain-death examination4. This can result in less uniformity between clinicians and poor communication with the family or carers of a person with a devastating brain injury. Students need more practice in communicating diagnoses and potential outcomes with the family or carers of a person with a devastating brain injury, Paquette says.
“It’s helpful to outline what the death based on neurologic criteria process will look like,” she says. “And it’s important to acknowledge that what someone is seeing might not match up with their notion of death.”
— Estate planning includes naming advocates in your key health and estate documents. But are your advocates truly prepared to make decisions on your behalf? Our expert shows what you need to do.
Going through the process of completing your estate planning documents is not an easy process. Working with an attorney to determine what documents you need, how you want the language written so that your assets are handled and decisions are made the way YOU want them, and choosing the best advocates to carry out those instructions can be very involved. No wonder it is a task that many people put off doing – it can be overwhelming!
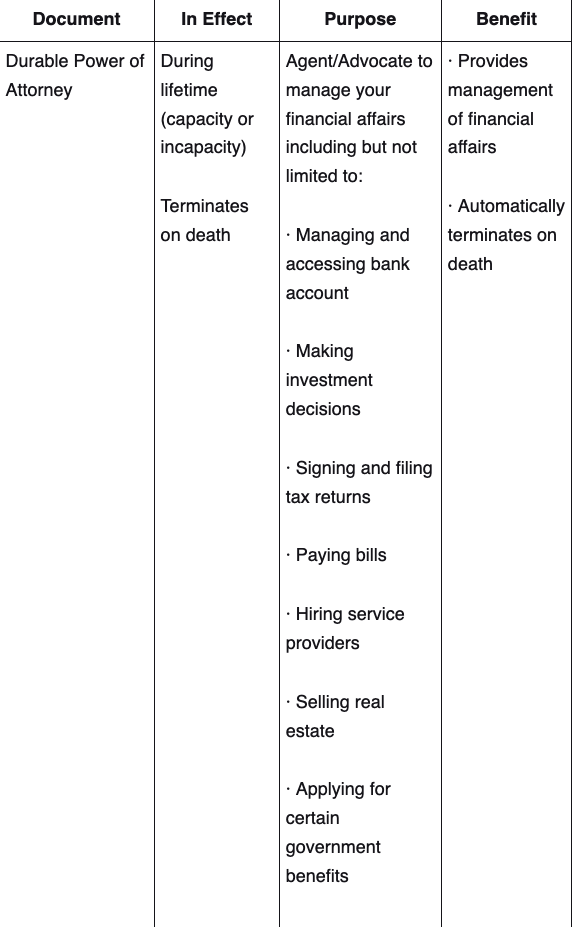
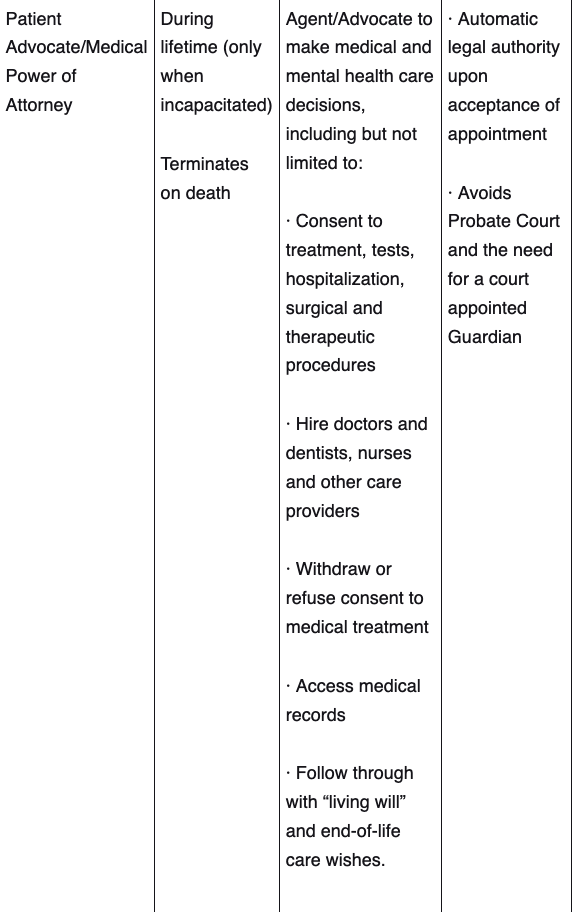
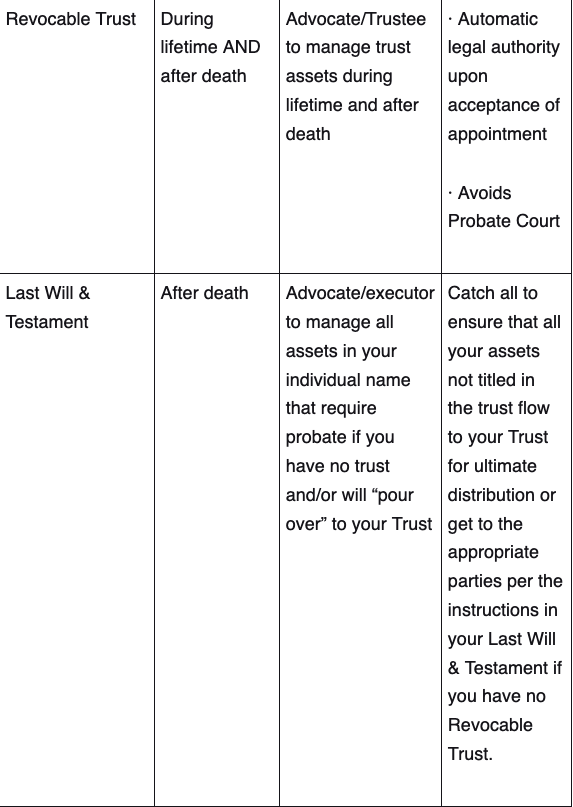
Common Documents With Named Advocates
The most common estate planning documents that individuals have drafted (and that will require advocates to be named) are the following:
Most clients are so relieved when their documents have been drafted; it is a huge weight off their shoulders to have so many important decisions made and in place. It feels satisfying to have the binder of documents drafted by the attorney in hand and completed.
Perhaps if you are even more “on the ball,” you follow through and get copies of your documents to your financial advisor and update your asset titling and beneficiaries according to the funding instructions provided by the attorney. If you have done that, you are ahead of the majority of clients, most of whom take the big binder home and file it away in a safe place and consider their estate planning completed! But is it?
Have you taken the final step and communicated to those you have chosen as your advocates that you have named them in your documents?
The Importance of Communicating With Your Advocates
It is not uncommon for people to name others as future advocates for them in their legal documents, but not to communicate to them that they have been named. If you’ve ever been in the shoes of being that named advocate, and getting that “surprise” call that you suddenly need to make a life and death decision about someone’s health treatment when you had no idea you were named as their health care advocate and had not had conversations with them regarding their wishes around end of life treatment, you might think differently about having those proactive conversations.
It is extremely important to take this last step, and not only communicate with your advocates that they have been named in your documents but also give them the key information that they will need to fulfill your wishes.
Here is the key information you need to share:
Patient Advocate/Health Care Advocate:
Drug allergies
Current medications (or where to find your medications list)
Your primary providers, your wishes on Code Status (i.e. DNR or full Code), and where your estate planning documents are located
Your past surgical history
Whether or not there is metal anywhere on your body
What your wishes are for end-of-life care and treatments (i.e. aggressive vs. comfort treatment)
Plans for future care and any professional relationships and resources that can be used to assist the advocate in their role (social workers, Geriatric Care Managers, etc.)
Durable Power of Attorney/Successor Trustee:
Contact information for your professional advisors and, if possible, an introduction to those professionals.
Instructions on where to find an “open me first” document (ex. Personal Financial Record System) that details your financial life (bank accounts, investment accounts, insurance policies, government benefits, employer benefits, etc.)
Where to find your estate planning documents and a review of your Trust (especially for your successor Trustee, so they have a heads-up on how they might be managing your assets)
An overview/general conversation about your wishes regarding handling your assets for future care and your values around money.
Executor/Advocate:
Contact information for your professional advisors and, if possible, an introduction to those professionals.
Instructions on where to find an “open me first” document (ex. Personal Financial Record System) that details your financial life (bank accounts, investment accounts, insurance policies, government benefits, employer benefits, etc.)
Instructions on where to find your Letter of Last Instruction document outlining your wishes for after death.
Where to find your estate planning documents, especially your Last Will & Testament, which will be the guiding document for your Executor.
An overview/general conversation about your wishes regarding after-death arrangements, about your Will, and how you would like your assets handled post-death, especially if there is no Trust for assets to flow to.
The more information you can share with your future advocates, the better prepared they will be to make the decisions you would want them to make on your behalf should they ever need to serve. An advocate’s job is to be your fiduciary, which means to make decisions in your best interest; without the benefit of having full information on you and your situation, you make it almost impossible for them to do their job to the best of their ability.
If you have taken the time to draft your estate planning documents, our best advice is to complete the process by fully preparing your advocates to serve in your best interest – they’ll be glad you did!
There are many ways people try to process and manage their grief, from talking with people close to them, to writing about their loss.
For others, immersing themselves in nature helps. But can taking a walk in a forest, going for a swim or setting out into the wilderness really help people work through their loss?
In a talk for Marie Curie, the Healing Power of Nature in Grief, TV presenter and survival instructor Ray Mears, author Raynor Winn and filmmaker Cat White shared their experiences of how nature provided them with comfort through grief – and how others might find comfort in it too.
1. Refocus and release
Most simply, nature can help people to take their mind off grief. When wild swimming, for example, “the shock to your system of cold water… you’re so cold that there’s nowhere else your brain can be at that moment in time,” says Cat, whose short film, Fifty-Four Days, reflected her real-life experience of daily swimming to process her grief.
And refocusing your attention on nature can also provide a sense of release. “When families go on journeys into wild places, it gives them a sort of release from the normal complexities of life,” says Ray.
“Even families with difficult relationships can be moved by being in a wild place where nature takes a hand in the events of the day. Time out from normal life can be very, very healing.”
2. A comforting sense of smallness
For many, grief can feel insurmountable. But nature’s vastness can provide an antidote. As Ray explains, in nature – particularly in wilder spaces – “you’re constantly reminded you aren’t the dominant force in that landscape.”
“I like to go to a very big wilderness and big forests where you feel absolutely tiny,” says Ray. Getting face-to-face with the scale of the natural world can be comforting because, as Raynor suggests, “nature puts things into perspective.” While this perspective won’t end our grief, it might help us manage it.
3. The importance of specific places
While the vastness of nature can help, finding specific meaningful places in nature can provide comfort too. For Ray, who spent time outdoors with people close to him who’ve died, “to be outdoors is to be forever reminded of them”.
Particular places can conjure specific memories and feelings. Ray suggests caution therefore, and a mindfulness to look after yourself when you’re grieving, because “unless you’re in the right frame of mind, it’s not easy to go there because the feeling is so profound”.
“But at the same time, it’s also warming. Those places and landscapes can be places to visit if you wish to visit those memories.”
4. Sharing in nature and grief
Like grief, nature belongs to everyone but is experienced individually. In the same way we share in nature – treading paths trodden before, swimming in lakes already swam in – sharing with others who are going through similar feelings can be helpful.
As Raynor explains, “Sometimes it’s enough to know that that place and feeling you’re inhabiting right now, you’re not alone because everyone who’s passed over that path has felt some element of what you’re feeling. There’s a sense of community within your isolation.”
As with grief, “anyone who spends time in nature… shares some sort of connection of knowing that they belong to something bigger and that you’re part of something with them”.
5. Nature’s endurance
Ultimately, grief is something we all experience. It’s a fact of life that people close to us will die. But nature’s longevity offers a different feeling: a sense of endurance. “Nature carries on when we think we can’t,” says Raynor. “If you allow yourself to experience that continuity of nature, it allows you to feel that’s possible within yourself.”
Its sense of endurance doesn’t mock our mortality; it helps us understand that we can carry on. As Cat explains, “Dawn will always come again. However overwhelmed we feel, nature has the possibility to remind us there will be another day and a sense of keeping going.”
Proximity, not prescription
Whether trekking through a forest or taking a stroll in a park, getting out in nature is one of the most straightforward strategies to help with bereavement. “It’s so accessible. And you don’t need a prescription,” says Ray, to walk through a park or go for a forest trek.
“You don’t need anything,” adds Cat. “It’s so easy. You need proximity – but that’s all you need.”
There are lots of ways you can get support when someone dies, from embracing nature to talking to someone.