Gerda Saunders, an author and former gender studies professor in Salt Lake City, Utah, was diagnosed with microvascular dementia in 2010 at age 60.
The time leading up to diagnosis and immediately after can be a whirlwind of emotions and confusion. But one thing, said Saunders, helped put her at ease: putting a plan in place for end-of-life care.
Saunders has chosen to pursue physician-assisted death when the time comes. “Preparation for the uncertain future is the most calming thing I’ve ever done,” she recently told Being Patient in an interview.
Saunders’ approach to end-of-life care is becoming more popular and accepted amongst people with a high risk of Alzheimer’s, a new study published in JAMA Neurology found. While we still can’t predict who will get dementia, there are several biomarkers that indicate a heightened risk for the disease. Researchers at the University of Pennsylvania interviewed people with one of these biomarkers, beta-amyloid, about their attitudes toward physician-assisted death once they knew their brains contained higher levels of the protein, which forms into plaques that destroy neurons in the brains of Alzheimer’s patients.
Of the 47 people interviewed, one in five said they would be interested in pursuing physician-assisted suicide if they were diagnosed with dementia and it progressed to the point of suffering or burdening others.
Physician-assisted suicide is legal in eight places in the U.S.—California, Colorado, Hawaii, Vermont, Washington, New Jersey, Montana and Washington, D.C.—but excludes dementia patients because states require the patient be of sound mind and have less than six months to live. Because the last stages of dementia can stretch out for much longer than six months, people with Alzheimer’s and other dementias do not qualify for “death with dignity” laws.
Most Americans support “death with dignity” laws, according to a 2018 Gallup poll that found 72 percent of people agreed that doctors should be able to assist a patient with a terminal illness in dying at their request. But the laws have always excluded patients with degenerative brain diseases who are deemed unable to make decisions for themselves.
Dementia patients can put advance directives into place, instructing hospital staff not to put extreme measures like feeding tubes into place. But those measures are not legally or ethically binding for medical staff.
Once she meets a set of criteria she has set for herself to determine quality of life, said Saunders, she will likely travel to Europe for physician-assisted death. She plans to carry it out herself and video it in order to avoid putting her husband, Peter, in legal jeopardy.
“We are managing it with all the intellect that we have and that is the best our family can do,” said Saunders, who has the support of her children and also promised to do the same for her husband if he meets certain criteria for quality of life before she does.
“I’ve put down a number of checkpoints: Do I appear or act happy for more hours in the day than I appear or act unhappy? Am I scared of people or my grandchildren or do I scare them? Do I consume more hours of care per day than I live on my own?”
It’s not always easy for family members to come around to the idea of a physician-assisted death—but for a patient who feels control has been snatched away, it can be a comfort. “It’s the hardest thing in his life to promise me that,” said Saunders of her husband’s commitment, “but he also asks it of me. My children and my family have given me an enormous gift in that promise.”
Anne Brescia sits in the room of her only child, Anthony Gabriel Brescia-Connell, who died of cancer in 2011. The hospital sent him home so he could die there with his family.
By Melissa Bailey
Anne Brescia sat beside her only child, Anthony, as he lay unconscious in a hospital bed at age 16. Just a few months before, he was competing in a swim meet; now cancer was destroying his brain. Brescia couldn’t save her son. But she was determined to bring him home.
Anthony Gabriel Brescia-Connell was not conscious for his voyage from Boston Children’s Hospital to his home in Medford, Mass., where he died on March 3, 2011, surrounded by his family and beloved stuffed animals. He may not have heard the parting blessings before a doctor turned off his portable ventilator and let him die naturally.
But having the choice to take Anthony home, away from the beeping hospital monitors, “meant the world to me,” his mother said.
Anthony’s journey was made possible through swift and unconventional efforts by the hospital staff, including a critical care transport team accustomed to rushing kids to the hospital to save their lives, not taking them home to die.
The experience galvanized Harriett Nelson, a nurse on that team who helped arrange the trip. It inspired her to conduct pioneering research on and advocate for “pediatric palliative transport” — a rare but growing practice that aims to give families choice, control and comfort at the end of life.
Palliative transport lets families move critically ill children from the hospital intensive care unit to their home or hospice, with the expectation they will die within minutes to days after removing life support.
It means “having parents go through the hardest thing they’ll ever know — in the way they want to do it,” Nelson said. Boston Children’s has sent 19 children to home or hospice through palliative transport since 2007, she said.
These final journeys — also offered by the Mayo Clinic, Children’s Hospital of Philadelphia and Kentucky Children’s Hospital — can involve elaborate planning, delicate transfers and even long helicopter rides. In some cases, families took a child far from home for a last-ditch effort to save their lives.
At the Mayo Clinic, palliative transport has helped culturally diverse families carry out end-of-life wishes for their dying children. In one case, a newborn girl rode 400 miles by ambulance to return to her Amish community, where she was extubated and died in her parents’ arms, in the company of her 11 siblings. In another, an 8-month-old Native American girl traveled 600 miles by air and ground ambulance to her rural tribal reservation, where she could participate in end-of-life rituals that could not be done in the hospital.
These trips, which can cost thousands of dollars, are typically offered free to families, paid for by hospitals or charities. Most children are taken home, where they transition to receiving care from hospice staff. Some go instead to hospice facilities.
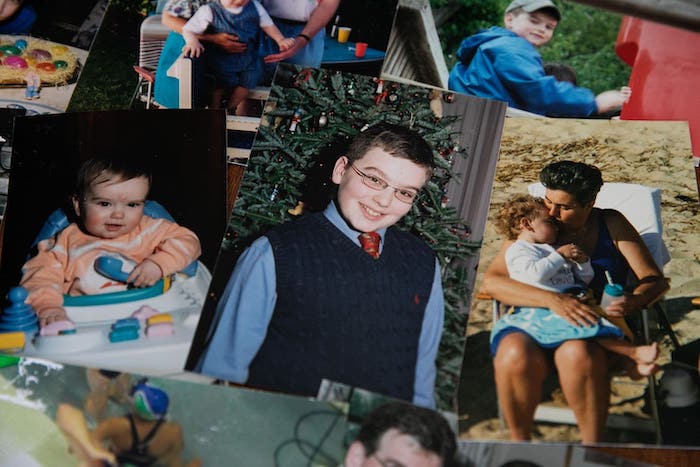
A collection of photos of Anthony Gabriel Brescia-Connell, who was 16 when he was transported from Boston Children’s Hospital to his home in Medford, Mass., where he died on March 3, 2011, surrounded by his family and beloved stuffed animals.
Megan Thorvilson, a pediatrician and palliative care specialist at Mayo, said palliative transport aims to address a gap between families’ preference and reality.
Most parents of terminally ill children would prefer that their child die at home, but most of these children die in the hospital, most commonly in the intensive care unit. Most pediatric ICU deaths happen in a controlled way, following the removal of life support, she said. That means there may be time to move the child to an alternative location to honor a family’s wishes.
Transporting children on life support is risky. At a palliative care conference, a nurse from Children’s Hospital of Philadelphia described the difficulties staff faced in trying to fly a 10-year-old girl home to Michigan. After she was rolled on her side several times to be transferred between vehicles, the child died before the plane could take off.
And dying at home is not what every family wants.
“We do sometimes overly romanticize the death at home,” Thorvilson acknowledged. Some parents would much rather have a child die in the hospital, with familiar nurses at the bedside for medical and emotional support. Some would rather keep this traumatic experience away from where they live.
Brescia, however, said she couldn’t bear to return home without her son.
A biologist who used to run an electron microscopy lab, Brescia wasn’t sure whether she and her husband, Brian Connell, would ever have children. Fertility treatments didn’t work. But on June 23, 1994, seven days before Brescia turned 44, she gave birth to a baby boy.
“Anthony is the love of my life,” said Brescia, who is now 68. “The OB/GYN put him on my chest and I really thought that my heart was going to burst.”
The mother-son bond was especially close: Brescia home-schooled her son for most of his life. Anthony grew to be 6 feet tall, full of curiosity. He loved identifying mushrooms, studied Arabic and oceanography, and aspired to go to MIT. He was an avid swimmer, competing on a team in Belmont, Mass.
One day in late 2010, while racing the backstroke, he became disoriented in the pool and was disqualified.
A neurologist prescribed rest. But over the next two weeks, Anthony grew only more tired and began to lose his balance. On Dec. 20, he was taken to Boston Children’s Hospital and diagnosed with a brain tumor.
The disease “came out of nowhere,” Brescia recalled. “He went from looking incredibly healthy and swimming like a healthy kid” to living at the hospital. At his bedside, she told him she’d bring him home to celebrate Christmas and eat stuffed shells.
His condition deteriorated quickly. The tumor could not be surgically removed. Anthony pushed through radiation and chemotherapy with the hope of going home, but the treatments failed. By late February 2011, the tumor began pressing on his brain stem, and fluid was building up in his brain.
Anthony was unconscious, relying on a ventilator to breathe. Brescia connected with the hospital’s palliative care team.
“I want to bring him home tomorrow,” Brescia told staff.
“I was scared to death he was going to have another incident,” she recalled. “I didn’t want them to do any more invasive procedures to reduce the pressure on his brain.”
Staff from the ICU, palliative care and transport teams scrambled to honor her request. The critical care transport team arranged for the use of its ambulance, a mobile ICU the size of a small bus.
The night before the trip, Brescia said goodbye in the privacy of Anthony’s hospital room.
“I don’t want to lose you,” she told him, holding his hands. “I’m going to let go. I want you to go where you need to be.”
On March 3, 2011, Brescia and her husband boarded the bus along with Anthony, a chaplain, two doctors, Nelson and a nurse from the ICU. They rode 10 miles to the family’s home, where Anthony was laid on a hospital bed in his living room, surrounded by his stuffed animals, on his favorite flannel sheets.
A pastor held a service for Anthony, and close family gathered to say goodbye. Then Brescia signaled for a doctor to disconnect the ventilator.
Anthony seemed to be at peace, Brescia said. After he died, she climbed into the bed with her son and held onto him for a while.
The death was still traumatic. But “it was really a gift to bring him home,” she said. “It was a significant act of compassion and kindness and love on the part of the Children’s staff.”
After Brescia’s experience, Nelson was inspired to offer the choice to more families.
First, she interviewed Brescia and other parents about whether palliative transport had a positive effect. All nine parents said it had. One family described holding a celebration when they brought their newborn baby home, even though he was about to die. They took family photos and used the nursery they had set up, establishing a brief sense of normalcy for four days before he died.
In her 14 years on Boston Children’s critical transport team, Nelson has found that parents benefit from palliative transport for various reasons: At home, they’re away from the noise of the hospital. They have control over who can visit. They feel more comfortable. And they don’t feel rushed after their child dies.
Nelson created a protocol that allows the hospital to offer palliative transport in a more routine way. Now, when children come to any of the hospital’s four ICUs, Nelson said, “we have the power to say, ‘You have a choice when it comes to the end of life.’ ”
The practice appears to be spreading.
After Lindsay Ragsdale, the physician who is director of the palliative care team at Kentucky Children’s Hospital in Lexington, presented her protocol for palliative transport at a conference last year, staff from 20 hospitals asked her to share her checklist, she said.
Mayo’s Thorvilson, who has worked closely on a half-dozen palliative transports, said it’s possible these last-minute trips from ICU to home could be avoided by earlier referrals to hospice, which might get kids home sooner. But when children with complex illnesses get sick, she said, “sometimes it’s hard to know whether this is just another bump in the road, or whether this is the natural end of the child’s life.”
“There’s something really unique about a child dying,” she said. “Everyone’s heart breaks, and we want to be able to do all that we can to be able to support the family in the midst of the tragedy.”
Eight years after Anthony’s death, his bedroom remains untouched, his socks still folded in his top drawer, swimming trophies on the cabinet, slippers under his chair. Pictures of him adorn every room in the house — on the fridge, the kitchen table, the living room stereo.
Looking through photos one recent morning of her son fishing and blowing out birthday candles, Brescia struggled to hold back tears.
“I couldn’t cure him,” she said. “I failed to protect him from a tumor — that’s how you feel. They did all they could. It wasn’t enough. Bringing him home was the best I could do.”
Nurse practitioner Nikki Johnston has been awarded the inaugural Health Minister’s Award for Nursing Trailblazers.
By Steve Evans
Nikki Johnston is passionate about dying.
She’s just won a big prize as Australia’s most innovative nurse. It was a recognition of the way she is changing the way the elderly end their lives.
Her mission as a nurse in Canberra is to help people have what she calls “a good death”.
She says too many people have “bad deaths” where fear and loneliness dominate their last moments.
Her radical idea is to involve people who are in their last months in the planning for those final fearful moments. The dying attend meetings where their own deaths are discussed.
She says a rigorous study of the results of the new system demonstrates clearly that it is a better way, and she’s pressing politicians to adopt it in the rest of Australia and beyond.
She also thinks there is too much emphasis on research to prolong lives at the expense of spending more to ensure that people die in peace at the right age.
Ms Johnston is a “nurse practitioner” who works in palliative care – it’s the most senior type of nurse, qualified to diagnose illnesses and prescribe drugs and treatments.
She has a missionary zeal for involving the patient in (arguably) the most important process affecting them – their end.
In the residential homes where the system is now used, the dying person attends the meetings and hears how their death will be dealt with. Their views are listened to and acted on.
“If we don’t ask the questions and give people the opportunity to talk about the end of life, we risk isolating people in their last months,” she says.
“They feel like no one gets it – no one understands – what’s going on, and that can be frightening.”
Researchers have studied 1700 people in the ACT at the end of their lives, comparing those where the system is in operation and those where it is not.
The study – the first of its kind in the world – involved rigorous measurement of a raft of variables like how soundly people slept in their last months and how much medication they needed.
The researchers devised a “quality of death” index. Ms Johnston says the results show that the new way works.
She argues that there should be a switch from maintaining uncomfortable and painful lives to the quality of death. “People are living longer but their quality of life is reduced so they are not living well enough or dying well enough,” she says.
“We are not valuing the end of life because we are not putting money into it.”
With the new system, people aren’t told bluntly that they are dying.
Ms Johnston says that she might have a conversation with a resident of an aged care home and ask them how they saw their future. In that conversation, the old person might well say that they thought they were dying.
“I ask them where they are at, what’s important, and most people tell me they are dying,” Ms Johnston says.
“If they are leading this conversation, It’s not confronting. They have taken us there.”
“Gently, we normalise death and dying. We help the staff to be able to talk about it. We support the relatives and loved ones through the process.”
She said that the elderly people she deals with generally don’t fear death. “Most people are ready. They are sick and they’ve had enough. They are ready to go.
“To help someone in their last months of life, we need to know them – to sit with them and talk to them. We need to know what’s important. How do we get this right for the person?”
That is what happened, for example, with Chris Dillon, whose death on March 29, 2017 was peaceful, according to her daughter Rose.
Chris Dillon and family dog, “Dublin”.
The aged mother had been in a residential home in Ainslie for just over two years.
According to her daughter, Mrs Dillon said one day that she felt tired and she was close to the end of her life.
Once that was recognised, the palliative care team became involved.
“She was a pragmatic person,” Rose says.
“She wanted to know what it would feel like, would it hurt, how would people know that she was dying. What would they do with her body?
“And then Nikki came along. She sat down really close to Mum and said: ‘I’m Nikki. I’m from palliative care and we need to talk about some things’.”
According to Rose, her mother simply replied: “What? About me dying?”
“So the conversation started naturally,” she says.
“The impact that Nikki had on Mum’s death was massive. It allowed Mum to have a peaceful death.
“She wasn’t frightened.”
The new system involves staff keeping a kind eye on residents
At the Calvary Haydon Retirement Community in Bruce, for example, manager Kim McGovern says she and her staff quietly look at residents every month to see “who might not be there next month”.
Kim McGovern of Calvary Haydon Retirement Community in Canberra.
Once people are identified, they are talked to sensitively.
An “individual care plan” is drawn up with the involvement of the resident.
“It’s their choice. We involve them early on,” Ms McGovern says. “It’s their last journey.”
The involvement of the dying person allows proper preparation, both medically and emotionally.
This means a final crisis, in which the patient is rushed to hospital to die in a chaotic emergency, is less likely.
Ms Johnston is an extraordinary character – bright and vivacious (at least when she’s expounding on the importance of helping people have “a good death”).
She may have dark moods, in that she says she needs to put her “armour” on before she attends some deathbeds.
And she does cry – after all, she’s got to know the person – but, as she puts it, “this isn’t my grief”.
In a survey at the start of this year, more than 8 in 10 U.K. adults said the role of hospices would become more important in the next decade.
By Dominic Rech
It’s approaching 1 a.m. in Bilborough, a suburb of the British city of Nottingham. Peter Naylor, 70, is slumped in his bed, only yards from the front door of his small bungalow.
He can’t walk, so we unlatch the door and reach him immediately. The low buzz of an oxygen concentrator greets us.
Tubes run around Naylor’s ears and across his face and curl up into his nostrils. Framed family photos are nestled on a shelf by his side, each capturing intimate moments from his life.
We too are experiencing an intimate moment with him — but for an entirely different reason.
He’s dying.
A Nottinghamshire hospice team that cares for the terminally ill is three hours into a night shift. Naylor is the third patient they are visiting.
He’s been struggling with diabetes and has had multiple heart attacks. His breathing is heavy and pronounced. He exhales before opening his mouth slowly to say, “I’m stuck on this bed. I have been for more than one year. I can’t get off. I can’t go to the toilet. I can’t do anything. I just lie here.
“I’m near the end of my life. It could be any day now.”
Outside access to hospice night services, like this one, is unusual given that patients are at a very vulnerable stage of life.
But the hospice team granted CNN access because they want to show how palliative care is provided in the UK and make us think more about the kind of death we want for ourselves and our loved ones. The topic is close to my heart because the team looked after my father before he died this year.
“We all think we are immortal, so we want to put more money into saving lives; no money is being put into palliative care because we don’t accept we are going to die,” said Tracey Bleakley, the chief executive of Hospice UK, the umbrella organization for hospices.
‘It means everything’
Hospices offer specialist care and support to people with terminal and life-limiting illnesses. They coordinate with the UK’s National Health Service to provide care for people who are often in the end stages of life, commonly those who no longer want to be in the hospital and want to receive care at home.
It costs £1.4 billion ($1.8 billion) a year to run hospices, according to the charity Hospice UK. They are funded partially by the National Health Service but rely heavily on fundraising and donations.
During our time with the overnight hospice team, we met multiple people receiving end-of-life care. Given the sensitivity of their personal circumstances, some patients didn’t want to be interviewed or photographed.
Naylor was willing to speak to us. After leaving a care home, the 70-year-old opted to receive end-of-life treatment in the comfort of his own bungalow.
But his condition progressively worsened. On one occasion, he fell while trying to go to the toilet. He was alone and unable to move. It was three hours before anyone came to help him.
As a result, the care he receives has been ramped up, and he not only gets visits from the overnight hospice team but now has a full-time carer who lives with him during the day. The extra support allows him to relax and sleep better.
“It means everything,” he said. “It’s the nighttime when I get frightened, when I am here on my own. But I roughly know when they are coming and can call them if I really need them.”
Life expectancy was increasing, and the way people were dying was fundamentally changing, he said. More people were dying of long-term, chronic illnesses such as cardiovascular diseases and cancer rather than infectious diseases.
Hospices took up the mantle of caring for people with these long-term terminal illnesses. Now, there are more than 200 hospices in the UK. The number of hospice programs in the United States has been on the rise since the first program started there in 1974; there were 5,800 as of 2013.
However, in many low-income and middle-income countries, end-of-life care is poor, according to The Lancet Global Health journal. Tens of millions of people in need of palliative care have severely limited access, even to oral morphine for pain relief.
Naylor is adamant that he wants to die in his own home — something that happens to less than a quarter of people in England, according to the UK’s Office for National Statistics.
He’s not alone. Before meeting him on the overnight hospice shift, we visit the home of Harry and Serena Perkins in Nuthall, Nottingham, just before midnight.
It becomes obvious that this visit is a routine one for both the hospice team and the patient.
We are welcomed by Harry’s warm gaze in the hallway. The 96-year-old was an engineer during World War II. After quickly greeting us, he shuffles off into the lounge with his wife.
He has been married to Serena since 1973. They met when Harry was checked into a hospital with pneumonia; Serena was his receiving nurse.
“I would have said this is the finest girl I could have ever married,” he says, perched on the sofa next to her.
Harry, who has bowel cancer and heart problems, uses the day support provided by the hospice once a week, when he sees friends and accesses day therapy. He is also visited by the night support team about 11:30 p.m. every night.
“I thought it was a nuclear bomb that was going to take me, but that’s finished. So it will be my heart or the cancer that takes me.”
Despite his health, Harry seems more concerned about Serena’s well-being than he is about his own.
“We look forward to them coming every night. They are lovely people. They take me upstairs to bed, get me changed,” he says. “But they also talk to my wife. Keep her company, which is very important.”
Serena too is grateful. “I didn’t realize what a weight I had only my shoulders until they came. It’s really given me my freedom back in a way,” she says.
The care helps enable Harry to continue living with Serena in their home. It allows him to enjoy the quality of life he wants.
As we get ready to leave, Harry stands to get ready for bed. He shakes my hand firmly and mumbles a proverb from former British Prime Minister Winston Churchill: “Never give up. Never, never, never.”
Who’s providing the care?
The Nottingham hospice CNN spent time with is a charity.
Although a third of its income comes from the UK’s National Health Service, the rest comes from fundraising; the hospice has to raise an average of £7,000 (about $9,000) a day in order to operate the services it provides, according to Jo Polkey, head of care at Nottinghamshire Hospice. Many hospices across the country face a similar funding shortfall.
“Somebody that requires palliative nursing care is when there is no treatment options left. Trying to make someone as comfortable as possible. We want to add to their lives rather than think of it as the ending,” she says.
Its main service is Hospice at Home, through which more than 60 nurses and health care care assistants provide care at home to people with terminal and life-limiting illnesses. They also provide the overnight support teams, a day therapy unit, and a bereavement care and support service.
“We are often dealing with people very much at the end of life and in the last few days, weeks and hours of life,” Polkey said. “I think our average length of stay [of a patient] is about 26 days. They don’t stay in the services very long before they die.”
What does it take to be a member of a hospice team? One of the first things she says is that they are very “resilient.”
The night shift is arguably where this is most palpable.
‘People die on your shift’
Two overnight carers, Deborah Royston and Sonia Lees, describe the highs and lows of their jobs in between visits to patients.
Aside from the late hours, the job requires a lot of driving, with many of the patients living across Nottinghamshire, a county near central England that is home to just over 800,000 people. The shift usually usually starts at 10 p.m. and finishes before 7 a.m.
Royston says she finds it particularly difficult when she develops close relationships with patients.
“It’s really sad … to deal with death on a daily basis. Sometimes, people die on your shift, but it’s good you can be there for both them and the family members in that time of grief.”
Another visit we made was to the Wollaton home of Linda Wagner, whose husband, Bob, relies on overnight hospice support. He has progressive supranuclear palsy, a rare condition that can cause problems with balance, movement, vision, speech and swallowing.
“I know some people don’t believe in angels. Well, I do, but that is how I would class [overnight carers] — as angels,” she said. “I didn’t know the support was out there before. If I’m struggling, I know there are other people out there going through the same thing. It’s just a wonderful thing.”
Despite difficulties that come with Royston’s field, she described the job as her “passion.” She’s been helping provide night support for 12 years and finds the opportunity to build relationships with patients and their families fulfilling, even though it can be heart-wrenching.
“I just love it. It makes my heart feel good. I get quite emotional about it because you meet some nice, wonderful people.”
A looming crisis in palliative care?
A pun doesn’t always seem fitting when talking about death, but Polkey’s use of one seems to strike a chord: “People are dying to come to our services,” she says.
Over the past three years, hospices have helped more than 200,000 people across the country annually, Hospice UK’s Bleakley says. However, research by her organization in 2017 found that 118,000 people each year could benefit from hospice and palliative care don’t receive it because they live in an economically deprived area, live alone or have a certain type of terminal condition, among other reasons.
Bleakley thinks there is a crisis in palliative care that is only going to get worse.
“We had a massive baby boom after the war, and now those people are starting to die, so we are already going to have an increase in the death rate. We are all living longer, and we are all ill for longer at the end of life.”
The UK’s aging population is only going to increase the pressure, Bleakley says. In 2017, 12 million UK residents were 65 and older: approximately 18.2% of the population, according to the Office for National Statistics.
In a survey at the start of this year, more than 8 in 10 UK adults said the role of hospices would become more important in the next decade.
Bleakley was also worried about what the UK’s planned exit from the European Union might bring.
“Anything that affects consumer confidence, from companies having extra money for supporting hospices financially to people choosing to run a marathon to raise money — numerous things are affected by Brexit,” she said.
“And on the work force side, we will see more members sucked out” of the National Health Service.
Inclusivity challenges
Another challenge for practitioners is inclusivity.
Kellehear, of the University of Bradford, says that not many ethnic minority groups in the UK are accessing palliative care.
Nottinghamshire Hospice’s Polkey noted, “we look after a lot of white middle-class people. However, we are sat in one of the most diverse cities in the country. … We desperately want to reach into communities. Diversity is something we are working on.”
Hospice UK is running a campaign called Open Up Hospice Care to try to address this issue.
“There are people in the LGBT community … minority groups, people in prison — a lot of these people feel that a lot of the traditional services don’t work for them,” Hospice UK’s Bleakley said.
She also says that funding is going to be a fundamental issue for hospices.
The National Health Service’s Long Term Plan, earmarking the UK’s key health plans and priorities for the next 10 years, includes a bigger focus on community care and training people in palliative care, but Bleakley says there is no indication that any more funding would be put into palliative care.
“It costs 1.4 billion (pounds) a year to run hospices, and the NHS is putting 350 million in; they are not putting in the true cost of care or anything like it.” she said.
However, she doesn’t just hold the government responsible. She says society as a whole has to be more engaged when it comes to end-of-life care.
Kellehear agrees. He promotes the idea of compassionate communities and cities, a more holistic approach to palliative care that includes the bereaved as well as those who die.
It is based on the idea that care shouldn’t fall simply to doctors, nurses and the surrounding families of dying people. Instead, the wider community should step in to support people with terminal illnesses.
“We shouldn’t wait for disaster to happen. It’s about going into the schools, going into the workplaces, and saying ‘look, this is everybody’s business. What are you doing to do your bit?’ There’s not enough of that going on in the UK.”
For example, he says, schools should prepare kids for what to do should a fellow student lose a loved one.
“The people we keep forgetting in palliative care is the bereaved, who often suffer from similar social consequences as people with life-limiting illnesses: depression, anxiety, loneliness, social rejection and even suicide,” he added.
“These people are best helped when communities come together to support the people who are at risk of these things.”
Bleakley thinks we need to face up to the reality of death more often.
“A good death is a legacy for the people we leave behind.”
Palliative care is a growing specialty that provides comfort care and that teaches patients and doctors how to talk about patients’ goals for life with serious disease and how to prepare for a good ending.
That’s what the family of a patient told Sunita Puri when she was a resident in internal medicine. They were chilling words for the young doctor as she took over the care of a very sick man on the overnight shift.
To Puri, the patient, who had widespread metastatic liver cancer, appeared to be dying. She tried to talk with the family about forgoing heroic measures, to let him have peace in his last hours. But they were adamant.
“Do everything,” they told her. Hours after admitting him to the intensive care unit, she was overseeing chest compressions to revive him after his heart stopped. “I was blinking back tears,” she recalls. The man died that night.
Few people would say they want to die while undergoing painful last-minute resuscitation or while hooked up to machines in a hospital. Yet it’s the death many Americans end up with. Now a palliative care doctor at the University of Southern California, Puri is fighting for an alternative.
In her new book, That Good Night: Life and Medicine in the Eleventh Hour, Puri writes about how palliative care specialists are working to change medicine from within — teaching other doctors how to talk to patients about their hopes and fears, not just their disease and treatment. Palliative care, she says, gives doctors, patients and their families a new vocabulary with which to talk about the way life’s goals can shift when you have a serious illness and how to plan for a good final chapter.
We spoke with Puri about the field of palliative care and what patients need to know.
This interview has been edited for clarity and length.
What is palliative care, and how is it different from hospice?
Palliative care is attending to the physical, emotional and spiritual suffering of patients and families who are dealing with a serious illness. Hospice is a type of palliative care that we provide in the last six months of life. And I would say hospice is even distinct from end-of-life care, which is really the care of patients in the last days and hours of their lives.
In our country, hospice is overwhelmingly provided in a patient’s home or in a nursing home, whereas palliative care is available at any stage of an illness. And so we can see people in the hospital; we can see people in clinics when they come to see their oncologist or their cardiologist. With palliative care, you can have us on your team just right alongside care like chemotherapy or dialysis — we’re meant to attend to your quality of life. And in an ideal circumstance, we will be there when you decide to transition to hospice.
How common is it now to have palliative care specialists available?
There’s actually very few of us, and many of us are concentrated in the big cities. So in rural areas or in nonacademic teaching hospitals, there’s definitely a shortage of palliative care docs around the country. Our presence and the need for us is growing though. So for example, the American Society of Clinical Oncology now has a recommendation that at the time of diagnosis of a serious illness, palliative care should be involved. Patients with a serious illness can ask for a consultation with the palliative care team if their other care providers don’t bring it up, either in a hospital or a clinic setting.
We have studies that show that for patients with, for example, metastatic lung cancer, if they got palliative care right alongside their cancer treatment — as opposed to just getting cancer treatment alone — the patients actually lived longer and had better quality-of-life scores.
What other advantages does palliative care offer?
I think the emotional and spiritual aspects of it are actually some of the most important supports that we can offer our patients.
One thing my patients tell me a lot is, “Thank you for listening.” And I think there is something about our field — focused on being silent and listening to people — that is deeply therapeutic for the vast majority of my patients. To say, “I’m going to be with you through this whole journey, no matter what the outcome with your treatment, and work with your other doctors to make sure we’re all on the same page about what therapies may or may not actually be helpful to you in the way that you define helpful.” I think there’s something pretty magical about that.
You wrote that when you found palliative care, you were finally able to become the kind of doctor you wanted to be. What did you mean by that?
I grew up the daughter of an anesthesiologist — she was always my first model for what a doctor should be. My mother is very technically skilled, but she is also deeply devoted to the idea that every human being is kind of an embodiment of the divine who she felt she was in service to. So, she really had this beautiful intertwining in her practice of being very scientific but also being very spiritual — being able to take people to the operating room and control their physiology to get them through an operation but also understanding that the body and nature has its limits.
And that’s what I wanted to be: somebody with the technical and scientific command of medicine but who understood that every human life is different from the other. In my medical training, there were so much focus on the technical and scientific aspects. But as I was learning those things, I was not also learning how to talk with someone who has a serious diagnosis. How do you explain to them how their life might change? How do you ask, if this is not something that we can cure, “What would be really important to you in the time that you have?” And this language was not given to me in medical training.
When people get a diagnosis like cancer, they sometimes talk about “being a fighter” or “fighting the disease.” Why do you find that kind of language problematic?
When we think of disease as a battle to fight, you kind of divide people into winners and losers — which is not a mentality I think benefits them.
What’s dangerous is that when we’re talking about a fight, if someone chooses not to “continue to fight,” then people will often tell me, “I feel like I’m giving up.” I have to reframe that for them to say, “You may be a fighter, but your body cannot fight this anymore. Can you hear that distinction between you and the natural limits of your body?” I have found that to be incredibly potent because people can see that this isn’t a personal thing.
You know, you did not deserve to get this horrible bout of heart failure, and your not “beating it” is not your fault.
What are the consequences for doctors and for the patient’s treatment of using this kind of language?
I think people feel an obligation, if they identify as a fighter, to keep trying any and every treatment offered to them — sometimes without a full appreciation of the risks of those treatments or whether those treatments might keep them in a place they don’t want to be, like an intensive care unit, instead of having the opportunity to go home. I think that sort of “fight or give up” mentality is such a toxic binary. And I’ve seen people suffer tremendously because they felt that if they said no to therapy, that they would be letting other people around them down.
From my perspective, when I was in my residency, when I heard those words, I then felt obligated to offer anything and everything to the patient or family — even when I knew that certain treatments were not going to help them but could very well hurt them. So I think hearing those words almost put a stop to any real in-depth conversation about what someone is hoping for and what realistically we as physicians can offer them to fulfill those hopes.
I still regret the ways that I offered therapies to patients that I knew would not be in their best interest. But I didn’t know how to talk about another way when I was in my training.
What kind of therapies might be harmful or not be in their best interest?
Being in a clinical trial is one example of a therapy people often feel they need to take but may not truly be in their best interests if it, for example, requires them to uproot their life and go elsewhere. Or if it has side effects that we may not really know about, because part of the trial is to figure out what the toxicities are.
And the other scenario I’ve seen is people in the ICU with an overwhelming infection or a set of post-surgical complications, and they’re suffering one complication after another, especially if they’re elderly. And we can keep trying to manipulate their physiology, using very powerful medications and machines, but we’re not always as attentive to what someone’s life would actually look like if we were successful in reversing some of the problems that they’re going through.
So when a palliative care team is involved and you have these kinds of difficult discussions early on in a serious diagnosis, what can a good outcome look like for the patient?
The advantage of getting to know people and their family early on when they first get a diagnosis is that we can really help them through their treatment. To think about and articulate what’s most important for them if a specific treatment doesn’t work or if it takes a huge toll on their quality of life. And when we can have those discussions, then a happy ending might be that they have their pain, their shortness of breath, their nausea, all of those things exquisitely well controlled. And they decide on their own terms when to transition, for example, to hospice.
When I was a hospice doctor, I think the best situations were when people were still able to be themselves and participate as much in living as they could — even though their bodies were failing. They could still be cognitively intact. Their symptoms were well controlled. They were in a place they wanted to be in. They were living their lives on their own terms for however long they had. And that to me is what a good ending can look like.
Even other doctors don’t always understand what palliative care is or embrace it. What do you think the obstacle is?
I think doing what we do in our field is a little bit of the rejection of our culture’s idea of what medicine exists to do. I think the public thinks of doctors as heroes that can beat diseases and extend lives. And in many important ways we are heroes. Surgery is safer. Childbirth is safer. We’ve eliminated certain infectious diseases almost entirely because of vaccines. But I think we are not good at knowing what to do when we can’t fix a problem.
For patients who have a terminal diagnosis, what advice would you give about how to decide whether or not to opt for some of the more extreme life-sustaining measures, like going on a ventilator or a feeding tube?
In planning ahead, I always encourage people to think about the quality of life that they value. What are the things that they would be OK not doing? And what are the things that if they couldn’t do them would make their life extremely difficult — maybe even not worth living? And if people can think about their values and their goals in broad strokes, the broad strokes can help inform the more specific question about CPR or a ventilator.
I encourage families to really look to their doctors to guide them. And to say, if there’s a question about going on a ventilator, “Is this for a reversible condition, as far as you can tell, doctor? Or am I taking a gamble, a big enough gamble that he may be stuck on the ventilator forever, and then I would have to make the decision to stop? Tell me more about that.” I think being able to ask your doctor openly and not feel alone in making some of these weighty decisions is extremely important. So there are those two components of it: thinking yourself, “What is the sort of life I value? What would be a life that would be too hard for me to live even with the help of medicine?” And to talk to your doctor, even if you’re healthy right now, because you want to prepare for the storm.
“People in this country don’t talk about death. When I would talk about it sometimes with people they would say, ‘Oh be optimistic! Don’t talk that way. You’re gonna be fine.’ You really need to look at it (death) and this is the perfect way to do it.” Ann Levy – psilocybin-assisted psychotherapy study participant
I remember the ride home being really quiet. Typically, my mom would be driving me nuts, loudly singing old Methodist hymns, rather than letting us listen to music on the radio. But this time she just drove silently as my grandmother, Lillian Brustad, stared out the window of our well-traveled station wagon. We had just left my grandmother’s oncology appointment in Rochester, New York and we were heading back to her home in Hamilton. There was no discussion about the appointment, no talk about any diagnosis, no ‘next steps’ and no ‘why me’s?’ What was said was said in a meeting with my mother, my grandmother and her doctors.
I’d break the silence with my repetitive pre-teen complaints as to why we should have stopped in Rochester, rather than waiting until Syracuse to pull into a Friendly’s restaurant for a Jim Dandy sundae. I’d debate from the back seat that stopping in Rochester would have made me full and happy. Stopping would have better allowed me to finish this book report on Mickey Mantle that I was putting off.
When I wasn’t complaining; there was silence…
We made many more trips to Rochester over the next few years. My grandmother remained stoic in her battle against cancer, despite it wreaking havoc on her physical body, eventually taking her life.
The final months of life are often marked by increasing physical and emotional suffering. As one approaches death, we often experience varying degrees of depression, hopelessness, anxiety, and a desire to hasten death. The prospect of our loved one’s looming death can lead to feelings of defeat, helplessness, and despair in family members and within the patient’s medical team.
How do you want to die? Most people hope to die at home, with their loved ones, but sadly an overwhelming majority of us die in a hospital or extended care home surrounded by beeping equipment.
What would a good death look like? Anthony Bocelli, PhD, is a palliative care psychologist and investigator in a study conducted at the NYU School of Medicine on the use of psilocybin-assisted psychotherapy to help patients and families deal better with end-of-life distress.
“Death needs to be humanized,” he says. “Although the end-of-life can be profoundly difficult, it can also trigger a search for meaning and an openness for the sacred.”
Maria Sabina called psilocybin mushrooms her ‘saint children.’ Sabina was the Mazatec curandera/healer that banker Gordon Wasson sought out to learn the secrets of ‘magic mushrooms.’ Sabina introduced Wasson and his wife Valentina to teonanácatl; the Psilocybe mushroom. ‘nti-ši-tho in Mazatec, meaning the ‘Little-One-Who-Springs-Forth’.
Wasson went on to famously detail his psychedelic experience in Life Magazine, introducing these sacred mushrooms to the Western world. Albert Hofmann, discoverer of LSD and chemist at the Swiss Sandoz Laboratories, isolated psilocybin in 1957 from mushrooms collected by Wasson’s team on their second trip to Oaxaca.
These sacred mushrooms have been used for millennia by indigenous cultures around the globe for healing and insight. Psilocybin-assisted psychotherapy melds this ancient sacred wisdom with modern day scientific technology. I am not talking here about eating a bag of ‘shrooms and tripping at a rock concert; this is about the therapeutic use of this valuable tool in a controlled setting under supervision by trained guides to help combat depression, addiction, and existential distress.
So why psilocybin mushrooms and why now? It has been said that psychedelics could be to psychiatry, what the microscope is to biology or the telescope was to astronomy. Bear in mind that telescopic science was prohibited in 1616 for over 100 years, in fear that people may discover that planet Earth was not the center of the universe.
Alicia Danforth, Ph.D, served as investigator on a psychedelic research study at Harbor-UCLA Medical Center examining the safety and efficacy of psilocybin as a treatment for advanced-cancer anxiety. She remarked, “It’s very important not to lose sight of the fact that research with psychedelic medicines has been going on for thousands and thousands of years. As long as there has been humans really. What’s new is when you get into the Western medical model.”
Dr. Danforth worked with Dr. Charles Grob on an important pilot study at Harbor-UCLA Medical Center on 12 patients who were facing end-of-life from advanced stages of cancer. Subjects were administered a placebo (niacin) during one session and the other session they received psilocybin.
I had the pleasure of discussing the study and their findings with Dr. Danforth. “Our participants were really near death. Some did not survive the six-month follow-up period,” she said.
Dr. Danforth detailed that they administered “one session at a low-to-moderate dose because we were the first cancer-treatment study in a new wave of psychedelic-assisted therapy and the FDA was really conservative. The main purpose for these little pilot studies is to establish that they are safe and is it even achievable. Does it work?”
The other studies that I will cite in this article worked with higher doses of psilocybin. However, Danforth stated that, ‘even with one session of preparatory psychotherapy session before (treatment day), then a really supported session on the day of treatment, then therapy afterwards, our study found a reduction in anxiety and a trend toward a reduction in depression.” She continued, “It’s more important to look at the trending that leads to larger studies so you can make stronger claims. We saw positive trends and there was a significant difference in the anxiety scores. The qualitative outcomes were good; the safety data were good. We didn’t have any serious adverse events and everything was green light go for the larger studies.”
As Danforth mentioned, humans have been conducting research for thousands of years on psychedelics. Prior to prohibition of these substances in the late sixties, there were more than a thousand studies conducted with more than 40,000 subjects and many showed positive trends.
During the 1960’s, Dr. Eric Kast, from the Chicago Medical School utilized LSD for a series of studies working with cancer patients encountering death. Several hundred advanced-stage cancer patients were administered LSD. Findings showed trends toward pain reduction for several weeks, relief of depression, improved sleep, and a lessened fear of death. Dr. Kast noted that some of these individuals showed a striking disregard for the gravity of their personal situations. They frequently talked about their impending death with an emotional attitude that would be considered atypical in our culture.
Another important study by William Pahnke from the Maryland Psychiatric Research Center, in Baltimore conducted a study that was published in the Harvard Theological Review in 1969. His work examined the psychedelic mystical experience in the human encounter with death. He found, “The most dramatic effects came in the wake of a mystical experience.” He reported a decrease in fear, anxiety, worry and depression. Often the need for pain medications was lessened, because the patient was able to tolerate pain more easily. There was a profound increase in serenity, peace, and calmness, with a marked decrease in the fear of death.
Roland Griffiths, Ph.D., is a Professor in the Departments of Psychiatry and Neurosciences at the Johns Hopkins University School of Medicine. He is the principal investigator of the Johns Hopkins Psilocybin Project. He and his team have been studying the effects of psilocybin and its ability to bring about mystical experiences. Their team conducted the largest and most rigorous study in this new wave of psychedelic research involving fifty-one patients who had received a potentially life-threatening cancer diagnosis.
“We found that the response was dose-specific,” Dr. Griffiths said. “The larger dose created a much larger response than the lower dose. We also found that the occurrence of mystical-type experiences is positively correlated with positive outcomes. Those who underwent them were more likely to have enduring, large-magnitude changes in depression and anxiety.”
The Johns Hopkins group reported that psilocybin decreased both clinician and patient-rated depressed mood, anxiety, and death anxiety. The results showed increased quality of life, sense of connectedness, and optimism. Participants expressed an increased belief that death is not an ending, but rather a transition to something even greater than this life. About 70% reported the experience as one of their top five spiritually significant lifetime events, including the birth of a child or death of a loved one.”
He continued, “There are potential risks associated with these compounds. We can protect against a lot of those risks through the screening and preparation procedure in our medical setting. About 30 percent of our people reported some fear or discomfort arising sometime during the experience. If individuals are anxious, then we might say a few words, or hold their hand. It is really just grounding them in consensual reality, reminding them that they have taken psilocybin, that everything is going to be alright. Very often these short-lived experiences of psychological challenge can be cathartic and serve as doorways into personal meaning and transcendence.”
Dr Charles Grob, the principal investigator on the UCLA study reported similar results, “Psilocybin facilitates a greater likelihood of achieving a psycho-spiritual state of consciousness — a mystical kind of experience. The old research literature from the 50’s and 60’s very strongly indicated that individuals in psychedelic research studies, who experienced a spiritual epiphany during the course of their many hour treatment sessions, were more likely to have a long-term positive therapeutic outcome.”
Why does psilocybin appear to efficacious, while modern pharmaceutical efforts are largely ineffective?
Dr. Griffiths explains, “Psilocybin acts very selectively at serotonin-2A receptors, which are a neurotransmitter that promotes positive feelings. Acting like a ‘lock and key’, so psilocybin can click in to this receptor site and activate a variety of processes.” With all of the classical psychedelics; LSD, psilocybin, mescaline; the thing that they have in common is that they activate serotonin-2A receptors.
Dr. Danforth added, “Sometimes when we are in a challenging situation in life, our thoughts can get stuck in a loop. Negative thoughts just continue and continue and continue and psilocybin in a therapeutic setting can function like a big hand coming in and jiggling the needle on a skipping record, so that a tune can resume.”
Yet another study — this one conducted by NYU Langone Psilocybin Research Project — examined the effects of psilocybin on the psychosocial distress with patients with advanced cancer. This trial was led by Stephen Ross, M.D. and Anthony Bossis, Ph.D. Their study included 29 patients facing end-of-life. In their sessions, subjects were either given either a moderate dose of psilocybin or a placebo (niacin), cross-switching to the other after about seven weeks after the first session. Findings were very similar to the studies at UCLA and Johns Hopkins. They found that psilocybin produced immediate, substantial, and sustained improvements in anxiety and depression leading to decreases in cancer-related demoralization and hopelessness, improved spiritual well being, and an increased quality of life. At the six-month follow-up, psilocybin was associated with enduring anxiolytic and antidepressant effects.
The NYU researchers further reported sustained benefits in existential distress and quality of life, as well as improved attitudes towards death.
There is growing anticipation that psilocybin could be rescheduled and open up further opportunities for psychedelic research. Decriminalization of psilocybin is going to the voters in the city of Denver on May 7.
“I look forward to a day, that if it were clinically indicated to be able to offer that service to certain clients,” Dr. Danforth said. “Expanded access is not available yet; no one in the United States is able to legally work with Schedule I substances in a clinical setting,”
She continued, “It’s possible in the near future that some in the MDMA (ecstasy) world we will have expanded access for PTSD therapy. It’s hard to anticipate what’s going to happen with MDMA and psilocybin, but I don’t think it’s going to happen overnight. Everybody’s kind of waiting to see what happens in Denver and what that’ll mean… There are a ton of opportunists rushing in trying to make a buck, but in terms of real clinical work, that process moves at a snail’s pace, as it should.”
I asked Dr. Danforth on additional prospects for psychedelic-assisted psychotherapy. “My private practice is almost exclusively adults on the autism spectrum and some of them have very severe social anxiety and MDMA would be a real powerful clinical tool.”
She continued, “Others are very interested at looking at psychedelics for the betterment of well people. Two streams of effort working here — treating people that are unwell or providing guidance for those that are well, like we have been doing for thousands of years. They may have spiritual reasons for altering consciousness. It’s not all about getting a competitive edge in Silicon Valley, but it’s about how do we make our community healthy. For me it just happens to be the healing aspect. For people that are really suffering is where my interests lie.”
So what are the most promising areas in psilocybin research?
“Two of the most promising areas are Palliative Care; reducing the stress near the end of life and addiction studies,” Danforth replied. “I’ve always been really fascinated with the smoking cessation studies at John Hopkins and with Michael Bogenschutz M.D. (NYU) studies on alcoholism. I think that was one of the most promising areas of study from the first wave of psychedelic research in the sixties. I’d like to see more funding and research around treating addiction.”
Danforth said it’s frustrating not being able to use all the tools she’d like when treating patients. “I feel a bit like a firefighter who’s still allowed to fight fires, but I just can’t bring my hose,” she said. “The answer isn’t, ‘well let’s just give everybody fire hoses,’ because a lot of people could be hurt in an uncontrolled setting. I hope that we can find a middle ground.”
Dr. Danforth advises, “Psilocybin was used as a sacrament for sacred rituals, with a lot of reverence, wisdom, tradition, and mentoring. I’m not sure we are grown up enough as a culture to just have widespread access.”
Dr Danforth’s associate on the UCLA study, Gurpreet S. Chopra, emphasized, “I think it’s kind of ridiculous to be a scientist and a doctor and not investigate and try to understand how we can use these tools in a Western Culture safely.”
I posed a similar thought to local clinical psychologist and founder of the Alaska Psilocybin Society, Dr. William Kerst. Dr. Kerst finds that psilocybin being a Schedule I substance to be ridiculous. “It clearly has potential medical benefit as demonstrated by the studies that are ongoing and not only is it not necessarily addictive, but it tends to be anti-addictive.”
“Working with the Alaska Psychedelic Society, I have had several patients that are struggling with end-of-life anxiety, which is one of the primary uses of psilocybin in some of these studies and they don’t have time for legalization efforts to get pushed through. They need relief and it looks like these substances may be able to do that, and right now we have to say, ‘no’ to these patients and that’s terrible. It’s heart-wrenching, honestly.”
Should you have further interest in investigating psychedelic substances, the Alaska Psychedelic Society is holding their monthly meeting on Saturday, April 27 from 2 to 4 pm at Uncle Leroy’s Coffee, located at 701 West 36th Avenue in Anchorage. Also visit the Society’s Facebook page to keep updated on future meetings as well as recent studies and articles regarding psychedelics.
The entire lifespan of most African Americans is consumed by efforts to overcome obstacles, inequality, and in many cases, institutional racism.
The most difficult point in this most tiring journey is often the end-of-life. For the disproportionate number of us is when death is accompanied by the dilemmas around how we choose to die.
Hospice; Palliative Care; Advance Directives; and Compet-ency become terms that we, or our loved ones, all of a sudden are faced with and expected to deal with.
Studies and observations show that, likewise disproportionately, we are not prepared for this final stage of life.
What we know is that African Americans are less likely than any other group to be prepared for end-of-life, and not surprisingly, are less likely to have a prepared Advance directive.
First, let’s talk about Advanced Directives. This is the document that should be prepared to outline, in detail, what type of care (if any) we desire as our lives come to an end, and we are not able to make decisions for ourselves.
An Advanced Directive includes things that typically are not even thought about during times when life is good.
Generally, it will include things such as a living will or do-not-resuscitate order, or in identification of a health care surrogate. Regrettably, it’s not until we are in a hospital ICU; Hospice Center; or even on Home Hospice that we (or our loved ones) are confronted with having to make difficult decisions, while dealing with imminent death.
In spite of the fact that studies show that 80 percent of Americans would prefer to die at home, the reality is that 60 percent of us will die in a hospital; 20 percent of us will die in a nursing home; and only 20 percent will end up in a situation where we will be able to make our transition in the comfort and peace of our own home.
If you are not competent, or capable, to make medical decisions but do not have an advance directive, or it is unavailable when needed, decisions will nevertheless have to be made.
In 2013, The Pew Foundation did a study and found that while 73 percent of all Americans have given “some thought” to end-of-life, only 37 percent of African Americans have done the same. This means that doctors and others on the care team of a terminally-ill patient may decide to continue providing care and treatment, when you may feel that your loved one has had enough, and should be allowed to die in peace, with dignity. In the absence of an Advance Directive, this could become a point of contention, and the patient is caught in the middle. Or, it could be the other way around, you may feel that there is still hope for a recovery, and the doctors feel that there isn’t. Again, the patient lies there in limbo, and often suffering unnecessarily. For African Americans, it’s worse. One study found that only 13 percent of all African Americans have an Advance Directive in place.
It can be a difficult, and often, an uncomfortable conversation, but collectively, we have to begin to have conversations during the “good” times in life with our families and loved ones about what we do and don’t want should we ever find ourselves in a position where we are unable to make medical decisions for ourselves.
Think about how often we attend funerals, and families are still reeling over how things came to an end with conflict and contention between families of a patient who died, and the medical staff at the hospital. Think about how different it would be if we made our wishes known, before something happened unexpectedly.
A few things that may be helpful for you in getting an Advance Directive for yourself:
First you need to familiarize yourself with the term: life-sustaining treatments. Nolo’s Plain-English Law Dictionary defines this as “Medical procedures that would only prolong the process of dying or sustain a condition of permanent unconsciousness. A patient who is receiving life-sustaining treatment will die soon, whether or not treatment is administered. Life-sustaining treatment may include a respirator, cardiopulmonary resuscitation (CPR), dialysis, surgery, and other medical procedures.” Would you want any of these? If so, under what circumstances?
Most importantly, let your loved ones know what you have in your Advance Directive. People only like surprises for their birthdays. Don’t wait for them to find out at an emotionally difficult time, when they are grappling with the inevitability of your death.
You don’t need a lawyer to create your Advance Directive. But you do need to make sure you understand the laws of the state you live in regarding Advance Directives. Some states have restrictions that you need to be aware of that may prohibit your wishes.








 What other advantages does palliative care offer?
What other advantages does palliative care offer?
