When I ask Matthew Cullen to share one of his favorite experiences volunteering at the Joan Nicole Prince Home, his answer surprises me.
“Giving my first bed bath,” he says.
When you give a bed bath, “you use a wash cloth to wash a patient’s body,” Cullen explains, adding, “The residents are really grateful for it. One resident told me, ‘Thank you for that. I feel much better.’
This is the third summer that Cullen, a senior at Union College, has spent caring for dying residents at the Joan Nicole Prince Home in Scotia.
His shifts are a mix of mundane tasks aimed at making residents more comfortable and keeping them company. Sometimes that involves chatting at the kitchen table. Sometimes it involves sitting quietly while they rest or sleep.
“A lot of time I’m the only person here,” says Cullen, a native of Guilderland.
Helping terminally ill patients live their final days in peace and comfort might sound like a lot of responsibility for a 21-year-old college student.
But Cullen is more than up to the challenge. The ebullient red-head speaks of his work at the Joan Nicole Prince Home with insight, compassion, even wisdom.
“It can be sad sometimes, but the great majority of the time, it’s happy,” Cullen says. “The patients are sharing their memories and stories with you, and you’re doing the same.
Cullen isn’t the only college student who spends his summers volunteering at the Joan Nicole Prince Home.
He’s enrolled in a unique summer program, called CARE (Community Action Research and Education), that sends college students to volunteer in residential homes for the dying, which provide free, round-the-clock bedside care to terminally ill patients whose families are unable to care for them.
CARE got its start at Union College five years ago, and has steadily evolved since then.
It is now offered in partnership with Skidmore College, and open to students from a handful of other schools, such as Siena College.
This summer there are 13 students volunteering at four different residential homes for the dying: the Joan Nicole Prince Home, Gateway House of Peace in Ballston Spa, Mary’s Haven in Saratoga Springs and Hospeace House in Naples.
“These students are seeing the dying process as it happens,” Carol Weisse, the Union College professor who founded CARE, told me.
But it isn’t all gloom and doom.
Far from it.
“There’s joy in these homes,” Weisse said. “For the students to see that, it makes death less frightening.”
Residential homes for the dying — also known as comfort care homes — serve a noble purpose.
The staff and volunteers at these facilities become a kind of surrogate family for residents, doing “everything a family member would do,” said Weisse, who directs Union’s Pre-Health Professions Program and is herself a longtime hospice volunteer.
Everyone deserves good end-of-life care, and residential homes for the dying ensure that people with little in the way of resources can get it. If anything, we need more of these homes — and more volunteers to keep them running.
CARE was initially geared toward students planning careers in health care.
The idea, Weisse told me, was to give undergraduates who might one day treat dying patients a better sense of how to communicate with and care for those with no hope for recovery. These days, CARE is open to any student with an interest in end-of-life care and a willingness to commit to the research project.
The Joan Nicole Prince Home is bright and cheery, with a back porch, meditation garden, living room and kitchen where executive director Amanda Neveu is baking cookies during my visit with Cullen. The home can accommodate two patients at a time, and each have their own bedroom and bathroom.
Neveu told me that residents — neither of whom are able to speak to me — enjoy speaking with younger people.
“It’s a legacy thing,” she said. “They want to share their stories and have them live on.”
Cullen is planning to go to medical school, as is Nurupa Ramkissoon, a 19-year-old Union College junior and Schenectady High School graduate who has spent her summer volunteering at the Joan Nicole Prince Home through the CARE program.
“It’s definitely been a little sad,” Ramkisson said. “The people who come here are very sweet, and you spend so much time with them. … There’s one resident who likes teaching, and she’s teaching us how to cook. It’s making her feel comfortable, like it’s her home.”
Weisse said her goal is to “cultivate a community of compassionate caregivers,” which sounds like a good goal to me.
At some point, every one of us is going to need a compassionate caregiver, and training students to step into this role could have lasting benefits.
Weisse believes she has created a program that could be implemented at residential homes for the dying all over the country.
“My hope and my dream is that this can spread,” she said.
The average life expectancy in the United States is now 78.6 years old, according to the most recent data available from the Center for Disease Control (CDC). That’s almost two times what it was a century ago, when it was just 39.
While some might believe we’re on a path toward immortality, at least for now, death remains the one certain rite of passage that arrives for everyone eventually, and Dr. B.J. Miller believes a reckoning is in order.
“It’s high time to review the very common, boring truth that we’re all going to die,” says Miller, a hospice and palliative care physician whose TED Talk, “What Really Matters at the End of Life?” has been viewed more than one million times. The twist: More open conversations about death and dying may in fact help us all get more meaning out of life.
That’s one takeaway from Miller’s new book, A Beginner’s Guide to the End: Practical Advice for Living Life and Facing Death, co-written with Shoshana Berger. Part manual for practical stuff (like how to deal with the mountain of paperwork when someone passes) and more heart-centric subjects (like personal legacy and grieving for loved ones), the book is intended as a resource for anyone who will experience its subject matter, aka all of us. Prevention spoke with him about why talking about death talk is on the rise in the wider culture—and why it’s something to start discussing sooner than later.
We’re about to be the oldest, frailest population ever.
Americans have reached a pivotal population point. “We are about to be, in actual terms and relative terms, the oldest, frailest population ever,” says Miller. “Everyone’s going to be living with chronic illness, everyone’s going to be dying from chronic illness, in numbers we’ve never seen before.” Mass migration into retirement centers and care facilities isn’t the solution—but a more open, pragmatic dialog about quality of life and personal desires could be, Miller believes.
So, it’s time to develop a “relationship” with death.
There’s a reason talking to a sick loved one or sitting down to write a condolence letter can be so paralyzing.
“We don’t have the right language, or we worry we’ll say something at the wrong time and scare the person we’re talking to,” Miller says. His solution: “Think about it like a series of conversations, not a long-time talk.”
Discussing death in the abstract with someone when their health is good can also help you understand what they may want, and need, down the line; furthermore, it can empower you to articulate those things for yourself. Will those kinds of talks potentially make you anxious? Of course. But the aim is normalization over time—and that comes with a silver lining. “There’s a secret in the hospice world: Most people who do this kind of work and are around this subject a lot will probably tell you that their lives are better for it,” says Miller.
Listen to your loved ones.
Miller has observed that patients know more about what’s going on with their health than anyone else does—or that they may be letting on. A person might hesitate to bring up their thoughts about dying because it sounds like negative thinking. “The patient themselves is languishing, not knowing how to talk about it, or they don’t want to hurt their family’s feelings,” Miller says.
His advice is to “keep an eye out. The moment dad says, ‘I’m not sure about this treatment,’ or [mom] starts talking a lot about God,” give them the opportunity to follow that thread. You can come at the conversation from a philosophical or spiritual angle, focusing on beliefs or fears, but the point is to listen and hear them out. “When they crack the window, dare to enter it.”
It’s okay—actually, essential—to talk about costs.
Miller has seen caregivers lose their jobs, drain their bank accounts, and undermine the financial stability of their own families. “It’s as though bankrupting yourself for a loved one is the currency to show how much you care, even though everyone in the mix knows the person is going to be dying,” he says. But while you can’t place a monetary value on a life, it’s okay to keep money in the conversation. “Invite this variable into the mix in a conversation with your doctor,” says Miller. “It’s not just the medication or the pacemaker. It’s the cost of living with this thing.”
Furthermore, he adds: “Our healthcare system is wired to extend bodily life at all costs, and as our technologies have improved you can prop up a body practically indefinitely,” Miller says. “As patients—as people—you have to upend the medical system. You have to disrupt it and say ‘no thanks.’ Otherwise you’ll land in ICUs with tubes in every orifice and your family has got to decide how to schedule unplugging you.”
Ask yourself: Can I afford to die?
“Our commercial world, our health and benefits—all of it shows this huge design flaw: Dying is not baked into the plan,” says Miller. “We tried to erase it and it can’t be erased.” The result: a framework, from retirement saving plans to health insurance programs, that don’t include the costs associated with death in the picture. Which means: “You need to save more than you think you do—sock away money.”
Bear in mind what’s covered, too. An experimental treatment could be entirely out of pocket, while hospice is highly subsidized. At the end of the day: “It’s about harm reduction. You’ve got two shitty options. But a less shitty option is better, and that could make an important difference.”
Think out of the box about legacy.
“Selfish people do not tend to die happy because they can’t see the world outside themselves,” Miller says. Learning to do that—to care about the world beyond your presence in it—can help us all become kinder people, but it can also help frame thoughts about what you want to leave behind.
Miller is referring to legacy, which might be the best shot we get at immortality. But while we tend to immediately jump to monetary donations, it can be any mark on the world you’ve left behind. Miller tells a story about a man who used to sit out on his front porch and wave at everyone who went by; when he passed, “the whole neighborhood changed, just because that guy wasn’t out there waving.” The bottom line: “You’re going to affect people, no matter what you do.” So try to leave behind something they will remember with a smile.
After Michael Draper was diagnosed with a rare brain disease, his husband retired to take care of him full-time
Terry Wicks, left, and Michael Draper
By DAVID TAFFET
Michael Draper describes the condition he’s been dealing with for seven years as a “designer disease.” His husband, Terry Wicks, said that when they finally received a diagnoses, “the bottom dropped out of our world.”
Draper went almost two years before receiving a diagnosis of MSA — multiple system atrophy — a progressive neurodegenerative brain disorder that results in death.
Wicks has become his full-time caregiver.
MSA is often misdiagnosed as Parkinson’s Disease, but it seems to be more related to other diseases like PSP and Alzheimer’s characterized by a build up of certain proteins in the brain. Wicks explained that with MSA, the proteins needed to transmit signals from one cell to another seem to crumple and block transmission. As that happens, brain cells die.
Functions that are automatic — maintaining body temperature, swallowing, breathing, eliminating waste — stop working. Speech is affected. Muscle coordination deteriorates. The person with MSA becomes unable to take care of himself.
In 2013, the couple was living in California. Draper was an executive with Yahoo. Wicks was an MRI technician.
Wicks remembers asking his husband one day, “Why are you so clumsy lately?”
After a year of a variety of symptoms presenting themselves and several doctors unable to diagnose what was wrong, they went to Stanford for a diagnosis. After almost a year of visits, their doctor told them that she was waiting for one more symptom to appear. When it did, she confirmed MSA.
Symptoms appear when a person is in his or her 50s. Draper was 52 when they first recognized something was wrong. Those manifestations progress for five to 10 years.
New drugs are being tried to halt progression, but Wicks said his husband’s condition was too advanced for the medications to work. And because it takes so long to diagnose, most people have progressed beyond the point where these medications will help.
Four years ago, both men had to stop working. Draper was unable to work any longer so Wicks, who’s seven years older, retired to take care of him.
They decided to move back to Dallas to be closer to family. Their doctor at Stanford told them Dallas was a perfect choice because a colleague of hers had recently opened an MSA clinic at UT Southwestern, so Draper would receive top medical care.
Wicks made a trip by himself and purchased a house in Garland. He said it was the only time in their 29 years together that he had bought a house without his husband.
Wicks describes himself as a planner. So before leaving, he had planned what they needed in a house. He found one in Garland that fit his needs — a 1980s one-story ranch without any stairs or steep inclines that could be outfitted for their needs.
Among the work needed on the house was a complete bathroom redo. They replaced the tub with a walk-in shower fitted with a large tiled seat and an entrance without a step so that a wheelchair can roll in.
Because someone with MSA eventually has trouble turning around, Wicks found something he calls a pivot disk, sort of a lazy susan for people. From his wheelchair, Draper can stand and Wicks rotates him 180 degrees so he can sit in the shower or on the toilet.
Wicks said a person who needs this level of care loses all personal dignity and they’ve worked to keep Draper as independent as possible as long as possible. When he couldn’t brush his own teeth with a regular brush, they got an electric toothbrush.
Draper joked that he could still use a razor as long as his husband didn’t mind seeing him with slash marks all over his face. An electric razor allows him to continue shaving himself for now.
While they still are able to make a trip to the hair salon to get his hair cut, their hairdresser said he’d come to house once he can’t get out any longer.
Until recently, Draper had been using mostly a walker. Lately, he’s less able to make it around the house that way, and he’s begun relying more on his wheelchair.
Over the last few weeks, Wicks said he’s also begun having to use a catheter in order to urinate.
Draper said he feels guilty that he’s putting his husband through this, but Wicks wouldn’t have it any other way.
To help them deal with their situation, they go to support groups. Spouses taking care of their spouses compare, commiserate and share. That’s how he learned about the pivot disk. Those with the rare disorder that may affect only about 15,000 Americans don’t feel as alone when they get together.
Wicks is also careful about caregiver fatigue. Draper’s parents will take care of him for a week while Wicks takes a trip to the Seattle area where the couple lived for a number of years to help decide if after his husband’s death, he wants to move back there.
Draper encouraged his husband to take the trip. This way, he can participate in making future plans even if he won’t share them himself. He wants to know his husband will be all right and will return to having a life beyond caregiving.
Wicks said he still is able to leave Draper alone for an hour to run out to the store for groceries. As Draper’s condition deteriorates, Wicks said he’ll have to hire someone to come into the house to relieve him so he can do errands.
Caregiving that includes everything from personal care to doing all of the housework is a full-time job, Wicks explained.
“Unless you’ve done it, you have no idea how much it entails,” he said.
In addition to the physical labor, caregiving involves stress. Wicks described what he’s going through as anticipatory grief. Most people don’t grieve until their spouse is gone, and Draper has already outlived original projections for his life expectancy with MSA.
Wicks doesn’t know if the grieving he’s going through now — imagining what life will be like without his husband — will facilitate the grief he’ll feel after his husband’s death or if he’ll experience the loss he’s expecting all over again.
But that anticipatory grief also propels him to make the best life he can for both of them. Draper still has his sense of humor even as communicating grows more difficult. But as they look at each other and tell their story wishing it was headed toward a different ending, there’s a contentment and bliss in their just being together.
With respect to end-of-life care, physicians’ likelihood of dying at home is similar to that of nonphysician patients, a Canadian study suggests.
“Overall, they did not consistently opt for less-aggressive care but instead used both intensive and palliative care more than nonphysicians,” Hannah Wunsch, MD, from the University of Toronto, Canada, and colleagues write in an article published online July 24 in JAMA Network Open.
Intensive end-of-life treatment is common in North America, often going against patients’ previously reported preferences. Previous studies have suggested that physicians in the United States are somewhat less likely to die in the hospital than other patients, suggesting they may be better able to match their care with their preferences.
To see if that pattern held true in a system with universal healthcare, Wunsch and colleagues compared the intensity of treatment received by physician and nonphysician patients at the end of life in Ontario, Canada.
“The primary outcome was location of death, with the hypothesis that physicians are more likely to receive less-intensive end-of-life care,” the authors write.
The researchers analyzed medical and death records of 2507 physicians and 7513 nonphysicians who died between 2004 and 2015.
They found that physicians were no more likely to die at home than nonphysicians (42.8% vs 39%; adjusted relative risk [aRR], 1.04; 95% confidence interval [CI], 0.99 – 1.09). However, physicians were more likely to die in an intensive care unit (ICU) (11.9% vs 10%; aRR, 1.22; 95% CI, 1.08 – 1.39).
The data also showed that, in the 6 months before death, physicians were less likely to visit an emergency department (73% vs 78.4%; aRR, 0.96; 95% CI, 0.94 – 0.98), but more likely to be admitted to an ICU (20.8% vs 19.1%; aRR, 1.14; 95% CI, 1.05 – 1.24), and to receive palliative care (52.9% vs 47.4%; aRR, 1.18; 95% CI, 1.13 – 1.23).
However, a subgroup analysis of patients with chronic conditions showed that physicians (n = 1375) were more likely to die at home than nonphysicians (n = 4117) (35.2% vs 30.7%; aRR, 1.12; 95% CI, 1.04 – 1.22). Among those with cancer in this subgroup, physicians were also more likely to die at home (37.6% vs 28.6%; aRR, 1.30; 95% CI, 1.13 – 1.50), and to receive chemotherapy in the last 6 months of life (37.9% vs 29.8%; aRR, 1.28; 95% CI, 1.13 – 1.46).
In an interview with Medscape Medical News, study coauthor Robert A. Fowler, MDCM, MS(Epi), also from the University of Toronto, was struck by how his group’s findings differed from the US studies.
“We wondered whether this might relate to differences in payment systems for healthcare services in the United States, in comparison to Canada where we have a theoretically universal healthcare system for in-hospital care, yet often have more limited options for home-based and palliative care at end of life.”
Overall, Fowler expressed surprise at the findings of both the US and Canadian studies — “chiefly, that many elements of end-of-life care are, despite some differences, remarkably similar among physicians and the general population.”
This was different from his group’s original hypothesis that physicians would opt for much less inpatient care.
“It was interesting that we did see that physicians were both more likely to receive treatment in an ICU, known for its use of technology-laden care,” he added, “and also more likely to receive palliative care at the end of life.”
According to Fowler, this offers a more nuanced perspective of what physicians may perceive to be optimal care at the end of life, as opposed to a simplistic notion of ‘more’ or ‘less’ being better: “Sometimes, more aggressive care is warranted,” he said, “yet, at other times, focusing more squarely on comfort is best.”
Mary Klein, center, speaks at a news conference in Washington on April 5, 2018, to urge D.C. officials to educate doctors about the city’s “death with dignity” law.
By Jon Meacham
Jon Meacham is the author of “The Soul of America: The Battle for Our Better Angels.”
Tuesday was to be the day — in the morning, because everything was taken care of. The goodbyes had been said, the tears shed, the coffin handmade. In the spring of 2018, Dick Shannon, a former Silicon Valley engineer with untreatable cancer, took advantage of California’s “death with dignity” law to end his own life once all other medical possibilities had been exhausted.
“My observation about the way people die, at least in America, is they . . . are not allowed the opportunity to be part of the process,” Shannon explained. “For my way of thinking, the part that bothers me just immensely is not being allowed to be part of that process. It’s my death. Go with what you believe, but don’t tell me what I have to do.” Discussing the ultimate decision with his doctor, Shannon remarked, “It’s hard to fathom. I go to sleep and that’s the end of it. I’ll never know anything different.” He paused, then said simply: “Okay.”
When the day came, Shannon was ready. The end-of-life medical cocktail was mixed in a silver stainless steel cup, and he drank it in front of his loving and tearful family. “I’ve accepted the fact that I’m dying,” he’d said earlier. “There’s nothing I can do to stop it. Planning the final days of my life gives me a sense of participation and satisfaction.” As he prepared to slip away, he told his family, “Just know that I love you — each and every one of you.”
America is becoming ever more like itself when it comes to death. From Walden Pond to Huck Finn’s lighting out for the territory, we’re a nation of individualists, shaped and suffused by self-reliance and a stubborn allegiance to the live-free-or-die motto of the Revolutionary era. With this twist: Baby boomers and their successor generations are insisting on being free to take control of death itself. Innovation, creativity and customization — the hallmarks of our time, an age in which we can run much of our lives from our mobile phones — are now transforming both how we die and the mechanics of remembrance that come afterward.
The coming revolution in death — and Dick Shannon’s story — is laid out with uncommon wisdom in a powerful, new HBO documentary, “Alternate Endings,” which debuts Aug. 14. Only eight states and the District of Columbia have death-with-dignity laws, but three of those states — Hawaii, Maine and New Jersey — have put their statutes on the books within the past year. And 18 other states considered such laws in the 2019 legislative season.
The movement has not attracted the same attention it once did; in the 1990s, Jack “Dr. Death” Kevorkian, the right-to-die advocate, drew considerable public alarm. As the documentary by Perri Peltz and Matthew O’Neill makes clear, the conversation has entered a new and compelling phase now that Americans are thinking about death as something as disintermediated as commuting, dating and shopping.
The United States has a long history of rethinking the rituals of death. Embalming became part of the popular understanding and tradition of death during the Civil War; the task then was to preserve the bodies of dead soldiers so their families could see them one final time. Abraham Lincoln may have done the most to raise the profile of embalming when he chose first to embalm his 11-year-old son and then when his own corpse was embalmed for the long train ride home to Springfield, Ill., after his assassination.
Now the death industry in the United States has evolved with the culture. For many, corporate consolidation has reshaped a funeral home industry, which was once made up almost entirely of local, family-owned companies. (And which, as Jessica Mitford wrote in her 1963 book “The American Way of Death,” unctuously gouged grieving families.) The Internet has disrupted the casket industry with Walmart and others selling directly to families. As “Alternate Endings” reports, there are now green burials (including using a loved one’s ashes to help restore coral reefs), space burials and even drive-through, open-casket viewings.
Once the great gatekeeper of life and death, organized religion, too, is losing its sway. In an era in which friends routinely ordain themselves on the Internet to preside at weddings, the rising numbers of Americans who are “unaffiliated” with any particular faith mean that institutions that once gave shape to life and meaning to death are being gradually supplanted family to family.
The issues raised by Dick Shannon’s story are the most profound. Many religious authorities — notably the Roman Catholic Church — oppose euthanasia (Greek for a “good death”). Such teachings face a generational head wind as more people (and states) move from deferring to institutions to simply making their own decisions. The questions involved are intricate and complex and painful — but it is plain to see that we are witnessing another rite of passage undergoing an irrevocable disruption.
When the Shannons held a “living wake” for friends to say goodbye to Dick, the family hung a banner on the wall: “Life is what you celebrate. All of it. Even its end.” Before passing, Shannon said, “I want it to be on my terms.” Given that death comes for us all, so, too, will many of us have to confront the agonizing decision that he faced with grace.
Most Americans die in hospitals, but acute care settings are by default focused on saving lives and therefore struggle to deal with death as something other than the unfortunate outcome of having no interventions left to try. An expert in end-of-life care notes that death is an essential part of life for patients and their families and suggests several steps physicians can take to make death a “healthy” experience.
For starters, Chapple said, one should acknowledge that the aim of acute care settings is to rescue patients, to avoid death at all costs.
“If there is an intervention to try, that’s what we’re going to do,” Chapple said, noting that this urge is reinforced by health care payment mechanisms, as well as by family members’ anguish. “So, it’s very difficult to move in a different direction. It’s like a train that you can’t jump off of.”
Trying everything, however, can undermine our cultural and clinical capacity to acknowledge the importance of dying, Chapple said. She suggested taking the following steps to reinforce the concept of dying in a healthy way.
Focus on patient safety and autonomy. “I worry that patients are overmedicated or undermedicated, that we’re not reacting to what’s really happening to the patient,” Chapple said. “Healthy dying is when patients themselves get to choose the agenda and get to take their own time—as long as they’re not suffering at all, or they appear not to be suffering—and we all just take their timetable and let it happen.”
Acknowledge death as a part of life. This begins with making the most of what Chapple called the “critical present” by suggesting that family members take time to reflect on the patient’s life. “It’s sort of antithetical to the way acute care is set up, which is doing all the time, rather than being, rather than existing and noticing the existential significance of where we are right at this moment,” she said.
Reset loved ones’ expectations. In critical care, Chapple often tells families, “This person has never died before, and this is our chance to make it the best dying they can possibly have.” She suggested preparing family members for what might happen logistically, such as transferring the patient to a step-down unit, and noting that the active dying phase can last several days.
Encourage family members to talk to patients. Hearing is thought to be one of the last senses to go in dying patients, so it may help to share memories. “Families may not talk to each other because they think the family knows all the stories,” she said, so members of the care team can help initiate this by asking about significant events in the patient’s life.
Note the importance of religious rituals. Ceremonies, prayers and songs can help make this time meaningful too.
Suggest loved ones say goodbye in their own ways. Let family members know the following, Chapple suggested: “If you want to … say to the person something that you’ve always wanted to say and never had the opportunity or you certainly want them to know before they die, this is the time to do that.”
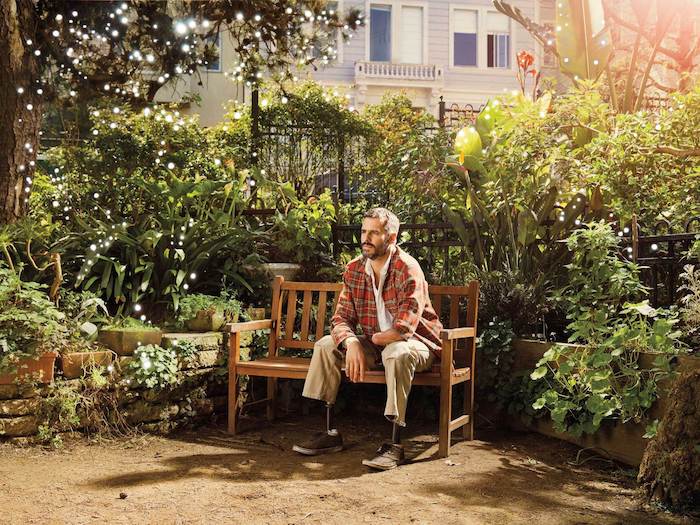
Hospice and palliative care physician Bruce (B.J.) Miller has made it his mission to help people “live well in the face of death.”
A hospice and palliative care physician at the University of California Helen Diller Family Comprehensive Cancer Center and former executive director of the Zen Hospice Project, Miller speaks nationally about end-of-life care, including the benefits of hospice and palliative care, and was featured in the Netflix documentary short film, End Game.
His new book, A Beginner’s Guide to the End: Practical Advice for Living Life and Facing Death, co-authored with journalist Shoshana Berger, is designed to educate the public about the options and obstacles that patients and families encounter at the end of life.
Miller’s has experienced palliative medicine both as a clinician and as a patient. An accident during his college years resulted in the amputation of one arm below the elbow and both legs below the knees.
“Part of the reason that I wound up becoming a doctor is that I came close to death in my own life, earlier than expected and in a dramatic enough way that I had little choice but to sit up and take notice,” Miller wrote in the book.
Miller spoke with Hospice News about perceptions of death in our society and its influence on patients’ choices, including hospice election, how patients should be cared for at the end of life, as well as the policy, practical and financial considerations that can impact that care.
“Hospice is a business too, and is affected by the same mundane staffing issues as any other: Illness, vacations, car trouble. The difference here is that a long wait for a bad latte will never be comparable to a late nursing visit when you are in desperate need for help,” Miller and Berger wrote in the book. “The hospice system is a part of our stressed health care system and that means it is stressed too. Burnout and turnover are significant problems across the industry; meanwhile, training programs struggle to impart the sort of knowledge and grizzled experience that good patient care requires.”
Regarding your book, A Beginner’s Guide to the End, what factors led you to decide that a resource like this was needed?
Being a clinician working in the hospice and palliative care space, I see patient after patient and family after family languish and suffer due to lack of information. This is certainly true anywhere in health care, but especially in our field because our explicit mission is to ease suffering. And this has proven very tricky. Most people don’t know what palliative care is. Many people know what hospice is, but they have so many misunderstandings of it.
I felt there was a need to get a general book out there to cover the waterfront, the hope being that essentially that we could raise the floor. We are not going to blow off the ceiling, but at least we can raise the floor and level the playing field so most everybody has some access to sound, up-to-date information. That was the impulse.
At several points in the book it’s mentioned that there is a kind of taboo around the topic of death. How do you think that influences people’s choices at the end of life, including electing hospice?
Our language gives us away. We have this old-fashioned notion that life is a fight against death, as though death were a foreign invader instead of a natural thing that is completely entwined with life.
We talk about death as a failure. In medicine we say, “He failed treatment.” That they “lost the battle,” and so forth. So we find all these exotic ways to keep the subject at a distance, and in daily life it has become easier and easier to become distracted from this. And it means that so many people wait way too long to elect hospice. And if they do enter hospice at all, it’s often in the final days where there is not much time to do all that we can to bring life to a close and provide some comfort.
Even beyond the election of hospice I think if we built awareness of our mortality into our daily lives, my guess is that we’d be much kinder to ourselves and to each other and much more appreciative of the life we have while we have it.
How do you see the hospice and palliative landscape changing? How you think the space could be different five years from now?
My hope would be that medical training in general absorbs the principles of hospice and palliative medicine and drives this kind of care earlier into the picture. Just about any clinician of any stripe should have some kind of basic facility with these concepts — eventually 100% of their patients are going to die.
My hope is that our workforce grows to meet the rising demand, and that payment gets worked out so people are incentivized to pursue careers in this important field. From a policy standpoint, hopefully there will be some legislation passed promoting training for hospice and palliative care.
I do think we in the field also really have to take quality seriously. We used to be able to just absorb the idea — it was just a fact that hospice in particular provided superior quality care as a medical model — and that’s still largely true. But we have to be careful, it’s not just about getting more people into the field; we have to keep our eyes on quality.
Do you think that current payment models for hospice, in particular the Medicare Hospice Benefit, are copacetic with the mission of providing multidisciplinary person-centered care in accordance with patients’ goals and wishes for end of life?
I think in general the hospice benefit does a very good job. I think its sticking points are the requirement that patients have six months or less to live and the idea of all the things that you can’t do while you are on hospice.
Those things made sense in 1982, but they don’t make much sense anymore. For example there are a ton of treatments that might be considered life extending that are actually palliative in nature. I see a lot of patients who are fully aware of all these trade offs and forestall their hospice election because they want access to certain treatments that could maybe help them live longer but also could make them feel better.
So those two sticking points are ripe to be revisited. Otherwise I think the hospice benefit is very sound, but I wonder how much longer the hospice benefit will look like the hospice benefit of today.
How do you feel about a possible Medicare Advantage carve-in for hospice?
I am not a policy expert, and there may be some counter arguments. but I wonder what the unintended consequences of that would be.
Right now Medicare sets the guidelines, and therefore there is a centralized power and policy hub. In sending the hospice benefit to private companies, will Medicare Advantage plans be allowed to dictate their own hospice benefit? If so, I have to imagine quality would go down due to cost-cutting measures which ultimately would also be quality-cutting measures.
You have spoken about how the health care system has diseases rather than people at its center. Do you think that is starting to change and how can the health care community accelerate that change?
I believe it’s starting to change in that the phrase “patient-centered care” is pretty well known and recognized, and I don’t hear anyone arguing against patient-centered care. So I think there’s an opening dialogue around it.
But I also watch some of my medical colleagues roll their eyes at it, and for good reason: Our population, health, and disease and treatments are so complex that it’s practically impossible for patients to make an informed decision, because we haven’t done a very good job of educating them. So it’s unrealistic to say that we can do whatever the patient wants.
What it is realistic is a shared decision-making model in which your clinician is your advocate and together you are working on a plan that’s realistic for the options in front of you, and together you make decisions. I think that’s the golden chalice we are trying to find.
A good example is that if you were to follow patient satisfaction surveys — if those were the gold standard of a patient-centered system — data show that patients prefer doctors who prescribe more medications because that feels like their doctor cares, but more medications is not always the best clinical choice.
That’s a case in point where it’s much more complicated than the satisfaction of the patient or the family, so I think the refinement here is to elevate the patient’s voice in the decision-making process and do the listening on our side as clinicians and encourage patients to speak up for what’s important to them, and together move forward. That is how things should work.
One of the most pervasive barriers to bringing patients into palliative care and hospice is awareness. Most people simply don’t know what these things are. What can hospice and palliative care providers do to move the needle on that issue?
No one seems to understand the difference between hospice and palliative care, and I wonder what policy could come along to help smooth out these false divides. I keep waiting for someone to organize a kind of mass public service announcement, explaining to the public what the solutions are and explaining the field.
As a clinician I am explaining the distinctions to people all the time, and I struggle to do it in a succinct manner; so I think that you need some real communications expertise. It’s a very tricky and complicated communications challenge to distinguish between these concepts in a way that is understandable and relatable, especially when for a lot of people it’s inborn to want to look away.
I would love to see some sort of mass public communication effort. That would go very far even among the health care community. Many of my doctor and nurse colleagues themselves couldn’t tell you the difference between hospice and palliative care. That is very common, so we have a massive communications problem that will take a multimillion dollar effort to get past.
You have spoken about the need to bring intention and creativity into dying. Where does hospice fit into that?
Dying is way bigger than a medical event. Hospice begins with a conversation about what is important to the patient and what is not important to them, and just the nature of that conversation helps people to live with intention.
You help and encourage them to think through what is important, what can they live with, what can they live with, coming to terms with the finitude of their time, and then you can work from there and to some level design your days. Hospice facilitates those conversations all the time.
I think the creative spark is a way of life, a way of thinking in which daily life is a creative act, including at the end of life. We are all improvising all the time, bobbing and weaving, checking our plans versus the reality on the ground. Creativity often flows from reaction to limitations, and this is our limitation: We don’t have endless time.