Through asking the hard questions, this app will coach you through end-of-life plans.
By Steph Panecasio
When someone you love passes away, it’s impossibly hard to prioritize all the logistics. You’re facing unimaginable stress and grief all at once, so when it comes time to negotiate funeral planning, insurance records, legal and financial documents, and more, it can be overwhelming.
So it’s important to get all of this sorted before you’re reeling from loss.
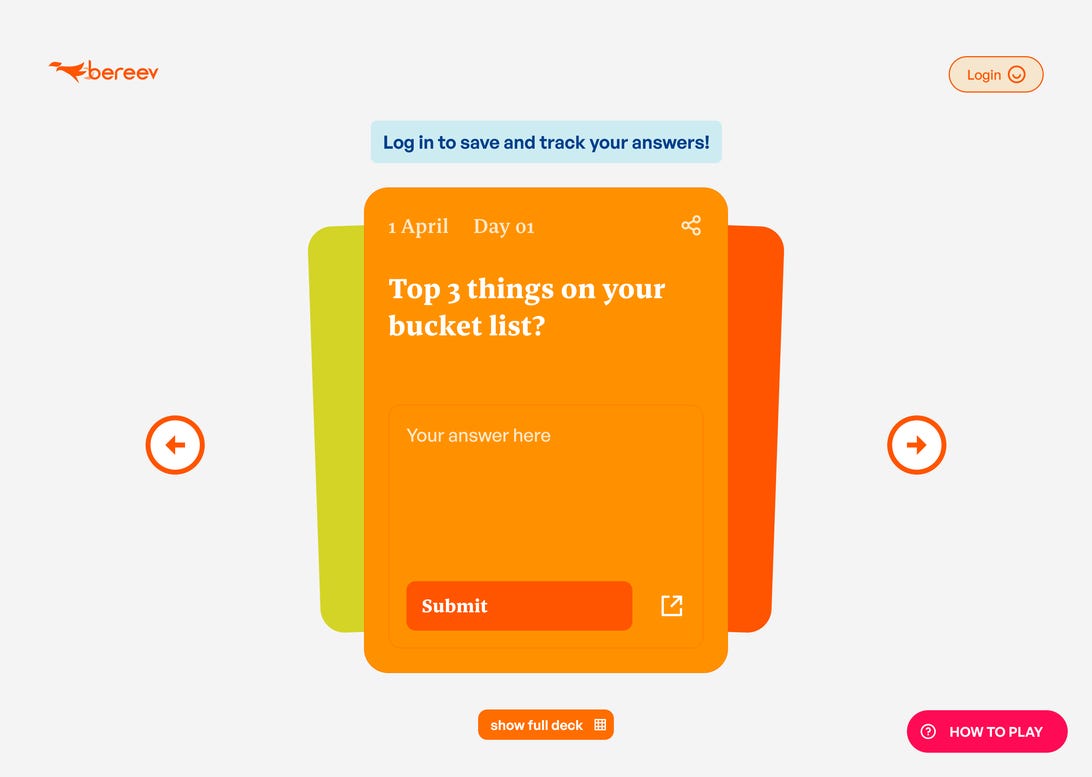
Enter Bereev, a death preparation app that’s beginning to make waves in Australia. Its purpose is to destigmatize the conversation surrounding end of life, turning death from a taboo topic to a dinner conversation. With planning and preparation, according to Bereev, we can ease the lives of the people we leave behind.
To spread the word, founder Izumi Inoue launched Death Convo Game, a campaign asking 31 questions about death over the 31 days of May.
The app asks you to start the conversation with your loved ones.
“Initially it was all about getting folks to get started on their preparations, mainly getting their affairs, instructions, documents, and messages in order so that the people they leave behind will get the chance to grieve, instead of running around dealing with the death admin which can be very traumatising,” said Inoue.
“We sat down as a team and asked ourselves, what are the biggest/most burning questions about death that we ourselves as individuals want to talk about? With that, we started off with close to a hundred questions, which we then put on a vote amongst a small group of our existing users and picked the top 31.”
The game, and the wider app, ask you to challenge your preconceptions about death. Each day, you’re prompted with a new question to open up a dialogue with your loved ones.
“How would you like to be remembered?”
“Who would you like to be surrounded by towards the end?”
“When do you feel most alive?”
For every day that users participate in the Death Convo Game, it gives them a greater chance to score free access to the Bereev app, where they can prepare their plans.
From there, the app coaches you through the difficult process of organizing your end of life plans, no matter what you might choose to do. It also has a focus on inclusivity, with options for Muslim users who wish to upload their Wasiat and Hibah to their preparation plans.
“We started off in Malaysia back in 2018 and Malaysia is a melting pot of cultures, ethnicities and religions,” said Inoue. “It taught us a lot in terms of navigating a spectrum of beliefs, and like it or not, death and religion can be very intertwined. Because of that, I think that every death tech startup should take their communities’ beliefs into account and weave that into their user experience.”
Death tech is a hugely promising arena, with everything from alternative cremations and funeral tech through to video games dealing with the concept of end-of-life care. It’s little wonder that apps like Bereev have such an invested audience, when all of us are guaranteed to face death eventually.
It stems from the concept of death positivity, which is all about destigmatizing the conversation. Death positivity doesn’t mean you’re looking forward to death — it just means that you accept what comes and that you learn to talk about it in a healthy way.
That’s why Inoue and the team behind Bereev believe it’s even more important to deal with the paperwork before it comes time.
“I’ve lost both of my grandparents and have seen with my own eyes the toll an unprepared death takes on the people left behind,” said Inoue.
“It causes friction, additional trauma and it tears families apart. No one in their right mind would want to inflict that one their already grieving loved ones. … I have a saying that I stick by: When I go to heaven, the last thing I want is to put my loved ones through hell.”
I’m no stranger to grief. After all, I’ve been alive for nearly 65 years. And I’ve spent almost 40 of them as a psychotherapist, midwifing people’s grief: the couple who split after their child dies because they remind each other of the loss, the woman who swears her dead husband talks to her every night, the man who can’t clean out his deceased wife’s closet even after three years.
Any therapist will tell you that death is not the only occasion for grief. We can mourn the loss of anything to which we have become attached: a pet, a job, a home, a way of life. In bereavement, what is best about us — our ability to love — becomes the source of our suffering. It’s a wonder that all grief isn’t prolonged and that anyone is able to love again rather than wander through life stunned by its cruelty. And it’s surprising that anyone actually believes that there are stages and time limits to grief or that we know enough about how it works to know what to expect of it.
I figured my job had acquainted me with all the varieties of grief. But then I took on an additional one. Since November 2019, I’ve been the first selectman of a small New England town (population: about 1,575). It means I’m its chief executive officer, as well as its chief of police, tree warden and cemetery sexton, and I wind the clock in the Scotland Congregational Church.
The new job has a lot more in common with the old one than you’d think, or at least more than I would have thought. In both cases, unhappy people tell me what is bothering them and often expect (or even demand) that I do something about it. Responding to concerns about high taxes or flooded storm drains does not, however, usually require an excavation of a complainant’s past trauma; when I can fix the problem with a phone call, I am gratified in a way I would not have expected.
When the American Psychiatric Association added prolonged grief disorder to its Diagnostic and Statistical Manual of Mental Disorders last fall, the organization’s president, Vivian B. Pender, explained that “the circumstances in which we are living” have made people more susceptible to prolonged bouts of grief. The association noted that in addition to Covid deaths, Americans faced many ongoing disasters, including, at the time, “the wind-down in Afghanistan, floods, fires, hurricanes and gun violence.”
“Check in with yourself” if you’ve lost someone, Dr. Pender recommended. “Grief in these circumstances is normal, but not at certain levels and not most of the day, nearly every day for months. Help is available.”
Dr. Pender’s comments marked the culmination of a process that began about a decade ago, when the association identified prolonged grief as a possible mental disorder, a designation that encouraged researchers and the pharmaceutical industry to fund studies into such matters as the brain chemistry of protracted mourning, the difference between prolonged grief disorder and depression and the merits of various talk and drug therapies. They have identified neural circuits, sharpened diagnostic criteria and developed treatment regimens. There’s even an app for it under study called My Grief.
Critics, including me, have called this yet another intrusion of psychiatry into normal life, pointing out that there are no biological markers to distinguish prolonged grief disorder from normal grieving, whatever that is, and that no one has yet come close to figuring out how neural circuits give rise to any experience, let alone one as complex as grief.
But we must acknowledge that the new diagnosis is already doing exactly what a diagnosis is supposed to do — garnering resources for suffering people and attention to their suffering. The occasions for grief, prolonged or otherwise, do seem to be multiplying, and there is more to mourn than the loved ones lost to Covid or war or climate change. Coupled with our polarized, paralyzed politics, these calamities seem to threaten the foundations of our cultural, political and natural worlds. Turning grief into a mental disorder at least draws notice to the enormousness of the losses we face and to the bereavement that underlies all of them: the loss of the familiar.
I am confronted frequently by the derangements of loss. Sometimes it’s obvious, like when a couple are furious about the location of the cemetery plot they are purchasing for their son who died from an overdose. Other times, it’s not quite so on the nose, such as when an applicant for a fishing license likens the masks we’ve mandated at Town Hall to Nazism or when a young couple, baby in arms, tell me the pistol permits I just signed for them are so they can defend themselves but can’t say exactly against what or when a woman calls to ask if anything can be done about her neighbor’s flag with an obscenity aimed at people who voted for President Biden.
But even if you have to squint a little to see it, the loss is always there, lurking behind the anger: loss of control, of certainty, of the confidence that hard work and persistence will pay off with a life that is predictable and secure.
You may have guessed that my town is a Donald Trump town, and you would be correct: He beat Hillary Clinton and Mr. Biden handily here, and MAGA hats seem as common here as caps advertising trucks or construction equipment. You don’t have to squint to see the loss written on those caps. What is nostalgia but a yearning for what once was, at least in imagination, and a wish to have it again — the truck that you can fix yourself, the world before the pandemic, the reliably upward trajectory of an American life? Isn’t anger a way to stave off the helplessness that accompanies the recognition that something precious is gone forever?
I am also nostalgic for the time, probably also imagined, when the Enlightenment dream prevailed. That tolerance would bring forward our differences so that reason could sort them out, with facts as our common ground. That fairness and liberty might pull in different directions but would not pull us apart. At the very least, that we could unite to fight a virus. I am also bereft, heartsick over the incipient loss of a shared world so total that we can’t even agree on what has been lost, let alone mourn it in unison. Or, for that matter, pick up the pieces and see if we can fashion something better out of them.
Perhaps the American Psychiatric Association is correct to turn prolonged grief into an illness and to cite the multiplicity of world-historical calamities to support this claim. Not because the diagnosis will lead to finding errant brain circuits to treat but because, as the links in the supply chain of our familiar world weaken and snap, we may need to be reminded that behind the outrage and blame is bereavement, that we may be entering a long age of grief and we have no one to console us for our losses or to build something new with, except one another.
Complex restrictions are preventing patients from accessing medical aid in dying, even in states where it is allowed. New legal and legislative efforts are pushing to change that.
Dr. Nicholas Gideonse, a hospice medical director and doctor at Oregon Health & Science University.
Five years ago, Dr. Nicholas Gideonse spoke with an older man who had received a terminal cancer diagnosis and was hoping to use Oregon’s medical aid-in-dying law.
Oregon’s Death With Dignity Act, in effect since 1997, permits doctors, after a complex process of requests and waiting periods, to prescribe lethal medication for dying patients to self-ingest.
The nonprofit group End of Life Choices Oregon had referred the man to Dr. Gideonse, a primary care doctor at Oregon Health & Science University and a hospice medical director, who had already helped many patients use the law.
But this time he could not. “I’m really sorry,” he told the man on the phone. “I’m not going to be able to help you with this.” Oregon’s law — and all the laws that permit medical aid in dying in 10 states and in Washington, D.C. — has residency requirements. This man would have qualified — except for that fact he lived in nearby Washington State.
The patient’s response, Dr. Gideonse recalled, was “stunned silence, deep disappointment.” A number of Dr. Gideonse’s primary care patients drive 20 to 30 minutes across the Washington border to his office in Portland. There, he can offer them any medical service he is qualified to provide — except that one — without proof of residency. And although Washington has its own aid-in-dying law, its southwestern region has few providers who can help patients use it.
Last month Dr. Gideonse, backed by pro bono lawyers and Compassion & Choices, an advocacy group for expanding end-of-life options, filed a federal lawsuit claiming that the residency requirement for Oregon’s aid-in-dying law is unconstitutional. “I realized how important this could be for patients seeking access,” he said.
The lawsuit is one of several legal and legislative efforts around the country to reduce the requirements that patients must contend with in order to receive aid in dying. In some states, lawmakers have already broadened the types of health care providers that can participate, or have shortened waiting periods or allowed waivers.
“I think of it as MAID 2.0,” said Thaddeus Pope, an end-of-life bioethicist at Mitchell Hamline School of Law who tracks such actions, referring to the acronym for medical aid in dying. “We found out there’s an access problem.” He added, “We set all these safeguards and eligibility requirements and they locked a lot of people out.”
Oregon led the shift in easing access, amending its law in 2019. The state previously required patients to make two verbal requests for life-ending medication, at least 15 days apart, to ensure that they had not changed their minds. Now, if the patient is unlikely to survive that long, their doctor can waive the 15-day waiting period.
“Fifteen days is everything when you are suffering,” said Kim Callinan, the president and chief executive of Compassion & Choices, which supported the change. “People who are eligible for the law are hitting roadblocks and barriers.”
In 2016, for example, Youssef Cohen, a political scientist at New York University, took the extraordinary step of moving across the country to use the Oregon law as he was dying of mesothelioma at 68. “He wanted the option to determine the end of his life,” said his wife, Lindsay Wright, who is an associate dean at the university.
To establish residency, the couple had to hurriedly sign an apartment lease, obtain an ID from the state motor vehicle agency, transfer medical records and arrange an immediate appointment with a Portland doctor to qualify for medical aid in dying. Dr. Cohen then faced the 15-day waiting period.
“He didn’t make it,” Dr. Wright said. “He died six days after we arrived. And he suffered.”
New Mexico, which in June became the most recent state to legalize medical aid in dying, has adopted a markedly less restrictive approach than other states. The largely rural state is the first to allow not only doctors but advanced practice registered nurses and physician assistants to help determine eligibility and write prescriptions for lethal medication. “In some communities, they’re the only providers,” said Representative Deborah Armstrong, a Democrat and the bill’s primary sponsor.
Although a doctor must also affirm that a patient is terminally ill, New Mexico patients can skip that step if they have already enrolled in hospice, as most do. The patient need only make one written request, rather than two or more requests, as other states require. A 48-hour waiting period between when the prescription is written and when it is filled can be waived. “People walk up and tell me how thankful they are to have this option if they need it,” Ms. Armstrong said.
California has simplified its 2016 law as well. In October, Gov. Gavin Newsom signed legislation that, starting in January, reduces the 15-day wait between verbal requests to 48 hours and eliminates the requirement for a third written “attestation.”
Similar bills died during the most recent legislative sessions in Hawaii, Washington and Vermont, but will be reintroduced, Ms. Callinan said. And in many states — including Delaware, Indiana, North Carolina, Virginia, Pennsylvania and Arizona — new aid-in-dying bills, if passed, will ease requirements for patients or expand the kinds of providers who may participate.
On the legal front, the Oregon lawsuit filed by Dr. Gideonse argues that residency requirements for aid in dying violate two sections of the U.S. Constitution, one barring state laws that limit the ability of a nonresident to access medical care and one prohibiting state laws that burden interstate commerce. The state must respond by Dec. 27.
“This is the only medical procedure we can think of that is limited by someone’s ZIP code,” said Kevin Diaz, the chief legal advocacy officer at Compassion & Choices.
A separate federal class action suit claims that California’s law, which like the others requires patients to self-administer the drugs that end their lives, discriminates against patients dying of neurodegenerative diseases that make it physically impossible to take medication without assistance.
The plaintiffs, charging violation of the Americans With Disabilities Act and California law, include patients with multiple sclerosis and A.L.S., also known as Lou Gehrig’s disease, and their doctors. (In denying a request for a preliminary injunction, a judge ruled in September that the plaintiffs were asking California “to cross the line to euthanasia.”)
Catholic organizations, anti-abortion advocates and some disability groups continue to oppose aid in dying. The California Catholic Conference, the church’s public policy organization, for example, argued in June that liberalizing the state’s law “puts patients at risk of abuse and the early and unwillful termination of life.”
But polls regularly report broad public support. Last year, Gallup found that 74 percent of respondents agreed that doctors should be allowed to end patients’ lives “by some painless means” if they and their families request it.
Liberalizing the laws will likely increase participation, the bioethicist Dr. Pope predicts. “We know from evidence around the world that if you reduce the waiting period, or allow waivers in certain cases, it materially expands access,” he said.
Experts do not expect a major surge, however. Even in states where the practice has been legal for years, aid in dying accounts for very few deaths, a fraction of one percent. Of those who successfully navigate the process, moreover, about one-third do not use the drugs and instead die of their diseases.
Still, should Dr. Gideonse prevail in his lawsuit and a likely appeal, residency requirements in other regions might also start to fall. That could allow New York or Pennsylvania patients to use New Jersey’s aid-in-dying law, for instance, or Maryland and Virginia residents to seek providers in Washington, D.C.
It is an outcome that would please Dr. Gideonse. “This is an action in support of a needed and very important service,” he said. “I’m optimistic.”
What role does the federal government play in assisting Americans in need of long-term care? The answers, which lie primarily within two programs — Medicare and Medicaid — may may surprise you. Here is a breakdown of the services they do and don’t offer.
Does Medicare cover the costs of long-term care?
No. This is a common misconception. As a reminder, Medicare is strictly a health insurance program that covers costs related to illnesses and injuries (and, to some extent, their prevention). As such, it will help pay for up to 100 days of rehabilitation or skilled nursing care after a major health issue, based on a doctor’s recommendation. But longer stays, such as a permanent move into a nursing home, are not covered.
What about Medicare Advantage?
You can check to see if there’s a Medicare Advantage plan in your area that offers limited caregiving assistance. You may be able to find one that provides meals or pays for installation of grab bars, says Howard Gleckman, senior fellow at the Urban Institute. A small number of so-called special needs plans offer some in-home support services. If a Medicare Advantage plan has a five-star rating, you may switch to it outside of the annual enrollment period.
What about Medicaid?
Medicaid does pay for long-term nursing-home care, but only for people with very low income and modest savings who can no longer handle basic daily tasks like dressing or feeding themselves. Gleckman says a good rule of thumb is that if you have less than $750 in income per month and less than $2,000 in financial assets (not counting a home), you likely qualify for Medicaid.
This excludes a large number of people who draw Social Security, given that the average monthly benefit check is more than $1,600. Remember that Medicaid is meant to help just the very poor. Most middle-class people and even low-income people do not qualify, although sometimes people use up their savings and spend so much of their income on care that they do become eligible.
But also note that the Medicaid program is a partnership between the federal government and each state, meaning criteria for who qualifies and what benefits are available can vary based on where you live. Some states provide some benefits to people with low incomes who are over the basic qualification limit, but they are expected to pay for part of the care.
What about care services at home?
It’s important to distinguish between medical care and daily care needs like bathing, eating, moving about and such.
As noted, Medicare will pay for assistance like physical therapy or skilled nursing care, whether in a facility for short periods or at home, where there is no specific time limit, while a patient is recovering from an illness or injury. A supplemental Medigap policy may help with some at-home medical care costs, Gleckman says.
“But for people who are unable to care for themselves at home and don’t have a family member to help manage their daily activities, Medicare doesn’t fill that gap,” says Tricia Neuman, head of the Kaiser Family Foundation Program on Medicare Policy.
Medicaid is another matter. If you meet its stringent requirements, some recipients can get coverage for aides to help with activities like dressing and toileting, says Sara Rosenbaum, a law professor at the George Washington University Milken Institute School of Public Health. But even those benefits only go so far. “Medicaid is not going to provide anything remotely like 12 hours of help,” Gleckman notes. And again, benefits — and funding levels — vary by state. Oregon and Minnesota, in particular, have robust programs to help people live at home or in the community instead of in nursing homes.
Veterans should check with the U.S. Department of Veterans Affairs, which has some programs for those needing ongoing care, including a foster care program through which veterans live with families who can help them. For broader background on long-term care, visit longtermcare.acl.gov. The Area Agencies on Aging are a good clearinghouse for information on nonprofits or other community resources. Go to eldercare.acl.gov.
What if I just need a break as a caregiver?
Some state Medicaid programs pay for adult day programs that offer medical services. And some Medicare Advantage plans are beginning to offer coverage for adult day care and other breaks for family members, says Robert Saunders, senior research director for health care transformation at the Duke-Margolis Center for Health Policy. “There are more options now than there used to be.”
In end-of-life situations, Medicare will pay for respite care in hospice. That palliative care coverage is available when someone is considered to be in the final six months of life.
Like taxes, death is still a certainty. But in America, the end of life isn’t what it used to be.
Today, one in five Americans lives in a state that permits medical aid in dying, sometimes simply called assisted dying. The idea is terminally ill individuals who have six months or less to live can apply for a medically assisted death to limit their suffering. And if they meet the criteria, they can have some say when they will take their last breath.
It’s been nearly 25 years since the country’s first assisted death law — Oregon’s Death With Dignity Act — went into effect. And since then, eight other states — Washington, Vermont, California, Colorado, Hawaii, New Jersey, Maine and New Mexico, as well as Washington, D.C., have enacted their own versions. What all jurisdictions with medical aid in dying have in common is the requirement that the patients must be of sound mind, have less than six months to live and they must be able to self-administer the lethal medication, prescribed by a physician, to end their lives.
Eleven other states have introduced medical aid in dying bills during the 2021-22 legislative session. It’s a growing movement that’s largely under the radar, much as death is in this society.
Assisted death is “not the path of least resistance. For many it’s the path of most resistance.”
In the latest survey by Susquehanna Polling & Research, two out of three voters (67%) said if they “had an incurable, terminal illness, still had a sound mind but less than six months to live and met the legal requirements,” they would want the option of medical aid in dying.
As the baby boomers age, medical aid in dying is expected to be an even bigger issue in the years ahead.
Anita Hannig, associate professor of anthropology at Brandeis University in Waltham, Massachusetts, says assisted death is “not the path of least resistance. For many it’s the path of most resistance.”
Indeed, the assisted dying laws in the ten U.S. jurisdictions are among the most restrictive in countries with such laws. That hasn’t stopped opposition from some religious and right-to-life groups, among others.
For her new book, “The Day I Die: The Untold Story of Assisted Dying in America,” Hannig spent hundreds of hours over five years on the frontlines of assisted dying in the Pacific Northwest, including witnessing several deaths among those who availed themselves of the law.
Next Avenue: You’ve taken a very deep dive into assisted dying in America, a world few families have experienced. As a cultural anthropologist, you’ve gone from researching birth and the beginning of life in Ethiopia to the opposite end of the life cycle. Why the shift?
Anita Hannig: I was showing a film called ‘How to Die in Oregon’ in my Medicine and Religion class at Brandeis. It’s such a lovely documentary about the law in Oregon and about all those assisted dying volunteers who go and help people die. And I was immediately hooked and thought, wow, birth and death are like bookends. You have home births and home deaths. And so I was curious to go over to the other side. I was very surprised by what I found.
You must have a unique perspective on birth and death as an anthropologist studying assisted dying and as a new mother who also lost a child during an earlier pregnancy.
Definitely. We’re so used to thinking about birth and death as opposites when they’re actually very similar. One of the main figures in my book, a former nurse and longtime assisted dying volunteer in Oregon, Derianna Mooney, taught me that birth and death are both sacred transitions — from one state of being to another, from nonbeing into being and being into nonbeing. And culturally we revere one, but we shun the other.
“I think part of the issue is that we have all the technology now, but our ethical and moral compass hasn’t really caught up with how we should use it.”
As a new mother, I can see people’s eyes light up when they watch us stroll by with our oversized pram. There’s so much positive attention. And all of this has to do with the fact that we love the beginning. It holds so much promise.
And yet we’re so afraid of the end. Similar to a birth, people do need help at the end of life. I love when Derianna says, “You’re going to the gate with them and you are letting them go, but you’re nurturing them through the gate.” What a beautiful vision.
One of the vexing issues surrounding death in our country especially is the role high-tech medicine plays in extending life — even when a longer life doesn’t always promise more quality. Is the assisted dying movement a sign that technology is frequently not making our final years better?
Yes. I think part of the issue is that we have all the technology now, but our ethical and moral compass hasn’t really caught up with how we should use it. And it’s not just in the United States. My 87-year-old grandmother, who passed away in Germany in March, underwent radiation for her breast cancer when she was two weeks away from dying. I’m flabbergasted when I think about why we offer this extremely invasive treatment to somebody who is close to dying. Thankfully, she was soon admitted to a beautiful hospice by a lake to spend what became her final days.
I got interested in this topic when a friend’s husband, suffering from Parkinson’s and no longer able to feed himself, was forced to starve himself to death since he lived in Maryland, a state without a medical aid in dying law. For people consigned to such a horrific death, can a doctor truly say they are following the Hippocratic Oath that tells physicians to do no harm?
That’s exactly the conclusion that a lot of doctors who help patients die come to because in that case doing nothing — such as not helping somebody die — is doing harm. Physicians who are at the forefront of assisted dying say their task is to prevent suffering. And how you prevent suffering in many of these cases is to help somebody die. I always come back to this question: Who is telling these patients that they need to hang on? For what? For whom? Sometimes they themselves are ready to go, but they want to stick around for the family or because there’s a societal expectation to fight.
At the beginning of your book, you almost took my breath away when you were helping one of the volunteers opening the capsules of Seconal and pouring powder into a bowl in one room while the patient, Ken, was waiting in the next room to receive the lethal medication. What were your thoughts as you prepared the medicinal mix that you knew would end a man’s life?
It’s a really good question. Anthropologists have a tool in our toolbox called “participant observation.” And that means you’re never just an impartial observer because your presence alone already changes what’s happening in the room. In order to really relate and put ourselves and the reader into the shoes of these people, you have to bring yourself into the situation wholeheartedly and authentically. And often that means becoming a participant in what is happening.
It’s an extreme privilege to be invited into that kind of intimate space. So, it would have felt very off- putting to just be sitting in the corner taking notes. Everybody in the room is carrying this person over the threshold together. And so you just kind of take your cues from what’s happening.
You don’t want to feel like a voyeur?
Exactly. You want to be in the moment and going through all the emotions other people are going through. It’s a different way of being present that allows you to faithfully experience the death alongside the people whose loved one is dying.
But this must have been a difficult moment for you. In your book, you described “a heavy sense of transgression rise up inside” of you as prepared the lethal medication.
You know what I think it is? It’s the feeling of internalizing some of the stigma that we carry and some of the taboo with which we treat death. And so being part of somebody’s death in this participatory way makes you ask, ‘Am I doing something wrong? Am I, in some bizarre way, enabling that person to die?’
But even if I hadn’t been there, things would have gone probably in a very similar way. I think it’s the cultural baggage that we feel around what it means to hasten the end of your life. Everyone there knew this is what Ken wanted. He chose this with one-hundred percent of his cognitive abilities. His wish was to be delivered from this world and you are enabling that transition.
Among the deaths you researched but didn’t witness was that of Louis, who was an outlier. His experience turned into a nightmare for the person who supervised his assisted death. Louis actually woke up after taking the lethal medication. What happened?
“Everybody in the room is carrying this person over the threshold together.”
Medicine is a human art and as an art, is prone to failure. And it just goes back to the ways the laws are written. They insist on self-administration. But when you are limited that way, you’re going to run into a bunch of problems such as people with gastrointestinal issues who can’t quite absorb the medication. And then you have people who can’t physically self-administer, like a lot of folks with ALS or other illnesses that affect their mobility or their hand range or who can’t drink something on their own or push the syringe on their feeding tube.
And people are getting a little more innovative with things like rectal catheters now, but there’s still a requirement that this has to be an act of volition — you have to be the one to push the plunger on your feeding tube or catheter, what have you. And in almost all other countries, you don’t have that requirement. A doctor can administer if you’re unable to administer yourself.
So after immersing yourself in this world of assisted dying for five years, what‘s your takeaway from this experience?
As a society, we have to make a concerted effort to become less alienated from death and dying. Of course, one could ask how alienated are we when the biggest newspaper in the country, the New York Times, can post images of corpses in Ukraine on its front page? But that doesn’t create closeness or connection. That just creates more fear.
Ideally, I think everybody should have to take a class on death and dying that could cover estates, hospice, and what life-extending procedures there are. In my death and dying class, I talk about people in South Korea who fill an entire gymnasium with coffins and the public comes in and gets inside the coffin to simulate what it would be to die. And they come out of this experience with a totally new zest for life.
This is what contemplating our mortality can do for us. It can take away some of the fear and some of the surprise when a loved one passes away because you will have thought about it in advance. I’m not saying assisted death is the way to go for everyone. We really need to pay more attention to end-of-life issues and prepare for the inevitable and have all of that be less stigmatized.
As the country’s pandemic death toll inches toward one million, has America’s attitude toward death changed at all?
Certainly it’s brought death into the lives of lots of people but not in a way to make them feel more connected to death. Many people weren’t able to see their loved ones in assisted living homes or couldn’t go to the funeral or they weren’t allowed to be present at a nursing home.
When I see the way that we’re tumbling back into life as it was before the pandemic, I don’t know that we’ve really thought critically about death. We just have this big fear-based relationship with death and it’s not lifting the curtain, really. I think people are thrilled to have escaped the pandemic. They see themselves on the other end of that mostly unscathed.
They dodged a bullet?
That’s exactly what it is. But I don’t think it’s made us really contemplate our mortality that much more.
So what will give you a signal that something has shifted in the American attitude toward death?
That people don’t automatically associate the topic of death with fear. And when people begin to realize what I witnessed and write about in the book — some of the empowerment that can come from determining the end of your life and even some of the joy. I hope I’m not out of line to call it joy. When I think of the deaths I witnessed, they weren’t unambiguously sad. There were also serene and heartfelt moments, some laughter and families felt at ease because their loved one wanted to die and they were helping them.
And those who chose to end their lives wanted their death to resonate beyond themselves and their families. Jean, one of the people whose death I witnessed, unbelievably spent the last few minutes of her life promoting her chosen way to die. I still remember her words:
“There are all these baby boomers who will want a better way to die. Our society doesn’t recognize that yet. They will someday.”
After more than a decade of argument, psychiatry’s most powerful body in the United States added a new disorder this week to its diagnostic manual: prolonged grief.
The decision marks an end to a long debate within the field of mental health, steering researchers and clinicians to view intense grief as a target for medical treatment, at a moment when many Americans are overwhelmed by loss.
The new diagnosis, prolonged grief disorder, was designed to apply to a narrow slice of the population who are incapacitated, pining and ruminating a year after a loss, and unable to return to previous activities.
Its inclusion in the Diagnostic and Statistical Manual of Mental Disorders means that clinicians can now bill insurance companies for treating people for the condition.
It will most likely open a stream of funding for research into treatments — naltrexone, a drug used to help treat addiction, is currently in clinical trials as a form of grief therapy — and set off a competition for approval of medicines by the Food and Drug Administration.
Since the 1990s, a number of researchers have argued that intense forms of grief should be classified as a mental illness, saying that society tends to accept the suffering of bereaved people as natural and that it fails to steer them toward treatment that could help.
A diagnosis, they hope, will allow clinicians to aid a part of the population that has, throughout history, withdrawn into isolation after terrible losses.
“They were the widows who wore black for the rest of their lives, who withdrew from social contacts and lived the rest of their lives in memory of the husband or wife who they had lost,” said Dr. Paul S. Appelbaum, who is chair of the steering committee overseeing revisions to the fifth edition of the D.S.M.
“They were the parents who never got over it, and that was how we talked about them,” he said. “Colloquially, we would say they never got over the loss of that child.”
Throughout that time, critics of the idea have argued vigorously against categorizing grief as a mental disorder, saying that the designation risks pathologizing a fundamental aspect of the human experience.
They warn that there will be false positives — grieving people told by doctors that they have mental illnesses when they are actually emerging, slowly but naturally, from their losses.
And they fear grief will be seen as a growth market by drug companies that will try to persuade the public that they need medical treatment to emerge from mourning.
“I completely, utterly disagree that grief is a mental illness,” said Joanne Cacciatore, an associate professor of social work at Arizona State University who has published widely on grief, and who operates the Selah Carefarm, a retreat for bereaved people.
“When someone who is a quote-unquote expert tells us we are disordered and we are feeling very vulnerable and feeling overwhelmed, we no longer trust ourselves and our emotions,” Dr. Cacciatore said. “To me, that is an incredibly dangerous move, and short sighted.”
“I completely, utterly disagree that grief is a mental illness,” said Joanne Cacciatore, an associate professor of social work at Arizona State University who operates the Selah Carefarm, a retreat for bereaved people.
‘We don’t worry about grief’
The origins of the new diagnosis can be traced back to the 1990s, when Holly G. Prigerson, a psychiatric epidemiologist, was studying a group of patients in late life, gathering data on the effectiveness of depression treatment.
She noticed something odd: In many cases, patients were responding well to antidepressant medications, but their grief, as measured by a standard inventory of questions, was unaffected, remaining stubbornly high. When she pointed this out to psychiatrists on the team, they showed little interest.
“Grief is normal,” she recalls being told. “We’re psychiatrists, and we don’t worry about grief. We worry about depression and anxiety.” Her response was, “Well, how do you know that’s not a problem?”
Dr. Prigerson set about gathering data. Many symptoms of intense grief, like “yearning and pining and craving,” were distinct from depression, she concluded, and predicted bad outcomes like high blood pressure and suicidal ideation.
Her research showed that for most people, symptoms of grief peaked in the six months after the death. A group of outliers — she estimates it at 4 percent of bereaved individuals — remained “stuck and miserable,” she said, and would continue to struggle with mood, functioning and sleep over the long term.
“You’re not getting another soul mate and you’re kind of eking out your days,” she said.
In 2010, when the American Psychiatric Association proposed expanding the definition of depression to include grieving people, it provoked a backlash, feeding into a broader critique that mental health professionals were overdiagnosing and overmedicating patients.
“You’ve got to understand that clinicians want diagnoses so they can categorize people coming through the door and get reimbursement,” said Jerome C. Wakefield, a professor of social work at New York University. “That is a huge pressure on the D.S.M.”
Still, researchers kept working on grief, increasingly viewing it as distinct from depression and more closely related to stress disorders, like post-traumatic stress disorder. Among them was Dr. M. Katherine Shear, a psychiatry professor at Columbia University, who developed a 16-week program of psychotherapy that draws heavily on exposure techniques used for victims of trauma.
By 2016, data from clinical trials showed that Dr. Shear’s therapy had good results for patients suffering from intense grief, and that it outperformed antidepressants and other depression therapies. Those findings bolstered the argument for including the new diagnosis in the manual, said Dr. Appelbaum, who is chair of the committee in charge of revisions to the manual.
In 2019, Dr. Appelbaum convened a group that included Dr. Shear, of Columbia, and Dr. Prigerson, now a professor at Weill Cornell Medical College, to agree on criteria that would distinguish normal grief from the disorder.
The most sensitive question of all was this: How long is prolonged?
Though both teams of researchers felt that they could identify the disorder six months after a bereavement, the A.P.A. “begged and pleaded” to define the syndrome more conservatively — a year after death — to avoid a public backlash, Dr. Prigerson said.
“I have to say that they were kind of politically smart about that,” she added. The concern was that the public was “going to be outraged, because everyone feels because they still feel some grief — even if it’s their grandmother at six months, they are still missing them,” she said. “It just seems like you’re pathologizing love.”
Measured at the year mark, she said, the criteria should apply to around 4 percent of bereaved people.
The new diagnosis, published this week in the manual’s revised edition, is a breakthrough for those who have argued, for years, that intensely grieving people need tailored treatment.
“It’s kind of like the bar mitzvah of diagnoses,” said Dr. Kenneth S. Kendler, a professor of psychiatry at Virginia Commonwealth University who has played an important role in the last three editions of the diagnostic manual.
“It’s sort of an official blessing in the world,” he said. He compared it to astronomers deciding on a definition of planet. “This one’s in, and Pluto we kick out.”
If the diagnosis comes into common use, it is likely to popularize Dr. Shear’s treatment and also give rise to a range of new ones, including drug treatments and online interventions.
Dr. Shear said it was difficult to predict what treatments would emerge.
“I don’t really have any idea, because I don’t know when the last time there was a really brand-new diagnosis,” she said.
She added, “I really am in favor of anything that helps people, honestly.”
Dr. M. Katherine Shear, a psychiatry professor at Columbia University and a founding director of the Center for Prolonged Grief, has been studying the condition since 1995.
A loop of grief
Amy Cuzzola-Kern, 54, said Dr. Shear’s treatment helped her break out of a terrible loop.
Three years earlier, her brother had died suddenly in his sleep of a heart attack. Ms. Cuzzola-Kern found herself compulsively replaying the days and hours leading up to his death, wondering whether she should have noticed he was unwell or nudged him to go to the emergency room.
She had withdrawn from social life and had trouble sleeping through the night. Though she had begun a course of antidepressants and seen two therapists, nothing seemed to be working.
“I was in such a state of protest — this can’t be, this is a dream,” she said. “I felt like I was living in a suspended reality.”
She entered Dr. Shear’s 16-session program, called prolonged grief disorder therapy. In sessions with a therapist, she would narrate her recollection of the day that she learned her brother had died — a painful process, but one that gradually drained the horror out of the memory. By the end, she said, she had accepted the fact of his death.
The diagnosis, she said, mattered only because it was a gateway to the proper treatment.
“Am I ashamed or embarrassed? Do I feel pathological? No,” she said. “I needed professional help.”
Yet, others interviewed said they were wary of any expectation that grief should lift in a particular period of time.
“We would never put a time frame around when someone should or shouldn’t feel that they have moved forward,” said Catrina Clemens, who oversees the victim services department of Mothers Against Drunk Driving, which provides services to bereaved relatives and friends. The organization encourages bereaved people to seek mental health care, but has no role in diagnosis, said a spokesperson.
Filipp Brunshteyn, whose 3-year-old daughter died after an automobile accident in 2016, said grieving people could be set back by the message that their response was dysfunctional.
“Anything we inject into this journey that says, ‘that’s not normal,’ that could cause more harm than good,” he said. “You are already dealing with someone very vulnerable, and they need validation.”
To set a year as a point for diagnosis is “arbitrary and kind of cruel,” said Ann Hood, whose memoir, “Comfort: A Journey Through Grief,” describes the death of her 5-year-old daughter from a strep infection. Her own experience, she said, was “full of peaks and valleys and surprises.”
The first time Ms. Hood walked into her daughter Grace’s room after her death, she saw a pair of ballet tights lying in a tangle on the floor where the little girl had dropped them. She screamed. “Not the kind of scream that comes from fright,” she later wrote, “but the kind that comes from the deepest grief imaginable.”
She slammed the door, left the room untouched and eventually turned off the heat to that part of the house. At the one-year mark, a well-meaning friend told her it was time to clear out the room — “nothing worse than a shrine,” he told her — but she ignored him.
Then one morning, three years after Grace’s death, Ms. Hood woke up and returned to the room. She sorted her daughter’s clothes and toys into plastic bins, emptied the bureau and closet and lined up her little shoes at the top of the stairs.
To this day, she is not sure how she got from one point to the other. “All of a sudden, you look up,” she said, “and a few years have gone by, and you’re back in the world.”
Sit shiva for seven days. Spend another 30 in sheloshim — a secondary mourning period — and say the Mourner’s Kaddish for a year. Between all of its mourning rituals, Judaism offers plenty of structure to mourners, which can offer comfort and a structured space in which to grieve.
But as many rituals as there are, there are even more ways to make them one’s own.
“There’s so many ways that grief and mourning are aligned from person to person, and it is so unique and personal,” said Naomi Less, an associate director at Lab/Shul, a New York Jewish community that welcomes members who don’t believe in God. With a significant number of people who identify as Jewish also identifying as not religiously observant, that adaptability in ritual has begun to prove key to ensuring that age-old rituals stay relevant — and that even the nonreligious find comfort in spaces where those rituals are observed.
“Your own experience of grief is wildly different for each loss,” Less said.
Even with religion taken out of the equation, it can be hard to negotiate your own grief along other people’s ways of grieving. When different approaches to religion come into play, especially within a family or communal group all mourning the same loss, it can be particularly tricky.
A recent study from the Pew Research Center found that about a quarter of Jews do not identify with the Jewish religion, meaning they consider themselves culturally and ethnically Jewish, but may also identify as atheists or agnostic. That number gets higher for Jews under the age of 50, with four of every 10 Jews aged 18-29 identifying as nonreligious.
The need for common practices for handling family divides is therefore increasing. To cope with this challenge, Less suggests adding practices that feel right, rather than subtracting ones that don’t.
“If they’re doing a more traditional funeral service, maybe there’s a piece of poetry you can bring in, maybe there’s a song as people are entering the space that evokes a memory,” she said.
That approach can help make sure there’s room in mourning rituals for everyone.
Rabbi Tzemah Yoreh of the City Congregation for Humanistic Judaism in Manhattan, which also welcomes secular Jews, offers similar advice.
“Find the reading, find the piece, find the memory that you’d like to bring to the occasion,” Yoreh said. For example, many of the secular mourners he works with like to recite the Torah passage that begins, “To everything there is a season, and a time to every purpose under heaven.”
When there’s real disagreement within families over how to observe mourning rituals for a loved one, it can be helpful to bring in a rabbi or someone else who can mediate. “Sometimes it’s helpful to have somebody to sit with you to talk about these things, because the emotions are running so high,” Less said. “It’s just nice to have somebody sit with you, actively listen, share back, and try to find commonalities for families.”
When the pandemic hit, Lab/Shul, where Less works, compiled a guide to mourning for its congregants, consistent with its emphasis on artistic expression.
The guide, which is available online, is largely geared toward adapting traditions for social distancing. But it also offers ways to mix up traditions that might be more palatable to those who aren’t religious, such as making a playlist of songs the loved one liked or volunteering to honor their memory.
“It’s kind of a glossary of Jewish mourning and the cycles of mourning,” Less said. “And then it offers different kinds of ideas for creative ways to make it your own, ways to make it more personal.”
Lab/Shul also offers a weekly virtual Kaddish call that usually attracts about 20 people. She says it has been a meaningful way for mourners from all walks of Jewish life to create community.
“These folks who came because they heard about this call are now wanting to connect in person,” Less said. “There are groups that have connected in different parts of the country because folks call in from everywhere.”
For people who want to say Kaddish but don’t believe in God, the synagogue also offers alternatives to the prayer in English that use nonreligious language.
Of course, there’s no one set of customs that all secular Jews will want to follow when it comes to mourning.
“Secular Jews tend to be individualistic and are not seeking those unifying rituals, necessarily,” Yoreh said. For them, resisting structure might be part of the point.