On July 14, 2014, my husband David and I sat down with our children to disseminate and discuss our health care advanced directives. It was David’s 69th birthday; he died about 2 months before his 70th.
David had endured several years of ill health, culminating in the removal of a kidney. In June, the month prior, we learned that the cancer had metastasized to his bones. As a couple, we wanted to make sure that all of the children understood our desires for end-of-life care. Thankfully we had had the foresight to discuss a broad variety of medical treatment options dispassionately, years before there was any urgent medical necessity. Suddenly those decisions became radically more real.
For 10 months, David endured two different rounds of chemotherapy, neither of which had the desired effect of stopping the cancer that was destroying his bones and causing unimaginable pain. He persevered through the agony of trying to move while his bones were crumbling. Radiation impacted his ability to swallow and to enjoy food, which became a non-option when he had a feeding tube inserted. We watched him fight and waste away, fight and waste away, yet always with the hope that one more treatment would be successful where others had failed.
We had talked about nutrition and hydration at the end of life, about ventilators and surgical intervention in the face of terminal illness, but we had not addressed the fundamental question that The Conversation Project urges us to consider: “What matters to you most at the end of life?”
Dr. Atul Gawande, author of “Being Mortal: Medicine and What Matters in the End” and a leading thinker about the role of the medical profession in caring for patients whose time is limited, reminds us that people have a broad variety of concerns besides prolonging their lives.
Doctors are trained to view death as the enemy and to battle on until the end. At some point, the battle was lost. Among David’s final words were, “Why didn’t he (the doctor) tell me it was so bad?”
Gawande writes that, while there is nothing wrong with sustaining hope, it is problematic if it prevents us from preparing for the more likely outcome.
He writes, “We’ve created a multimillion-dollar edifice for dispensing the medical equivalent of lottery tickets – and have only the rudiments of a system to prepare patients for the near-certainty that those tickets will not win. Hope is not a plan, but hope is our plan.”
The Conversation Project is an important first step in considering what we each might value most if we have the luxury of knowing that our time is limited. What would be a good enough day to want to go on, and what is the tipping point where we would be ready to let go? The answer will be different for each of us, and we must have the conversation now.
David felt loved until the very end; he enjoyed the best possible support from friends, family and community. And, I wish that we had had more time to lay down our swords, to cease the raging battle, and to have quietly enjoyed more the time with which we were blessed.
Our culture is changing and growing and learning. The Deutsch Family Shalom Center at Temple Chai recently hosted more than 100 individuals who courageously undertook the first steps to have “the conversation.”
At 10:30 a.m. on Sunday, Jan. 8, we will gather to share our experiences and address other concerns as we move forward in these challenging and uncharted waters. Attendance at the first gathering is not required.
What a gift to our family and loved ones to ensure that our financial affairs are in order, our burial arrangements are understood, and to have articulated our answer to that question, “What matters to me at the end of life is…”
Siblings Elizabeth H. Moore, left, Samuel P. Harrington, Hannah H. Graziano and Jane H. Coble worked together to fulfill their father’s goal of dying at home.
By Samuel Harrington
The blessings and curses of families are not limited to holiday gatherings, graduations, weddings and funerals. They also exist at the transition of the matriarch or patriarch from life to death.
Like many elderly Americans, my father wanted to die at home. He was clear on that point. But also like many elderly Americans, he gave mixed signals about what treatment he would accept or decline with that goal in mind.
So when at age 92 my father began his decline from aging with grace to decaying from old age several years ago, my sisters and I began creating a plan that would allow him to reach the end as he wished.
First, we reinforced his household help. Then we scheduled a series of periodic days-long supportive, reconnaissance visits. (None of us live near him.) My father told us that he did not want to be resuscitated if he collapsed. But how should we deal with a nonfatal emergency without losing him to overly aggressive care? Would it be possible, in fact, to do nothing?
My siblings deferred to me, the only physician in the group, for medical advice. My oldest sister was the first to visit his apartment in our new rotation. Knowing his desire to die at home, she was anxious about what she should do if something happened, and she peppered me with questions.
“What should I do if he falls and hurts himself?”
“If he is in pain, call 911, then call me.”
“What should I do if he seems to be having a stroke?”
“Call me. And if you can’t get me right away, call 911.”
“What should I do if he gets pneumonia?”
“Call me.”
“What if I find him dead in bed?”
“Wait until he is cold and blue, then call 911.”
“Okay. I get it.”
After digesting my responses and discussing them with our two other sisters, she typed up a plan that carefully explained our reasoning. She (or whoever was visiting) was to call for help if our father was in pain. Whoever was in attendance was not to take action about other medical problems until I had a chance to weigh in.
Most families are not as united as my sisters and I were around the concept of a painless death at home. If the opportunity for such a death arose, we would seize it. This is what his advance directive stipulated, and it is what he frequently verbalized. “I have lived too long” and “I want to wake up dead” were his mantras. We wanted to honor his wishes.
Participation in the slow decline of an aged parent comes with obligations. There are dues to be paid — for example, showing up regularly for visits, no matter how inconvenient, and taking time to check in with siblings and provide detailed updates. Teamwork, coordination and cooperation help smooth this emotion-wrought journey. When family members do not or cannot work through disagreements, the result can end up punishing the person everyone is trying to comfort and protect.
Unfortunately, my experience as a physician and hospice trustee has shown me, an odd sort of competition can crop up in these situations. Some patterns are predictable. The most common is when siblings compete to prove who cares the most. This is frequently seen upon the arrival of an estranged family member at the deathbed, and it has been described in medical journals as “The Daughter From California Syndrome.” Classically, the syndrome unfolds as the guilt-ridden newcomer urges overly aggressive treatments.
Other patterns are less predictable. In some families, a previously restrained sibling will assert dominance as the designated agent or proxy with power of attorney for health care. That one child has been designated as health-care proxy is not to be envied or taken as a sign that he or she is preferred over another.
Sometimes a financially successful sibling will dominate the decision-making, thinking that the managerial skills that built their business will now translate into medical decision-making ability.
Frequently, religious schisms will arise. I have seen, for example, one sibling’s conservative religious belief that the patient should fight on compete with another one’s new age spirituality urging everyone to “let go.”
The fault lines in decision-making that result from any of these scenarios will prolong some aspect of the dying process, usually to the detriment of patients like my father who have asked for a non-medicalized death at home.
Even though a single person (the competent patient or the health-care proxy for an incompetent one) has the technical responsibility and authority to make difficult medical decisions, the choice to accept or decline a high-risk procedure — such as heart-valve replacement or emergency surgery — is usually the result of a discussion among family members during or after a consultation with the treating physicians.
This is because these discussions most often involve a sick, weak, impaired elderly parent or grandparent and a de facto family committee. It is the rare physician who will exclude family members from a consultation and limit the discussion to the one with power of attorney. It is rarer still for a physician, in the heat of urgent care, to parse the advance directive signed by the patient specifying what they do — and don’t — want if an agitated family member is demanding action.
Doctors are most comfortable proceeding with a high-risk treatment or withdrawing life-sustaining technology such as a mechanical ventilator when the family is unified. On the other hand, if the family is fragmented, doctors are more likely to move the conversation toward, and then proceed with, what they think is “best.” Often this will be an expedient combination of what is medically acceptable, legally conservative and reflective of the doctor’s best interpretation of the family’s majority opinion, even if it defies the patient’s wishes. What the doctor thinks best will also likely be influenced by his or her own end-of-life philosophy.
I have seen many families unable to come to agreement. I have seen many patients overtreated or undertreated in defiance of their wishes. I have seen agonizing scenes of dysfunction, such as a son demanding that cardiac resuscitation be performed on his just-deceased mother. This situation occurred because the mother did not include him in her final conversation with physicians, when she changed her status from “full code” — which had instructed them to intercede if her heart stopped or she stopped breathing — to “do not resuscitate.”
Although my family was in good agreement about my father’s wishes to die at home and to take no measures to prolong his life, our tools were limited. He was not yet a candidate for home hospice — that requires a life expectancy of six months or less — and a new type of very specific advance directive (called a POLST order) was unavailable to him.
In the absence of such orders, I could think of various scenarios that would test our teamwork and resolve.
What if our father developed exceptionally upsetting symptoms such as seizures or massive bleeding from the bowels? What if he became unmanageably delirious? What if the “need” for emergency surgery arose because of a bowel obstruction or a fall with a major fracture?
Would the pain compromise his resolve to use such an acute medical problem as an “exit strategy,” a way to die naturally? Would one of us become guilt-ridden about our “active passivity” regarding medical intervention? At the very end, the inability to “let them go” is a common development.
Fortunately for my siblings and me, there were no dramatic decisions to make in the two years between our first family consultation and my father’s death at age 94. A year before his death, he had stopped seeing his physicians for checkups. Six months before his death, he enrolled in home hospice, and three months before the end, he stopped taking his non-palliative medications (blood pressure pills, cholesterol lowering pills, water pills, potassium supplements).
“This will be our last visit,” my father said as I kissed him goodbye and left for the airport following a 10-day visit. He was prescient. My oldest sister arrived the next day, and he died two weeks later. I was tempted to return as it was clear the final day was approaching, but there was little point. We had all said our goodbyes. We had all reconciled ourselves. The hospice nurses were visiting him daily, and he was protected, as he wished, from aggressive intervention. The eldest embraced her responsibility to care for him, and the rest of us embraced our obligation not to interfere. We were a team. We were his family.
Harrington, a retired gastroenterologist and former hospital trustee in the Johns Hopkins Medical System, is writing a book about end-of-life decision-making.
Physician Orders for Life-Sustaining Treatment, or POLSTs, are available in about 25 states.
Unlike a traditional advance directive, which expresses wishes in general and requires interpretation by emergency and hospital physicians, POLST orders are developed and signed by the patient’s primary-care physician to expand “Do Not Resuscitate” orders to include options for comfort care only or to set limitations on breathing support, feeding tubes, antibiotics, transfusions, etc. When they arrive in the emergency room with the patient, these orders are immediately implemented and require no interpretation by emergency physicians. They are appropriate for seriously ill or elderly, frail patients.
More information about POLST can be found at polst.org.
Cecelia Clayton, MPH, is the executive director at Karen Ann Quinlan Hospice.
Q: How can I learn more about advance directives/advance care planning?
Cecelia Clayton
A: During National Hospice Month it’s important to know your options. All adults can benefit from thinking about what their health care choices would be if they are unable to speak for themselves. These decisions can be written down in an advance directive so that others know what they are. Advance directives come in two main forms:
Proxy Directive (Durable Power of Attorney for Healthcare)
A proxy directive is a document you use to appoint a person to make healthcare decisions for you in the event you become unable to make them yourself. This document goes into effect whether your inability to make healthcare decisions is temporary because of an accident or permanent because of a disease. The person that you appoint is known as your “healthcare representative” and they are responsible for making the same decisions you would have made under the circumstances. If they are unable to determine what you would want in a specific situation they are to base their decision on what they think is in your best interest.
Instruction Directive (Living Will)
An instruction directive is a document you use to tell your physician and family about the kinds of situations you would want or not want to have life-sustaining treatment in the event you are unable to make your own healthcare decisions.
You can also include a description of your beliefs, values, and general care and treatment preferences.
This will guide your physician and family when they have to make healthcare decisions for you in situations not specifically covered by your advance directive.
Advance Directive: Your Right to Make Health Care Decisions
You have the right to:
Ask questions about your care.
Completely understand your medical condition.
Accept or refuse any treatments.
Make future decisions by completing an advance directive.
If you have a life-limiting illness — you have the right to choose the hospice of your choice.
Karen Ann Quinlan Hospice has ready-made packets with current Living Will information available at no charge. The packets can be picked up at the desk at the hospice office at 99 Sparta Ave, in Newton, or call the hospice at 973-383-0115, or at 800-882-1117 to have one mailed to you.
Free seminar
More information will be available at the “Ask An Elder Law Attorney” seminar that will be held from 10:30 to 11:30 a.m., Dec. 8 at the Pike County Public Library in Milford, Pa.
The event is free to the public and light refreshments will be served.
Attendees will be able to ask questions about elder care, estate planning, living trust, last will and testament, advance directives and more. For more information, visit www.KarenAnnQuinlanHospice.org/Seminar.
Here is a checklist to consider to plan ahead or if you need help now.
Get the information you need to make informed choices about end-of-life care.
Get to know end-of-life care services that are available, such as hospice and palliative care providers.
For information, visit the National Hospice and Palliative Care Organization’s website: www.nhpco.org
Discuss your thoughts, concerns and choices with your loved ones.
Talk to your doctor about different treatments.
Establish advance directives (a living will and medical power of attorney) for your state.
Talk to your healthcare agent, family and doctor about your choices.
Discuss your choices often, especially when your medical condition changes.
Keep your completed advance directives in an accessible place.
Give photocopies of the signed originals to your healthcare agent, alternate agents, doctor, family, friends, clergy and anyone else who might be involved in your healthcare.
Assess your financial situation, create a financial inventory and determine what end-of-life goals you want to accomplish that involve money.
Learn about the cost of end-of-life care, how medical bills and expenses will be paid for if you are not able to.
Make financial decisions such as how you want to give your money and possessions to others upon your death.
Prepare for the time when you cannot handle money matters; appoint a durable power of attorney.
Plan your funeral/memorial service.
The living will is a direct result of the Karen Ann Quinlan landmark case won by Joseph and Julia Quinlan in 1976 on behalf of their daughter, Karen Ann.
‘You get to die only once, and you have one chance to get it right’
By Alan Kirk
Discussing your end-of-life plans is about making your death less traumatic for your family and loved ones, and having your own wishes respected, as much as possible.
[H]ow would you like to die? Is this a question you ever ask yourself? More importantly, is it a question you ever answer? And, most importantly, is it an answer you share with your family?
For many it seems, the answer is no. Yet, when asked, it is something many of us would like to do. When the Irish Hospice Foundation (IHF) carried out research, they found 60 per cent of people thought there wasn’t enough discussion about death, yet 66 per cent have never discussed what they want around their end-of-life care with family.
“It’s a clear case of what people want versus what people do,” says Sharon Foley, chief executive of the IHF. “You get to die only once, and you have one chance to get it right. It’s so important to think about what you want for yourself at the end of life, now, while you still have capacity, to ensure the proper care and support for you, and less trauma for your family and loved ones.”
>When the doctor asked to talk to my dad and I, and we followed him into a side room, I knew it wasn’t good. All previous conversations had been in the ward corridor. This room had comfy chairs and a box of tissues. The room itself was the opening conversation about my mum’s death. He sat us down and explained that my mum’s stroke had been catastrophic causing significant brain damage, paralysis, double incontinence and that her chances of survival were not good. I had seen enough of my mum to know also that, if she did survive, her chances of living were not very good either.<
The doctor asked us what we wanted to do, if my mum needed to be resuscitated. Neither of us hesitated or even looked at each other to confer. We both said immediately, “Do not resuscitate.” We were lucky. We knew what my mum would have wanted. She had told us often enough. But I often wonder what would have happened if we had looked at each other first, and one of us defiantly had said yes.
But this is what often happens, as the decision over a parent or spouse’s death is left up to family members who are already in a deep place of distress. We know medical science is improving all the time and people are living longer, an obviously positive development. But it is also a challenge to respond to the care needs of an ageing population. While the medical profession has rightly focused on quantity of life, has society focused enough on the issue of quality of life? And, in particular, end of life?
According to Foley, no. “I liken it to the discussions in the 1980s around breast cancer. Women didn’t discuss it with friends. There were whispers about the ‘Big C’ and, as a result, women didn’t get screened, or get any support. Now screening and support are a part of life. We need the same sea change around our wishes regarding end of life.”
Critical conversation
For obvious reasons, thinking about our, or our parent’s death, is an upsetting notion, but, as Justin Moran of Age Action explains, it is critical to have that conversation while you still can. “We all think and prepare for what we leave behind in terms of our house and our legacy, but what about your own death? Thinking clearly about how you might want to be treated – or not – and ensuring decisions aren’t left to those you are leaving behind is about empowering people to make decisions for themselves while they can.”
The Irish Hospice Foundation encourages people to give guidance to family through a a campaign called Think Ahead and Have Your Say campaign, and this year legislation has come out introducing the opportunity for us all to leave a “living will”.
The Advanced Healthcare Decisions Bill gives people the chance to communicate their final healthcare requests when they might no longer be in a position to do so, and to provide healthcare professionals with important information about the patient’s treatment choices. You can also appoint a designated healthcare representative – a close friend or family member – to make healthcare decisions on your behalf if you no longer have the capacity to make those decisions.
A good death
“There is a lot of debate around what a ‘good death’ is,” says Foley. “This is about making death – something already heartbreaking and distressing for all – as respectful to the wishes of the patient as possible.”
Justin Moran acknowledges these are hard conversations to have with our parents or children. “It’s about ensuring that you retain as much control as you can over that part of your life.You don’t want to leave that responsibility to the people you love, who are already going through a tough time.”<
But is it enough? Back in that hospital room, we agreed to a DNR if my mum stopped breathing. But it was another five and a half years before she took her last breath. In the final months, in consultation with doctors, we took a further step to withdraw active life-prolonging treatment after she suffered a series of hospital-admitted infections which caused distress to everyone, especially her. We knew my mum’s wishes. But even at the end all we could do was withdraw treatment and wait and watch for the several weeks that nature took its course. She was never in pain. But she was distressed. She watched us, watching her die.
In many ways my mum had a “good death”. She died in my arms at home, with my dad and brother holding her hands. We had spent the previous two weeks constantly by her side, talking and touching, loving and laughing, holding her tight and letting her go. But, as her daughter, it was a terrible death.
Once we knew she was dying, once doctors confirmed she had passed the point of any recovery, there was nothing we could do but let her linger and languish as her body slowly shut down. She could easily have died when we had nipped to the loo, or gone to put the kettle on. The stress of that fear haunts me still. The conversation about dying has only just begun. But, for now, if we love the life we live, if we love the family we leave behind, if we want to be in control of our living, then as a society and individually, we need to talk more about dying.
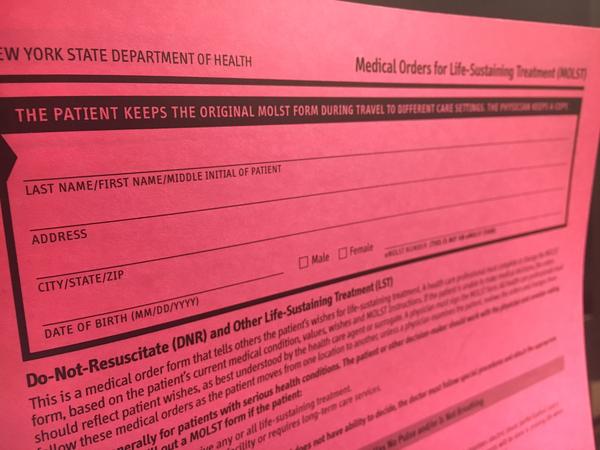
The top portion of a paper MOLST form. It says, “The patient keeps the original MOLST form during travel to different care settings. The Physician keeps a copy,” on all four pages.
Dennis Rodgers flips over a bright pink piece of paper and rattles off his choices: “Attempt resuscitation or do not attempt resuscitation… to do limited intervention or to take no medical intervention… and another section, whether to intubate or not to intubate.”
Rodgers, 82, says he and his physician filled out the form together when he moved to a community outside of Rochester, N.Y.
For years physicians in New York state have asked seriously sick patients to fill out this paper document, capturing their wishes in case of emergency.
Most Americans don’t plan ahead for end of life. But for those who do, like Rodgers, there’s a risk that the right people won’t even see the document when it really matters. After all, a piece of paper is easily lost or left behind in an emergency.
Advocates and lawmakers in New York are now pushing to shift the paper system to a mandatory electronic database for better access. But the requirement would call for a technology fix that’s not coming easily.
Most states have some version of these documents, typically called a Physician Order for Life Sustaining Treatment, or POLST. In New York state, the form is called MOLST. It stands for Medical Order for Life Sustaining Treatment.
Unlike advance directives, the MOLST form is a detailed legal document, prepared with a physician. MOLST forms are not meant for the general population. They’re meant for patients who physicians suspect may die within a year.
Without a POLST-like form, physicians or paramedics are trained to keep someone alive including aggressive life-sustaining treatment, if need be.
Nearly everyone benefits if patients make their medical wishes clear. Patients make sure they’re not subjected to measures they don’t want. Family members don’t have to wonder. And insurance companies can save money.
End of life care is one of the biggest medical expenses in our health system. About a quarter of traditional Medicare costs are for expenses patients incur in their last year of life, according to a report from the Kaiser Family Foundation.
“The majority of states right now have a POLST process. The question is how effective is that process if I can’t get access to that as a health care provider?” asks Rick Bassett, chair of the national POLST technology committee.
A handful of states have established electronic databases for these forms — eMOLST is New York state’s version. Lawmakers are considering a bill that would require doctors to submit an electronic version when they fill out a hardcopy within 14 days.
In theory, this would ensure access to the form no matter which clinic or hospital a patient may end up in during an emergency, explains Patricia Bomba, vice president and medical director of geriatrics at Excellus BlueCross BlueShield and director of the MOLST program.
“It just is the better way to do it,” she says.
Excellus currently funds the MOLST and eMOLST systems, 100 percent.
But even the electronic solution has its own problems to work out.
“Even if you fill out one of these forms — having it actually pop out in front of the right person at the right time has been a really big challenge,” says Kirsten Ostherr, a Rice University professor focusing on health and medical digital media.
There are major access issues, Ostherr says, in general, when it comes to electronic medical records. For one, different hospital electronic record systems don’t link to each other or to the E-MOLST database, which is separate. And outside providers, like paramedics don’t usually have access to these systems.
The current eMOLST system is just not accessible for busy doctors, explains Daniel Mendelson, director of palliative care and associate chief of medicine at Highland Hospital in Rochester.
“Expecting a medical provider to look in their own record is reasonable. Asking them to look at an outside record and multiple outside records is probably not going to happen,” he says.
Mendelson was on the original team that developed the paper MOLST form in New York. He’s a self-described “power user” and embraces technology. But he doesn’t use eMOLST because it doesn’t directly connect to the system his own hospital uses for patient information.
For his own father, he trusts the paper form more than the eMOLST system.
“It’s not that people are not hardworking and well meaning, but how many tasks can you load somebody with in an emergency?” Mendelson asks.
At least two hospitals in New York state have successfully developed a direct connection between an electronic health records system and eMOLST.
The in-house information technology team at NYU took a few months to work on the connection, start to finish, according to Christine Wilkins, advance care planning program manager at NYU’s Langone Medical Center. Providers can use one password to sign on and view medical records and a patient’s eMOLST.
Wilkins says they hope the easier to use technology will help doctors start using eMOLST more. And that will ultimately benefit patients.
“It’s about having a more robust conversation, but then, it’s having a much better way to document what their wishes are. And for that documentation to be seen across the board,” Wilkins says.
Another hospital, Orange Regional Medical Center, in Middletown, N.Y. also established single sign on for its providers earlier this month.
Currently, the eMOLST system has roughly 10,000 patient files, according to Katie Orem, eMOLST administrator at Excellus BlueCross BlueShield. That’s about 10 percent of New York state residents who die from chronic disease every year, she says. If the bill passes, New York would have a statewide database.
Never mind assisted-dying, our health care system needs to change the way it deals with the natural end of life
By Mohamed Dhanani
Mohamed Dhanani, left, with his father-in-law Ijaz Ahmad at a wedding last year. “The eight different doctors who treated my father-in-law all had different ideas about what (his wishes not to be life support) meant, and how involved the family should be in making treatment decisions,” writes Mohamed Dhanani. “This inconsistency — the waiting, the arguing, the feeling of powerlessness — was our family’s worst experience with a health care system of which we are so often proud.”
I’ve spent much of my career in the health care field, but it took a very personal experience to drive home just how poorly prepared health care providers are to help us through the one certain life-experience that awaits us all: death.
It happened in a hospital in southern Ontario. My father-in-law, Ijaz Ahmad, who lived with insulin-dependent diabetes for 35 years, went into the hospital for a partial foot amputation due to a bone infection.
Prior to surgery, a routine diagnostic test was performed requiring dye to be inserted into his bloodstream. After the surgery, the dye put him into kidney failure while it was being metabolized. Within a day of the surgery all of his organs started to fail and he was put on life support for what we were told would be two to three days so his organs could rest and strengthen — after which, we were told, “the doctors would bring him back.”
He spent the next 18 days on life support. And what became clear over that long 18-day ordeal is that what had clearly become the end of his life would have been unnecessarily prolonged depending on which of the eight doctors we interacted with was treating him that day.
Like so many families who have had the difficult but essential conversation with an aging parent around their end-of-life wishes, we had spoken with him about his wishes. He was clear he did not want to be on life support.
The eight doctors who treated my father-in-law all had different ideas about what those wishes meant, and how involved the family should be in making treatment decisions. This inconsistency — the waiting, the arguing, the feeling of powerlessness — was our family’s worst experience with a health care system of which we are so often proud.
Some of the doctors acknowledged his wishes but said life support was an essential part of the treatment plan; it was just a temporary measure to aid in his recovery. Others made very little effort to consult with us, and another outright refused! Another doctor assured us he would “bounce back,” though nurses told us this was increasingly unlikely and that the doctor was prone to sugar-coating discussions with families.
Because of this inconsistency, different members of my family were hearing different things — and that made it even more difficult for us to make a decision we all felt comfortable with. Finally, I pulled aside the latest doctor treating my father-in-law and asked him for an absolutely frank and direct discussion. Only then were we able to make an informed decision that respected my father-in-law’s wishes and provided as much comfort as possible to our family.
On my father-in-law’s 18th day on life support, and on what was to be the final day of his life, a new doctor was treating him. This doctor had trained and practiced in the U.K., and had only recently started to work in Ontario. His European training and experience gave him a different perspective on end-of-life care, and one for which we were grateful.
In Europe, the societal conversation on end-of-life care is more advanced than in Canada — they have grappled publicly with these essential issues of decision-making in health care for many years, and physicians have therefore become more comfortable discussing end-of-life decisions with their patients and families.
Not only is this an essential conversation we need to normalize as families and as a society, it is something our health care system must take on as an essential part of its work. All doctors must be trained to discuss end-of-life care in a direct and compassionate way with patients and their families. This will only become more important as people live longer, and as their health issues become more complex as they reach the end of their lives.
Over the last few years, Canadians have engaged in an impassioned debate on assisted death, a debate that culminated in landmark — and controversial — legislation in Parliament. But assisted death is just a small part of the issue.
As my family’s experience illustrates, end-of-life care and the difficult discussions surrounding that care are too inconsistent — inconsistent between institutions and inconsistent between doctors within a single hospital. It is something we can and must fix.
Surrounded by family and friends my father-in-law peacefully passed away within minutes of removing the breathing tube. He was 66 years old. May his soul rest in eternal peace.
Take control over the end of your life: what you need to know about advance care directives.
Many agree on the factors contributing to a good death. People want to be treated with dignity, have relief from pain and, as much as possible, to control what happens to them.
Advance care planning is one way to exercise control. The process involves discussing and expressing preferences about the kind of care you would or would not want in a situation where you lack the mental capacity to make decisions.
As part of this process, you can write an advance care directive – a document that can be legally binding. It states your views and instructions about health care and other personal matters.
You can also appoint someone you trust to be you health care decision-maker. Despite its usefulness, only a small number of Australians (around 14%) currently have an advance care directive.
Why have a directive?
Studies show at least one-third of patients receive non-beneficial treatments at the end of their life, including tube-feeding and surgical procedures when there is little hope of the patient getting better. This is despite many older Australians saying they do not want medical interventions to keep them alive when their quality of life is poor.
With a good advance care directive in place, people are more likely to have their wishes for care respected. People with a directive are also more likely to experience fewer unwanted medical interventions, less likely to be moved from their home or community care to a hospital, and less likely to die in a hospital.
A directive means you can tell people your health care wishes so your choices can be legally respected.
If a patient who doesn’t have a directive is seriously ill and unable to communicate, doctors will consult with family or others close to the patient about their care. Family members and caregivers often experience stress and guilt when making decisions for a loved one at the end of their life. These decisions are made easier if they are guided by the values and preferences expressed in an advance care directive.
There are two kinds of directives: statutory and common law. A statutory directive means the person completes a document that meets specific government requirements – such as this one in South Australia or this one in Queensland. This week, the Victorian government introduced a bill to parliament to make advanced care directives legally enforceable.
New South Wales and Tasmania don’t have statutes that create forms for advance care directives, but people can make common law directives. This means they can state their health care wishes in their own way and they can be legally respected.
In 2009, the NSW Supreme Court ruled that a hospital had to follow the medical instructions a man had recorded in worksheets. The man was hospitalised with serious illness, lost consciousness and went into kidney failure. The court said the hospital had to respect the written instructions that refused blood transfusions and dialysis.
States that have statutory advance directives may also allow a person to make a common law directive. So it is not always necessary to use a government form. People interested in making an advance directive or appointing a health-care decision-maker should look up the rules in their state or territory; there are some good websites with accurate information.
What’s in a directive?
People often think of an advance care directive as a document that refuses consent to specific treatments. For example, you can specify you don’t want CPR or tube-feeding if you have a life-threatening medical problem with little chance of recovery.
This is true. But directives can also be used to document your values, say what quality of life means to you and specify if you have spiritual or lifestyle beliefs you want respected. For instance, you can write down things that would help create a home-like environment if you have to be cared for in a facility, such as music you would like to listen to or treasured items you would like in your room.
A person might complete an official statutory form to appoint someone as their health-care decision-maker, then attach a statement of values.
A statement of values, wishes and preferences can be helpful for appointed decision-makers and for care providers. Websites such as My Values can help you consider issues about medical care and dying you may not have thought about before.
What else do I need to know?
You are encouraged to review your advance care directive, and other legal documents, to make sure they are up-to-date and reflect your current wishes and instructions.
It is also vital to share your directive with your health-care providers, appointed decision-maker (if you have one), family members and other loved ones who may be called on to help make decisions. Doctors cannot follow a directive if they don’t know it exists.
There is no mandatory central registry in Australia to make sure doctors have access to directives when needed. But people with an electronic health record – known as My Health Record – can include their advance care directive information there.
Advance care planning is typically promoted in health-care settings. But some people are more likely to talk to a lawyer than a doctor about their health wishes. This often happens when a person seeks legal help on other aspects of future planning, such as writing a will or appointing a financial decision maker.
I have argued that legal and health professions can work together more effectively to help their clients plan for their future health care. Doing so promotes their clients’ interests and autonomy. It makes sure people’s values and wishes are known, even beyond a time when they can no longer speak for themselves.