For people who have recently lost a loved one, humour can trigger episodes of intense grief–but it can also help in the recovery process, according to a new study.
A University of Alberta study uncovers an often-overlooked trigger for both grief and healing in people coping with the loss of a loved one.
By Gillian Rutherford
When Donna Wilson pulled up to visit her aunt and uncle on their farm near Eatonia, Sask., a few years ago, she came across a comical scene: Her uncle Doug was running around the yard chasing turkeys. The birds kept jumping up on his dog and he was trying to shoo them away with a broom.
It’s a memory Wilson plans to remind her aunt Doreen of soon. Doug died over the winter, and her aunt is grieving. Wilson hopes that sharing a funny story about him will help them both.
“I loved my uncle Doug, and I remember he was always smiling and laughing about something,” said Wilson. “Hopefully we will laugh together and it will be healing.”
Wilson, a nursing professor at the University of Alberta, recently published study findings that show humour can trigger moments of intense grief for people who have recently lost a loved one, but humour can also be helpful in the recovery process.
The key–as always with humour–is timing, plus you’ve got to know your audience, says Wilson.
The study was part of a larger inquiry into grief triggers–thoughts, memories, or events like anniversaries and family gatherings, special places, songs, even jokes. Very little research has been done on triggers and how bereaved people manage them, Wilson says, but they can be incapacitating.
“You can be driving past the hospital where your husband died, and suddenly have a massive grief trigger and have to pull over,” she said. “Now think about if that’s a pilot who’s flying a plane, or a surgeon, or a truck driver going down the highway.”
Working through the stages of grief
Researchers report there are nearly 300,000 deaths each year in Canada and on average 10 people grieve each death. For the study, Wilson and her team did in-depth interviews with 10 middle-aged and older Canadians who had lost a parent, child, sibling or spouse within the past two years, asking about their experiences with grief and recovery.
They all described being completely overwhelmed by grief at first, then being frequently hit by “hard-grief” triggers. Most found a way to reshape their lives without the loved one after about a year, and over the next year they were able to welcome good memories of the deceased person without triggered episodes of crying or extreme sadness. Eight of the 10 interview subjects said humour helped with their recovery.
“I think nobody realized humour is present for our mental health, even in grief,” said Begoña Errasti-Ibarrondo, associate professor with the University of Navarra and a visiting academic at the U of A. “In Spain, for example, at funerals sometimes we make jokes if it is appropriate and we tell funny stories about the person or the tricks they used to play.”
“Humour is what made it possible for me to live,” said one interview subject quoted in the paper. “I looked forward to the times I could laugh or smile; I could get a break from my grief.”
Researchers say when you are supporting someone who is grieving it is important to talk to them about the person who died. However, they caution it’s best to check first with the bereaved person before turning to humour, as some may not be ready or may find it inappropriate.
“Grief is very personal and so is humour,” said Errasti-Ibarrondo.
The saying “laughter is the best medicine” dates back to the King James Bible, originally published in 1611. We now know laughter releases endorphins and positive hormones that contribute to physical and mental health.
For her part, Wilson will continue to remember how her uncle Doug liked to use humour to cope with the frustrations of daily life. Once he was planning to take his family out for a drive when he noticed one of his car tires was deflated. “Well, at least it’s only flat on one side,” he told them with a laugh.
On a literal level, it should be impossible to make sense of someone saying “I’m dead” unless you’re attending a successful séance. Yet here we are in 2022, not only proclaiming our own expiration but reveling in it. Far from speech beyond the grave, “I’m dead” has come to communicate one of the highest pleasures of life: the giddy throes of uncontrollable laughter. When someone says “I’m dead” or even just “dead” in 2022, they’re telling you that they couldn’t be more tickled by what just happened. So how did being dead become a good thing?
Death and laughter have been strange bedfellows since ancient Greece, where, legend has it, the fifth-century-B.C. painter Zeuxis died from laughing at the portrait he was painting of a supposedly ugly old woman—a hilarious anecdote later immortalized in an equally hilarious painting by the Dutch master Arent De Gelder. And Zeuxis’s isn’t the only classically depicted death by laughter. The Stoic philosopher Chrysippus, by several accounts, kicked the bucket because he couldn’t stop laughing after witnessing a donkey eating his figs. Bizarrely, King Martin I of Aragon is said to have died laughing at a joke also concerning an animal eating figs. Legends of giggly demises litter history; as recently as 1989, a Danish audiologist is said to have passed away guffawing during a screening of A Fish Called Wanda. Apparently, the best medicine is also sometimes the sweetest poison. Although I admit it would be a great way to go, I myself will be avoiding all zoo-adjacent fig farms in the near future out of an abundance of caution.
The connection between death and laughter was consummated in English by—who else?—Shakespeare. In his comedy The Taming of the Shrew, after the exit of the vivacious and eccentric couple Petruchio and Katharine, Petruchio’s servant, Grumio, says, “Went they not quickly, I should die with laughing.” From then on, the phrase to die laughing was part of the language as a hyperbolic idiom—we all know it’s an exaggeration, but something within the fiction rings true to our relationship with laughter and death. The fatal violence of hilarity proliferated in English over the following centuries. From the 1930s slang to bust a gut to the idea of being “in stitches” to the ironic Catcher in the Rye Holden Caulfield–ism “That killed me,” there’s something about the experience of uncontrollable laughing that seems to put us into close contact with our inevitable nonexistence.
And it makes sense. Intense laughter expresses itself in violent convulsions and temporary loss of bodily control. Who among us hasn’t been part of a tickle-fest that verged on sadomasochistic brutality? Times when I laugh so hard that I cry can feel like an out-of-body experience—a sublime mania that temporarily relieves me of the burden of consciousness. Perhaps we say “I’m dead” because we’ve intuited that deep and frenzied laughter gives us a taste of the eternal unknown toward which we’re all always hurdling. This sense of comatose comicality yielded our Friday-level clue “That’s so funny I can’t even function.”
The central goal of right-to-die organisations has not changed much over the past 150 years. In 1872 a British writer, Samuel D. Williams, wrote a book advocating the use of the novel anaesthetic chloroform to give patients “a quick and painless death”. In 1931 the British eugenicist Dr Killick Millard proposed legalisation of euthanasia “to substitute for the slow and painful death a quick and painless one”.
Now that legalisation has arrived, however, doctors have realised that a Q&P death is easier said than done.
Writing in a recent issue of The Spectator (UK) Dr Joel Zivot, a Georgia physician, expresses his doubts about whether lethal medications are the way forward. He studied the autopsy reports of more than 200 prisoners executed with lethal injections and found that many may have died in great pain.
“The death penalty is not the same as assisted dying, of course. Executions are meant to be punishment; euthanasia is about relief from suffering. Yet for both euthanasia and executions, paralytic drugs are used. These drugs, given in high enough doses, mean that a patient cannot move a muscle, cannot express any outward or visible sign of pain. But that doesn’t mean that he or she is free from suffering.”
Dr Zivot believes that pentobarbital, which, it seems, is used in Oregon in 4 out of 5 assisted suicides, caused pulmonary oedema – the lungs fill with liquid secretions and the person can die in agony. “Advocates of assisted dying owe a duty to the public to be truthful about the details of killing and dying. People who want to die deserve to know that they may end up drowning, not just falling asleep,” he writes.
Nor is death necessarily quick.
In Oregon, where statistics are gathered about the mode of death, the median time to death throughout the 23 years of the Act is 30 minutes but the maximum time is 4 days and 8 hours. The median time for people to fall unconscious is 5 minutes, the maximum is 6 hours.
At least in the United States, doctors who participate in assisted suicides are aware of these issues. Dr Lonny Shavelson, a California physician who specialises in this novel field, has helped to organise the American Clinicians Academy on Medical Aid in Dying. This provides a forum for doctors to establish a best-practice for helping people to die.
It turns out that the very diseases from which the patients suffer can make the drugs less effective. Dr Shavelson spoke with Medical Xpress last year about some of the difficulties:
“Shavelson and [his colleague retired anesthesiologist Dr Carol] Parrot have identified which patients are more likely to linger, and can recommend adjustments. People with gastrointestinal cancer, for example, don’t absorb the drugs as well. Former opiate users often have resistance to some of the drugs. Young people and athletes tend to have stronger hearts and can survive longer with low respiration rates.
“We’re learning. Hypothesis, data and confirmation. This is what science is,” he said. “Our job is to stop the heart; that’s what they want us to do.”
An art installation by Suzanne Brennan Firstenberg in remembrance of Americans who have died of COVID-19, near the Washington Monument in Washington, D.C.
The numbers paint a clear picture of devastation, though they can’t capture the individual and familial pain of losing loved ones – which will no doubt transform many more millions of Americans’ lives.
The impact of this mass death on American society as a whole is less clear, especially since the pandemic is not over. While there have been a few moments of public remembrance – 700,000 white flags placed on the National Mall, and President Joe Biden’s brief words noting the “one million empty chairs around the dinner table” – the country is only beginning to grapple with the shared grief of so many deaths.
Instead, there is public discord surrounding those who died. In a country divided over basic facts about the virus, deaths have been exploited for political purposes, or wrapped into conspiracy theories.
As a scholar of religion who has studied the history of death in America, I am quite preoccupied with how the country makes sense of, honors and remembers the COVID-19 dead. The magnitude of death today immediately brings to my mind the event that killed the second-highest number of Americans: the Civil War.
My first book, “The Sacred Remains,” looked at the conflict’s impact on Americans’ attitudes toward death, during another period of extreme division and overwhelming loss of life.
The unprecedented death toll had profound consequences on American cultures of death for generations, particularly through the emergence of the funeral industry.
Throughout the 19th century, most Americans died, and had their bodies tended to, at home. Last moments with the corpse were with loved ones, who were responsible for washing and preparing it for the final rituals before burial, generally in local churchyards.
But the Civil War provided an opportunity for a game-changing development. Embalming was an innovative method of preserving bodies that allowed some Northern families to have their war dead retrieved from the mostly Southern battlefields and brought back to be buried in Northern soil.
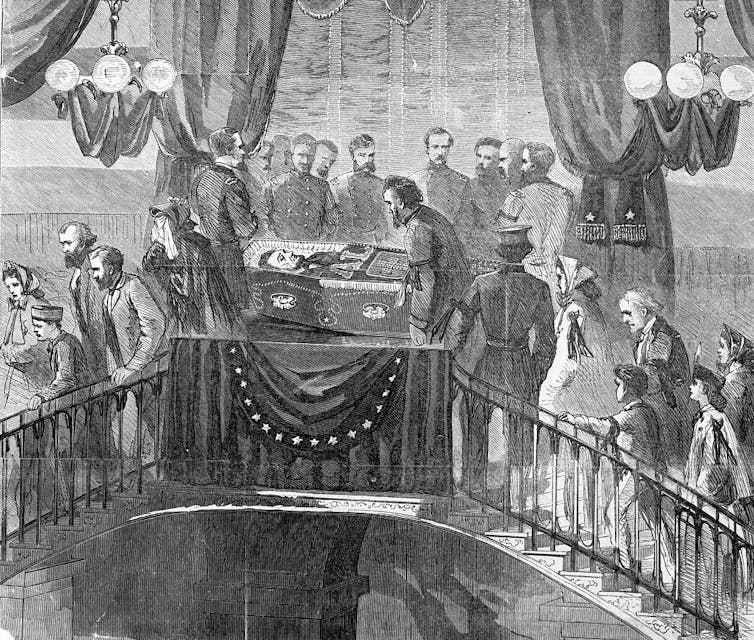
The display of President Abraham Lincoln’s embalmed body after his assassination was a pivotal moment in this transformation. His corpse was transported on a train from Washington, D.C., to Springfield, Illinois, with frequent stops in many Northern cities where it was put on display for grieving Americans.
A drawing depicts Americans viewing Abraham Lincoln’s body at City Hall in New York City in 1865.
As embalming became more common, it helped legitimize a new class of professional experts: funeral directors, whose homes became a mix of business, mortality, religion and their own domestic life. By the early 20th century, this new business had established a fairly standard American way of death, centered on the viewing of an embalmed body to bring a community together.
Americans’ relationship to their dead would never be the same. The intimacies the living had with the dead before the Civil War gradually disappeared, as funeral homes managed the care of more and more bodies.
Meaning-making
One of my intellectual heroes, sociologist Robert Hertz, wrote a famous essay about death and society in 1907. He argued that social groups represent themselves as immortal, capable of overcoming the death of any member. The community’s survival depends greatly on transcending death, so it transforms the dead into sacred symbols of group identity and social cohesion.
Hertz’s studies focused on death in small societies in Borneo. Yet his exploration of the relationship between the death of the individual and the life of the social group is pertinent now, in the context of the pandemic – as it was in the aftermath of the Civil War.
The victorious Union turned dead soldiers into symbols of the nation. Their deaths were seen as sacred sacrifices to preserve the country. For religion scholars, this is a clear example of American civil religion. In the U.S., civil religion is a patriotic culture that sees America as a sacred, exceptional country, built on shared ideals, myths and traditions.
But the Northern victors did not “control the narrative,” as we say these days. Indeed, a very striking and still-present counternarrative soon developed among the vanquished Confederates after the war. The losers built an alternative civil religious culture, what historians refer to as “the religion of the Lost Cause.”
Daughters of the Confederacy unveil the ‘Southern Cross’ monument at Arlington, Va., in 1917.
For many white Southerners, the battlefield dead did not signal God had abandoned their cause but rather illuminated his support for values associated with the Confederacy – values the United States is still grappling with today. They saw the loss as a temporary setback, but believed that ultimate victory would come if they maintained some form of Southern cultural purity based on notions of racial, regional and religious superiority.
Looking ahead
The politicization of death is not uncommon in American history, particularly during times of profound social crisis. And since the start of the pandemic, the same has happened with COVID-19 victims.
Death during a pandemic is obviously different from death during a civil war. In both cases, however, it is difficult for a divided country to experience unity in the face of an enormous loss of life and to agree on what those deaths mean for the nation.
Unique aspects of the pandemic make national mourning, and united healing, even more complicated. For example, the virus has not taken an equal toll across the country. The death toll shows significant disparities among different economic and racial groups. And the need to prevent contagion has intensified the physical separation between the living and the dead, making some meaningful rites of mourning difficult or impossible.
Many communities have made efforts to commemorate the pain of the pandemic, such as through Dia de los Muertos, a Mexican holiday honoring those who have died. But there have been minimal efforts to help make sense of the deaths on a national level: to rally around a compelling public narrative about the tremendous loss of life and grief. It remains to be seen if Americans will eventually incorporate the losses into a unifying civil religion, or only use them to reinforce polarization.
One million dead and counting will certainly require more efforts, more reflection and more soul-searching to help American society overcome and indeed draw strength from this unimaginable number.
A small Colorado town maintains the country’s only public outdoor funeral pyre. Philip Incao saw it as his own perfect ending.
The cremation of Dr. Philip Incao at the country’s only public open-air funeral pyre in his adopted hometown, Crestone, Colo. His shrouded body was laid on a metal grate and covered completely with wood.
Philip Incao was about 6 years old when he asked his mother if it was true he would die. Yes, she replied. And what happens afterward? he asked.
“Nothing,” she said. “You just die, that’s all.”
It was a profoundly unsatisfying answer, and one that Dr. Incao later identified as the starting point for a lifetime of study.
He pursued a path that wound through medical school, training in holistic healing and devotion to the early 20th-century esoteric Rudolf Steiner, a polymath who theorized that the spiritual world could be explored through scientific methods.
Decades of searching led him all the way to an unconventional decision about what would happen to his body after his death.
Before Dr. Incao died of prostate cancer on Feb. 28 at age 81, he arranged for a cremation in his adopted hometown, Crestone, Colo., at the country’s only public open-air funeral pyre.
“All the old forms, all the old rituals, are being loosened up,” he explained in interviews in the months before his death. And through this type of cremation, he planned to be a part of that shift.
He knew his body would be wrapped into a simple shroud, carried on a wooden stretcher into an enclosure, and placed on a platform a few feet from the ground. His sons and his wife would light the fire and watch his body burn for several hours. The next day, they would collect the ashes. He had attended several cremations at the pyre, and he was ready.
Dr. Incao’s family members carried his body to the pyre.The pyre itself is a utilitarian structure: two waist-high stuccoed concrete walls lined inside with firebrick, and spanned by a plain metal grate.
About 70 people have been cremated at the pyre in Crestone since it opened more than a decade ago. Its services are restricted to residents and landowners in Saguache County, with a population of less than 7,000 people spread across some 3,000 square miles.
Set inside a circular wooden fence a few miles out of town, with the Sangre de Cristo range of the Rocky Mountains looming in the background, the pyre itself is a utilitarian structure: two waist-high stuccoed concrete walls lined inside with firebrick, and spanned by a plain metal grate.
The simple design represents a defiant upending of American death rituals. Instead of a body being whisked away by a funeral home, it stays on view at home for several days. And rather than being chemically “preserved” and placed in a sealed coffin, it remains on ice, but otherwise in its natural state.
“Burial as a practice in the U.S. is basically designed so that the American family doesn’t have to deal with the dying,” Dr. Incao reflected in December. By then, he was mostly confined to his bed, where he rested, met with friends, sorted through his belongings, and read books about reincarnation and near-death experiences.
More than half of Americans are cremated after death, a remarkable change from the 20th century, when it was “completely against American sensibilities,” said Gary Laderman, a professor in the department of religion at Emory University. But Crestone’s approach goes even further, defying one of traditional cremation’s core promises, to make the body disappear quickly and invisibly. A body on the pyre turns into ash and smoke while friends and family keep vigil for hours under the open sky.
Community cremation sites are commonplace in some parts of India, but they remain taboo in the United States. A Buddhist retreat center in northern Colorado maintains a private pyre, but efforts to open public sites like Crestone’s have faltered, running up against squeamish cultural sensibilities about death.
“Burial as a practice in the U.S. is basically designed so that the American family doesn’t have to deal with the dying,” Dr. Incao reflected in December.Dr. Incao spent his life exploring the teachings of Rudolf Steiner, which guided his interest in philosophy and spirituality as well as his approach to his medical career.
“Folks who haven’t had direct experience of open-air cremation, whether it’s in Colorado or in Asia, can have some pretty strange associations,” said Angela Lutzenberger, a hospice chaplain who bought 63 acres of land in Dresden, Maine, that she hopes to turn into a pyre site. “They build up creepy ideas about what it could be.”
It is not a coincidence that Crestone is the pyre’s home. About 200 miles south of Denver, the former gold mining town has attracted a population drawn to Eastern religious practices and wisdom traditions for decades. Its reputation solidified in the 1980s, when a Danish-born spiritual seeker and her oil magnate husband established a sprawling development just outside town that bills itself as the “largest intentional, interreligious and sustainable living community in North America.”
The winding roads around that development — with street names like Serene Way and Jubilant Way — lead to several towering Buddhist shrines, retreat centers and a spiral ziggurat commissioned in the 1970s by the father of Jordan’s Queen Noor. Some locals refer to a “vortex” of energy in the area.
“There’s no other place quite like this in America,” said Dr. Incao’s son Sylvan, who visited his father there often over the years.
Sylvan had come to Crestone on a chilly week in March that would culminate in his father’s cremation. Fliers with information about the ceremony were posted at the health food store and the cafe next door, which function as the town’s social center. “Please carpool whenever possible,” the flier read. “Pyre lit at 8 AM.”
Bruce Becker, left, and Noah Baen, treasurer of the Crestone End of Life Project, stood in the smoke during Dr. Incao’s cremation.Credit…A vista of the San Luis Valley above Crestone.
Dr. Incao had moved to Crestone with his second wife, Jennifer, in 2006, after practicing “anthroposophic” medicine — a Steiner-inspired holistic approach that many mainstream physicians characterize as pseudoscience — in upstate New York and Denver.
Dr. Incao graduated from the Albert Einstein College of Medicine in New York City, but his career radically changed course when he was introduced to alternative medicine and Steiner’s work. Steiner lectured widely on topics including philosophy, Christianity, finance, architecture and art. His ideas about education led to the Waldorf school movement; his thinking on agriculture inspired biodynamic farming.
Steiner’s view of medicine was a revelation for Dr. Incao. He went on to spend his life exploring the teachings of Steiner, whose work guided not just his interest in philosophy and spirituality but his medical career.
He believed in reincarnation, which he felt gave a sense of purpose to life. And he was devoted to the idea of what he considered a “natural” approach to medicine.
For Dr. Incao, that meant choices that would seem extreme to many, even some members of his family. He strongly opposed vaccination, publishing articles and offering testimony against childhood vaccines and eventually opposing the Covid-19 shots. When he became sick, he declined traditional treatments for his cancer, including chemotherapy. He was at home in Crestone, where many residents are skeptical of traditional medicine.
Dr. Incao believed that the moment of death was just the beginning of “the process of separation of the human identity,” which he said took about three days.
And why be cremated outdoors? “You do it because it makes a lot more sense than the alternative, which is giving the body over to the undertaker,” he said. He decided on cremation after moving to Crestone, and officially signed up about four years ago.
Sylvan, 49, and his brother Sebastian, 47, supported their father’s plans, which they saw as in keeping with his spiritual sensibility and nonconformist streak. “He loved nature,” said Sebastian, an acupuncturist in New York. “It seemed like a very powerful way to liberate his spirit.”
Sebastian, right, and Sylvan supported their father’s plans, which they saw as in keeping with his spiritual sensibility and nonconformist streak.Stacks of cedar are carried to the clay oven.
Their older brother, Quentin, 51, was not so sure. He knew his father was a nonconformist, but he was still shocked when Dr. Incao told him about his intentions, on one of Quentin’s visits from his home in Montana. “It just didn’t make sense to me, I couldn’t understand it,” he recalled. He had agreed to be a pallbearer, but he was dreading the action of physically placing his father’s body on the pyre.
At a memorial service a few days before the cremation, the three brothers, their families and others gathered in Jennifer’s backyard art studio for a ceremony and eulogy delivered by a priest from the Christian Community, a small religious movement inspired by Steiner.
Dr. Incao’s body lay in repose at the front of the room, with wreaths of fresh carnations and other flowers on his body. “Into the calm of soul being walks the soul of our dear Philip,” the priest said, reading from a hand-transcribed book of sacred texts. “He is now on the other side of the threshold but his love has not stopped.” At the small outdoor reception afterward, deer grazed in the yard.
“It’s one of the most beautiful volunteer activities,” said Fane Burman, who has assisted at about a dozen cremations, helping stack the wood and tending to it as it burns. The nonprofit that operates the pyre, the Crestone End of Life Project, provides about a dozen local volunteers for each cremation. Although Mr. Burman does not always know the person who has died, “once the fire gets burning it brings tears to my eyes.”
Funeral guests delivered offerings of flowers and juniper boughs atop Dr. Incao’s body.About 70 people have been cremated at the pyre in Crestone since it opened more than a decade ago.
On a cool Saturday, the family gathered at 7 a.m. to accompany Dr. Incao’s body from his home to the pyre about four miles west. A volunteer had wrapped the body in a shroud of sheets the night before and covered it in roses. The stretcher was carefully loaded into the back of Sylvan’s black pickup truck, and Quentin and Sebastian rode in the back with their father — “our last moments with him,” Quentin said. The truck slowly turned right at a small hand-painted sign reading “Pyre.”
By 7:30 a.m., about 70 people lined the path into the pyre site. A volunteer rang a bell to signify the start of the ceremony, and another played a tune on his handmade flute as the procession wound its way to the inside of the fence. The pallbearers laid the stretcher on the metal grate.
Dr. Incao’s ceremony began with family members and friends laying juniper branches and flowers on the body. Incense burned in a terra cotta pot tended by a volunteer, while others added logs until they were piled above the rim of the pyre. Then Jennifer and Dr. Incao’s sons lit large sticks in the incense pot and ignited the pyre together.
As the fire started to burn, Sylvan put his arm around Sebastian. A harpist played a tune as the flames crackled. Quentin wiped tears from his eyes, from smoke or emotion or both.
Smoke billowed thickly for about 10 minutes, and died down. By then, fire was putting off enough heat to warm the circle. Flaky ashes swirled in the air, which smelled of incense.
A “threshold choir,” which specializes in singing for the dying, performed some of the tunes they had sung for Dr. Incao in his last few months. “Safe passage, pilgrim of the spirit,” they sang. “We are all just walking each other home.”
Sylvan spoke about how he had always teased his father about wearing so many layers, always being cold. “With the fire going, he’s warm enough,” he concluded with a smile. Another friend performed a “hallelujah” — another Steiner concept — in which she solemnly circled the pyre, lifting and lowering her arms, moving forward and backward.
Quentin, who had questioned his father’s plans from the start, watched the ceremony quietly and intently. “It was almost like a weight lifted, to know he’s moved on,” he said later, as the crowd dispersed and the ashes smoldered.
He knew, in the end, it was what his father had wanted.
Better care is needed for patients with late-stage cancer who may be facing the end of their life, and death doulas — also referred to as “soul doulas” or “end-of-life doulas” — may provide a resource that help patients and their family members cope with this difficult stage, according to Lorraine Holtslander.
“A death doula has education and expertise to support persons and families facing serious illnesses, including through death and grief,” Holtslander, a professor at the University of Saskatchewan College of Nursing in Canada, said in an interview with CURE®. “The doula provides support to access needed resources, make the best decisions and planning and preparing ahead for critical illness.”
Death doulas can help “fill the gaps” between the clinical and personal side of care, explained Holtslander, as they aid patients and families in navigating the health care system while also ensuring that important aspects such as their culture, gender and sexuality are honored through the end of their life. They may also offer services such as aromatherapy and music therapy.
“More people are wanting to take control over how they manage life-threatening illnesses, be supported to do their own future planning and move away from a strictly medical approach to death and dying, toward a more natural end of life,” she said.
Holtslander noted that death doulas are just one aspect of often-underutilized end-of-life-care resources that may be available for patients and their families. She mentioned that palliative care is always appropriate for patients with serious illnesses like cancer and ensuring that patients’ wishes are met starts with a conversation.
“It is so important to know what are the values, wishes and beliefs of the person facing serious illness or end of life so that the best decisions will be made,” Holtslander said. “We all face end-of-life at some point. Let’s make it the best experience, filled with courage and meaning, as there are many choices and options to bring comfort to the person and family.”
Options for patients with late-stage cancer may include palliative care, which focuses on symptom management and psychosocial wellbeing and hospice, which is care for the end of life.
“Patients with advanced cancer should access palliative and hospice care sooner, rather than later, in the process, which research shows will increase both the quality and quantity of their days and time,” Holtslander said. “If a patient is wanting to die at home, supports can be in place, such as the palliative care team, hospice resources and information, and doulas to support family caregivers.”
Death doulas not only help the patient through the end of their life, but also support loved ones through the grieving process after the patient with cancer dies. These professionals may be utilized at any time throughout the process, from completing the advanced-care plan up until and after death.
“Death doesn’t need to be scary of painful; it can be a very beautiful, truly spiritual experience,” Holtslander said.
However, more needs to be done for patients with late-stage cancer facing the end of their life, according to Holtslander.
“We can do better for people with advanced cancer, providing them with the best options, individualized plans of care, and more control over what is happening to them,” she concluded.
Death, of course, is a part of life for everybody. And for doctors, death comes with the territory of being a healer. Despite enduring more exposure to death than most, physicians still experience strong and lasting emotional reactions to it, including intense feelings about their own professional responsibility and competence.
COVID-19 brought this burden on doctors and other healthcare workers into sharp focus. Healthcare workers are dealing with mass mortality at a time when patients need more help than ever, but fewer resources are available to treat them.
This article examines how patients’ deaths affect their physicians, and how deaths from once-in-a-generation catastrophes like COVID-19 have complicated these encounters. We look at the stigma surrounding doctors and their emotions, and how such attitudes jeopardize healthy coping. Finally, we explore strategies that doctors can use to deal with patient death.
How do patient deaths affect physicians?
Even the most experienced physicians can have difficulty coping when a patient dies. Despite this—and despite the fact that physicians are confronted with death more than the average person—there is scant research examining how exposure to death affects them.
Available literature suggests that more exposure to patient death is strongly linked with more work-related stress, according to an article published in BMC Medical Education. Stress caused by the death of a patient at work can lead to burnout, which data suggests affects nearly half of all doctors treating terminally ill patients. To make matters worse, a high level of stress negatively impacts the quality of patient care, note the authors of a study published in BMJ Supportive and Palliative Care.
Sometimes, doctors feel the effects of a patient’s death long after it occurs. Feelings of numbness, guilt, and stress after a patient dies are common in the short term, but when surveyed, 61% of physicians reported that the most memorable patient death they witnessed continued to be a source of emotional distress for them in the long term, noted the BMC authors.
Patient deaths in the emergency department (ED) can be especially tough for doctors to deal with. There is typically no established patient-doctor relationship and death can occur suddenly, even in young and otherwise healthy patients, leading to more distress and emotional trauma for the healthcare workers tasked with preventing death from occurring, the authors added.
This takes its toll. According to a survey cited in the BMC article, 28% of ED doctors have considered quitting and 32% have thought about changing professions.
COVID-19 made it harder to cope with patient deaths
Dealing with medical emergencies means ED doctors are typically exposed to more sudden deaths than other physicians. But with the outbreak of COVID-19, doctors were confronted with unprecedented levels of patient death alongside increased demand for healthcare services, fewer resources per patient, and less time to do their jobs.
Together, these stressors are sometimes referred to as “cumulative grief,” a phenomenon that data from the US Department of Health and Human Services (HSS) suggests negatively impacts physicians’ health and the care they provide.
“Under normal circumstances, healthcare workers have more time to grieve and manage stress following the death of a patient. With increased deaths, the behavioral health impact of grief and the risk of burnout increase. This can result in compassion fatigue, low morale, exhaustion, burnout, and errors that could harm patient care,” according to the HHS report. You can read more about compassion fatigue and burnout here.
Systemic attitudes toward physician grief
Physicians recognize the need to help a patient’s bereaved family members and friends cope with death—breaking bad news is part of the job. But there is no standard advice for physicians who need that same support.
Traditional medical culture hasn’t looked kindly upon doctors’ emotional responses to death, notes psychologist, speaker, and author Elaine Kasket of London Metropolitan University, in a blogpost with BoardVitals.
“It is socially ingrained through medical school, and the cultures in both the UK and US medical establishments see a physician’s emotional response to death as a sign of weakness and even incompetence,” she said. “It feeds into this popular image of the physician as some kind of superhuman ultimate rescuer of human life; unable to do his or her job if they give in to or even acknowledge their emotions.”
Confronting this issue requires a fundamental change in the medical community’s perspective and policy. “There needs to be a sea change in medical culture to make support available,” she said, “and for it not to be stigmatized, to help physicians cope with grief, depression, despair or sadness.”
Strategies for coping with patient death
Out of necessity, and often in the place of a glaring absence of strategies in their training, physicians often develop their own ways of coping with their patients’ deaths. Sometimes, these coping mechanisms are unhealthy, such as when a doctor dons a morbid sense of humor (although some researchers maintain humor is healthy), tries to become numb to death, or externalizes the problem, as with alcohol abuse or overeating, according to the BoardVitals blogpost. Click here to read more about the drinking habits of doctors and the pandemic.
According to an article published in the Journal of Graduate Medical Education, oncologists at Memorial Sloan Kettering Cancer Center in NYC responded to the dearth of resources for physicians coping with death by introducing their own method, known as “Patient Death Debriefing Sessions.” Introducing these short sessions gave resident oncologists and other members of the treatment team a practical way to address their emotional needs after a patient died.
Patient death debriefing sessions were less than 10 minutes long, held within 24 to 28 hours of the death, consistently held after each patient death, and led by the attending physician. The sessions focused on residents’ emotional reactions to patient deaths, guided by a pocket card tool.
Memorial Sloan Kettering residents reported finding these sessions to be helpful and educational.
There is no shortage of techniques available—including yoga, mindfulness, exercise, and healthy hobbies—to help physicians relieve some of the stress and personal grief they feel when a patient dies. Read about some of those techniques here. And, of course, any physician needing support can lean on family members and friends, reach out to a counselor, and/or find a grief support group.
Just as important, however, is that doctors must give themselves permission to grieve—and society and the medical establishment can help take pressure off physicians by realizing they may need to grieve in the face of death, like any other human being.

















{kind=link}