[P]resident Trump’s Supreme Court nominee is a constitutional originalist who opposes all forms of assisted suicide and ruled twice against the Affordable Care Act’s contraception mandate but has never ruled on abortion.
Trump announced the nomination of Neil Gorsuch on Tuesday night, kicking off what Democrats have said will be a contentious confirmation process to fill the seat of the late Antonin Scalia. Gorsuch is currently serving on the 10th Circuit Court of Appeals, which holds jurisdiction over six western states
The 49-year-old Gorsuch holds a Harvard law degree and a PhD in legal philosophy from Oxford.
In 2009, he authored “The Future of Assisted Suicide and Euthanasia,” in which he argues against the practice from both a moral and legal standpoint.
“It is an argument premised on the idea that all human beings are intrinsically valuable and the intentional taking of human life by private persons is always wrong,” Gorsuch wrote in the opening pages of the book.
Federal rulings on physician-assisted suicide have been limited. Most recently, a 2006 Supreme Court ruling continued to defer to the states on the matter. In 2009, the Montana Supreme Court ruled against prosecuting doctors who provide aid in dying but made no ruling on the broader legality. But its opponents are still hankering for a fight: In a November op-ed, Wisconsin’s deputy solicitor general urged another legal battle over the issue and a change in conservative legal tactics.
In Hobby Lobby’s lawsuit challenging the Affordable Care Act’s contraception mandate, Gorsuch sided with the company in an initial circuit court ruling in 2013 as it sought a religious exemption to the mandate. The ensuing Supreme Court decision allowed privately owned for-profit companies to claim a religious objection to the mandate that they cover contraception for their employees.
In a later case also centered on the law’s contraception requirements, Gorsuch joined a dissent in a ruling that denied a motion by other opponents of the mandate claiming religious objections. The dissent blasted the majority for their “dangerous approach to religious liberty.”
With Trump’s recent executive order instructing federal agencies to “ease the burdens” of Obamacare, the contraception mandate could once again end up entangled in litigation.
On the landmark abortion case Roe v. Wade, however, Gorsuch’s appointment does not move the court in a different direction. Though he has never ruled on abortion before, Gorsuch is expected to vote as the deeply conservative Scalia did should the issue appear again before the justices.
The security of the 44-year-old Roe v. Wade ruling is among liberal groups’ chief concerns when it comes to Trump’s judicial nominees.
Trump said during the 2016 campaign that he is personally opposed to abortion, and that he would appoint judges who would overturn Roe v. Wade so that states could decide their positions on the issue individually.
Senate Republicans now face a procedural decision if Democrats try to block Gorsuch’s confirmation. Senate Majority Leader Mitch McConnell can employ the so-called “nuclear option” — which would allow Trump’s nominee to pass via simple majority rather than the usual 60-vote margin. But McConnell has in the past sounded reluctant to change the chamber’s rules.
Many Democrats, incensed that Senate Republicans never gave former Obama Supreme Court nominee Merrick Garland a hearing or vote after his nomination in March 2016, vowed to oppose Trump’s nominee even before Gorsuch was announced. It remains to be seen, however, if enough Democrats will unite to stop his nomination without a change in Senate rules.
When President George W. Bush appointed Gorsuch in 2006 to the 10th Circuit Court of Appeals, he was confirmed by the Senate with a voice vote.
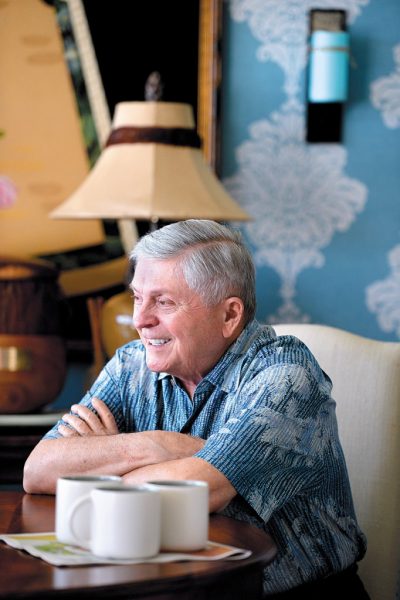
Longtime lobbyist John Radcliffe, 74, terminally ill with stage-four cancer, is working to change Hawaii’s laws that prohibit access to life-ending medication when suffering becomes unbearable
[P]utting one’s life on the line for a cause is nothing new to lobbyist John Radcliffe. The deft negotiator made a career of it. But now he literally is doing so to awaken our community to an issue.
If he and supporters are successful, Hawaii will be among seven states to legalize medical aid in dying.
Radcliffe, 74, who is terminally ill with stage-four cancer, has been in the news a lot lately to express his wish to have access to life-ending medication should his suffering become unbearable. But currently in Hawaii that is a crime.
Through legislative and legal action, Radcliffe hopes to empower individuals to make life-ending decisions that do not subject doctors to prosecution in order to assist patients in that process.
Radcliffe’s family is in full support of his wish, but unless things change, this will not be among the options available to him when he suffers prolonged, debilitating pain.
Words matter in discussing this sensitive issue. So Radcliffe is quick to set parameters on what he is — and isn’t — talking about.
John Radcliffe says if the legal system is a barrier to quality of life, you change the law
“Aid in dying is a medical practice to treat adults who are terminally ill with six months or less to live,” Radcliffe explains. “They must be mentally capable of making their own decision to request a prescription for life-ending medication from their physician, which would be self-administered.”
Aid in dying, he emphasizes, is not assisted suicide or euthanasia.
“To a terminally ill person, the term ‘assisted suicide’ is offensive and hurtful,” the Makiki resident says. “I want to live, but my condition is incurable. There is no hope for a better outcome.
“Suicide is secretive and often impulsive, without involvement of family, friends or health care professionals,” he adds.
Medical aid in dying also is known as death with dignity.
“The issue is really about dignity, pain and unnecessary suffering,” Radcliffe says. “I come from the position that you should do as much as you can as well as you can for other people for as long as you can.
“I am in a unique situation to do that,” asserts the government relations expert.
Radcliffe was diagnosed with incurable colon cancer in 2014 that has metastasized to his liver. He’s been hospitalized three times, been in the emergency room 15 times and has had 42 chemotherapy treatments.
He took his 43rd chemo treatment Wednesday, Jan. 18, while seated next to state Sen. Rosalind Baker at the opening of the state Legislature.
That’s a bit dramatic, we say about his unorthodox tactic of persuasion.
“Nah,” Radcliffe says with a laugh. “No one even noticed. That’s why I have to make a point of it. When you talk to legislators about cancer, it tends to be theoretical. Well, this isn’t theoretical to me. This is real.”
As a union organizer and lobbyist for four decades, including 13 years as executive director of the Hawaii State Teachers Association, Radcliffe knows that addressing social problems with lawmakers is not easy.
His credibility is at stake. “The legislators know me,” says the co-founder and president emeritus of Capitol Consultants of Hawaii. “They trust me. They know I won’t lie to them or give them bad information.
“But I can’t imagine that with 80 percent of voters being in support that they would be opposed,” Radcliffe suggests.
A poll conducted last November by Anthology Research shows 80 percent of Hawaii voters across all demographics believe a medical aid in dying option should be legal. Strong support (55 percent) outweighs strong opposition (8 percent) by an almost seven-to-one margin, while 12 percent oppose the option.
“This is about the ability to have a choice when you’re suffering,” Radcliffe states. “It’s comforting to some people to know they have a choice, as it is to me.
“I want to be in control of my life, as I’ve always been. It’s about quality of life. If the legal system is a barrier, ‘you change the law.’”
That’s the second strategy he and the advocacy organization Compassion & Choice Hawaii will mount after years of failing to get legislation passed.
Radcliffe, retired oncologist Dr. Chuck Miller, and Compassion & Choices Hawaii are plaintiffs in a lawsuit against the state of Hawaii asserting that the Hawaii Constitution and existing state law allow the practice of medical aid in dying.
“Mr. Radcliffe can’t wait and see whether the courts or the Legislature will ultimately solve this question, but our hope is that this option will be made available to him as soon as possible. By filing litigation now, we have put the process in motion on all fronts,” says Mary Steiner, Compassion & Choices Hawaii campaign manager.
Aid in dying currently is permitted legally in Oregon, Washington, Montana, Vermont, California and Colorado.
In Hawaii, a Governor’s Blue Ribbon panel on living and dying with dignity in 1998 recommended changing existing laws, rules and practices to give wider choices in end-of-life decisions, including physician-assisted death.
End-of-life options include declining treatment or avoiding unwanted medical treatment, palliative care (pain management) or VSED (voluntarily stopping eating and drinking).
Radcliffe’s is not the only story of a terminally ill person seeking end-of-life options. There are many stories of patients, families and friends who know the plight of long-suffering individuals.
There are heart-wrenching accounts of bewildered care-givers who experience the helplessness and difficulty of aiding agonized loved ones. They suffer in silence.
But proponents of legislation urge citizens to let their voices be heard, whether it’s by letters to legislators, testimonies to help educate the community, or joining forces to add representation to the cause.
“If this means anything to people, they must show up,” Radcliffe urges. “This is the year that this must happen.
“It’s too late for me. But it doesn’t have to be for others,” he implores.
Opponents cite spiritual, moral and modern medical advances to counter the need for more options. In fact, emotions run high when the dialogue is about death — the D word.
“Local people no like talk about dis kine stuff,” Radcliffe says.
Actually, all people don’t enjoy bringing up the subject. Talking about death is a social taboo. It’s just not done
in polite society. But with Hawaii’s aging population, it is an essential and timely topic for private and public discourse.
In Oregon, for instance, end-of-life care reportedly is improved since the law’s implementation in 1997. It is said to be thanks in large part to the dialogue the law encourages between people and their doctors.
Hospice use is high and referrals are up, as is other use of palliative care.
But what of the man to whom we address this living eulogy?
“I want to be remembered as a good, loyal friend and a decent human being,” he says.
“I hope this legislation passes without trouble,” he reflects, citing the move toward patient-directed care. “It would say something about us as a people. If we aren’t humane people, then who are we?”
As an inspired philanthropist once said, “There’s a lot of difference between human being and being human.”
Many will remember the contributions John Radcliffe has made to this community. He has spent his life fighting for causes. This will be his last and perhaps best fight.
As retired teacher Carol Sakamoto says in tribute, “Wish him well, and tell him that all the teachers will be praying for his success and thank him for his many years of service.”
That’s what living well and making a difference is all about.
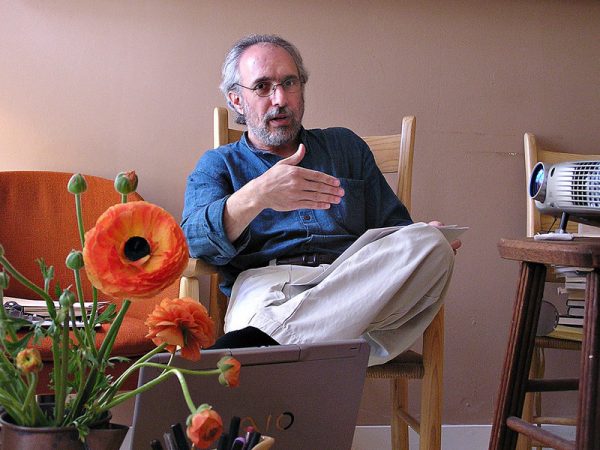
Dr. Lonny Shavelson heads Bay Area End of Life Options, a Berkeley, Calif., medical practice that offers advice and services to patients seeking aid in dying under the state law enacted last June.
By JoNel Aleccia
[I]n the seven months since California’s aid-in-dying law took effect, Dr. Lonny Shavelson has helped nearly two dozen terminally ill people end their lives with lethal drugs — but only, he says, because too few others would.
Shavelson, director of a Berkeley, Calif., consulting clinic, said he has heard from more than 200 patients, including dozens who were stunned to learn that local health care providers have refused to participate in the state’s End of Life Options Act.
“Those are the ones who could find me,” says Shavelson, who heads Bay Area End of Life Options and is a longtime advocate of assisted suicide. “Lack of access is much more profound than anyone is talking about.”
Across California, and in the five other states where medical aid-in-dying is now allowed, access is not guaranteed, advocates say. Hospitals, health systems and individual doctors are not obligated to prescribe or dispense drugs to induce death, and many choose not to.
Most of the resistance comes from faith-based systems. The Catholic Church has long opposed aid-in-dying laws as a violation of church directives for ethical care. But some secular hospitals and other providers also have declined.
In Colorado, where the nation’s latest aid-in-dying law took effect in December, health systems covering nearly third of hospitals in the state, plus scores of clinics, are refusing to participate, according to a recent STAT report.
Even in Oregon, which enacted the first Death with Dignity law in 1997, parts of the state have no providers within 100 miles willing or able to dispense the lethal drugs, say officials with Compassion & Choices, a nonprofit group that backs aid-in-dying laws.
“That’s why we still have active access campaigns in Oregon, even after 20 years,” says Matt Whitaker, the group’s state director for California and Oregon. “It becomes a challenge that causes us to have to remain extremely vigilant.”
In Washington state, where the practice was legalized in 2009, a Seattle hospice patient with advanced brain cancer was denied access to willing providers, so he shot himself in the bathtub, according to a 2014 complaint filed with the state health department.
“Refusing to provide information or appropriate referrals directly led to the unnecessarily violent death of this patient,” said the complaint filed by an anonymous hospice nurse. “I strongly believe this constitutes patient abandonment.”
Lack of access was also an issue for Annette Schiller, 94, of Palm Desert, Calif., who was diagnosed with terminal thyroid and breast cancer and wanted lethal drugs.
“Almost all of her days were bad days,” recalled Linda Fitzgerald, Schiller’s daughter. “She said, ‘I want to do it.’ She was determined.”
Schiller’s hospice turned down her request, and she couldn’t find a local referral, forcing Linda Fitzgerald to scramble to fulfill her mother’s last wish.
“I thought it was going to be very simple and they would help us,” says Linda Fitzgerald. “Everything came up empty down here.”
Annette Schiller of Palm Desert, Calif., who was 94 and diagnosed with terminal thyroid and breast cancer, had trouble finding doctors to help her end her life under California’s new aid-in-dying law.
Opponents of aid in dying cite providers’ reluctance as evidence that the laws are flawed and the practice is repugnant to a profession trained to heal.
“People consider it a breaking of professional integrity,” says Dr. David Stevens, chief executive of Christian Medical & Dental Associations, which has worked to stop or overturn aid-in-dying laws in several states.
But those decisions can effectively isolate people in entire regions from a legal procedure approved by voters, advocates said.
In California’s Coachella Valley, where Annette Schiller lived, the three largest hospitals — Eisenhower Medical Center, Desert Regional Medical Center and John F. Kennedy Memorial Hospital — all opted out of the new state law. Affiliated doctors can’t use hospital premises, resources or systems in connection with aid in dying, hospital officials said.
“Eisenhower’s mission recognizes that death is a natural stage of the life journey and Eisenhower will not intentionally hasten it,” Dr. Alan Williamson, vice president of medical affairs of the non-profit hospital, said in a statement.
Doctors may provide information, refer patients to other sources or prescribe lethal drugs privately, Williamson said.
“All we have done is say it can’t be done in our facility,” he added.
In practice, however, that decision has had a chilling effect, says Dr. Howard Cohen, a Palm Springs hospice doctor whose firm also prohibits him from writing aid-in-dying prescriptions or serving as an attending physician.
“They may be free to write for it, but most of them work a full day. When and how are they going to write for it?” he said. “I don’t know of anyone here who is participating.”
Patients eligible for aid-in-dying laws include terminally ill adults with six months or less to live, who are mentally competent and can administer and ingest lethal medications themselves. Two doctors must verify that they meet the qualifications.
Many doctors in California remain reluctant to participate because of misunderstandings about what the law requires, says Dr. Jay W. Lee, past president of the California Academy of Family Physicians.
“I believe that there is still a strong taboo against talking about death openly in the medical community. It feels like a threat to what we are trained to do: preserve and extend life,” Lee says, adding that doctors have a moral obligation to address end-of-life concerns.
There’s no single list of doctors willing to prescribe life-ending drugs, though Compassion & Choices does offer a search tool to find participating health systems.
“They don’t want to be known as the ‘death docs,’ ” says Shavelson, who has supervised 22 deaths and accepted 18 other people who were eligible to use the law but died before they could, most within a required 15-day waiting period.
Officials with Compassion & Choices said past experience indicates that more providers will sign on as they become more familiar with the laws and their requirements.
At least one California provider, Huntington Hospital in Pasadena, originally said it wouldn’t participate in the law, but later changed its position.
Other health systems have opted to not only participate, but also to help patients navigate the rules. Kaiser Permanente, which operates in California and Colorado, has assisted several patients, including Annette Schiller, who switched her supplemental insurance to Kaiser to receive the care.
Within weeks, Schiller was examined by two doctors who confirmed that she was terminally ill and mentally competent. She received a prescription for the lethal drugs. On Aug. 17, she slowly ate a half-cup of applesauce mixed with Seconal, a powerful sedative.
“Within 20 seconds, she fell asleep,” her daughter recalled. “Within a really short time, she stopped breathing. It was amazingly peaceful.”
Sue Rodriguez, of North Saanich, on March 8, 1993. Rodriguez lost her legal challenge to the Criminal Code’s prohibition on assisted death, but died in 1994 with assistance from an anonymous physician.
[S]eventy-seven people on Vancouver Island died with medical assistance in 2016, more than any other region in B.C. — and most other provinces.
Some speculate the high number might be the result of demographics and a long history of advocacy for the right to assisted death.
For each assisted death performed, between five and 10 patients are deemed ineligible, Island Health said.
A Times Colonist survey of provincial coroners, health ministries and health authories found that British Columbia ranked among the highest of medical assistance in dying, with 188 assisted deaths recorded. That was one more than Ontario, where the chief coroner recorded 187 deaths.
Prince Edward Island, with a population of 148,600, recorded the lowest number of assisted deaths at zero.
Within B.C., the most deaths were recorded in the Vancouver Island Health Authority’s jurisdiction, followed by Vancouver Coastal Health at 58, Fraser Health at 24, Interior Health at 23 and Northern Health at six.
Dr. David Robertson, Island Health’s executive lead on medical assistance in dying, said there seems to be a strong base of supporters for assisted dying, including physicians willing to deliver the procedure.
“They have made the service, medical assistance in dying, probably more available than it might be in other parts of the country,” he said.
Robertson said some support on the Island likely comes in part from the fact that Sue Rodriguez lived in North Saanich.
Rodriguez suffered from amyotrophic lateral sclerosis and wanted the legal right to end her life with the help of a physician. She lost her legal challenge to the Criminal Code’s prohibition on assisted death, but died in 1994 with assistance from an anonymous physician.
“Many of the other high-profile patients who’ve been part of the history of the change of the law come from B.C. too,” Robertson said.
He also noted that there seems to be an older, fairly well-off population on the Island.
“This is just my observation as a citizen, but we have an older population, many of whom have moved here to retire. And these are people used to making decisions that control their lives. And it seems to me not very surprising that they want to make a decision, too, about the end of their lives.”
High demand on Vancouver Island doesn’t mean there isn’t also opposition, said Eike-Henner Kluge, a biomedical ethics professor at the University of Victoria whom Rodriguez consulted before pursuing her lawsuit.
“There will always be individuals who say life is sacred and under no circumstances may you artificially end a life,” he said.
He also pointed to Victoria’s aging population as a reason for the higher demand on Vancouver Island.
“Whenever you look at why a particular medical intervention is at a certain level, you want to look at the population in question,” he said.
“You may recall Victoria used to be described as the ‘newlywed and nearly dead.’ As the population gets older, it gets more susceptible to disease and more moribund and, that being the case, you will find more individuals who don’t want to die unpleasant deaths.”
Cory Ruf, communications co-ordinator for Dying with Dignity Canada, said he couldn’t speculate on the cultural reasons why Vancouver Island might have a higher rate of assisted deaths than other parts of the country.
“But we can say that we’re in touch with at least as many assisted-dying providers on Vancouver Island as we are in Toronto,” he said. According to the 2011 census, the most recent year available, 2.6 million people live in Toronto, compared with 759,366 on Vancouver Island.
“It suggests that resources and supports for physicians on Vancouver Island may be better than they were in other parts of the country [when assisted dying was legalized]. We do know that Island Health was very proactive in devleoping its policies for medical assistance in dying,” Ruf said.
“There may be underlying reasons we can’t fully grasp in terms of culture and demographics, but I think that … in some places more than others, decision-makers have created a climate where physicians feel supported [on Vancouver Island].”
Data was not available for all provinces, including Quebec and New Brunswick.
Alberta Health Services had the most complete data, reporting that cancer, multiple sclerosis and ALS were the most cited health conditions. Some of the reasons applicants were found ineligible included a loss of capacity or competency, mental illness or death was not deemed “reasonably foreseeable.”
Four patients in Alberta were transferred from faith-based facilities for the procedure.
In Manitoba, ages ranged from 29 to 100 and averaged 70. Nine died in hospital, one in hospice and 14 at home.
Crofton’s Ernie Sievewright and wife Kay (in picture) died with the assistance of a doctor.
by Robert Barron
Surrounded by his many friends and loved ones, Ernie Sievewright finally died with dignity in his Crofton home on Jan. 15.
After wading his way through a long bureaucratic process that began late last spring, the wheelchair-bound senior from Crofton was finally allowed to legally commit suicide with the assistance of a physician on Sunday under Canada’s new Medical Aid in Dying legislation, which became law in June.
His death follows the physician-assisted suicide in their home on Jan. 11 of his beloved wife Kay.
Kay had been suffering for some time from complications of multiple sclerosis and other medical issues at a nursing home in Duncan.
That makes Ernie and Kay among the first couples to successfully access doctor-assisted suicide in Canada since the Supreme Court of Canada voted unanimously to strike down the federal prohibition against it in Bill C-14.
Bill C-14 restricts physician-assisted deaths to mentally competent adults who have a serious and incurable illness, disease or disability.
Sievewright suffered from cauda equina syndrome, a serious neurological condition that causes loss of function of nerve roots along the spinal cord.
Before his death, Sievewright said the quality of life he and Kay had was continuing to deteriorate rapidly, so they decided that death was preferable.
“It was very difficult for me to see Kay in pain all the time, and I live at home alone in a wheelchair dealing with the pain of my own illness and counting on friends to come by and pick me up when I fall,” he said.
“There’s no value in our lives anymore, so we had to ask ourselves what was the point of sticking around. We didn’t want to minimize our decision, but it was well thought out and we had discussions with friends and family. We all agreed that this was the best for both of us.”
But the approval process was long, and both had to meet with countless doctors and other specialists for their assessment and approval, so it took many months before they were finally given the green light.
Both died quickly and painlessly by lethal injections delivered by a doctor.
Sievewright invited the Cowichan Valley Citizen to his home just 36 hours before his scheduled death.
It was the happiest this reporter had seen him in the four months since I first met the Irishman with his infectious grin.
During that encounter in October, Sievewright was frustrated with all the meetings and consultations with doctors and delays he and Kay were facing in the process.
All that was in the past in the hours after he held Kay’s hands on Jan. 11 while the lethal injection was being administered to her.
“I feel really, really good,” he said at his kitchen table while friends looked on.
“I was a little upset that we couldn’t go together, but now I’m glad that Kay went first and I was with her at the time. She went so peaceful and beautifully and it was a great relief for me to see that. I’m not frightened now of my own death.”
Sievewright said he still wished the process could have been easier and quicker, but all the doctors and medical officials he and Kay dealt with were very kind, and did the best they could for the couple under the new law.
Dr. David Robertson is the co-chairman of Dying with Dignity Canada’s physicians advisory council.
He said there are no day-to-day records of exactly how many people have died through doctor-assisted suicides across Canada since Bill C-14 was legislated in June.
But Robertson said it’s been estimated that approximately three doctor-assisted deaths have been occurring a week on Vancouver Island for the last six months.
“I think the numbers across Canada are steadily increasing, particularly on the Island which has a long history of activism on this issue,” he said.
Robertson said it’s a fact that some doctors and nurses have personal views and are reluctant to participate in doctor-assisted deaths, “but many others are very willing”.
He said there are currently only 12 physicians on the Island who have taken the required training to perform the deaths, and many more are in the process of completing the education.
But Robertson said the numbers of medical staff who have the training and expertise have little to do with the amount of time it takes for people to make their way through the medical bureaucracy.
“We have the same requirements in B.C. as the rest of the country, and there are numerous documents and forms to be filled out and steps that have to be taken,” he said.
“There are very high standards to fit the criteria, so this is no simple process. It’s not a decision that patients or the medical community take lightly. We’ll continue to monitor physician-assisted suicides across the Island and the country and develop the process as we go to better fit the needs out there.”
As for Sievewright, he was just happy to finally get to the end of his long journey.
“Kay said she’d have the boat in the water with a full bait bucket and at least one dog on board waiting for me when I get there, and we’ll go fishing on flat and calm seas,” he said with a smile.
“I’m hoping that this really happens because it would be fantastic. Kay and I have lived a rich and full life. All is now in order, and we’re ready to move on.”
[K]ay Carter had been suffering from spinal stenosis for years and knew she was going to become debilitated before she would die. Rather than wait until she was no longer in possession of her own body, the 89-year-old chose to die on her own terms. She left this world peacefully at the hands of a Swiss palliative care physician with her loved ones by her side.
Physician-assisted suicide was not legal in Canada at the time of Carter’s death, and as her condition worsened she knew she would lose the capacity to consent to have a physician assist her, so she travelled to Switzerland while she was still able-bodied.
“She had a premature assisted death because she couldn’t get one here in Canada,” explained Michael Begg, a professor of legal studies at Capilano University. “Some would say that the criminal prohibition killed Kay Carter, since it forced her to die years early.”
Carter’s story made up the framework for the legal case, Carter v. Canada, which over a five-year period would challenge the Harper government to reform the assisted suicide law in the Supreme Court of Canada. Carter was able to die on her own terms, but many before her had been denied that right, and their stories date as far back as Canada’s founding.
She received death threats and found herself having to wear a bulletproof vest into the clinic where she work … Many abortion doctors who ultimately quit practicing did so because of threats or attacks made against themselves or their families.
The Criminal Code of Canada was written in 1892 according to the moral guidelines of Victorian society. Protestant Christian worldview shaped legislature, and both suicide and assisted suicide were outlawed. The taking of one’s own life was an unforgivable sin, and those who were found guilty of it could not be buried in consecrated ground or ever hope to gain access to heaven.
In 1972, the law prohibiting suicide was repealed. The right to refuse life-saving medical treatment or intervention was also introduced, giving people more autonomy over their health care. Assisted suicide was still illegal, classified as murder for which physicians could receive a prison sentence of up to 14 years, but support was growing with newfound understanding of detrimental ailments that were prolonging people’s suffering well beyond what they were willing or able to cope with.
In 1993, ALS patient Sue Rodriguez appealed for the right to die with a physician’s assistance. She argued that in not being allowed to seek help, the law circumvented section seven of the Charter of Rights and Freedoms, which guarantees any individual rights to life, liberty and security of person.
“The government can violate a Charter right – but only where the courts find the violation is ‘justifiable’,” said Begg. People recognized that in denying Rodriguez the right to die, her personal autonomy was stripped away and in essence, the government claimed ownership of her body. The Supreme Court ruled that the state of the law was justifiable. “In 1993 there was a fear of potential abuse,” Begg continued, but the fear displayed by the courts was unfounded, because at the time there was no evidence to prove that the practice of euthanasia would go down a slippery slope. Rodriguez ultimately took her own life with the assistance of an anonymous physician.
“The political parties had no will to change the law to allow assisted dying because it was such a political hot potato. Most Canadians didn’t have a strong opinion on it, liberals and conservatives were not eager to take proactive steps to change the law,” said Begg. Carter’s family challenged the law again in 2011. In the time since Rodriguez had gone to court, Oregon, Belgium, Luxembourg and the Netherlands had legalized assisted suicide and set up regimes to carefully monitor assisted death and ensure that the practice was not being abused. The Canadian courts saw this and overturned the previous ruling, legalizing assisted suicide on Feb. 6, 2015.
Legalizing assisted suicide couldn’t be achieved overnight however, so the Supreme Court suspended the law for one year so regulations could be drafted. The Harper government put off writing the bill until Justin Trudeau entered office in Nov. 2015, and the Liberal government was hard pressed to draft euthanasia proceedings in time for the Feb. 6 deadline. The bill was further extended, and on June 6, 2016 formally became law, with regulations introduced on June 17.
“This is a legal right that Canadians have but if you don’t have a provider, you don’t have access, then you can’t exercise your right,” said Dr. Ellen Wiebe, a former full-service family doctor who specializes in women’s health and end of life treatment. “When I discovered that the palliative care physicians, who normally would be doing the end of life care would not…have anything to do with assisted death, then I realized that there would be a need for providers and that I could be one.”
As one of few doctors who provide abortion services and euthanasia, Wiebe has risked her life to tend to patients. Those who she has treated have been extraordinarily grateful for her services, she explained, but certainly there have been others who have frowned upon her work.
In 1994, an anti-abortion terrorist shot her colleague, Gary Romalis. The attack put Dr. Wiebe at risk since she was known publicly. She received death threats and found herself having to wear a bulletproof vest into the clinic where she worked. Her young son was terrified, and it was his fear that caused her to wonder if her work was putting her children at risk. Many abortion doctors who ultimately quit practicing did so because of threats or attacks made against themselves or their families.
Saddened that the stigma surrounding abortion never subsided as she had hoped, Wiebe pressed on and ultimately began performing end of life care for the same reasons she had when she began performing abortions. Wiebe was determined to provide a service that few others would because it was so steeped in stigma. She calls herself an activist for complete bodily autonomy.
Following the outcome of Carter v. Canada, Wiebe had one year to learn all of the skills she would need to administer euthanasia treatment. She travelled to the Netherlands and studied under doctors who had been practicing euthanasia for years. In Canada she set up a support group where doctors could learn and support each other in preparation for June 6 when the ruling became law.
Though she has observed far greater support in Canada for the right to die since then, Wiebe knows that controversy will linger for years to come. “The support is certainly solid, but there’s still lots of people who disagree,” she said, “and that will always continue, I think, because in the Netherlands where they’ve had decades of legal euthanasia they still have people who are against it.”
There are several activist groups in Canada currently speaking out against assisted suicide, including the Quebec-based Physicians’ Alliance Against Euthanasia. The coalition has spoken out against assisted suicide on the basis that intentionally ending life is a complete contradiction of the goals of practicing medicine. Some anti-euthanasia physicians have affirmed that they will not be participating in the practice while activists have stated that they intend to reverse the law yet again and call for a total ban on assisted suicide.
The Carter v. Canada ruling stated that a physician’s decision to participate in assisted dying was a matter left to his or her own conscience or personal religious beliefs. Abortion services are the same. A medical practitioner cannot be forced to provide a service that contradicts their personal beliefs. When there are no providers, a medical service that is a right guaranteed by law is made difficult if not impossible to obtain. Criminal law is mandated at the federal level and health care is regulated at the provincial level. A province can virtually outlaw euthanasia by making it inaccessible, which can be challenged in court on the grounds that personal Charter rights have been violated.
“There is potential to use the Charter to force a particular province to make assisted death more accessible,” said Begg, but if a physician doesn’t want to see their patients die when they believe there is a chance of saving them, they can’t be forced to.
“I had a patient who chose his date six months out…and he did live that long so he was able to die on the date that he had originally chosen.”
A primary fear is that people with non-debilitating or lethal conditions will give up living if an easy death is a viable alternative.
In Dec. 2012, Belgian twin brothers Marc and Eddy Verbessem died by lethal injection after finding out that they were going blind. Already deaf, they had no means of communicating with anyone but each other and their close family. They had lived together all their lives, and their brother reported that they felt they had nothing left to live for. Knowing that they would never see the other’s face again, they couldn’t bear to go on living.
In a bizarre twist, an amendment was added to the assisted suicide bill just days after their deaths enabling minors and Alzheimer’s patients to receive an assisted death. Despite making their wishes clear, the Verbessem brothers were an unusual exception to Belgium’s laws since they were neither terminally ill nor suffering unbearable physical pain. A case of an able-bodied person with no degenerative disease killing themselves followed by additions that would allow children to die also is the slippery slope that legislators feared when judging Rodriguez v. British Columbia.
Another fear is that the sick or the elderly will feel burdened or be pressured into undergoing euthanasia by their relatives if their medical treatments are costing too much. To prevent abuse of the conditions that allow for assisted suicide, Wiebe assesses her patients before they can receive the lethal treatment.
“Certainly it’s part of our job to assess each patient and be sure that they’re not being pressured. I haven’t seen anything that made me worry,” she said. “Every one of them I am satisfied that we did the right thing and that their choice was a good one.” She consults with her patients, often with their families or support groups present, to discuss their illness and their wishes. She asks her patients about their relationships and monitors how they interact with their family members before making a final judgement. It’s a subtle but obvious way, she said, to be sure that their wishes are entirely their own.
Patients are also required to undergo a 10-day reflection period before euthanasia will be administered. The reflection period was mandated to prevent patients from making hasty decisions after being diagnosed.
“There’s two reasons we’re allowed to shorten up the time from the 10 day reflection period, and those are somebody’s in danger of losing capacity — losing the ability to consent — or in danger of dying in those 10 days,” Wiebe explained. “I’ve had people who are within 24 hours of death, for example, and those have to be done very quickly, and others spend a long time deciding. I had a patient who chose his date six months out… and he did live that long so he was able to die on the date that he had originally chosen.”
Since June 6, Wiebe has consulted with over 100 patients and assisted 40 of them in ending their lives on their own terms. “It is wonderful work. Doctors love having grateful patients and I have the luck of being able to do something that people really appreciate,” she said.
The battle for the right to die has hardly abated. The regulations were written hastily so that they would meet the Supreme Court deadline of June 6, and as a result many Canadians believe the laws to be too restrictive. Safeguards such as the mandatory waiting period ensure that vulnerable people cannot undergo euthanasia before the terms of their illness have been fully processed, and two witnesses are required to attest to their wishes.
“The biggest of the flaws in the Trudeau government’s bill, critics say, is that the Criminal Code only allows assisted death for those who are facing imminent death,” said Begg. Only those suffering from a terminal condition can seek assistance, omitting hundreds of people who are suffering irreparably but not likely to die. People like Kay Carter, who would have lived in agony.
Most of us wonder, every once in a while, when we might die.
Noreen Campbell knew it would be Thursday and it was.
On Monday, she walked from her kitchen into her sun room, which looks onto a rural North Saanich property.
“I’ll go in here,” she said, sitting down in an overstuffed, beige leather chair. Her daughters, Mary and Jane, would be at either side, she said, and her husband, Cliff, would be there, too.
Campbell, 71, could still walk, talk and form coherent thoughts. She wasn’t bound to a hospital bed or so far gone that her family had to wonder about her level of consciousness. But as a registered nurse for 53 years, she had watched many people suffer in their final days and said she had reached her threshold.
“Some people might think I’m too capable, but why should you wait until you have to roll me in?” Campbell said.
“I’m ready.”
Campbell was among the first to receive approval for medical assistance in dying. That was in August, two months after landmark legislation was enacted to allow the procedure in Canada.
She chose to share her story in the hope that it might open the door for others facing death and draw attention to gaps she saw in the process. “I have this feeling that if you’re not part of the solution, you’re part of the problem. With my background, the failure to do something would be negligent,” she said.
“I believe this is the message: To reassure patients and their loved ones that there is an alternative — and give them hope and courage.”
Campbell’s health decline began with a bit of discomfort in 2012. She had a toothache that wouldn’t go away.
“One day, I was sitting and thinking and it was like a smack to the side of the head. I was the educator for the surgical unit that does oral cancer and I thought to myself: ‘What would cause the pain to stay in the same place, be consistent and get worse?’ I asked for a biopsy. And I had very extensive oral cancer,” she said.
“I think it was missed because I’m not a smoker.”
She underwent surgery to remove tissue and bone in her face and jaw, alleviating what had become horrific pain.
About a year after the surgery, she was diagnosed with chronic obstructive pulmonary disease, which is a progressive obstruction of airflow into or out of the lungs.
As a nurse, Campbell had watched many people die. Her worst fear was respiratory disease, she said, having seen, more than once, the extreme suffering of a person who is desperate for air. Faced with the same future, she began planning a trip to Switzerland, where assisted dying is legal.
A Supreme Court of Canada ruling in May 2015 meant she wouldn’t have to make the trip.
The assisted-dying movement largely began in Canada in the 1990s, with Sue Rodriguez, also from North Saanich.
Rodriguez suffered from amyotrophic lateral sclerosis (ALS) and wanted the legal right to end her life with the help of a physician. She lost her legal challenge to the Criminal Code’s prohibition on assisted death, but died in 1994 with assistance from an anonymous physician.
More than 20 years later, in 2015, the Supreme Court unanimously voted to strike down the prohibition and allow medically assisted death. It was legalized with passage of the Medical Assistance in Dying Act on June 17, 2016.
Two days later, Campbell submitted her application.
“I was ready,” she said.
Noreen Campbell underwent a medical assistance in dying procedure Thursday, here she spends time with her horse Dasha in Victoria.
Campbell told her doctor she wanted it as a backup. A respiratory infection could put her in the agony of not being able to breathe and she wanted the power to control her end, if that was the case.
“Simply put, I’d rather end it in two minutes than two days.”
Gradually, her disease progressed to the point where symptom management became a 24/7 job, she said. It had been years since her health began to decline and it became clear that she was dying.
“I think it is this perfect storm. It’s not one symptom, it’s things coming together and they just start to pile up. It’s not just my inability to breathe or my jaw pain. It’s everything. And when you know, ‘This will not get any better’ … there’s a point where you make your decision. And my point was when I was overwhelmed and I felt like I could no longer cope.
“I am dying. I am getting weaker. I can do less, symptom control is overwhelming me. I’m going to die; end of story. And I suddenly get this choice: Do I want to die in less than five minutes? Compared with [experiencing what] the people I’ve witnessed who died over hours and days went through — there is no choice. Otherwise it’s called torture,” she said.
Campbell pressed her finger over her breathing tube each time she spoke, allowing air to pass through her voice box.
Facing death made her reflective, she said.
“We all know we’re going to die, but we don’t have it in our heads. I think, culturally, we have a lot of escapism. When you look at the time before antibiotics, in the 1900s, you were grateful to be alive. But in the 2000s, we’re looking for a way to get out of this life. We have not prolonged healthy living; we have prolonged life by preserving chronic illness.”
After so many years serving at bed sides, she said being in a hospital bed and then as an at-home patient gave her a new perspective on care. Not enough attention is given to a patient’s suffering or quality of life and patients still aren’t provided with all the information they need to make informed decisions, she said.
It begins with doctors talking over a patient’s head — though in her case, she understood what they were saying. And it continues with the difficulty of obtaining information about medical assistance in dying.
Campbell said ambiguity in guidelines from the College of Registered Nurses of B.C., accompanied by recommendations to consult your employer and legal representation, for example, would discourage nurses from communicating with patients about the option unless they ask for it specifically. “I see this as an absolute conflict with suicide-prevention guidelines, which say, if someone walks in and says ‘I can’t go on,’ my question [as a nurse] should be, ‘What’s the matter?’ Not, ‘I can’t talk about that,’ ” Campbell said.
Before Bill C-14 passed into law in June, the federal government added conditions that would exclude many individuals from medical assistance in dying, arguing it needed to protect vulnerable people. It limited the right to mentally competent adults who are suffering unbearably, in an advanced and irreversible decline and whose natural deaths were reasonably foreseeable.
The law has been simultaneously celebrated for opening access, challenged on the basis that it would conflict with medical staff’s freedom of religion and criticized for being too narrow.
Justice Minister Jody Wilson-Raybould has said if assisted-dying was available to anyone suffering from a serious medical condition, then it would be an option for survivors of sexual abuse and soldiers with post-traumatic stress disorder. And the Council of Canadians with Disabilities has said the act needs more restrictions to protect people with new disabilities, who might feel hopeless before they adjust to their new reality.
A 25-year-old woman with spinal muscular atrophy has launched a constitutional challenge, with the B.C. Civil Liberties Association, to expand the right beyond those facing “foreseeable” death.
For Campbell, too, the law doesn’t go far enough. The requirement of “foreseeable death,” doesn’t take into account what can be unbearable suffering from chronic illness.
Suffering, she said, is not always a virtue.
“We should be looking more at what quality of life means to people,” she said.
“I think suffering, pain, does help people mature. That’s the difference between being a kid and an adult. Even if it’s your first broken-heart romance and you see the dud later and think, ‘Thank God,’ there’s a certain amount of pain that’s necessary to make us an understanding society and for people to develop empathy and sympathy. But the idea that suffering is always worthwhile, it’s just beyond me.
“From the time when I was approved, from the time I decided, ‘yes,’ I would say I have experienced the most calm. It’s hard to imagine, but it’s given me a chance to do things,” Campbell said, when asked if she was afraid of death.
She completed a manuscript on wound care, her specialty as a nurse. She became an honorary member of an East Coast chapter of the activist group Raging Grannies (she asked that the story end with “Rage on!”). And she published a video explaining her choice with the advocacy group Dying with Dignity.
She said she didn’t believe in bucket lists — they just cause anxiety. But the knowledge that she would get medical help in dying, when it was time, meant she didn’t have to waste time wondering.
“The other thing we don’t have is a roller-coaster. When you have people who are chronically ill, they’re desperately ill, then recover, then desperately ill, then recover. When you have medical assistance in dying, your focus can be on a comfortable death.”
On Thursday, she went into her sun room and sat down with her family. Her physician gave her a sedative, then via IV, something that would stop her heart. But first she sent the following in an email:
“This is my day — I was able to watch my grandson play hockey, we have had a string of celebrations — tears sure — but so much laughter. Thank you Canadians for making a peaceful death possible for me and sparing my family and friends from witnessing a death with fear and suffering.”