It can be a tough conversation for most doctors: talking to a patient who is dying.
It can make many physicians uncomfortable, which is why they can benefit from training to help teach them how to talk to patients about death and dying.
One of these efforts has been put together by Anna-Gene O’Neal, who runs Alive Hospice in Tennessee, according to STAT. She launched the SHARE simulation lab last year that allows physicians and other clinicians to run though scenarios with actors, who play the part of patients.
For instance, a doctor interacts with a “patient” who has lung cancer and has undergone chemotherapy. When he tells her she doesn’t need more chemotherapy, she wonders if she has beaten the disease, but the doctor must tell her the cancer has metastasized and she has only six months or less to live.
The simulation is recorded and the video given to the doctor as a way to learn how to deal with patient emotions that include confusion, denial, anger and grief. O’Neal watches the tape with the doctors on a big-screen TV and encourages direct and honest communication with patients. Clinicians pay $350 to work through four scenarios and then watch the videos and get feedback. She recommends doctors:
Be aware of their body language. Look patients in the eye and focus on them.
Communicate like it’s a conversation. Become comfortable with long pauses after breaking difficult news to a patient.
Be direct with patients about their prognosis.
Hospitals and hospice programs are setting up training programs across the country. Stanford’s palliative medicine department has used similar techniques to train hospice nurses in California, STAT said. Oncologists at the University of Rochester Medical Center in New York observe other doctors having conversations with patients facing terminal illness. And in Arizona, administrators of Hospice of the West in Phoenix hold regular training sessions at staff meetings.
The Florida Hospital Association has also partnered with the Institute for Healthcare Improvement to provide hospitals and communities with training designed to generate end-of-life care discussions early on, according to Hospitals & Health Networks. Hospital training began in May and community training will get underway as part of the Conversation Project, which aims to help patients die in circumstances and surroundings that they choose.
The statistics show that more doctors are engaging in end-of-life counseling sessions with Medicare patients. In 2016, the first year doctors could charge Medicare for the service, nearly 14,000 providers billed almost $35 million—including nearly $16 million paid by Medicare—or advance care planning conversations for about 223,000 patients from January through June, according to data released from the Centers for Medicare & Medicaid Services.
It’s not just the pandemic. For citizens of a wealthy country, Americans of every age, at every income level, are unusually likely to die, from guns, drugs, cars, our bodies.
Last week, the National Center for Health Statistics alerted Americans to two facts about life and death in the U.S.
The first fact was sadly unsurprising: The coronavirus pandemic killed so many people that U.S. life expectancy fell from roughly 79 in 2019 to 76 in 2021—the largest two-year decline in nearly a century. The drop was sharpest among Native Americans and Alaska Natives, whose life expectancy fell to 65, close to the national average during World War II.
Life expectancy is perhaps the most important statistic on the planet, synthesizing a country’s scientific advances, policy errors, and social sins into a single number. The number is built on a weird hypothetical. The formula for life expectancy says: If Americans lived their entire life in one year—say, 2021—repeating it over and over again like an extended Groundhog Day experiment, how long would the typical person survive? It’s a useful exercise for the purpose of capturing one year’s conditions. But it imagines a life that nobody will ever live. U.S. life expectancy will almost certainly surge in 2022 and beyond, not only because the worst of the pandemic is over, but also because the disaster accelerated technology like mRNA vaccines that could raise life expectancy in future decades.
The second fact was perhaps more alarming: The U.S. fared worse in life expectancy than other high-income countries. While most of the developed world saw conditions improve in the second year of the pandemic, more Americans died of COVID after the introduction of the vaccines than before their invention.
Any explanation of this fact must begin with the American right’s bizarre rejection of the vaccines. During the Omicron wave, Americans were less likely to be vaccinated, less likely to be boosted, and significantly more likely to die of COVID than just about all peer nations. “People don’t think of blood-pressure medication as a political act, but due to the misinformation from some media and elected leaders, Americans saw vaccines as a political statement rather than a health decision,” says Joshua Sharfstein, a vice dean at the Johns Hopkins Bloomberg School of Public Health.
The American mortality mystery clearly goes much deeper than the pandemic, however. The U.S. suffers from a raft of local epidemics that have turned America into the death trap of the wealthy world.
Before the 1990s, average life expectancy in the U.S. was not much different than it was in Germany or the United Kingdom, as I’ve reported. But according to a paper comparing U.S. and European mortality, American babies are more likely to die before they turn 5; American teens are more likely to die before they turn 20; and American adults are more likely to die before they turn 65. “Europe has better life outcomes than the United States across the board, for white and Black people, in high-poverty areas and low-poverty areas,” says Hannes Schwandt, a Northwestern University economist and co-author of the paper. Despite our extraordinary wealth, innovation, and panoply of glittering appliances, Americans overall suffer from something like a lifelong death premium.
Some of the most immediate causes of America’s high death rate are guns, drugs, and cars. The U.S. has more guns and gun violence than any other rich country. We have more drug-overdose deaths than any other high-income country—both overall and on a per capita basis. Even before the pandemic, life expectancy in the U.S. declined for consecutive years in 2015 and 2016, largely because of the opioid epidemic and drug overdoses. The U.S. has a higher death rate from road accidents than Canada, Australia, Japan, South Korea, and the European Union. Even on a per-miles-driven basis, the U.S. still has a higher death rate than much of Europe.
So how can we fix the problem? In recent months, I’ve been researching an abundance agenda, and I can see at least two places where more abundance could, in a roundabout way, lead to more longevity: housing and preventative care. (I know, when all you have is a hammer, everything looks like a nail, but sometimes, nails really are everywhere.)
In the past few decades, the lack of housing in and near America’s most productive cities has pushed middle-class families farther away from the best-paying jobs. Among other things, this has increased commute times for people who drive to work. Americans are in their cars more than the citizens of any other OECD country, and the price of driving is paid in more than just vehicle deaths. The frequency of long commutes and the absence of walkable areas might explain why Americans are world leaders in the category of sitting on our butts. One pedometer analysis found that the typical American barely takes 5,000 steps a day. This was significantly fewer than residents of other countries in the study, including Australia (9,695 steps), Switzerland (9,650 steps), and Japan (7,168 steps).
When you combine all of this sitting with America’s array of calorie-dense food options, you get another feature of American exceptionalism: our obesity rates. At 40 percent among adults, the U.S. obesity rate is double the average of most European countries and eight times higher than Korea’s or Japan’s. Although the precise relationship between weight and health is contentious, the nonpartisan Commonwealth Fund has stated bluntly that America’s obesity levels are responsible for roughly one-fifth of deaths among American adults ages 40 to 85. One should neither reduce obesity to a function of walking nor reduce America’s sedentary lifestyle to its inability to build sufficient homes in and near urban areas. But more homes built near central business districts would likely reduce driving times and hopefully increase total aerobic activity.
If America’s housing shortage makes us less healthy, America’s doctor shortage ensures that treatable illnesses go unchecked and lead to more expensive cases. The U.S. has fewer general practitioners per capita than most rich countries, in part because our long and expensive medical education encourages doctors to become highly paid specialists. And along with this lack of affordable and accessible primary care, we have the highest rate of avoidable deaths of any rich nation. (Examples of the OECD’s definition of “avoidable” mortality include deaths related to alcohol, shootings, accidents, and influenza.) Expanding the number of primary-care physicians would reduce the chances of treatable conditions, such as moderate hypertension, blooming into costly maladies, such as heart disease.
This has all been quite gloomy, so let me end with two somewhat optimistic observations. The U.S. has world-class health care in some categories, such as cancer treatments. American men have the lowest rate of deaths from prostate cancer among rich countries, due in part to aggressive screening. And breast-cancer mortality rates are falling faster in the U.S. than in similar nations. These facts suggest that the U.S. is not utterly incompetent but rather selectivelycompetent, and that if we refocus our health-care policies on certain tangible outcomes, we can improve quickly.
Another stunning fact is that immigrants to the U.S. live as long, or longer, than just about any group of people in the world. In fact, foreign-born Americans live so much longer than native-born Americans—seven years longer for men, and 6.2 years longer for women—that immigration alone accounted for roughly half of America’s total life-expectancy gains from 2007 to 2017.
What’s this about? Maybe self-selection bias among immigrants makes them more conscientious than the typical native-born American. Maybe they are more likely to move to urban areas, like New York City, that have more walking, less smoking, and generally healthier behaviors. Maybe some combination of foreign-born habits and U.S. health-care coverage is a good formula for a long life. I truly don’t know. But I’d like to.
America’s unusually high mortality rate is our national shame. It ought to be our national obsession.
Grief and depression share similar symptoms, but each is a distinct experience. Making the distinction between the two is important for knowing how to treat and cope with your symptoms.
This article discusses the difference between grief and depression, focusing specifically on which symptoms overlap and which symptoms are different. It also presents the various treatment options that are commonly used to treat symptoms of depression and, in some cases, to treat the symptoms of grief.
Clinical Perspectives of Grief and Depression
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) removed a “bereavement exclusion” from the diagnosis of major depressive disorder (MDD).1 In the DSM-IV, the bereavement exclusion stated that someone who was in the first couple of months after the death of a loved one generally should not be diagnosed with MDD.
However, the DSM-5 recognizes that while grief and MDD are distinct, they can also coexist. What’s more, grief can sometimes trigger a major depressive episode, just as with other stressful experiences.2
Studies have shown that the extreme stress associated with grief can also trigger medical illnesses—such as heart disease, cancer, and the common cold—as well as psychiatric disorders like depression and anxiety.
In addition, the DSM-5 text revision (DSM-5-TR) added a new diagnosis for people experiencing extreme grief after one year of the death of a loved one. This condition is called prolonged grief disorder (PGD). It is considered a trauma– and stressor-related disorder.
PGD is marked by intense and distressing emotional pain and yearning for the lost loved one, thoughts that are preoccupied with the loss, disruption in one’s sense of identity, emotional numbness, and avoidance of reminders of the loss. PGD symptoms are disruptive to a person’s everyday functioning and ability to reintegrate into life.3
Given the similarities between grief and depression symptoms, there are times when it may be tricky to distinguish between the two. A better understanding of their similarities and differences can help.
Grief tends to decrease over time and occurs in waves that are triggered by thoughts or reminders of its cause. This is how it differs from depression, which is more pervasive and persistent throughout all situations.
In other words, a grieving person may feel relatively better in certain situations, such as when friends and family are around to support them. But triggers like the birthday of a deceased loved one or going to a wedding after having finalized a divorce could cause the feelings to resurface more strongly.
Depression, on the other hand, tends to be present no matter what the circumstances are. (An exception to this would be atypical depression, in which positive events can bring about an improvement in mood.4 A person with atypical depression, however, tends to exhibit symptoms that are the opposite of those commonly experienced with grief, such as sleeping excessively, eating more, and gaining weight.)
Additionally, grief usually causes a person to feel a longing for or an urge to see their lost loved one again; depression tends to result in the opposite. Someone with depression doesn’t necessarily feel the urge to do anything or see anyone.5
Grief
Intense sadness
Difficulty accepting that whatever caused the grief occurred
Excessive focus on the episode of grief or avoidance of it altogether
Thoughts of “joining” the deceased
Sensation of hearing or seeing things related to the loss
Anger and irritability can be potential signs of both grief and depression as well.
Treatment for Grief and Depression
There are treatment options for the symptoms of depression and grief. Of course, treatment varies based on a person’s unique circumstances. Be sure to consult with a doctor or mental health professional to discuss what options are best for you.
Therapy
Psychotherapy is a treatment option for both grief and depression. It can be greatly beneficial in helping you process what you are feeling and teach you strategies that can help you cope.6
Grief-specific cognitive behavioral therapy may be helpful for some people with prolonged grief disorder. This therapy method uses similar techniques as cognitive behavioral therapy (CBT), like reframing negative thoughts and learning healthy coping mechanisms. In addition, this type of therapy can help you learn how to maintain a healthy attachment to your lost loved one.7
Interpersonal psychotherapy (IPT) is a treatment method often used for depression but has the potential for treating complicated grief as well. IPT focuses on resolving symptoms, building up relationships, and getting involved in mood-boosting activities.8grief counseling made up of components of both CBT and IPT. In CGT sessions, you may repeat the story of how you lost your loved one as well as set personal goals for yourself and your relationships.9
Medication
Antidepressants are the most common class of medication prescribed to treat depression. Examples include:10
For someone experiencing extreme and disruptive symptoms of grief, a doctor might prescribe an antidepressant as well.
It’s most often recommended that for major depressive disorder, you complete a course of medication along with attending therapy sessions at the same time.
Support Groups
Social support can be a powerful tool when you are coping with symptoms of depression or symptoms of grief. Many mental health professionals recommend attending a support group of people who are experiencing similar challenges as you.11
>While the symptoms of grief and depression are similar, it’s important to talk to a doctor and/or mental health professional who can reach a diagnosis and help you pursue treatment options to cope with your symptoms. Remember, there is relief and there are resources that can help you heal.
Every person grieves differently and there is no right or wrong way to do it. Talk openly with a therapist or someone you trust, and remember that grief is not a sign of weakness.
Likewise, depression is an illness like any other. Reaching out for help when you experience depression symptoms is a sign of strength and can help get you on the road to effective treatment.
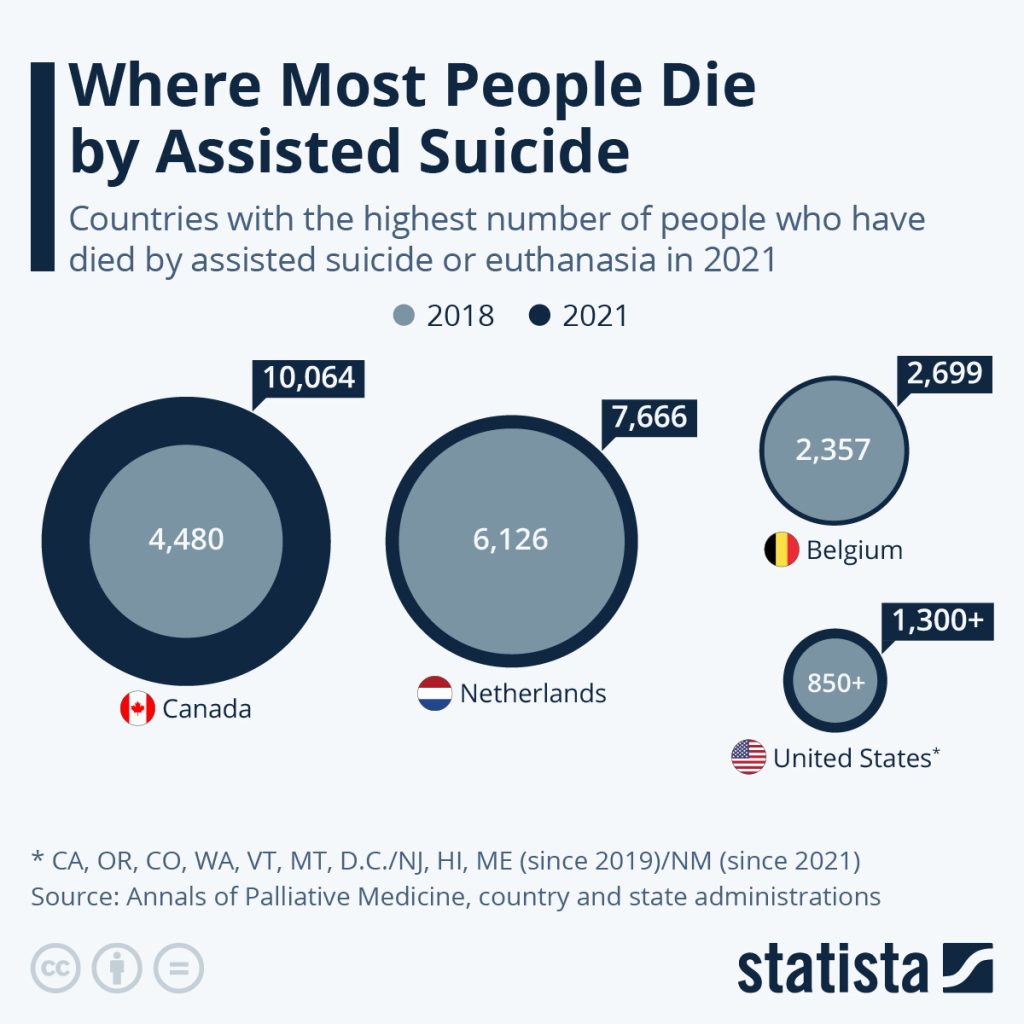
The Netherlands and Belgium which, like Canada, allow both have seen numbers rise more slowly. Assisted dying has been legal there since the early 2000s, however, while Canada legalized it in 2015 and has considered those who p have a disability but are not terminally ill for assisted dying since early 2021.
In 2021, assisted dying accounted for 3.3 percent of all deaths in Canada.
The United States also saw a faster rise in those dying by self-administered physician-assisted suicide over the past four years (euthanasia is not legal in the U.S.). This was also aided by the fact that four states – New Jersey, Hawaii, Maine and New Mexico – legalized it between 2018 and 2021, while two more populous ones, Colorado and California, started the practice in 2016.
Switzerland is another practitioner of physician-assisted suicide, but not euthanasia. 1,196 people died with assistance in the country in 2019, the latest year on record. Assisted dying is also legal or will become so soon in Luxembourg, Colombia, Spain, Austria, New Zealand and most Australian states.
The practice of both self-administered medication-assisted suicide and euthanasia – where a doctor administered deadly drugs upon request – have been legal in the Netherlands, Belgium and Luxembourg since the 2000s and has been practiced in Switzerland, which only allows the former, since the 1980s.
Colombia legalized euthanasia in 2015 and assisted suicide this year and both types also became legal in Canada in 2015.
In the past two years, Spain, Austria and New Zealand have made euthanasia and assisted suicide legal.
Similar laws also came into effect in several Australian states, starting with Victoria in 2019 and Western Australia in 2021. The remaining states in the country except for the Northern Territory will roll out these laws throughout the rest of 2022 and into 2023.
In the United States, the first states to legalize assisted suicide were Oregon in 1994, Washington in 2008, Montana in 2009 (via a state Supreme Court decision) and Vermont in 2013. The number of states who adopted the practice has risen recently, when it was legalized in California and Colorado in 2016, Hawaii, New Jersey and Maine in 2019 and New Mexico in 2021. Active euthanasia remains illegal in the country.
In Italy and Germany, national parliaments are currently grappling with legislating assisted dying after high court cases were decided in favor of proponents of the practice.
Creators of the services say their goal of providing easily accessible and organized help for people in distress has never been more necessary
By Sophia Laurenzi
What do you do after someone dies? Most people expect to deal with intense grief, but they might not realize how many logistical details arise after a death. Those tasks can feel overwhelming: deciding who to call, learning where to get death certificates, planning memorials and navigating finances.
“It’s so daunting … to figure out where to even start,” grief therapist and author Claire Bidwell Smith says. Bidwell Smith’s mother died when she was 18, and her father when she was 25.
Shortly before his death, he helped her make a checklist of all the things she would have to do: call the mortuary, Social Security and the bank; order this many death certificates; plan for what to do with his things. “I sat there with tears dripping down, being like, I don’t want to do this,” Bidwell Smith says. “But the minute he died, I was so grateful to have that list.”<
Now, new apps and websites with names such as Cake, Lantern and Empathy exist to help people navigate the tumult and confusion after a loss, offering tools that range from organized checklists for the early days of funeral planning to resources for later concerns such as closing a deceased person’s credit card account or finding a home for the deceased person’s pet.
The creators of these apps and websites say their goal of providing easily accessible and organized help for people in distress has never been more necessary. “The pandemic has increased people’s understanding of why this is important, as well as the actual need” for services, says Suelin Chen, who co-founded Cake in 2017.
Cake, which says 40 million people a year visit its website, provides a list of what tasks people need help with and then creates a checklist, along with offering guides to tasks like making an online memorial page for a loved one. The website hosts a library of thousands of articles related to death, including how to express condolences to a friend and how to plan an eco-friendly burial service. Cake, which is free to users, also provides help with other end-of-life needs, such as advice for talking to elderly parents or how to create a will.
The website Lantern, founded in 2018, and Empathy, founded in 2021, likewise provide guides on what tasks must be tackled after a death, with information about options at each step and timing.
Lantern, whose co-founder Liz Eddy was inspired to create the website after her grandmother died and ended up Googling what to do next, aims to be a one-stop resources for mourners. Among other things, it provides information about how to write a eulogy and “do an ash scattering ceremony,” and offers a list of “best funeral songs,” with traditional/religious, somber and joyful possibilities. Empathy’s “Obituary Writer” function, meanwhile, promises it “can craft a publication-ready tribute based on your answers to a few questions.” For a fee, it also offers one-on-one support from a professional after-loss consultant who essentially acts as a concierge for after-loss tasks.
“We connect people with services and give them tools, but a lot of it is really an education platform,” Eddy says.
Other companies are working to move beyond just providing information to creating tools that will handle some of the post-death logistical burden.
EstateGrid is working on building a service that will automate much of the bureaucratic aftermath of death. It starts with automated discovery of assets, liabilities and accounts, using the deceased person’s identity and death certificate to generate a list of what needs to be done. The platform will offer tiered levels of services, such as free tools and paid options, for the automation processes.
“Every life leaves a mess,” the website says, which also offers help in selling a house, finding investment accounts, appraising valuables and finding a new home for a pet.
The mobile app Empathy, which also features an easy-to-navigate checklist, offers premium services such as an obituary writer that promises to create a polished obituary based on the mourner answering a few questions. The paid option, which costs $8.99 for one month or $64.99 for a year, also includes tools that automate closing the deceased person’s accounts, memberships and subscriptions. The app uses software to pre-fill forms and streamline processes that usually take dozens of separate phone calls.
The companies are not just about logistics, however. They also include grief resources as part of their tools.
Experts say that makes sense. It’s hard to separate out logistics following a death and the grief people must deal with. The logistics “can be so overwhelming and terrifying, and actually sometimes get in the way of the grieving process,” psychologist Jordana Jacobs says. When the tasks that follow a death take up so much time and energy, it can shift focus away from grief, at least temporarily. As psychotherapist Megan Devine says, “Logistical support doesn’t change grief, but it reduces suffering.”
>Empathy provides grief meditations, journaling and chat support (which is another premium feature). Empathy co-founder Ron Gura says his company has focused on helping people dealing with both issues. “We don’t think you can decouple them,” he says.
The text-based company Grief Coach focuses on the emotions that follow a death, using advice from grief experts to send personalized texts to your phone. These messages — which range from describing breathing techniques to use when feeling overwhelmed to reminders that grief is not a linear process — are designed to provide extra help that family and friends often want to but don’t know how to give.
Founder Emma Payne created Grief Coach after her husband died by suicide and she stopped hearing from many friends and families. Ten years later, she went to a friend’s funeral and learned how devastated many of her people were to have lost touch: They just didn’t know what to say. Grief Coach costs $99 a year, which includes adding up to four friends and family members who also receive texts with suggestions on how they can support the grieving person, such as reminders of the deceased’s birthday.
Grief Coach does not replace human support; instead, it teaches grievers how to find and ask for support and helps their loved ones show up in meaningful ways. Experts say that logistical support from technology can be helpful as a stand-alone, but that digital grief support is best used as a supplement to personal support or therapy that is often needed to process and move forward from profound loss.
“My hesitation around technology is that we just have to make sure we don’t lose the intimacy inherent in what is healing about connection through grief,” Jacobs says. “We have to make sure we still make these technological products very human, because it is through that humanity … that we actually heal the most from loss.
Bidwell Smith, whose father made her that critical checklist, says she believes that even though technology cannot replace those healing connections, it can enable people to connect with each other.
“Grief is so lonely, and it can be very isolating,” she says, but she is encouraged to see people with similar experiences find each other in online communities like social media and new after-loss websites and apps. “I think anything where someone can feel more connected and less alone in what they’re going through is a good thing.”
There is no easy way to deal with what happens when a loved one dies. But by helping demystify essential tasks and offering resources for both logistics and grief, these digital services leaders say they hope they can help lift some of the burden off mourners, giving them a little more space to heal and connect with the support they need.
Alice Matthews helps palliative patients write their life story, sometimes with a “children’s book” version for their kids.
By Justine Toh
When we think of how we’ll be remembered after death, it may seem that simple words and basic descriptions don’t do us justice.
But for parents with a terminal illness and those on their deathbed, plain language is sometimes best.
“Dad was an artist. He painted the world that he saw. People loved his drawings.”
How else do you tell your life story — or explain death — to a young child?
Alice Matthews knows something of the challenge of putting a life into a story.
Since 2017, the SBS and ABC journalist has volunteered as a biographer with the Sacred Heart Community Palliative Care Biography Service based at St Vincent’s Hospital in Sydney.
The work involved sitting by the bedsides of the dying and, over a series of sessions, recording their stories.
For Alice, bearing witness to people’s lives, crying along with them, helping them grieve, reflect, and consider their legacy was an enormous privilege.
“We talk a lot in the service about holding space for someone,” she told RN’s Soul Search.
“There is an incredible spirituality in doing that, sitting with somebody, being with them and not really having to say or do anything except that.”
Death: the storybook version
Alice mostly saw elderly clients, part of a group often “shunted and pushed aside” by the wider world.
“What better way to return value to them than to sit and talk about their life and the value of their life which hadn’t disappeared,” she said.
Such clients often met their deaths with acceptance or comfort in their various religious and spiritual beliefs.
Others died “before their time”, as we would say.
If they had young children, Alice would put together a “storybook” version of their dying parent’s longer biography.
Some of the best-loved children’s books feature themes of loss and death.
For one client, a dad with a young daughter, Alice worked with the family to come up with a child-friendly “circle of life” explanation of death.
“I remember sitting in the room with them as the wife read it to her husband. That was one of the moments where we all sat there in tears,” Alice said.
“I didn’t know how he would react. He wasn’t verbal at that point.
“We waited a moment and then saw that he’d typed: ‘That was beautiful.’
“That was one of those moments where you feel the entire weight of the heartbreak — but also the relief.”
Once upon a time
Another writer who understands this struggle to give language to death is author Chloe Hooper.
Chloe’s partner Don Watson, the historian, author, and speechwriter, was diagnosed with an aggressive form of leukaemia in 2018. Things looked grim.
Then there was the uncertainty: how to explain his possible demise to their young sons — Tobias, then six, and Gabriel, three at the time.
Writing offered some comfort in the face of grief for author Chloe Hooper.
Few age-appropriate titles on the shelf seemed right. So, Chloe embarked on a quest to find the perfect book.
“The right story can help us find a path through the forest. It can help us take our straw and weave it into gold,” she said.
“Quite quickly, I realised that storytelling and perhaps re-storying this situation would be a way to help us through.
“The electricity and potential of ‘Once upon a time’ might be a way for us to light the dark.”
Chloe’s search for the best words to explain death — recounted in her book Bedtime Story — turned up the innumerable ways in which adults have explained death to children.
Grief and enchantment
Along the way, she made a surprising discovery: beloved children’s authors had suffered significant bereavement in their lives.
Roald Dahl, for one, described himself as “limp with despair” as he began writing Charlie and the Chocolate Factory after losing his seven-year-old daughter.
Dahl wasn’t alone. The Brothers Grimm, Hans Christian Andersen, J R R Tolkien, Frances Hodgson Burnett, C S Lewis, J K Rowling — death had touched them all.
Writer Roald Dahl was familiar with death, both in his personal life and in his children’s books.
Writing couldn’t overcome death, but it seemed a comfort in the face of it.
“It made me realise that an ingredient of enchantment is grief,” Chloe told me, referring to the often magical settings of the stories penned by those writers.
What she was looking for — the perfect story to tell her children about death — “was embedded in all of the stories that surround us.”
Mythic narratives similarly stalked the border between life and death, Chloe noticed.
Descent and return narratives saw characters like the Greek hero Odysseus — and even religious figures like Jesus Christ — descend to the dead before returning to the land of the living.
These stories, and their authors, couldn’t help but stray into spiritual territory.
For Tolkien, fairy tales were ultimately about escaping death. C S Lewis, author of the Narnia series, found himself a Christian after becoming convinced that the story of Jesus Christ’s death and resurrection was what Tolkien called a “true myth”: the fairy tale that came true.
‘Everything will be alright’
Plenty of people — including Chloe Hooper — are agnostic about that.
But every parent knows it’s their job to protect their kids. According to the late sociologist and theologian Peter Berger, “to become a parent is to take on the role of world-builder and world-protector”.
For Berger, this makes parents practically godlike.
Parents represent “the underlying order of the universe that it makes sense to trust,” he writes in A Rumor of Angels: Modern Society and the Rediscovery of the Supernatural.
Take the most basic parenting move: hushing a crying child in the dead of night. For Berger, when a mother rocks her bub, murmuring “Everything will be alright,” she relates to her child the way we imagine a god should relate to their creation.
Even the most ardent skeptic gets that a god’s job is to guarantee order and safety and beat back the encroaching darkness.
This casts new light on the stories we spin about death: from fairy tales to storybook versions of the “circle of life”.
What are these if not our attempts to love those we must eventually leave? Our efforts to weave out of the world’s sadness a life-giving spell?
Perhaps we’d rather not read the stories of our lives that get written on our deathbeds.
But even if such stories are prompted by the most decisive of endings, they pulse with love and concern for the living left behind.
Death doesn’t exactly get the last word because these stories are, in the end, about life.
Being honest and facing mixed emotions about a loved one’s death can help with healing
“All people are fallible humans, in life and in death, too. We disagree with one another and we don’t always get along. But there is always a possibility to get it right when both people are alive. We lose that opportunity when someone dies. We lose the chance for closure.”
Jacalyn Wetzel, a writer and therapist from Mississippi, recently lost her father. Wetzel describes her relationship with her father as complicated, so it is not surprising that her emotions surrounding his passing are complicated, too.
Wetzel explains, “Growing up, I had a lot of resentment towards him. My dad made many missteps in his own life and his choices hurt me. When I was an adult, things started to turn around, especially in the last two years. He showed more often than not that he was trying to fill the cracks he had left from years before.”
“Grief is even more complicated when everything between you wasn’t rainbows and sunshine.”
Losing a loved one is always hard. It doesn’t matter if the relationship was good, difficult or a combination. Rebecca Soffer, who runs the website Modern Loss (and wrote a book of the same name), explains, “All people are fallible humans, in life and in death, too. We disagree with one another, we argue, and we don’t always get along. But there is always a possibility to get it right when both people are alive. We lose that opportunity when someone dies. We lose the chance for closure.”
Adds Wetzel, “Grief is even more complicated when everything between you wasn’t rainbows and sunshine. It’s still grief, just the same.”
As a point of clarification, the term “complicated grief” is used to describe a disorder where a person experiences long-standing grief where feelings of grief do not dissipate over time and are debilitating. This article focuses on grief when the relationship itself is complicated.
Fear of Honest Reflection
Psychiatrist Gail Saltz, associate professor of psychiatry at the New York-Presbyterian Hospital Weill-Cornell School of Medicine and host of the “How Can I Help?” podcast, explains, “Funerals are for paying respect to someone. These rituals are about giving comfort and support to the mourners.”
People rarely delve into the complexities of a relationship, especially when speaking publicly about a deceased loved one. We have been taught not to speak ill of the dead, so in general, eulogies are focused on discussing the deceased’s best qualities and sharing stories that put them in a good light.
Saltz says, “What is said at a memorial is not going to give a clear picture of the total person.”
But most relationships are not all good but rather multi-dimensional, especially between family members. Some relationships are fraught or even toxic. Because of the differences in situations, so, too, may be a person’s reaction to the loss.
No Rules for Grief
“Different circumstances can lead to different emotions surrounding death,” explains Saltz. “Many people think grief is just about being sad. But you can also feel a range of other emotions including guilty, perturbed, lonely or ambivalent.”
“The idea that there are five stages of grief that happen consecutively and for a specific amount of time is misguided,” says Soffer. “Grief isn’t organized; it’s a mess and a natural human experience. There is no ‘normal’ way to grieve.”
The idea that there is a correct way to grieve can impede the healing process. Well-meaning friends and family can make people feel judged about how they are grieving or comment on how a person “should” feel rather than listening to the person’s feelings.
“Many people have a picture in their mind of what a mother/daughter or sister relationship should look like,” explains Saltz. “But all relationships are individual. If a person had conflicted feelings about a person when they were alive, they will probably continue to have mixed feelings when they are gone.”
“Whether tears fall or not, it doesn’t mean there wasn’t love there. Love is just as complicated as grief and people aren’t perfect.”
Wetzel recalls that when her stepfather passed away several years ago, some people commented, “Well, he is only your stepfather” or “You are lucky you still have your real father.” The comments stung.
Wetzel says, “My stepfather raised me from the time I was a little kid. In many ways he was more of a father to me than my biological father had been. Although people didn’t mean it, these types of comments upset me.”
Conversely, Wetzel has been made to feel she isn’t grieving enough for her biological dad, especially by his extended family. She herself says she has been waiting for the “dam to break” and is starting to wonder if it ever will.
“I try not to judge myself, “says Wetzel. “Whether tears fall or not, it doesn’t mean there wasn’t love there. Love is just as complicated as grief and people aren’t perfect.”
Safe Space to Grieve
Soffer believes people do themselves a disservice when they don’t allow themselves to fully face all of their mixed emotions about the person and what has been lost.
“It can be lonely when you hide your true feelings or are afraid to speak openly for fear of being judged. Honest reflection can help us learn, build and move forward healthily,” she says.
Well-meaning family and friends can be helpful, but they may also be biased. “People who know you or knew the deceased may have pre-existing beliefs about the relationship or the person,” says Soffer. “If they aren’t able to offer you space where you can speak honestly without judgment, it may be better to seek grief support elsewhere.”
Finding a safe space to share your feelings is key to healing. Peer-to-peer grief support groups (in-person and online) and professional grief counselors are great options. “With a grief counselor, the grief discussed is ‘yours only,’ and you don’t have to worry about another person’s feelings,” explains Soffer. “It may take a few tries to find the right grief counselor, a person you are comfortable talking to about the tough stuff.”
For Wetzel, telling her story on social media proved cathartic. “I have always tried to be real and honest with my followers,” she says. “I needed to explain my absence, so I shared that my father had passed. But then I was getting a lot of condolences which made me feel the need to be transparent about our relationship and my conflicted feelings of grief.”
Wetzel found most people appreciated her candor and many expressed having been in similar situations. “At the time, I was feeling guilty and alone. It was helpful to know others had gone through the same type of experience,” she says.