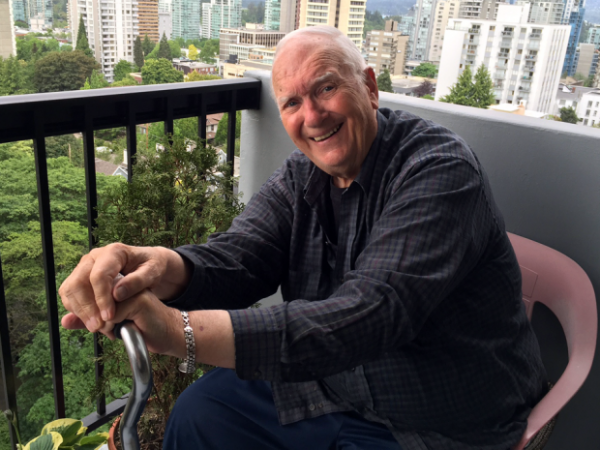
Ian Shearer’s daughter, Jan, says she was surprised by his request for doctor-assisted death, but she realized that he was dying “a slow, painful” death.
Ian Shearer had had enough of the pain and wanted a quick, peaceful end, his life marred by multiple afflictions.
But the Vancouver man’s family says his last day alive became an excruciating ordeal after the Catholic-run hospital caring for him rebuffed his request for a doctor-assisted death, forcing him to transfer to another hospital.
The combination of the cross-town trip and inadequate pain control left Shearer, 87, in agony through most of his final hours, says daughter Jan Lackie.
“To hear him crying out, screaming … was just horrible,” said Lackie, breaking into tears as she recalled the day in late August. “That’s what keeps me from sleeping at night … I don’t want any other person to go through what he did.”
Shearer’s experience at St. Paul’s Hospital highlights one of the thorniest issues concerning assisted death: the decision of most faith-based — but taxpayer-funded — health-care facilities to play no part in a practice made legal by the Supreme Court of Canada and federal legislation.
Ian Shearer and daughter Jan Lackie.
Lackie said the suffering her father endured shows why it is important that church-governed facilities, including dozens of hospitals, nursing homes and hospices across Canada, be required to allow assisted deaths within their walls.
“We have nine judges who said ‘Yes’ to medical assistance in dying,” she said. “I don’t understand how the Vatican has so much power, even here in Canada.”
But the bill that implemented the Supreme Court’s ruling in June does not oblige any institution to permit the practice.
And Catholic health organizations say their objection to assisted death flows from deeply held beliefs, while noting there are numerous other, less contentious procedures available at some facilities but not others.
“Life is sacred and the dignity of the person is important,” said Michael Shea, president of the Catholic Health Alliance of Canada. “These organizations neither prolong dying nor hasten death, and that’s a pretty fundamental value for them.”
Shaf Hussain, a spokesman for Providence Health Care, which operates St. Paul’s, said he could not comment on Shearer’s case specifically. But under a policy finalized this summer, he said, the Catholic organization arranges to transfer patients as comfortably as possible when they express a desire for assisted death.
Even the medical assessment required under the law and the signing of consent forms must take place outside Providence properties.
“All feedback we take very seriously,” said Hussain. “We’ll be working with our partners in the health care system to ensure the patients’ needs do come first … and to minimize the discomfort and pain.”
Shearer, a retired accountant originally from Calgary, suffered from spinal stenosis – a narrowing of the spine that can put pressure on the spinal cord – heart disease, kidney failure and, toward the end, sepsis, said his daughter.
He spent about three weeks at St. Paul’s, the closest hospital to where he lived in Vancouver, said the Calgary woman. The spinal condition was so debilitating, “just to touch him, he would scream.”
Lackie said she was surprised by his request, but supportive, realizing that her father was dying “a slow, painful” death.
It would be days, however, before Shearer was transferred to Vancouver General, and on the designated date – Aug. 29 – the ambulance arrived more than three hours late, said the daughter.
The man’s dose of the pain drug fentanyl had been reduced to ensure he was lucid enough to consent to the assisted death, but as time wore on the pain grew worse, and there was a shortage of the narcotic on his ward, she said.
Already in agony, Shearer cried out desperately with each bump during the four-kilometre ambulance ride, said Lackie.
He eventually received the series of injections ending his life at Vancouver General, a “beautiful,” peaceful death, she said.
Jan Lackie holds father Ian Shearer’s hand on his last day, when a Catholic hospital’s refusal to consider his request for assisted death forced a painful transfer to another hospital.
Dr. Ellen Wiebe, a B.C. physician who has carried out several assisted deaths, provided the service for Shearer, one of three patients from St. Paul’s she has seen for the same reason.
To get around the hospital’s ban on patients even being assessed there, she said she makes “flower visits:” masquerading as a friend bringing a bouquet.
Assisted-death bans can not only lead to suffering during the transfer itself, but effectively deny patients the right in areas where there is no alternative to the faith-based institution, said Shanaaz Gokool, head of the group Dying with Dignity.
“This is going to be a real issue, and it’s going to be a real issue across the country.”
The facilities are causing vulnerable patients suffering because of a decision that benefits only the institution, argued Juliet Guichon, a bioethicist at the University of Calgary.
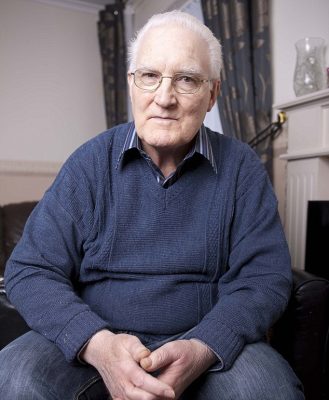
[A]fter almost 20 years of living with a pacemaker, Nina Adamowicz decided she no longer wanted the device that was keeping her alive.
It had been implanted in 1996, and for the first decade it ‘improved’ her life and symptoms — she had a form of hereditary heart disease.
The pacemaker sent regular electrical pulses to keep her heart beating steadily, and she was grateful for ‘being given extra time’, she later recalled.
However, she then had a heart attack and her health declined so that by 2014, her heart was working at just 10 per cent of its capacity.
Last year, Polish-born Ms Adamowicz, 71, who had lived in the UK for more than 30 years, revealed she wanted the pacemaker turned off, even though she knew it would lead to her death.
After almost 20 years of living with a pacemaker, Nina Adamowicz decided she no longer wanted the device that was keeping her alive
It was like being ‘in line for execution and being told “not yet”, she said in an interview for BBC Radio 4.
‘It’s not about “I want to die”, I’m dying,’ she added.
After a series of medical examinations and psychological tests to determine whether she understood what switching off her pacemaker would mean, doctors agreed, and last October Ms Adamowicz went into a local hospice with her family for the pacemaker to be turned off – a procedure that took 20 minutes.
She described her body as feeling heavy and she felt a little nauseated – but she also felt at peace, her family told the BBC.
She slept through the night, returned home in the morning and died that night.
Her case – thought to be the first of its kind in the UK – raises profound ethical issues about when it is right to turn off someone’s pacemaker, or indeed withdraw other medical treatment such as dialysis for kidney failure, if that’s what they want.
In fact the law itself is very clear on this point, according to Miriam Johnson, professor of palliative medicine at Hull York Medical School.
‘A mentally competent adult has the right to refuse medical treatment, whether it is turning off a pacemaker or stopping dialysis, even if that treatment is prolonging their life and withdrawing it will lead to their death,’ she says.
‘By turning off the device, the disease or illness will kill the person, not the doctor.’
However, some doctors feel it’s uncomfortably close to euthanasia — the difference is that euthanasia involves overriding Nature.
Some doctors feel that turning off a pacemaker is uncomfortably close to euthanasia — the difference is that euthanasia involves overriding Nature
‘The difficulty with a case like this is that when a patient is dependent on a pacemaker, there is a direct connection between withdrawing the treatment and them dying within the next few hours,’ adds Professor Johnson, explaining that doctors’ role after all is to protect the vulnerable.
Around 35,000 patients in the UK have a pacemaker fitted each year. The device’s role is to keep the heart beating steadily – it gives it a boost by delivering electrical impulses so that the heart contracts and produces a heartbeat.
The computerised match-box sized device is implanted just under the skin, usually just below the left shoulder and electrical leads are then fed down a vein into the heart.
‘In a significant number of pacemaker cases if you suddenly took the pacemaker away, the heart would stop beating,’ explains Dr Adam Fitzpatrick, a consultant cardiologist and electrophysiologist at Manchester Royal Infirmary and Alexandra Hospital, Cheadle.
He adds: ‘It is very unusual for a patient to ask for their pacemaker to be turned off.’
Even if the patient is dying, a pacemaker does not need to be switched off, says the British Heart Foundation.
‘A pacemaker’s purpose is not to restart the heart and it won’t cause discomfort to someone who’s dying,’ said a spokesperson for the British Heart Foundation
‘Its purpose is not to restart the heart and it won’t cause discomfort to someone who’s dying,’ said a spokesperson.
But the picture is slightly different with other heart devices such as Implantable cardioverter defibrillators (ICDs) which are used to correct an abnormal heart rhythm rather than helping the heart beat steadily.
These devices, implanted in around 9,000 people in the UK every year, kick in when an abnormal heart rhythm occurs which can cause sudden cardiac arrest (where the heart stops beating).
Implanted under the collarbone as a pacemaker is, they work by firing a small electric shock into the heart to kick-start it (some pacemakers have this function too).
This might happen once every few months or not even for years.
However, this can be both painful and traumatic, especially at the end of life, and can lead to a prolonged and distressing death by continuing to give electric shocks.
In one particularly upsetting case reported in a US medical journal, a man suffered 33 shocks as he lay dying in his wife’s arms — the ICD ‘got so hot that it burned through his skin’, his wife later reported.
Implantable cardioverter defibrillators work a bit differently from a pacemaker, as they are used to correct abnormal heart rhythm with an electrical current
‘Dying patients often have multi-organ failure which can cause metabolic and chemical changes that may trigger arrhythmias, faulty heart beats and in turn activate the ICD,’ explains Dr James Beattie, a consultant cardiologist at the Heart of England NHS Foundation Trust, Birmingham.
‘If the device goes off when the patient is conscious, the shock is like a blow to the chest, causing discomfort and distress. It may also fire repeatedly.
‘This may result in a distressing death for the patient and distress for the families.’
Yet despite this suffering, 60 per cent of hospice patients do not have their implant deactivated before death, according to U.S. research published in the Annals of Internal Medicine.
Furthermore, a 2011 survey by the National Council for Palliative Care suggested that only 40 per cent of UK hospices have access to the technology to deactivate the device urgently, potentially risking an undignified and painful death in hundreds of patients should they suddenly deteriorate.
Switching off the device involves holding a magnet over it, temporarily closing a magnetic switch incorporated in it.
To turn it off permanently the device has to then be reprogrammed remotely using a ‘wand’ attached to a computer.
Despite the risk of suffering, 60 per cent of hospice patients do not have their implant deactivated before death, according to U.S. research
Medical professionals and families face a number of dilemmas when deciding whether to turn off an ICD.
One is the difficulty in accurately predicting when the patient is reaching the end of their life.
‘Determining this isn’t always clear, especially with a condition such as heart failure when patients may have survived crises over many years,’ explains Professor Johnson.
‘This can be complicated further if the patient is suffering from dementia and unable to make decisions about their care.’
There is also an understandable reluctance by patients and their families to take away anything that can prolong life.
‘Patients and their families frequently think of the device as entirely beneficial,’ says Professor Johnson.
‘There is also often unrealistic expectation about what doctors are able to do to keep people alive.’
Many doctors shy away from these conversations, too. A 2008 report from the National Audit Office found a significant lack of confidence in handling end-of-life care across all medical specialities — with cardiologists topping the league.
‘Given they are trained to save lives, talking about death can be seen as professional defeat,’ says Dr Beattie.
But if patients and doctors don’t have that conversation ‘we’re storing up trouble because decisions then have to be made at times of crisis and without planning’, says Simon Chapman, of the National Council for Palliative Care.
New guidance for patients and medical staff to guide them through the ethical minefield of withdrawing heart devices was published earlier this year in the journal Heart.
Just how difficult making such decision can be was dramatically highlighted in the case of Fred Emery.
When his health suddenly went downhill six years ago, doctors recommended turning off the defibrillator that had been keeping him alive for the past 14 months.
When Fred Emery’s health suddenly went downhill six years ago, doctors recommended turning off the defibrillator that had been keeping him alive for the past 14 months
The 73-year-old former manual worker from Kings Langley, Hertfordshire, had had the matchbox-sized device implanted in his chest following a 26-year battle with heart disease.
During that time he’d had two heart attacks, and had already undergone two triple heart bypass operations as well as having several stents (tiny metal tubes) inserted to prevent his arteries blocking.
However, Fred then developed heart failure and ventricular tachycardia — a potentially fatal heart rhythm
Having a defibrillator not only helped with the heart failure, but also any sudden cardiac arrest triggered by the faulty heart rhythm.
But Fred’s condition deteriorated and doctors suggested that as he was nearing the end of his life, it was time to turn off this life-line — to spare him and his family the ordeal of it repeatedly jolting his heart back to life when his body had reached the natural moment of death.
However, despite doctors’ predictions, Fred pulled through and later had the defibrillator reactivated, and it went on to save his life several times before his death this year. His family was angry that doctors had written him off before his time.
Despite doctors’ predictions, Fred pulled through and later had the defibrillator reactivated, and it went on to save his life several times before his death this year
‘It was awful when they told him to turn it off,’ his wife Shirley, 70, told Good Health. ‘Fred was taken ill at 4pm, and by the next morning the defibrillator was turned off. It was too soon to make that decision — he wasn’t himself and was under pressure to switch it off.
‘After it was reactivated, Fred had six more years. Without the ICD we would have lost him several years ago.
‘He kept it on until a week before his death. By then his heart was working at 15 per cent, he was in a hospice and there was no coming back so we made a decision to turn it off to give him some dignity at the end. He knew what was happening.
Marjorie Severance had lived 91 years, five months, and two weeks when, if you believe such things, she decided she could let herself die.
She had completed all of her funeral and memorial service plans. Her finances were set. “Gramma Marj,” as she was known to her many grandchildren and great-grandchildren, spent the last weeks of her life sprucing up her jewelry collection and choosing beneficiaries.
Her granddaughter, Jan Schultz, who was helping with the jewelry, was dragging her feet getting the two last rings fixed.
“I had a feeling that as soon as this was done, she’d be done,” Schultz recalled.
When a great-grandson visited her for supper at her assisted-living facility in Madison, Wis., earlier this month, Gramma Marj ushered him out early. The family laughed about it, but the next day she barely woke.
Schultz called Gramma Marj’s son in Texas and told him to get there fast. Then she told her grandmother that her son was on his way and would arrive the following day. Gramma Marj’s eyes stayed closed; she was alive but largely unresponsive.
The next day, her son arrived. She opened her eyes for him. And then, not long after, in the solitude of her room, Marjorie Severance passed away.
The question of whether Severance somehow prolonged her life will forever remain a mystery. But it is hardly a mystery that stands on its own.
Hospice and palliative care clinicians routinely see cases in which people who are nearing life’s end seem to will themselves to hold on until a certain point, after which time they let go.
And while some people hold on long enough to see a loved one, others seem to do the opposite, clinging to life until they are left alone.
Dr. Toby Campbell, an oncologist and palliative care specialist at the University of Wisconsin, Madison, said patients tend not to have a lot of control at the very end of their lives. But that doesn’t mean they don’t have any.
“People in end-of-life care wouldn’t bat an eye if you asked if they think people can, to a certain degree, control those final moments,” Campbell said. “We’d all say, ‘Well, yeah. Sure.’ But it’s inexplicable.”
If these well-timed deaths are anything but coincidental, medical scientists appear unlikely to be able to provide an explanation anytime soon. A body of scientific literature called “the will to live near death” explores questions at the fringe of this topic, but the research focuses more squarely on how one’s will to live might affect life expectancy.
When it comes to extending one’s life by hours, seemingly through sheer will, Campbell believes the dying “probably have some kind of hormonal stimulus that’s just a driver to keep them going. Then, when whatever event they were waiting for happens, the stimulus goes away, and there must be some kind of relaxing into it that then allows them to die.”
In one memorable experience, Campbell recalled three sisters who had gathered in the hospital room of their elderly mother after she’d suffered a stroke. One sister lived nearby and the others joined from out of town, holding vigil for several days.
The mother was unresponsive, and though her prognosis was grim, she wasn’t actively dying. “They were having really a lovely time bonding together, but then life was kind of moving on and in truth they were ready for mom to die,” Campbell said.
One morning, he told them that their mother might actually want to die — but not with them present. Some people deem the dying process too personal to share, while others don’t want to expose family members to the trauma of watching them go.
The sisters, Campbell said, ” immediately grabbed onto the idea, and right then, they said, ‘Mom, we’re going out for breakfast. We’ll be gone for two or three hours, and then we’re going to come back and see you. So if you need to be alone to do this, now’s a good time.’”
Campbell left the room. The sisters left soon after. Their mother died while they were gone.
“They were sad, of course,” he said. “But they felt like they had done right by her.”
Jan Schultz felt that way too. Her grandmother had worked her way from bank teller to vice president over a 40-year career in finance. She was a proud matriarch, both loving and deeply beloved. Schultz said it would have been out of character for Gramma Marj to die before her son arrived, and it would have been equally out of character for her to burden him or anyone else with the sight of her death.
So in retrospect, it was little surprise that when Gramma Marj’s son arrived, her condition noticeably changed.
“I could almost see a sense of calmness over her when he arrived,” Schultz said.
Gramma Marj opened her eyes for him. She heard him leave. And then, after he was gone, her heart went quiet.
When a loved one is critically ill, hearing that it’s time for hospice care can be devastating news. On top of the emotional upheaval of coping with a terminal illness, you may be unsure what hospice care really is — and believe it’s just an indication your loved one will likely pass away.
Yet the time your loved one spends in hospice care doesn’t have to be sad — for anyone. In fact, says Toni Norman, the senior director of hospice operations for Brookdale Senior Living, hospice can be a deeply rewarding time of great comfort for patients and their families.
“Hospice care is not about waiting for someone to die, and that’s unfortunately a very common misconception,” Norman says. “The goal of hospice is to provide to a patient, who has a life-limiting illness, the physical comfort and medical care they need to stay in their home for as long as possible, while at the same time supporting their caregivers. The hospice team helps families by educating, supporting and identifying any needs they have, ranging from chaplain support to finding mortuaries and veteran benefits.”
The decision to begin hospice care is a communal one, with the patient, caregivers, loved ones and medical professionals contributing to the dialogue. “A terminal diagnosis from a doctor usually begins the process of seeking hospice care,” Norman says. “Also, as a family member’s health begins to decline due to illness, conversations about end-of-life care are proactive and compassionate.”
Brookdale Senior Living’s hospice care providers often encounter common misconceptions about hospice care. Norman offers the truth behind some mistaken beliefs:
* Hospice is for the last few weeks of life. The hospice Medicare benefit is for the last six months, if the disease follows its normal course.“Most people who enter hospice have done so because they’ve received a diagnosis of a life-limiting illness,” Norman says. “But people who enter hospice often live longer, and with a better quality of life, than terminally ill people who do not go into hospice. Many are even able to come off hospice service if their condition improves.”
* Hospice means giving up. Hospice is actually a commitment to a high level of care for a loved one. “It means making them as comfortable and safe as possible so they may enjoy time with their loved ones for as long as possible,” Norman says.
* Patients are heavily medicated. Patients receive medication under strict physician guidelines, and caregivers closely monitor comfort care protocols so each patient’s pain and symptoms are uniquely managed.
* Hospice patients can no longer see their doctors. Patients can continue to see any of their previous doctors. Rather than taking anything away, hospice adds a layer of medical support.
* Hospice care ends when a patient dies. Because hospice cares for the patient’s caregivers and loved ones as well as the patient, hospice team members continue their support for 13 months after the patient passes away. The hospice team provides grief support for the families and will continue to work with them to address any lingering questions, and to help identify their needs.
“The hospice team is comprised of the assigned physician and nurses to provide the direct medical care to the patient, while a chaplain, social worker and bereavement counselor provide additional support and education to families and caregivers,” Norman says.
Hospice ideally occurs in a patient’s home, whether that’s a personal residence or assisted living community. It is a Medicare-reimbursed benefit, and most private insurance providers do also cover some hospice costs.
“End-of-life care isn’t just about taking pain medications to relieve symptoms until death,” Norman says. “It helps people gain emotional strength and carry on with daily life, while improving the quality of life. The goal is to help patients and their families make every remaining moment as comfortable and enriching as possible.”
Never mind assisted-dying, our health care system needs to change the way it deals with the natural end of life
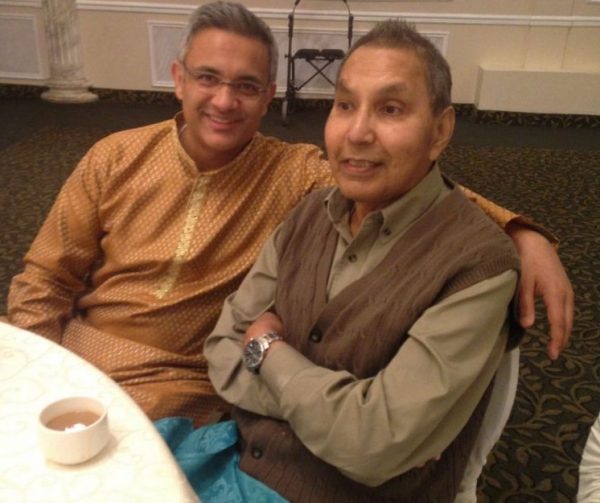
By Mohamed Dhanani
Mohamed Dhanani, left, with his father-in-law Ijaz Ahmad at a wedding last year. “The eight different doctors who treated my father-in-law all had different ideas about what (his wishes not to be life support) meant, and how involved the family should be in making treatment decisions,” writes Mohamed Dhanani. “This inconsistency — the waiting, the arguing, the feeling of powerlessness — was our family’s worst experience with a health care system of which we are so often proud.”
I’ve spent much of my career in the health care field, but it took a very personal experience to drive home just how poorly prepared health care providers are to help us through the one certain life-experience that awaits us all: death.
It happened in a hospital in southern Ontario. My father-in-law, Ijaz Ahmad, who lived with insulin-dependent diabetes for 35 years, went into the hospital for a partial foot amputation due to a bone infection.
Prior to surgery, a routine diagnostic test was performed requiring dye to be inserted into his bloodstream. After the surgery, the dye put him into kidney failure while it was being metabolized. Within a day of the surgery all of his organs started to fail and he was put on life support for what we were told would be two to three days so his organs could rest and strengthen — after which, we were told, “the doctors would bring him back.”
He spent the next 18 days on life support. And what became clear over that long 18-day ordeal is that what had clearly become the end of his life would have been unnecessarily prolonged depending on which of the eight doctors we interacted with was treating him that day.
Like so many families who have had the difficult but essential conversation with an aging parent around their end-of-life wishes, we had spoken with him about his wishes. He was clear he did not want to be on life support.
The eight doctors who treated my father-in-law all had different ideas about what those wishes meant, and how involved the family should be in making treatment decisions. This inconsistency — the waiting, the arguing, the feeling of powerlessness — was our family’s worst experience with a health care system of which we are so often proud.
Some of the doctors acknowledged his wishes but said life support was an essential part of the treatment plan; it was just a temporary measure to aid in his recovery. Others made very little effort to consult with us, and another outright refused! Another doctor assured us he would “bounce back,” though nurses told us this was increasingly unlikely and that the doctor was prone to sugar-coating discussions with families.
Because of this inconsistency, different members of my family were hearing different things — and that made it even more difficult for us to make a decision we all felt comfortable with. Finally, I pulled aside the latest doctor treating my father-in-law and asked him for an absolutely frank and direct discussion. Only then were we able to make an informed decision that respected my father-in-law’s wishes and provided as much comfort as possible to our family.
On my father-in-law’s 18th day on life support, and on what was to be the final day of his life, a new doctor was treating him. This doctor had trained and practiced in the U.K., and had only recently started to work in Ontario. His European training and experience gave him a different perspective on end-of-life care, and one for which we were grateful.
In Europe, the societal conversation on end-of-life care is more advanced than in Canada — they have grappled publicly with these essential issues of decision-making in health care for many years, and physicians have therefore become more comfortable discussing end-of-life decisions with their patients and families.
Not only is this an essential conversation we need to normalize as families and as a society, it is something our health care system must take on as an essential part of its work. All doctors must be trained to discuss end-of-life care in a direct and compassionate way with patients and their families. This will only become more important as people live longer, and as their health issues become more complex as they reach the end of their lives.
Over the last few years, Canadians have engaged in an impassioned debate on assisted death, a debate that culminated in landmark — and controversial — legislation in Parliament. But assisted death is just a small part of the issue.
As my family’s experience illustrates, end-of-life care and the difficult discussions surrounding that care are too inconsistent — inconsistent between institutions and inconsistent between doctors within a single hospital. It is something we can and must fix.
Surrounded by family and friends my father-in-law peacefully passed away within minutes of removing the breathing tube. He was 66 years old. May his soul rest in eternal peace.
Jennie Dear has an evocative piece for us examining the scant evidence that scientists have so far about the mysterious threshold between life and death—what the body goes through and how a person subjectively feels it, both in terms of pain and hallucinations:
“A lot of cardiac-arrest survivors describe that during their unconscious period, they have this amazing experience in their brain,” [neuroscientist Jimo Borjigin] says. “They see lights and then they describe the experience as ‘realer than real.’” She realized the sudden release of neurochemicals might help to explain this feeling. … Most of the patients interviewed [for a study at a hospice center], 88 percent, had at least one dream or vision.
One reader says of Dear’s ostensibly morbid piece (“What It Feels Like to Die”): “The article is comforting in a way I did not anticipate.” Another reader agrees:
I kissed my dad goodbye on the forehead right before he died. He smiled briefly. So, this article was some comfort in maybe explaining that smile of his.
This next reader also lost her father:
I remember when my dad was dying, and my mom forbade any of us from telling him that he was dying. I thought that that was terribly selfish on her part, and I told my husband that if I were dying I would want to know.
When my mom passed away, she was “treated” to the experience of my sisters bitterly arguing as to who was the favorite. (I knew I wasn’t and just held her hand.) My husband got my sisters to stop. Finally, the doctors came in and actually said she had permission to die … Mom was like that; you had to have permission in her mind for everything.
My dear husband is gone now, and I just hope that when I go, I’ll be thinking of him.
That reader’s line—“if I were dying I would want to know”—prompted a question in my mind I’ve long answered in the affirmative: “Do you want to be awake for your death and know it’s coming?” The conventional wisdom says most people prefer to die in their sleep, but, as long as there’s no intense pain involved, sleeping seems like a disappointing way to experience one of the most profound parts of life—it’s ending. And whenever I think of that question, I’m reminded of these lyrics from Björk’s “Hyperballad”:
I imagine what my body would sound like
Slamming against those rocks
And when it lands
Will my eyes be closed or open?
Would you rather be sleep or awake? How exactly would you prefer to die? What’s the ideal situation? Email hello@theatlantic.com if you’d like to share.
Back to a few more stories from readers regarding the death of a loved one. This memory is particularly poignant:
Twelve months ago, my 33-year-old daughter Phoebe began to die from metastatic melanoma. Over the next 10 weeks at a hospital in Melbourne, she went through each of the experiences outlined in Jennie Dear’s article. During this time, Phoebe asked her nurse how would she know when she was about to actually die. Donna told her that something would happen and she would know—both vague and oddly specific, but Phoebe was satisfied.
A week before her death, having gotten her pain under control, Phoebe was at home to say goodbye to her animals, clean out her cupboards, and give away her possessions. She was standing in the yard throwing a ball for the dog when she suddenly sat down, as I watched from the kitchen. I’m sure she realized as she collapsed to the bench that her time had come. I doubt that there could be a lonelier moment in a person’s life.
She didn’t speak again. Her hearing and hand gestures reduced over a few days to squeezing, then nothing but breathing quietly. Her brother-in-law, who was with her at the end, said she simply stopped breathing.
Each person’s death is different, so I found Dear’s article comforting in a way I did not anticipate.
One more reader for now:
My father was put into hospice, and all his meds were stopped. He “recovered” and lived another six months. After they “kicked him out” of hospice, he and I spent a lot of quality time together. When the end came, he was ready even though he could no longer speak. The hospice nurse came and looked at all the meds and found that while we still had the liquid morphine, we no longer had the Ativan, so we ordered a stat delivery from the pharmacist.
Giving morphine to a dying person can feel a lot like murder, and listening to the death rattle is more distressing than listening to a crying infant, but I think that the death experience is far worse for the person attending the death than for the one who is dying.
The Ativan was given to my father late in this process, but that was the drug which provided him with joy and relief. Shortly after he received the drug, I believe I witnessed him greeting his mother who had died 40 years ago.
My father then developed what is called a Cheyne-Stokes respiration; he would breath rapidly for a few minutes and then stop breathing. He resumed breathing like clockwork at 65 seconds from his previous breath. This lasted for hours. His last breath sounded much like a laugh, and I thought it was his way of saying good-bye.
I thought the event would be gruesome, but it was a special bonding experience which has helped me to reduce my fear of dying.
Take control over the end of your life: what you need to know about advance care directives.
Many agree on the factors contributing to a good death. People want to be treated with dignity, have relief from pain and, as much as possible, to control what happens to them.
Advance care planning is one way to exercise control. The process involves discussing and expressing preferences about the kind of care you would or would not want in a situation where you lack the mental capacity to make decisions.
As part of this process, you can write an advance care directive – a document that can be legally binding. It states your views and instructions about health care and other personal matters.
You can also appoint someone you trust to be you health care decision-maker. Despite its usefulness, only a small number of Australians (around 14%) currently have an advance care directive.
Why have a directive?
Studies show at least one-third of patients receive non-beneficial treatments at the end of their life, including tube-feeding and surgical procedures when there is little hope of the patient getting better. This is despite many older Australians saying they do not want medical interventions to keep them alive when their quality of life is poor.
With a good advance care directive in place, people are more likely to have their wishes for care respected. People with a directive are also more likely to experience fewer unwanted medical interventions, less likely to be moved from their home or community care to a hospital, and less likely to die in a hospital.
A directive means you can tell people your health care wishes so your choices can be legally respected.
If a patient who doesn’t have a directive is seriously ill and unable to communicate, doctors will consult with family or others close to the patient about their care. Family members and caregivers often experience stress and guilt when making decisions for a loved one at the end of their life. These decisions are made easier if they are guided by the values and preferences expressed in an advance care directive.
There are two kinds of directives: statutory and common law. A statutory directive means the person completes a document that meets specific government requirements – such as this one in South Australia or this one in Queensland. This week, the Victorian government introduced a bill to parliament to make advanced care directives legally enforceable.
New South Wales and Tasmania don’t have statutes that create forms for advance care directives, but people can make common law directives. This means they can state their health care wishes in their own way and they can be legally respected.
In 2009, the NSW Supreme Court ruled that a hospital had to follow the medical instructions a man had recorded in worksheets. The man was hospitalised with serious illness, lost consciousness and went into kidney failure. The court said the hospital had to respect the written instructions that refused blood transfusions and dialysis.
States that have statutory advance directives may also allow a person to make a common law directive. So it is not always necessary to use a government form. People interested in making an advance directive or appointing a health-care decision-maker should look up the rules in their state or territory; there are some good websites with accurate information.
What’s in a directive?
People often think of an advance care directive as a document that refuses consent to specific treatments. For example, you can specify you don’t want CPR or tube-feeding if you have a life-threatening medical problem with little chance of recovery.
This is true. But directives can also be used to document your values, say what quality of life means to you and specify if you have spiritual or lifestyle beliefs you want respected. For instance, you can write down things that would help create a home-like environment if you have to be cared for in a facility, such as music you would like to listen to or treasured items you would like in your room.
A person might complete an official statutory form to appoint someone as their health-care decision-maker, then attach a statement of values.
A statement of values, wishes and preferences can be helpful for appointed decision-makers and for care providers. Websites such as My Values can help you consider issues about medical care and dying you may not have thought about before.
What else do I need to know?
You are encouraged to review your advance care directive, and other legal documents, to make sure they are up-to-date and reflect your current wishes and instructions.
It is also vital to share your directive with your health-care providers, appointed decision-maker (if you have one), family members and other loved ones who may be called on to help make decisions. Doctors cannot follow a directive if they don’t know it exists.
There is no mandatory central registry in Australia to make sure doctors have access to directives when needed. But people with an electronic health record – known as My Health Record – can include their advance care directive information there.
Advance care planning is typically promoted in health-care settings. But some people are more likely to talk to a lawyer than a doctor about their health wishes. This often happens when a person seeks legal help on other aspects of future planning, such as writing a will or appointing a financial decision maker.
I have argued that legal and health professions can work together more effectively to help their clients plan for their future health care. Doing so promotes their clients’ interests and autonomy. It makes sure people’s values and wishes are known, even beyond a time when they can no longer speak for themselves.