Dementia strikes about one in 13 lesbian, gay or bisexual seniors in the United States, a new study finds.
“Current estimates suggest that more than 200,000 sexual minorities in the U.S. are living with dementia, but — before our study — almost nothing was known about the prevalence of dementia among people in this group who do not have HIV/AIDS-related dementia,” said Jason Flatt. He is an assistant professor at the University of California, San Francisco School of Nursing.
The study included more than 3,700 lesbian, gay and bisexual adults, aged 60 and older. Over an average follow-up period of nine years, the rate of dementia in this group was 7.4 percent. The dementia rate among Americans aged 65 and older is about 10 percent.
The study was to be presented Sunday at the Alzheimer’s Association annual meeting, in Chicago.
The findings “provide important initial insights,” Flatt said in an association news release.
But “future studies aimed at better understanding risk and risk factors for Alzheimer’s and other dementias in older sexual minorities are greatly needed,” he added.
High rates of depression, high blood pressure, stroke and heart disease among sexual minorities may contribute to their dementia risk, the researchers say.
“Encouraging people to access health care services and make healthy lifestyle changes can have a positive impact on both LGBT and non-LGBT communities,” said Sam Fazio, director of quality care and psychosocial research for the Alzheimer’s Association.
But effective outreach to LGBT groups must be sensitive to racial, ethnic and cultural differences, Fazio added. This could result in earlier diagnosis, which has been linked to better outcomes, he said.
Flatt added that the study points to important implications for meeting the long-term caregiving needs of the LGBT community.
“Given the concerns of social isolation and limited access to friend and family caregivers, there is a strong need to create a supportive health care environment and caregiving resources for sexual minority adults living with dementia,” Flatt said.
Research presented at meetings is usually considered preliminary until published in a peer-reviewed medical journal.
What happens when seniors who can’t recognize their own kids try to navigate the hazards of physical intimacy with one another? Zosia Bielski looks at the challenges for elderly people, nursing homes and families
Harriette Stretton, 80, and her 94-year-old sweetheart, Denis Underhill, embrace at Bloomington Cove Care Community in Stouffville, Ont. Their relationship came as a relief to their families, though staff would phone their children to let them know what was going on between the pair.
By Zosia Bielski
When Karen Best abruptly lost her communications job at the age of 57, her family found it strange: she’d been a workaholic all her life. For a while, they assumed she was depressed, as she whiled away the hours watching cat videos online in her housecoat.
Within the year, Ms. Best was diagnosed with early-onset Alzheimer’s and frontotemporal dementia. By the time her family placed her in long-term care in Welland, Ont., Ms. Best had stopped calling her grandchildren by their names and lost most of her language. Staff would ask if she wanted a blueberry or a chocolate-chip muffin; she couldn’t reply.
Which made the phone call from the nursing home one month into Ms. Best’s stay all the more alarming: caregivers were anxious about her and a male resident. Staff needed her daughter, Cassandra Trach, to come in right away. “She had been found with no pants on, and he had no pants on, in his room,” said Ms. Trach, a 33-year-old account executive in the Niagara region. “This was something I was wholly unprepared for.”
Cassandra Trach, right, and mother Karen Best take a stroll with Ms. Trach’s children by the Welland Pan Am Flatwater Centre in Welland, Ont.
Ms. Best and the elderly man would walk together, holding hands, and she would also seek him out for closer contact, according to staff. Like her, he was able-bodied but suffering from dementia. Ms. Best and her new companion were also both married – in Ms. Best’s case, for three decades – but had seemingly forgotten their spouses.
Every time nursing-home employees discovered the couple undressed together, they’d call Ms. Trach and her father, who jointly possess power of attorney for Ms. Best. “It felt like they wanted us to decide, do we let this relationship go and happen, or do we try to redirect?” Ms. Trach said. “It’s so grey. What do I do?”
For Ms. Trach, it was a painful predicament. Could her mother – an advanced dementia patient who sometimes couldn’t communicate what she wanted for breakfast – meaningfully consent to a new sexual relationship? Dementia had rendered most of her thoughts inscrutable, her desires opaque. Who could tell if she wanted or understood this?
Amid ever-widening cultural conversations about sexual consent, dementia remains uncharted territory. As Canadians live longer, more are moving into long-term care with advancing dementia disorders. It’s a growing population with complex needs, not least of all in their intimate lives.
In the close-quarters environment of nursing homes, these people’s sexuality poses difficult ethical dilemmas for staff and for families. Those who care for uniquely vulnerable dementia patients walk a fine tightrope. They have to protect their residents from sexual abuse while respecting their needs for human connection – and a private life.
This is proving challenging for Canadian caregivers. There is no unified strategy on sexuality and dementia in this country. No cognitive test exists to determine, once and for all, whether a person with Alzheimer’s can consent to sex or not.
Instead, nursing-home employees are often left on their own to decide whether their residents with dementia can consent to intimacy safely – even as residents’ awareness shifts from moment to moment, their speech recedes and their thoughts become difficult to access.
When poorly trained staffers are left to untangle such ethical knots, they can bring their own value judgments to bear. A prevailing squeamishness about elder sex can provoke alarmist reactions. The result is great inconsistency around dementia patients’ sexual lives in long-term care across Canada, a point that troubles Alzheimer’s advocates.
“It’s all over the map,” said Judith Wahl, a Toronto legal consultant who fielded complaints about homes for three decades as executive director of the Advocacy Centre for the Elderly and now educates long-term care staff across the country about consent and dementia.
In interviews, more than a dozen sources detailed questionable attitudes on the ground.
They described personal support workers seemingly making up policy on the fly, with some barring any kind of touch between residents, and others not paying close enough attention to their most defenceless patients and those who might exploit them.
“Homes should put their minds to looking at how they manage this,” Ms. Wahl said. “It’s really hard to do this well.”
Ms. Best takes a stroll with Ms. Trach and her two children. Ms. Best is still married, as was her male companion in their long-term care facility in Welland, but the two had seemingly forgotten their spouses and formed a relationship with each other.
Consent and capacity
Despite an ever-widening social reckoning around sexual consent, dementia presents a new frontier.
Just 28 per cent of Canadians fully understand what consent entails, according to research conducted earlier this year by The Canadian Women’s Foundation. Consent becomes decidedly more complicated when one or both people involved have dementia.
Just as a person’s sexual consent can quickly swing from “yes” to “no” during an intimate encounter, so can dementia patients’ abilities to recognize and navigate what’s happening around them.
“Consent is so challenging,” said Mary Schulz, director of education at the Alzheimer Society of Canada. “It’s a moving target. Our instruments for assessing that are quite blunt.”
The starting point is Canada’s sexual-consent law, which is no different for people living with dementia than it is for anybody else. The Criminal Code is clear: Consent can be spoken or unspoken, but it needs to be affirmative and happen in the moment; passivity cannot be construed as a “yes,” and nobody can consent (or dissent) on anyone else’s behalf, not even with power of attorney.
“With medical treatment, if you’re not competent, [the decision goes] to somebody else on the hierarchy – often a family member,” said Jane Meadus, a lawyer with the Advocacy Centre for the Elderly. “With sex, you can’t do that.”
Although the law is clear, it’s not always helpful within the context of nursing homes. Who determines “capacity to consent to sex” is not readily established in Canada. Often, it falls to personal-support workers to resolve the most critical questions: Do their residents with dementia understand what they’re doing, including the consequences? Can they pull back at any time?
With little consent training, staff aren’t always equipped to answer with full certainty.
Fine balance
Deepening the dilemma is the contradictory nature of the nursing home. These places are supposed to serve as patients’ homes, where they’d normally enjoy a private life. At the same time, these are highly monitored environments where every risk is mitigated. Caregivers have to prioritize safety and dignity simultaneously.
“They’re in a bind, because we’re not really good at telling them how to do that,” Ms. Meadus said.
At long-term care homes in most provinces, residents now have a “bill of rights” that allows them to receive visitors of their choice in private. Ontario and Prince Edward Island spell out residents’ rights to form relationships in care, even letting friendly residents share rooms. “Residents are treated with respect and dignity at all times, including during intimacy,” reads Nova Scotia’s patient bill of rights, the only document to use the word directly.
These philosophies represent a stark evolution from the oppressive old-age institutions of the past. But, even as residents’ rights are increasingly protected on paper, what happens on the ground doesn’t necessarily follow.
“It gets extremely tricky,” Ms. Meadus said. “You get some homes that have tried in the past to say, ‘Nobody can have sex, that’s it.’ And you get other homes where it’s laissez-faire: ‘As long as it feels good, they can do it.’ It is a very difficult balance that people are trying at, but we haven’t got it right yet.”
Advocates voiced concern about caregivers overstepping. They described religious staff members taking moral exception to LGBTQ patients and to residents having extramarital liaisons. They spoke of homes that have operated as “no sex zones,” where caregivers overzealous about their duty to protect patients have dissuaded them from engaging in all touch with one another, right down to holding hands. Staffers are afraid that such simple, comforting gestures might spiral into sexual abuse and liability.
They’ve got some cause for concern. Long-term care is one of the most highly regulated sectors in Canadian health care. Homes track everything and must report sexual abuse to their provincial ministries of health and long-term care, and to police. Ministries will cite homes if staff members fail to protect their residents from harm. Families of residents can also sue a home for damages; these cases are overwhelmingly settled out of court.
“The default position for long-term care staff – not necessarily rightly, but quite understandably – is in case of doubt, nobody touches, nobody hold hands, nobody is allowed to have sex,” said Ms. Schulz of the Alzheimer Society of Canada. “They go to that extreme position because they’re at a loss. But that is denying a person their human experience, which is just not on.”
On the other end of the spectrum, employees at more progressive homes don’t always consider the sexual risks as closely as they should, some legal advocates say. Ms. Wahl said she’s dealt with too many complaints about employees looking the other away, assuming the affection between two residents is mutual when it might not be. “Just because somebody’s old,” she said, “doesn’t mean that you just ignore the fact they could be sexually assaulted.”
Ms. Wahl rattles off what she’s seen. Some staffers will decide that a resident is seeking out sex because he or she walked into another resident’s room – this even as clinicians know that dementia patients often wander without aim. Other caregivers mistakenly assume that sex between a resident and visiting spouse is automatically consensual. This disregards Canada’s 1983 marital-rape law, which makes clear that even those married for decades need to get agreement from each other before having sex.
Ms. Wahl is most perturbed by family members infantilizing their elders. She said she’s seen many adult sons and daughters objecting to parents forming relationships in care. Sometimes, Ms. Wahl said, staffers hand over the sexual decision-making to these family members, assuming it’s the right thing to do because they have power of attorney.
“You can’t have substitute consent to sex,” Ms. Wahl cautioned, pointing to Canada’s sexual-assault laws.
Family ties
Adult children can be the strictest gatekeepers. Many will try to stymie their parents’ late-in-life
When Karen Best was found undressed in her room with her new boyfriend, staff told her daughter about it, which was an ‘unnerving’ experience, she says. ‘What am I supposed to do with this information?’
relationships, lawyers and Alzheimer’s advocates say.
Children are rightly protective, but many are also simply recoiling from their parents’ sex lives.
“Unnerving” was the word Ms. Trach used as she fielded call after call about her mother being found undressed again with her new boyfriend at the nursing home in Welland. “What am I supposed to do with this information?” Ms. Trach asked, exasperated.
Even though staff reported that her mother encouraged the intimate relations, Ms. Trach was distressed. She wondered about her mom’s motivations for pursuing the man.
“Is she consenting to it because, like a teenage girl, she’s seeking approval? … Is she doing this because she’s lonely?” Ms. Trach asked. “How can you tell with someone with dementia?”
She got few answers. Balancing her mother’s need for affection with her safety was “agonizing.” In the end, the family did not interfere with the relationship, although they asked that the pair be monitored as closely as possible by staff.
“If this is something that gives them joy and happiness,” Ms. Trach said, “maybe we have to put our own discomfort aside.”
Along with the other adult children of parents with dementia who spoke with The Globe and Mail, Ms. Trach decided to speak out on behalf of her mother, who is now largely non-verbal, to spread awareness about the sensitive issues of consent and connection in long-term care homes. Ms. Trach said she went public so that nursing homes “are awesome by the time we have to live in them.”
Ms. Best sits in the car on an excursion with Ms. Trach and her children. Her dementia has left her largely non-verbal.
Shedding stigma
Today, in old-age institutions and outside of them, deeply ageist aversion persists toward elderly adults and sex – never mind those beset by Alzheimer’s.
“It can seem kind of, almost obscene, in some people’s minds, to be thinking about sex when you’re talking about someone who’s perhaps cognitively impaired, elderly or physically frail,” Ms Schulz said. “And it can seem somehow irrelevant: ‘How can you even be thinking about this when we’re dealing with massive issues of cognitive decline?’”
The Alzheimer Society of Canada is in the midst of overhauling its resources for families and other caregivers on the issue of sexuality and dementia. It’s enlisted the help of Lori Schindel Martin, an outspoken associate professor at Ryerson University’s Daphne Cockwell School of Nursing.
At Canada’s first sexual-consent conference, held in 2016 at Trent University in Peterborough, Ont., Prof. Schindel Martin asked the next generation of nurses to consider what human touch means for residents’ well-being.
“Research tells us,” Prof. Schindel Martin told the audience, “that older people will have an increased quality of life, enhanced self-esteem and will heal from their depression because they connected with someone on a level that involves their skin.”
Prof. Schindel Martin took the opportunity to call out what she views as pervasive censorship of elderly people’s sexuality.
She laced her keynote with eye-opening composite cases from two decades spent on the front lines as a gerontology nurse working with dementia patients. There was the man who adorned his walls with framed Playboy centrefolds; nurses protested and refused to go into his room. Another woman would lift her skirt over her shoulders and proposition male residents, or “sailors” as she called them. And there was the husband who visited his wife every day from lunch till 7 p.m.; the housekeeper was shocked to walk in on him one day with his head between his wife’s legs.
They were visceral vignettes meant to illustrate the very real sexuality of older adults, as well as our profound unease around it. Speaking from her small, turquoise-blue office at Ryerson last April, Prof. Schindel Martin argued that ageism permeates everything about this issue: we see elderly people as asexual beings taking afternoon tea together, not pinning nude centrefolds to their walls.
The academic says we need a rethink. Pointing to nursing homes’ risk assessments, cognitive questionnaires and panicked phone calls to family, Prof. Schindel Martin wondered if anyone would ever subject randy first-year college students to any of this heavy-handedness.
“One’s humanity and capacity for relationships become examined very deeply in ways that we don’t do with other people,” Prof. Schindel Martin said. “What we’re able to control are older people … to remove them from each other and create rules.” (At Trent, she likened it to “killing a mosquito with a hammer.”)
Prof. Schindel Martin insisted that most of what she’s witnessed in clinical practice involved people seeking each other out for company, belonging and warmth. She wants stronger training so caregivers can better discern harmless courtship from more problematic sexual behaviour.
“We need to step back and rethink what could happen in our worst imaginings,” Prof. Schindel Martin said. “We don’t even have good prevalence incidence data about how often these things happen.”
Canada does not collect comprehensive data on sexual abuse perpetrated by residents against other residents in long-term care. A cross-country scan revealed many provinces lump together reports of all kinds of abuses – physical, verbal, financial and sexual. Most provinces also fail to differentiate between different types of abusers, counting exploitative residents, visitors and staff members all together. Provinces that did break out these statistics reported “founded investigations” and not all reports, meaning tallies appeared conspicuously low. (For example, between 2012 and 2017, Nova Scotia reported just 18 proven investigations of non-consensual sexual activity between residents in 135 long-term-care homes.)
What we do know is that Canada’s dementia population is swelling. The number of Canadians over 65 with dementia increased 83 per cent between 2002 and 2013, according to the Public Health Agency of Canada, which found that some 76,000 new cases are diagnosed every year in this country. Today, more than half a million Canadians are living with dementia, according to the Alzheimer Society of Canada. By 2031, that number will nearly double.
Denis Underhill’s room at Bloomington Cove is decorated with paintings made by his father.
Culture change
His sweetheart, Harriette Stretton, has a more sparsely decorated room. A birthday card reading ‘I love you!’ is taped to the wall.As baby boomers become caregivers to aging parents and round the corner into old age themselves, they want long-term-care options that actually feel like home, not the cold, controlled institutions of generations past. They want their rights recognized, including the freedom to enjoy intimate relationships in some semblance of privacy, the way you would at home.
Experts believe the way forward lies within a broader push for “person-centred” health care that focuses on knowing patients individually: if you don’t bother trying to know them or their needs, how can you help them? Person-centred care doesn’t solve all the difficult, sometimes inscrutable questions facing nursing-home staff about consent, capacity and dementia. It’s by no means a magic bullet, but experts believe it is, at the very least, a more empathetic approach that doesn’t stigmatize ailing, elderly people looking for human connection.
At Sherbrooke Community Centre, a long-term-care facility that houses 263 people in Saskatoon, chief executive Suellen Beatty said caregivers need to be “really good detectives,” who decipher the unmet needs of their residents – not who admonish them. Married residents trying to take up with others in the nursing home are often seeking love and attention, Ms. Beatty said. For them, help can take on many different forms: extra hugs from staff, more visits from a spouse or something tactile, such as pet therapy.
Ms. Beatty argued that caregivers should prioritize residents’ happiness instead of only seeing them as fragile. “We want to make this a risk-free world for people, and then we wonder why they disengage,” Ms. Beatty said. “We can make this so safe that we take all the joy out of life.”
Set amid woodlands and farmers’ fields in Stouffville, Ont., Bloomington Cove Care Community is another nursing home that bills itself as person-centred. Here, all of the 112 residents have dementia. Most are women in their 80s; there are just 28 men here.
Residents are encouraged to keep their familiar routines, waking up, showering and eating on their own clock. Bedrooms are private and filled with things from home – a favourite arm chair, ornately framed oil paintings, school portraits of grandchildren. Outside each room hang memory boxes, wood and glass curio cabinets filled with war memorabilia, weathered wedding photos and other treasures. Meant to stir recollection, the boxes also remind residents which room is theirs.
Many here are in the advanced stages of the disease. Some tire themselves out pacing, others hoard, Vitrines with memories from each resident, such as this one for Mr. Underhill, line the hallways of Bloomington Cove.hallucinate or grow depressed.
“It’s very hard to grow old,” said executive director Janet Iwaszczenko, walking the teal and beige halls.
For those suffering from frontotemporal dementia, the disease often impairs judgment and the ability to read context and social cues. People can become disinhibited around sex. Residents will occasionally mix up staff members for their spouses and require “redirecting.” Sometimes, residents will court each other. “There’s no filter,” Ms. Iwaszczenko explained. “There’s no understanding of social appropriateness.”
Things get especially tricky when residents who are married pair off with their nursing-home neighbours. These extramarital relationships often catch families off guard. Nurses and social workers observe residents, talk to them and to their spouses and relatives, documenting everything on residents’ charts.
“[Families] have a lot of upsets going through this horrible disease with someone they love,” Ms. Iwaszczenko said. “We talk about it. That’s the most important thing.”
Mr. Underhill and Ms. Stretton, both widowed, have been inseparable at Bloomington Cove for the past three years.
Sweeties
On a sunny morning in April, staff gathered for a “risk huddle” in a glassed-in office looking out into a communal dining room. Registered practical nurse Mun Lee went over the pressing issues of the day: patients adjusting to new medication, protocols for changing bed linens and good hygiene practice (“long toenails must be trimmed,” Ms. Lee instructed).
An elderly man sailed past the windows, blowing kisses to staff through the glass. It was Denis Underhill, a sociable, 94-year-old Second World War veteran. Talk at the meeting turned to Mr. Underhill and another resident, 80-year-old Harriette Stretton. Both widowed, the two had been inseparable for three years. “They’re very in tune with each other,” Ms. Iwaszczenko said.
They’d share meals, walk the halls and sing old songs such as Easter Parade to each other. He’d talk about wanting to marry her, often. There were frequent hugs, kisses and naps. Ms. Lee raised the pair’s nap time at the staff huddle. “Close the door,” she said. “Give them privacy.”
Ms. Stretton and Mr. Underhill’s relationship came as a relief to their families.
“There seems to be an underlying sense of comfort that he knows he is not alone,” Mr. Underhill’s daughter, Nancy Beard, said.
Staff would phone Ms. Beard and Ms. Stretton’s daughter, Theresa Elvins – who have power of attorney – to let them know what was going on between the pair.
“There were a couple of instances where I’d get a call: ‘We found your mom and Denis in bed together.’ And I’m like, ‘Oh my god,’” Ms. Elvins recalled (Ms. Beard refers to it as “canoodling”).
Mr. Underhill’s health declined in the winter and Ms. Stretton’s recognition has grown spottier. “You can tell there’s a glimmer,” Ms. Elvins said. “She knows she should know us and that we’re familiar, but she couldn’t tell you that I’m her daughter.”
Asked if her mother was aware in her romantic relationship, Ms. Elvins was certain. “I knew that she had feelings for him,” she said. “I knew she was communicating what she felt, and not what she thought someone told her to feel.”
Today, the two infatuated elders remain together, although it’s never been clear whether they know each other’s names: they call each other “sweetie,” Ms. Elvins said.
“Even though they might not remember who you are, they still have feelings and needs just like anyone else.”
Ms. Stretton and Mr. Underhill share a moment in his room, where Ms. Stretton’s daugther, Theresa Elvins, says she often finds her mother when she came to visit. The two sometimes take naps together.
Angela and Pete had the perfect marriage but it all ended when he tragically died at the age of 34. Angela was overwhelmed with grief when her late husband’s best friend stepped up to play a major role in her life.
I was married to Pete for only two years and I was madly in love with him. We’d only been dating for three months when we got engaged, it was a whirlwind romance of the most romantic kind, better than anything I could imagine. He was the kindest, sweetest man and everybody adored him.
Then tragedy struck and he was involved in a motorbike accident and killed instantly. I was at work when I heard the news and to this day, I still can’t believe he has gone. My life fell apart all around me. When I say everyone was devastated, I’m not exaggerating; friends, family, workmates, casual acquaintances, there was an outpouring of grief.
But I believe nobody was more impacted than me. For a long time I struggled to get out of bed, I couldn’t eat, couldn’t sleep, my grief took over my life. The only person who really stuck by me in terms of helping me get over the initial first stages of grief was his best friend, Andrew, who became my rock.
He was also grieving the loss of Pete but he would come over first thing in the morning, make sure I got up and had breakfast, he helped me and his family prepare for the funeral, and after the funeral when so many people went back to their own lives and I was pretty much forgotten, Andrew was by my side at all times.
So it was no great surprise that after leaning on each other so heavily in those painful months after Pete’s death that Andrew and I got closer and closer, eventually falling in love. We waited for a year before we let everybody know that we were now a couple and perhaps that was too soon because I was shocked at the reaction of people that I thought were friends.
Most of all I was shocked by the reaction of Pete’s family who were horrified that Andrew and I were together. Only Pete’s sister was accepting of us, she said she was pleased to see us both smiling again and that we both deserve happiness after having Pete ripped out of our lives in such a shocking way. Pete’s parents and his brother were a different story, his mum said she was ashamed of me, that Andrew and I must have been having an affair which was not true at all.
Pete’s parents made my life very difficult and because I inherited the house we’d bought shortly after we married, they objected to me living there with Andrew, which was pretty ludicrous.
Looking back, I realise they were still grieving and I became the target of their anger. But it was really upsetting that they didn’t see that what had happened in the aftermath of Pete’s death was some kind of miracle, that two people that Pete had loved, found happiness together. We’re now expecting a baby and I’m determined to reach out to my former in-laws and hope they will give this baby their blessing and instead of feeling all this anger towards me, that they finally have compassion for me.
She encouraged her husband to find new love after she was gone. A year later, he reflects on what her generosity has meant to him.
By Jason B. Rosenthal
I am that guy.
A little over a year ago, my wife, Amy Krouse Rosenthal, published a Modern Love essay called “You May Want to Marry My Husband.” At 51, Amy was dying from ovarian cancer. She wrote her essay in the form of a personal ad. It was more like a love letter to me.
Those words would be the final ones Amy published. She died 10 days later.
Amy couldn’t have known that her essay would afford me an opportunity to fill this same column with words of my own for Father’s Day, telling you what has happened since. I don’t pretend to have Amy’s extraordinary gift with words and wordplay, but here goes.
During our life together, Amy was a prolific writer, publishing children’s books, memoirs and articles. Knowing she had only a short time to live, she wanted to finish one last project. We were engaged then in home hospice, a seemingly beautiful way to deal with the end of life, where you care for your loved one in familiar surroundings, away from the hospital with its beeping machines and frequent disruptions.
I was posted up at the dining room table overlooking our living room, where Amy had established her workstation. From her spot on the couch, she worked away between micro-naps.
These brief moments of peace were induced by the morphine needed to control her symptoms. A tumor had created a complete bowel obstruction, making it impossible for her to eat solid food. She would flutter away on the keyboard, doze for a bit, then awake and repeat.
When Amy finished her essay, she gave it to me to read, as she had done with all of her writing. But this time was different. In her memoirs she had written about the children and me, but not like this. How was she able to combine such feelings of unbearable sadness, ironic humor and total honesty?
When the essay was published, Amy was too sick to appreciate it. As the international reaction became overwhelming, I was torn up thinking how she was missing the profound impact her words were having. The reach of Amy’s article — and of her greater body of work — was so much deeper and richer than I knew.
Letters poured in from around the world. They included notes of admiration, medical advice, commiseration and offers from women to meet me. I was too consumed with grief during Amy’s final days to engage with the responses. It was strange having any attention directed at me right then, but the outpouring did make me appreciate the significance of her work.
When people ask me to describe myself, I always start with “dad,” yet I spent a great deal of my adult life being known as “Amy’s husband.” People knew of Amy and her writing, while I had lived in relative anonymity. I had no social media presence and my profession, a lawyer, did not cast me into public view.
After Amy died, I faced countless decisions in my new role as a single father. As in any marriage or union of two people with children, we had a natural division of labor. Not anymore. People often assumed Amy was disorganized because she had list upon list: scattered Post-it notes, scraps of paper and even messages scrawled on her hand. But she was one of the most organized people I have ever met.
There are aspects of everyday life I have taken on that I never gave much consideration to in the past. How did Amy hold everything together so seamlessly? I am capable of doing many things on my own, but two people can accomplish so much more together and also support each other through life’s ups and downs.
Many women took Amy up on her offer, sending me a range of messages — overly forward, funny, wise, moving, sincere. In a six-page handwritten letter, one woman marketed her automotive knowledge, apparently in an effort to woo me: “I do know how to check the radiator in the vehicle to see if it may need a tad of water before the engine blows up.”
While I do not know much about reality TV, there was also this touching letter submitted by the child of a single mother, who wrote: “I’d like to submit an application for my mom, like friends and family can do for participants on ‘The Bachelor.’”
And I appreciated the sentiment and style of the woman who wrote this: “I have this image of queues of hopeful women at the Green Mill Jazz Club on Thursday nights. Single mothers, elegant divorcées, spinster aunts, bored housewives, daughters, wilting violets … all in anxious anticipation as to whether the shoe will fit, fit them alone, that the prince from the fairy tale is meant for them. That they are the right person.”
I couldn’t digest any of these messages at the time, but I have since found solace and even laughter in many of them. One thing I have come to understand, though, is what a gift Amy gave me by emphasizing that I had a long life to fill with joy, happiness and love. Her edict to fill my own empty space with a new story has given me permission to make the most out of my remaining time on this planet.
If I can convey a message I have learned from this bestowal, it would be this: Talk with your mate, your children and other loved ones about what you want for them when you are gone. By doing this, you give them liberty to live a full life and eventually find meaning again. There will be so much pain, and they will think of you daily. But they will carry on and make a new future, knowing you gave them permission and even encouragement to do so.
I want more time with Amy. I want more time picnicking and listening to music at Millennium Park. I want more Shabbat dinners with the five of us Rosies (as we Rosenthals are referred to by our family).
I would even gladly put up with Amy taking as much time as she wants to say goodbye to everyone at our family gatherings, as she always used to do, even after we had been there for hours, had a long drive home ahead of us and likely would see them again in a few days.
I wish I had more of all of those things, just as Amy had wished for more. But more wasn’t going to happen for her or us. Instead, as she described, we followed Plan “Be,” which was about being present in our lives because time was running short. So we did our best to live in the moment until we had no more moments left.
The cruelest irony of my life is that it took me losing my best friend, my wife of 26 years and the mother of my three children, to truly appreciate each and every day. I know that sounds like a cliché, and it is, but it’s true.
Amy continues to open doors for me, to affect my choices, to send me off into the world to make the most of it. Recently I gave a TED Talk on the end of life and my grieving process that I hope will help others — not something I ever pictured myself doing, but I’m grateful for the chance to connect with people in a similar position. And of course I am writing to you now only because of her.
I am now aware, in a way I wish I never had to learn, that loss is loss is loss, whether it’s a divorce, losing a job, having a beloved pet die or enduring the death of a family member. In that respect, I am no different. But my wife gave me a gift at the end of her column when she left me that empty space, one I would like to offer you. A blank space to fill. The freedom and permission to write your own story.
Here is your empty space. What will you do with your own fresh start?
[T]he death of a spouse or partner can be one of the most devastating events in a person’s life bringing with it it’s own particular difficulties. As a result of this death you may have lost your life’s partner, lover, confidante, father or mother of your children, breadwinner, home-maker and possibly your best friend. You may be forced to make more changes than from any other event you will ever experience.
Even if you maintained a great deal of personal independence within your relationship you can be surprised and frightened to discover just how ‘dependent’ you have been on your partner. Over the years you may have related closely to one another’s fears and joys so that when one dies you feel incomplete. Your life has lost its structure and its purpose. You may be left with many unfulfilled needs – emotional, physical, practical, intellectual and social. It is hard to imagine all the areas of life your spouse once filled until you experience the gaps.
Grieving, in itself, is emotionally and physically exhausting. When you have the additional burden of taking on the roles that were previously performed by your partner, going on living may appear to be just too much. New tasks should be embarked on slowly with as much help as is available. Major decisions should not be taken when vision is clouded by anxiety and panic.
Friends may avoid social contact with you because of embarrassment. You are now a single person. Some may see you as a threat to their relationships. You may feel isolated, no longer part of a group, not invited out, or you may exclude yourself as you feel uncomfortable without your partner. Many surviving partners experience the unwanted sexual advances from those whom they counted among their or their partner’s friends.
The feeling of loneliness can be overwhelming and will probably come to you at your most vulnerable times – at night, weekends and holidays. Plan for this – at night keep the radio on, change your routine. Plan a project or outing for a weekend or holiday. Make contact with another lonely person.
Financial difficulties may arise – especially if your spouse or partner died without making a will. You may not be aware of your financial state and even if matters are in order there is often a delay in getting things sorted out. If there is a reduction in income the effect on your standard of living may cause family problems especially when children’s expectations also have to be adjusted. This can add to feelings of fear, anxiety and anger. Your local Citizens Information Centre may be of help with practical matters.
Sexual loss. The loss of love making which included touch, warmth and sharing a bed with your partner can be very painful. It can be tempting to succumb to sexual advances from another. However, such action based on acute need and deep grief is potentially hazardous. Until you have let go of the past, it is better not to make a commitment to someone new.
If your partner dies in the early years of the marriage / relationship not only do you grieve the loss of a beloved person but also the loss of a new, exciting romantic relationship with the prospect of years of mutual love and companionship. You may also grieve the hope of parenting a child or more children together. You may feel that you are the only one of your generation who has been cheated out of hopes for the future. Young widows and widowers may also be expected to comfort the parents of the dead partner.
If the death occurs in your mid-life years you may have the additional stress of feeling trapped by the total responsibility for all the many needs of teenage children which can also prevent you from expressing your own grief. The agency ‘Parentline’ can be helpful in assisting with parenting problems. At this time you may also feel a loss of identity especially if you have no interests or work outside the home.
For the elderly bereaved – the loss of a life’s partner can cause increased trauma, create health problems and may affect your will to live. Sometimes, with the best of intentions, adult children may smother the surviving parent with care and attention. They do not allow you space to grieve or to make your own decisions. If your family are far away you can feel all alone and may even feel abandoned.
For those in same sex relationships there may be added difficulties. The relationship may have been ignored or denied by the family of one or both partners. This can create added stress for you in the grieving process. As the surviving partner, you may find yourself excluded from decision-making concerning the funeral and burial. You may even be precluded from attending.
Perhaps work colleagues and the wider community may just think that a ‘friend’ has died, but you have lost your life partner and companion and you have to keep your grief hidden. This intensifies all aspects of the grieving process, leading to strong feelings of loneliness, isolation, anger and, at times, frustration. If the death has been from Aids, this can lead to further social isolation. It is important that you can find someone to whom you can unburden your feelings.
Whatever your age when you are bereaved, your feeling and reactions will be influenced by the nature and duration of the relationship. If the relationship had been ambivalent, feelings of relief, regret and guilt can be confusing. It is important, when dealing with these feelings, to be totally honest with yourself. Put words on your feelings, voice them aloud or write them down. It is always helpful to talk about your feelings with someone who will listen in a caring and confidential way. This will help you to discover what you are feeling, why you are feeling like this and what you can do about it. Joining a support group for bereaved people may be helpful.
The Bereavement Counselling Service is there to listen and provide support as you struggle with your grief. In our modern world just surviving can be hard work. It is doubly hard to pull yourself out of an emotional trough but it is not impossible. Each time you cope with a crisis and make a major decision you will feel good about yourself. When you reach a goal you will gain satisfaction and self-assurance through your own competence. With time and effort you will recover to lead a full and rewarding life once again.
[I]t’s never easy meeting your boyfriend’s exes, but it’s even harder when it’s at your partner’s funeral. So it was that I first met Donal, the love of Simon’s life. Handsome and charming, eloquent in his grief, I hated him before I even gave myself the chance to know him. While we got on fine at the wake, I had every intention of that being the only time we ever spoke.
This was made a lot harder by my decision to run the London marathon in our Simon’s name. As soon as the torrent of sweaty finish line selfies hit Facebook, Donal knew exactly why I had just run 26.2 miles, even though I’d done everything in my power not to bring his attention to what I was doing. It was about my pain, not anyone else’s.
“I wish we could have been better friends,” Donal messaged me.
“Well, we’re not the ones who are dead yet mate,” I wrote back. “So let’s Skype?”
We agreed to talk a few days later. Donal was immediately the most charming man I’d ever met. He was pleasant, complimentary, truthful, funny, and open about the fact he had felt just as alienated at Simon’s funeral as I had.
“What do you miss most about him?” he asked.
“His eyes,” I said. Donal nodded and smiled.
“I miss that ass, frankly.”
He paused, and then told me that I was the only other person who truly understood how he felt about Simon. I felt the same way: to speak to the only other person who had slept next to Simon was, perhaps, the most liberating thing in the world. Like the first time you make a Sean Cody joke with a new gay friend and realize that, for once, you’re speaking to someone who gets your shorthand.
We were both incredibly similar people—and both equally unaware of the chemsex and meth epidemic in London before meeting Simon—and both of us were trying to respond to his loss proactively. I wrote a play, he was making a film. He was helping support people he met who were in recovery, and I’d just run across half of London for Stonewall.
As we sat there, talking about our experiences with the same man, he started to cry as he told me that he wished he’d fought more for Simon to move out with him and get help in California, where the community was a lot better than it was in London.
This was not the first time Donal had told me this. At the wake, I had seen this as the most selfish opinion in the world: Didn’t I have a right to have met Simon too? This time round, less salty than I was when recently bereaved, I told him to stop being a fucking hero. Neither of us could have saved him, and we’d be arrogant to think otherwise. He smiled and told me he understood exactly why Simon fell for me.
We pledged to speak more, and we do. When Donal was back in England recently, we even popped into the bar where Simon and me—and Donal and me—had first met. Donal introduced me to the manager behind the counter, a man who I had bought pints from many times, knowing that we both had the same loss in our hearts, but had never spoken to.
“You won’t believe it,” said Donal, “but David here ran the marathon for Simon.”
The manager turned to look at me. He shook my hand. All three of us were choked up.
“Well then you’re not paying for those drinks,” he said.
Fran Leibowitz said in “The Impact of AIDS on the Artistic Community” that the crisis killed off the greatest audience for art New York had ever seen. For me, it also seems to have decimated a generation of mentors. Not just because of the body count, of course, but because of ageism in the gay community, a lack of social spaces that aren’t for clubbing, and because I’m sure we, as a generation younger, can seem uncomfortably ignorant of the defining moments of the gay liberation movement in the 20th century. Before Donal I had met nobody who could say certainly that what I was experiencing was not entirely new, and could confidently tell me when what I was feeling was important or when I was being a fucking idiot.
And this is as true for bereavement as it is for homosexuality. Both can feel incredibly isolating: many experience it, but it’s almost like everyone is speaking a different language when they try and share their stories. What Donal and I give each other as Simon’s partners is also what I was desperately in need of as a gay man: A confidante. Much-needed perspective. And an understanding that we are all part of something tough and beautiful together. And, I hope, I will give somebody else that when I’m older.
That is a question that a great many cancer patients would love to hear from their oncologists, but unfortunately, sexuality is not a topic that gets much attention.
A panel of experts here at the Palliative Care in Oncology Symposium (PCOS) 2017 tackled the subject of sex and the cancer patient and presented preliminary data demonstrating how “low-tech” interventions can make a dramatic difference for patients.
Sexuality is a somewhat taboo topic in oncology care, and perhaps even moreso in palliative care, explained panel member Anne Katz, PhD, RN, certified sexuality counselor at Cancer Care Manitoba, Canada. “But we know that this is important to patients and their partners across the cancer journey.”
She cited a study (Psychooncology. 2011;21:594-601) that found that fewer than half (45%) of all cancer patients had a conversation with their healthcare provider about sex. By cancer type, 21% of lung cancer patients had such a conversation, as did 33% of breast cancer patients, 41% of colorectal cancer patients, and 80% of prostate cancer patients.
Men, it seems, get the “sex talk” a lot more frequently than women do.
According to Dr Katz, the “whole thing is skewed” by prostate cancer. More than twice as many men speak to their providers about sex as compared to women.
“If we didn’t talk about nausea, if we didn’t talk about constipation, we would be regarded as negligent, even indulging in malpractice,” Dr Katz pointed out. “Yet we are leaving out conversations about this very important quality-of-life issue, which persists into end-of-life care.
“Sexuality is much more than just intercourse. It is about touch and intimacy and about much more than what we do in the bedroom,” she said.
A recent study (J Cancer Surviv. 2017 Apr;11:175-188) again showed that a “preponderance” of men (60%) had a discussion about sex with their provider, whereas fewer than half as many women did (28%).
However, healthcare providers thought “they were doing a good job,” with almost 90% reporting that they were. “So there is a very large gap as to who is saying what and who is hearing what,” explained Dr Katz.
Another problem is that the cancer patient is much more likely to raise the topic with their provider, rather than the reverse. This is a problem, she pointed out, “because in every other area, we raise the topic with our patients, indicating that its important. By not opening the door, by not starting the conversation, we are saying to our patients that ‘this is not important and I don’t want to talk about it.’ ”
Panelist Sharon Bober, PhD, founder and director of the Sexual Health Program at the Dana-Farber Cancer Institute in Boston, Massachusetts, agreed with that summation. “We have to expand our perspective on what sexuality is, in the context of serious illness and palliative care. It’s too easy to be reductionist and think about whether some can or cannot have sex – this isn’t what it’s about.”
Sexuality, she noted, is a human experience across the lifespan. It’s a multidimensional experience that involves physiology, behavior, emotion, cognition, and identity.
“What we can take from some of the qualitative and survey work that’s been done to date is that expressions of sexuality can be a vital aspect of providing comfort and relieving suffering, maintaining connections in the face of life-limiting illness, and affirming a sense of self when other roles are lost,” Dr Bober explained. “When sexually is not made part of care, there is an implicit message that is it no longer important and/or the challenges cannot be addressed.”
Unfortunately, providers often took a medicalized approach, as was evidenced in one study (Contemp Nurse. 2007 Dec;27:49-60). Patient sexuality and intimacy were largely medicalized; the discussion remained at the level of patient fertility, contraception, and erectile or menopausal status, Dr Katz noted.
“There is a lot of active avoidance,” she said. She pointed out that the “patient reports the topic and the oncologist takes three steps back and flies out the door.”
Some of the reasons given for not discussing sexuality were reactions of colleagues, fear of litigation, and fear of misinterpretation.
The topic needs to be brought up in the context of quality of life, she emphasized, “but we need to open the door.”
There is the fear of not knowing what to say, but there is “Dr Google, there are books, there are experts, and if you don’t know, you will find the resources to refer patients to them,” Dr Katz said. “We have a responsibility to discuss sexual side effects of cancer treatment.”
Very Brief but Very Effective
Sexual function is profoundly disrupted by gynecologic cancer treatment, and 90% of patients with ovarian cancer report distressing changes in sexual function. “The good news is that ovarian cancer patients are living longer, and almost 50% of survivors will live many years post diagnosis,” explained Dr Bober. “But they often have to endure multiple surgeries and multiple rounds of chemotherapy, and sexuality and distress are generally not addressed.”
She pointed out that with ovarian cancer patients, “no one talks about this. The thought Is often that you have bigger fish to fry, you may not live anyway ― there are all kinds of reasons that this doesn’t get addressed.”
Dr Bober described an intervention that they devised at Dana Faber to address sexual dysfunction in ovarian cancer survivors. Not only was it brief, easily accessible, and “doable” by patients, but final results showed that it was quite effective.
The format was integrative. It was composed of a single half-day group intervention with a didactic teaching and experiential exercises, coupled with an individualized action plan. After the session was completed, the participants were asked to reflect on what was pertinent to them and what they were going to work on during the next 6 weeks.
The session was followed by a brief telephone call, in which the action plan was reviewed and additional support was offered if needed, to uncover additional challenges that needed to be addressed.
Because this was a pilot study, it did not include a control group per se, Dr Bober explained, but participants served as their own controls. This was accomplished by having a 2-month run-in period, during which women filled out surveys at baseline then waited for 2 months before completing the survey a second time before beginning the intervention. The purpose of the 2-month run-in period was to estimate changes in symptoms that could not be attributed to the intervention.
The design comprised three modules. Module 1 was targeted on sexual health education, which discussed vaginal health, enhancing arousal, and increasing low desire. Module 2 involved body awareness and relaxation training, in which participants learned pelvic floor education, progressive muscle relaxation, and body scan. Module 3 involved a mindfulness-based cognitive training, which sought to increase nonjudging awareness of automatic thoughts, with progression from avoidance/distraction to acceptance.
The cohort included 46 women with stage I-IV ovarian cancer who reported at least one distressing sexual symptom. The mean time since diagnosis was 6.3 years (range, 1 – 20 years). “Twenty years is a very long time to be dealing with distressing sexual problems,” emphasized Dr Bober.
Within this group, 13% were currently receiving chemotherapy, and 44% were currently taking medication for anxiety, depression, or pain.
In evaluating the program, 97% of the women found the it helpful, 100% found it easy to understand, and 95% found the it enjoyable.
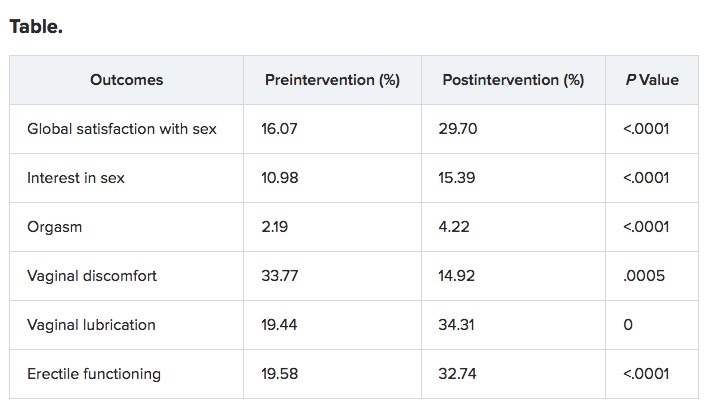
With regard to helping sexual functioning, “There were no changes during the run-in period, for the most part, demonstrating that time alone did not change the situation,” said Dr Bober. “But at month 2 after the interactions, there was significant improvement over multiple domains of sexual function. And for the most part it held over to 6 months.”
Although the pilot study was not focused on mental health per se, there was significantly less psychological distress observed in the participants, especially regarding symptoms of depression and distress.
It was a small pilot study, she emphasized, but the implications are that brief sexual health rehabilitation in the context of serious illness is effective. “There was meaningful improvement in sexual function and emotional distress, and improvements at 6 months.”
Dr Bober emphasized that there is an enormous need for evidence-based intervention research, with interventions conducted outside of an academic center in order to reach more people. “There is a need for identify optimal methods for delivery,” she said. “In some of the palliative care literature, patients talk about struggling with this issue within 2 to 3 months before they die, so this is not something that is relevant only if you’re well.”
Pilot Study in Transplant Patients
Similar to other oncology settings, sexual dysfunction is a common long-term complication for survivors of allogeneic hematopoietic stem cell transplant (HCT), but it is rarely discussed, and interventions to enhance sexual function in this population are lacking.
The preliminary efficacy of a multimodal intervention designed to improve sexual function in allogeneic HCT survivors was very encouraging, reported Areej El-Jawahri, MD, instructor of medicine at Harvard Medical School and director of the Bone Marrow Transplant Survivorship Program at the Massachusetts General Hospital, Boston.
Dr El-Jawahri and her colleagues conducted a pilot study to assess the feasibility and preliminary efficacy of the intervention in a cohort of 50 patients. The participants were at least 3 months’ post transplant and had screened positive for distress caused by sexual dysfunction.
“There was a very wide age range, from 24 years to 75 years,” she said. “The median time from HCT at enrollment was 29 months, but there was also a wide range between 3 and 173 months.”
The primary endpoint of the study was feasibility: 75% of patients who screened positive would agree to participate and attend the first visit, and at least 80% would attend at least two intervention visits.
The majority of patients had acute leukemia (55%), and nearly 64% had chronic graft vs host disease (GVHD).
The format consisted of monthly intervention visits with trained study clinicians. The visits focused on assessing sexual dysfunction, educating and empowering patients to address this topic, and implementing therapeutic interventions that targeted their specific needs.
The PROMIS Sexual Function and Satisfaction Measure, Functional Assessment of Cancer Therapy-Bone Marrow Transplant (FACT-BMT), and Hospital Anxiety and Depression Scale (HADS) were used to assess sexual function, quality of life (QOL), and mood at baseline and 6 months post intervention.
The study met its primary endpoint of feasibility; 94% (47/50) agreed to participate, and 100% of this group attended at least two interventions. The median number of visits were two (range, two to five). The median duration of the first visit was 50 min; for the second visit, it was 30 min. In addition, 28% (13/47) had a partner attend an intervention visit.
Results were encouraging, Dr El-Jawahri pointed out. “Sexual activity in the group increased.”
Before the intervention, 32.6% of patients reported not engaging in any sexual activity; that number declined to 6.5% after the intervention.
In men, the following therapies were implemented: phosphodiesterase inhibitors (PDI) on demand (57%), psychoeducation (52%), penile constriction rings (48%), referral to a sexual health clinic (9%), daily PDI treatment (4%), topical GVHD treatment (4%), and hormone replacement therapy (4%).
For women, therapies included vaginal estrogen (67%), dilator (63%), lubricant (58%), psychoeducation (42%), topical GVHD treatment (42%), topical lidocaine (8%), and referral to a sexual health clinic (4%).
“All outcomes were clinically and statistically significant,” said Dr El-Jawahri.
The program was efficacious in improving QOL and mood.
“This has very promising efficacy, but we need to conduct a randomized clinical trial, and there is a need to asses longer-term outcomes,” Dr El-Jawahri concluded. “It also has potential for adaptation to other types of cancer survivors as clinicians to deliver this kind of intervention and allow for dissemination.”


 The study was to be presented Sunday at the Alzheimer’s Association annual meeting, in Chicago.
The study was to be presented Sunday at the Alzheimer’s Association annual meeting, in Chicago.