IT IS easy to forget that adultery was a crime in Spain until 1978; or that in America, where gay marriage is allowed by 37 states and may soon be extended to all others by the Supreme Court, the last anti-sodomy law was struck down only in 2003. Yet, although most Western governments no longer try to dictate how consenting adults have sex, the state still stands in the way of their choices about death. An increasing number of people—and this newspaper—believe that is wrong.
The argument is over the right to die with a doctor’s help at the time and in the manner of your own choosing. As yet only a handful of European countries, Colombia and five American states allow some form of doctor-assisted dying. But draft bills, ballot initiatives and court cases are progressing in 20 more states and several other countries (see article). In Canada the Supreme Court recently struck down a ban on helping patients to die; its ruling will take effect next year. In the coming months bills will go before parliaments in Britain and Germany.
The idea fills its critics with dismay. For some, the argument is moral and absolute. Deliberately ending a human life is wrong, because life is sacred and the endurance of suffering confers its own dignity. For others, the legalisation of doctor-assisted dying is the first step on a slippery slope where the vulnerable are threatened and where premature death becomes a cheap alternative to palliative care.
These views are deeply held and deserve to be taken seriously. But liberty and autonomy are sources of human dignity, too. Both add to the value of a life. In a secular society, it is odd to buttress the sanctity of life in the abstract by subjecting a lot of particular lives to unbearable pain, misery and suffering. And evidence from places that have allowed assisted dying suggests that there is no slippery slope towards widespread euthanasia. In fact, the evidence leads to the conclusion that most of the schemes for assisted dying should be bolder.
Nothing is hurt, nothing is lost
The popular desire for assisted dying is beyond question. The Economist asked Ipsos MORI to survey people in 15 countries on whether doctors should be allowed to help patients to die, and if so, how and when. Russia and Poland are against, but we find strong support across America and western Europe for allowing doctors to prescribe lethal drugs to patients with terminal diseases. In 11 out of the 15 countries we surveyed, most people favoured extending doctor-assisted dying to patients who are in great physical suffering but not close to death.
No wonder that, just as adultery existed in Spain before 1978, so too many doctors help their patients die even if the law bans them from doing so. Usually this is by withdrawing treatment or administering pain-relief in lethal doses. Often doctors act after talking to patients and their relatives. Occasionally, when doctors overstep the mark, they are investigated, though rarely charged. Some people welcome this fudge because it establishes limits to doctor-assisted dying without the need to articulate the difficult moral choices this involves.
But this approach is unethical and unworkable. It is unethical because an explicit choice that should lie with the patient is wholly in the hands of a doctor. It is hypocritical because society is pretending to shun doctor-assisted dying while tacitly condoning it without safeguards. What may turn out to be more important, this system is also becoming impractical. Most deaths now take place in hospital, under teams of doctors who are working with closer legal and professional oversight. Death by nods and winks is no good.
Better is to face the arguments. One fear is that assisted dying will be foisted on vulnerable patients, bullied by rogue doctors, grasping relatives, miserly insurers or a cash-strapped state. Experience in Oregon, which has had a law since 1997, suggests otherwise. Those who choose assisted suicide are in fact well-educated, insured and receiving palliative care. They are motivated by pain, as well as the desire to preserve their own dignity, autonomy and pleasure in life.
Another fear is that assisted dying will downgrade care. But Belgium and Holland have some of the best palliative care in Europe. Surveys show that doctors are as trusted in countries with assisted dying as they are in those without. And there are scant signs of a slippery slope. In Oregon only 1,327 people have received lethal medicine—and just two-thirds of those have used it to take their lives. Assisted dying now accounts for about 3% of deaths in the Netherlands—a large number—but this is less a rush to assisted dying than the coming to light of an unspoken tradition in which doctors quietly brought their patients’ lives to an end.
Wear no forced air of solemnity or sorrow
How, then, should assisted dying work? For many the model is Oregon’s Death with Dignity Act. It allows (but does not oblige) doctors to prescribe lethal drugs to patients with less than six months to live who ask for them, if a second doctor agrees. There is a cooling-off period of 15 days.
We would go further. Oregon insists that the lethal dose is self-administered, to avoid voluntary euthanasia. To the patient the moral distinction between taking a pill and asking for an injection is slight. But the practical consequence of this stricture is to prevent those who are incapacitated from being granted help to die. Not surprisingly, some of the fiercest campaigners for doctor-assisted dying suffer from ailments such as motor neurone disease, which causes progressive paralysis. They want to know that when they are incapacitated, they will be granted help to die, if that is their wish. Allowing doctors to administer the drugs would ensure this.
Oregon’s law covers only conditions that are terminal. Again, that is too rigid. The criterion for assisting dying should be a patient’s assessment of his suffering, not the nature of his illness. Some activists for the rights of the disabled regard the idea that death could be better than a chronic condition as tantamount to declaring disabled people to be of lesser worth. We regard it as an expression of their autonomy. So do many disabled people. Stephen Hawking has described keeping someone alive against his wishes as the “ultimate indignity”.
One exception to this distinction should be children. The decision of whether to endure chronic conditions should be left until adulthood. But, as with adults, children facing imminent death from terminal diseases should, in consultation with their parents and doctors, have the right to be spared their last agonising hours.
The hardest question is whether doctor-assisted dying should be available for those in mental anguish. No one wants to make suicide easier for the depressed: many will recover and enjoy life again. But mental pain is as real as physical pain, even though it is harder for onlookers to gauge. And even among the terminally ill, the suffering that causes some to seek a quicker death may not be physical. Doctor-assisted death on grounds of mental suffering should therefore be allowed.
Because patients’ judgments may be ill-informed and states of mind can change, especially among the mentally ill, society should help people to die only when safeguards are in place. These should include mandatory counselling about alternatives, such as pain relief, psychotherapy and palliative care; a waiting period, to ensure that the intention is enduring; and a face-to-face consultation with a second, independent medical expert to confirm the patient’s prognosis and capacity. In cases of mental suffering the safeguards should be especially strong.
The most determined people do not always choose wisely, no matter how well they are counselled. But it would be wrong to deny everyone the right to assisted death for this reason alone. Competent adults are allowed to make other momentous, irrevocable choices: to undergo a sex change or to have an abortion. People deserve the same control over their own death. Instead of dying in intensive care under bright lights and among strangers, people should be able to end their lives when they are ready, surrounded by those they love. Complete Article HERE!
Sheila Kitzinger, the natural childbirth activist who died in April, pioneered the idea of birth plans. Her daughters, Celia and Jenny, describe how their mother made a death plan – so she could die at home according to her own wishes
By Celia and Jenny Kitzinger
Sheila Kitzinger, the writer and natural childbirth campaigner.
Our mother, Sheila Kitzinger, champion of women’s rights in childbirth, died in April. In writing her own fantasy obituary for a newspaper many years earlier, she imagined dying at the height of her powers: “She died as she would have wished, flat on her back on a table with her legs in the air, in front of a large audience, demonstrating with vigour the dangers of making women lie down, hold their breath till their eyes bulge and strain as if forcing through a coconut to push a baby out. She claimed that treating the second stage of labour as a race to the finishing post … could result in cardiac arrhythmia and even a stroke. She made her point.”
Rather than the melodramatic early death she conjured up here, Sheila died quietly at home surrounded by her family, at the age of 86.
Sheila spent her life campaigning for autonomy and choice in childbirth and challenging the medicalisation of birth. She pioneered birth plans to support women in making their own decisions. When it came to dying, she expressed the same values of choice and control, and she planned ahead. She appointed one of our sisters, Tess, with lasting power of attorney for health and welfare and also wrote an advance decision. This preparation was invaluable in ensuring that her choices were respected and in allowing her to die at home as she wanted.
Being at home was essential to her idea of a “good death”. She wanted to be in familiar surroundings, on her own territory, with the support of those who knew her. She particularly did not want to go into hospital, aware as she was of the cascade of interventions that can befall people at the end of life, just as they can women in childbirth.
In her autobiography, she records that Cicely Saunders, founder of the modern hospice movement, once said to her backstage at a conference where they were both speaking, “You and I are doing the same work.”
Her concerns about hospital treatment had also been cruelly refined and reinforced by our family experience of the treatment of our sister, Polly, who was severely brain injured in a car crash six years ago. We were all very aware of how institutions have their own systems, policies and agendas that can strip control from the individual.
Sheila wrote about her own mother’s death decades earlier. Following a brain haemorrhage, her mother could no longer swallow, and Sheila resisted a feeding tube. “I consulted Father and we both agreed, ‘No. She would want to be at home. She wouldn’t want invasive procedures.’ Later he told me that he wished he had the courage to care for his father that way when he was dying. Instead, he had him admitted to hospital and everything was done to prolong his life by every means possible. Looking back on it, he thought it was wrong, and now he felt guilty.”
At 86, Sheila had cancer and many other diseases of old age. After the first bout of cancer a year earlier, she had accepted treatment. When the illness returned she declined further investigation or intervention.
As her health declined she lost interest in eating or drinking – it was painful to watch her become progressively thinner and more frail. At times she was able to enjoy someone reading to her, she would gamely invite the family join her to sip a little sparkling wine or eat a chocolate, and the ritual of tea at 5pm still seemed to give her pleasure. But it was deeply distressing to witness how vulnerable she became.
In the last few months of her life, Sheila stopped talking about planning her next book and talked with us about her wishes for her death. She also revisited and confirmed the short advance decision (AD) she had written some years earlier. This was a single paragraph (signed and witnessed, and legally binding on her carers and medical professionals) which declared: “If the time comes when I can no longer take part in decisions for my own future, I want to receive whatever quantity of drugs can keep me free from pain or distress, even if death is hastened. If there is no reasonable prospect of recovery I do not consent to be kept alive by artificial means. I do not wish to be transferred to hospital and should like to die in my own bed.”
Except for the last few days, when she was unconscious, Sheila was able to communicate her wishes herself. But her AD was immensely valuable in supporting her choices. Her GP surgery tried to insist, a few weeks before she died, that Sheila should be transferred to hospital after a “mini-stroke”. She said no. The GP questioned her mental capacity to refuse hospitalisation. We read out her AD and she stayed home.
Later her AD was useful when another doctor was considering transferring Sheila to hospital to clarify her diagnosis and it helped her to avoid various interventions. One of the last whole sentences Sheila said was, “I decline antibiotics if I get pneumonia” and, later, she nodded when offered morphine. Anyone in doubt about her capacity to make her own choices, or concerned to ensure they had done everything possible as a healthcare professional, could read her AD or talk with her LPA for health and welfare – and be empowered to provide “person-centred care” with confidence that they knew what her wishes were.
Sheila Kitzinger’s simple cardboard coffin at her home, decorated by her family with peacock feathers and pictures of birds.
A home death is not right for everyone. We were lucky that Sheila’s symptoms were well controlled, and that’s not always possible at home. The whole situation placed many demands and stresses on the whole family. However, once it was (belatedly) agreed that she was at the “end of life” we were provided with well-coordinated NHS support. It also helped that we are a large family so when one of us was at the end of her tether, another could step in.
This support structure allowed Sheila to die, as she had lived, on her own terms. It also allowed us to have positive memories of the last weeks of her life – and that now helps us with our grief.
Sheila’s burial reflected the values she had lived by – and was shaped by her own distinct choices. She was critical of the “business” of funerals and preferred not to have her body handed over to the professionals. Instead, the day after she died, we – her daughters – washed and dressed her body one last time and carried her downstairs to place her in a bright orange cardboard coffin, decorated with peacock feathers.
Sheila opted for a simple, private burial – much to the surprise of some friends and colleagues who had expected an opulent public funeral extravaganza. Sheila wanted her body buried “without fuss”. So we carried her coffin from the house, to a tune from our time in Jamaica in the 1960s, placed it in the back of a car, and drove to a woodland burial ground. We lowered the coffin into the ground, scattered it with sprigs of rosemary and camellia blossom from our lovely garden and read some of Sheila’s own poetry:
“After the soaring, a peace like swans settling on the lake After the tumult and the roaring winds,
Deborah Ziegler holds a photo of her daughter, Brittany Maynard, with her husband Gary Holmes after the California Senate passed a bill allowing physicians to assist in the death of terminally ill patients.
LESS THAN a month before she died, Brittany Maynard posted a video explaining her decision to move to Oregon to take advantage of the state’s law allowing terminally ill people to end their own lives. Maynard, 29, had been diagnosed with an aggressive and terminal brain cancer and said she wanted to die on her own terms. “I hope to pass in peace,” she said. Her video, viewed more than 9 million times in the first month, and her death, after she ingested medication prescribed by a doctor, helped fuel a national movement for “death with dignity.”
In addition to Oregon, four other states — Washington, Vermont, New Mexico and Montana — allow physicians to provide aid in dying. After Ms. Maynard’s death in November, lawmakers in more than 20 states and the District — backed by advocates Compassion and Choices, and the Death with Dignity National Center — introduced end-of-life legislation. In many cases, the bills are pending; in states where they didn’t advance, including Maryland, lawmakers vowed to try again. A recent Gallup poll showed nearly seven in 10 Americans agree that terminally ill adults should have the right to medical assistance in bringing about a peaceful death.
Meanwhile, D.C. Council member Mary M. Cheh (D-Ward 3) has sponsored a bill modeled on Oregon’s law for the nation’s capital. That has the potential to bring Congress into the debate.
The issue stirs strong emotions. Some opponents, including the Catholic Church, cite religious or moral grounds, seeing any form of assisted dying as anathema to teachings that life is never to be taken. Some physicians believe the practice violates their oath only to heal, and some disability rights activists fear that they will be vulnerable to abuses. Others warn of a slippery slope to euthanasia.
Oregon’s 18 years of experience do not confirm any of these fears. Enacted in 1997, Oregon’s Death with Dignity Act allows terminally ill adults who are residents of the state to obtain and use prescriptions from their physicians for self-administered lethal doses. Stringent protections include a life expectancy of less than six months, a finding of mental capability, a concurring opinion from a second doctor, mandatory discussion of hospice and other options, waiting periods and more.
Oregonians have made sparing use of the law, with 859 deaths as of Feb. 2 . The state collects data on each case, and there have been no reports of coerced or wrongly qualified assisted deaths. The typical patient is about 71, suffering from terminal cancer, well-educated, with health insurance and enrolled in hospice. About one-third of prescriptions were never used, suggesting some terminally ill people are comforted by knowing they have an alternative to extensive suffering should they need it.
Such suffering has been described by Diane Rehm, the WAMU-FM radio host. Her husband, incapacitated by Parkinson’s disease and without an Oregon-style option, starved himself to death over an agonizing 10 days. Barbara Blalock, a Rockville doctor, said at a joint Maryland legislative committee hearing that she has had patients ask, “Is there a way that we can avoid intolerable suffering at the end of life?” Dr. Blalock said she often has to say no, “and I always felt as a physician I was failing them in some way.” Ms. Maynard said of her decision: “I do not want to die. But I am dying. And I want to die on my own terms.”
Death with dignity laws need to be carefully thought out, written and monitored. Oregon and the states that followed its example show that such care is possible. We hope the rest of the nation catches up with this humane option for life’s end. Complete Article HERE!
Sesame Street was talking about grief before it was cool. Okay, so talking about death and grief still may not be cool (wait, do people even say “cool” anymore? Am I showing my age?). Let’s just say this: Sesame Street was tackling this topic long before the internet was full of tools and activities for supporting grieving kids. As early as 1983 they were helping kids understand death and grief. 30 years later they are still at it, better than ever.
Then
The first time Sesame Street really tackled death was when Mr. Hooper died in an episode that aired on Thanksgiving Day in 1983. When Will Lee, the actor who played Mr. Hooper, died of a heart attack there were many ways that Sesame Street could have handled it. Rather than shying away from the topic of death and grief, Sesame Street used this as an opportunity to do what they do best – teach. In the “Farewell, Mr. Hooper” episode, Sesame Street used Big Bird to help kids understand death and grief.
Now
In 2010 Sesame Street and Sesame Workshop received grants through a number of defense organizations and Walmart to put together resources for children on grief and loss. Launched with a great TV special, they put together an incredible combination of resources for grieving kids and adults supporting those kids. Many of these resources are available for free viewing and download. Check out a preview of the video here of the special done with Katie Couric, Elmo, and the families of several children who have experienced losses:
Or check out the whole video by going to the PBS website HERE!:
Over the years Sesame Street has kept up this trend of tackling tough topics head on, to help kids in times where they may feel unsafe, unsure, scared or confused. After 9/11 Sesame Street helped kids with fires and emergencies in an episode on a fire at Hooper’s Store.
After Hurricane Katrina Sesame Street tackled this topic through a series of episodes about a hurricane on Sesame Street.
Love Never Dies
In 2004, 21 years after Mr. Hooper’s death on the show, Grover takes Elmo on a walk (cab ride) down memory lane. At the very start of this journey Elmo learned about Mr. Hooper and how Hooper’s Store got his name.
To this day Mr. Hooper’s picture still hangs above Big Bird’s nest and can be seen in the hurricane episodes. Thanks Sesame Street, for facing this tough topic head on. And thanks for reminding kids (and all of us) that those we love and lose remain part of us, even 30 years later.
‘My obstetrician’s tears stunned me but also provided immediate comfort. They normalised the mad grief that had begun to set inside me.’
Around this time 10 years ago, I was poised to start my first job as an oncologist when personal tragedy visited in a way that would forever change the way I would practice medicine.
I had returned from my Fulbright year at the University of Chicago, blessed with only the joys and none of the irritations of being pregnant with twins. Landing in Melbourne, I went for a routine ultrasound as a beaming, expectant parent. I came out a grieving patient. The twins were dying in utero, unsuspectedly and unobtrusively, from some rare condition that I had never heard of. Two days later, I was induced into labour to deliver the two little boys whom we would never see grow. Then I went home.
If all this sounds a little detached it is because 10 years later I still have no words to describe the total bewilderment, the depth of sorrow and the intensity of loss that I experienced during those days. Some days, I really thought my heart would break into pieces. Ten years later, the din of happy children fills our house. But what I have found myself frequently reflecting on is how the behaviour of my doctors in those days profoundly altered the way in which I would treat my patients.
An experienced obstetrician was performing my ultrasound that morning. Everything was going well and we chatted away about my new job until he frowned. Then he grimaced, pushed and prodded with the probe, and rushed out before I could utter a word. He then took me into his office and offered me his comfortable seat. Not too many pregnant women need a consultation at a routine ultrasound.
“I am afraid I have bad news,” he said before sketching a picture to describe the extent of the trouble. I thought for a fleeting moment that my medical brain would kick in and I would present him with sophisticated questions to test his assertion that the twins were gravely ill. But of course, I was like every other patient, simultaneously bursting with questions while rendered mute by shock.
I was well aware that doctors sometimes sidestepped the truth, usually with the intent of protecting the patient. I knew he could easily get away with not telling me any more until he had more information but I also knew that he knew. I read it in his face and I desperately wanted him to tell me.
I asked the only question that mattered.
“Will they die?”
“Yes,” he said, simply holding my gaze until his tears started.
As I took in the framed photos of children around his office he probably wished he could hide them all away.
“I don’t know what to say,” he murmured, his eyes still wet.
Until then, in 13 years of medical training, I had never seen a doctor cry. I had participated in every drama that life in bustling public hospitals offers but never once had I seen a doctor cry.
My obstetrician’s tears stunned me but also provided immediate comfort. They normalised the mad grief that had begun to set inside me. Yes, the doctor’s expression said, this is truly awful and I feel sad too.
“You are sure?”
“There is a faint chance that one lives but if you ask me, things look bad. You know I will do everything I can to confirm this,” he said.
The obstetrician had told the unflinching truth and in doing so almost surgically displaced uncertainty with the knowledge that I needed to prepare myself for what lay ahead. I had test after test that day, each specialist confirming the worst. I think I coped better because the first doctor had told the truth.
Two other notable things happened that week. Among the wishes that flowed, another doctor wrote me an atypical condolence note. His letter began with the various tragedies that had taken place that week, some on home soil and others involving complete strangers. “I ask myself why,” he wrote, “and of course there is no answer to why anyone must suffer.”
Until then, everyone had commiserated only at my loss – and I was enormously grateful – but here was someone gently reminding me that in life we are all visited by tragedy. All the support and love in the world won’t make you immune to misfortune, he was saying, but it will help ease the pain.
Finally, there was the grieving. I lost count of the pamphlets that were left at our door to attend support groups, counselling sessions and bereavement seminars but we were resolutely having none of it. My midwife called me out of the blue – it was a moving exchange that taught me how deeply nurses are affected too. But I didn’t need counselling, I needed time. I valued the offers but I knew that my catharsis lay in writing. I wrote myself out of suffocating grief, which eventually turned to deep sadness and then a hollow pain, which eventually receded enough to allow me to take up my job as a brand new oncologist. How I would interpret the needs of my patients was fundamentally altered now that I had been one myself.
Cancer patients are very particular about how much truth they want to know and when. I don’t decide for them but if they ask me I always tell the truth. A wife brings in her husband and his horrendous scans trigger a gasp of astonishment among even the non-oncologists.
“Doctor, will he die from this?” she asks me.
“I am afraid so,” I answer gently, “but I will do everything in my power to keep him well for as long as I can.”
It is the only truthful promise I can make and although she is distressed she returns to thank me for giving her clarity. Sometimes honesty backfires, when the patient or family later say they wanted to talk but not really hear bad news. I find these encounters particularly upsetting but they are rare and I don’t let them sway me from telling the truth.
Oncology is emotionally charged and I have never been afraid of admitting this to the very people who imbue my work with emotion. I don’t cry easily in front of patients but I have had my share of tears and tissues in clinic and contrary to my fears, this has been an odd source of comfort to patients. In his Christmas card, a widower wrote that when my voice broke at the news that his wife had died he felt consoled that the world shared his heartbreak.
It can be tricky but I try to put my patients’ grief into perspective without being insensitive. It’s extraordinary how many of them really appreciate knowing that I, and others, have seen thousands of people who are frightened, sad, philosophical, resigned, angry, brave and puzzled, sometimes all together, just like them. It doesn’t diminish their own suffering but helps them peek into the library of human experiences that are catalogued by oncologists. It prompts many patients to say that they are lucky to feel as well as they do despite a life-threatening illness, which is a positive and helpful way of viewing the world.
I will never know what kind of a doctor I might have become without the searing experience of being a patient. The twins would have been 10 soon. As I usher the next patient into my room to deliver bad news, I like to think that my loss was not entirely in vain. Complete Article HERE!
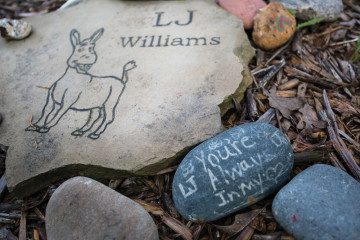
A simple memorial stone serves as the only visible marker for this shaded gravesite.
There is nothing unusual about these three girls. They are sisters. They have eyes and ears and they will remember this part of their lives forever. Taylor Ann, 9, is the oldest, and determined to speak for the others, even when it gets her in trouble. She is a smiley redhead with freckles and talks without punctuation or taking breath.
Tori is the second-oldest at 7. She is exactingly articulate, pronouncing each syllable in “e-ver-y-thing.” She has light brown hair and a slight lisp, evidence that she is growing as she speaks, her baby teeth falling out and her adult teeth growing in. Her voice is perfectly childish and curious.
Texie, 4, is the baby sister, but not the youngest sibling. That title goes to the girls’ 2-year-old brother, Junior. Texie’s placement on the second-to-bottom sibling rung sets her just high enough to grab her older sisters’ attention, but she is still something of a baby when it comes to conversation. Even so, her sporadic observations are often quite sharp. Of the three girls, Texie has the most recognizable voice when they’re all talking at once. It’s a soft garble she uses in hiccup-like bursts to coo to her stuffed animal or scream “Caaaoooolllerr the feaddderrrs!” at the ruffled bird in her coloring book. She has baby-blue eyes and platinum-blond hair, and she makes her sisters laugh.
The sound of the three of them speaking at once is not unusual. Tori and Taylor Ann bicker over the details of a story about a kitten while Texie boks like a chicken. When I ask about their oldest brother, L.J., Taylor Ann quickly gives an answer she thinks will satisfy me, and then goes back to talking about her cat. “No,” I say, clarifying my question. “How long were you with him at your house after he actually died?”
“Oh, you mean like right after he died?” The other two are quiet now. “Um, just a night. Yeah, just one night.” The distinction is meaningful because, as Taylor Ann had told me earlier, the sisters were with L.J. for a whole year after they knew he was going to die. I look at the younger girls and they’re not interested in talking about it. We’ve talked about it enough over the last three months. Every time they visit Eloise Woods, the natural-burial park where their brother is buried and where I work, they reveal a new angle of their experience of his death. Today’s angle is that they don’t feel like talking about it.
“Let’s go see L.J.,” Tori says.
“Yeah!” the other girls shriek.
We leave the coloring books on the small table between the two sheds where we always meet and walk down Cardinal Trail to visit his grave.
I was wearing hiking boots and jeans with a bloodstain on one of the belt loops when I caught the eye of the lady at the gas station.
“Going to the beach?” she asked coyly.
“No,” I said, giggling. “A cemetery.”
“Ooooooh,” she gasped, her interest piqued.
I didn’t have time to get flirty about death. I swiped my card and rushed back to my car. Just broaching the subject of what I do often turns into a lengthy discussion about the complicated politics and emotions surrounding natural burial. It’s imperative that I engage in these discussions, and most of the time I do. Word of mouth is one of the few ways people learn that they can in fact bury people in Texas without embalming, without a vault, without even a casket. They can even bury on their own land if they meet the requirements of their county and aren ’t concerned with complicating resale of the property. But such conversations are rarely brief, and I had to get to the Woods.
We weren’t sure what time the family would be arriving with L.J., the 11-year-old who had died the night before. Specifics weren’t part of the deal with his family. Though we’d known for close to a year that they would have a home funeral followed by a natural burial, we knew little else. Even the boy’s condition—why he was terminal—was discussed only vaguely by the family. All we knew was that he was in a wheelchair and that he didn’t have long to live.
Home funerals usually lead to natural burials, but not always. Most of our families employ conventional funeral homes, hold a service in a chapel and transport the body to us in the funeral home’s vehicle. We have good relationships with many funeral homes in Austin, even though we can tell their employees feel out of place when their shiny loafers step onto our roads, mulched to prevent erosion. They usually give us a couple of days’ notice before they arrive. The night L.J. died, Ellen MacDonald, my boss, the owner of Eloise Woods, emailed me at 1 a.m. telling me to show up the next morning at 8.
L.J.’s family decorates his casket in preparation for burial.
Every time I drive to Eloise Woods, the sun strobes on my left cheek as it passes between houses and trees. It’s a bright nuisance, just beyond the reach of my visor. I drive along Austin’s eastern edge, and once I’m past the airport and under the toll road, it’s a straight shot to the burial park. I listen to music at a loud volume, usually a certain Warren Zevon live album. I roll down my windows and daydream the rest of the way to the cemetery.
When I park at the Woods 25 minutes later, I remember that I’ve forgotten my hat and will be feeling the full heat of a June day. I complain about it to Ellen as I walk from my car. “I hardly slept last night,” she responds. “I just figured I’d get out here as early as I could to get it set up. The grave still needs to be deeper because I guess they’re bringing him in a casket now.” Under Texas law, a bare body, or one in a permeable encasement such as a shroud, must be buried at least 24 inches deep. An impermeable case, such as a casket, must be covered by at least 18 inches of earth. The first few feet of topsoil is where the most aggressive organic activity takes place, turning whatever has been buried into plant food. We had dug 2.5 feet deep, enough that L.J. in a shroud would be covered with 24 inches of soil. But a family member had offered to build a casket at the last minute, and now we needed to dig at least another foot to ensure that a full 18 inches of soil would cover his little box.
It’s about 50-50 at the Woods when it comes to shrouds vs. caskets. Only one person has been buried without any covering at all—an infant from a Hindu family. Cremation is a custom in that religion, a manner of releasing and purifying the soul, but children are considered already enlightened, and so natural burial with nothing between the body and the earth is traditional. Ellen told me she had laid rose petals on the soil before the baby was placed in the grave, a gesture in line with why someone had offered to construct a casket for L.J. Burying a child in raw dirt isn’t easy.
Ellen wore an apron with a picture of a cat wearing a chef’s hat and the words “The Chef Breathlessly Awaits Your Order” printed beneath.
“I thought it was cute, you know? Kids like cats. Something kind of fun for today,” she explained. Ellen is good at remembering what’s most important and forgetting everything else. Today was all about being there for the kids.
Ellen had no connection to funerals or burials when she bought the Eloise Woods property in 2009. She had completed a doctorate in neuroscience at Stanford University before becoming a stay-at-home mom in Austin. She was so inspired by the show Six Feet Under, where she first learned about natural burial, that she decided to get into the death business herself. She became obsessed with creating a space in Austin where people can bury their dead themselves, a place where the memory of the deceased can continue to grow with the landscape.
Ellen is the reason I got into natural burial. Her accomplishments as an industry outsider signified a shift in my profession and revealed an opportunity largely untouched by traditional industry professionals. In Wisconsin, where I received my funeral director’s license, combining the business of funeral homes and cemeteries is prohibited under the state’s anti-combination law. Due to this 80-year-old statute, I became accustomed to hearing each business condemn the other, usually over outrageously high prices.
When I got to Texas, which allows the two businesses to be combined, it became apparent that such criticisms stemmed from a shared anxiety about the future of the industry as a whole. Cheap, efficient cremations have risen in popularity since the ’90s, eating into the conventional funeral industry’s profits. Families with little interest in embalming or holding a service make it harder for funeral homes to maintain their value.
Even Houston-headquartered Service Corporation International, the nation’s largest funeral corporation, appears to be acknowledging this change of venue. In October 2014, having lost a battle to overturn Wisconsin’s anti-combo law, Service Corporation opted to sell the last of its 16 Wisconsin funeral homes, keeping the five cemeteries it owns in the state. For people in search of a final resting place for their ashes or bones, a cemetery is the only choice. Natural burial parks that are accustomed to working with families without the involvement of a funeral home make that choice easier.
L.J.’s family surrounded his memorial stone with rocks carrying special notes. Owner Ellen MacDonald creates hand-engraved memorial stones for everyone buried at Eloise Woods, like this one featuring Donkey, L.J.’s favorite character from the movie Shrek.
The first burial I worked at Eloise Woods was for a young man in his late 20s. This last summer we buried three kids: one boy of grade-school age and two infants. There are more than 60 occupied plots in the park, a quarter of them for infants and children.
I met L.J.’s family for the first time about a month prior to his death. His three sisters attacked me with questions and whirled with an exuberance that only children seem able to bring to their first experience of death. Having never seen me or even heard my name, they grabbed my hands and Texie crawled into my arms as we set off to explore the graves.
“What happens if you are the last person on earth and everyone else dies?” Tori asked.
“I guess it would be very quiet,” I answered.
“Do you know the month and day you are going to die?” she asked. I said I did not.
“When you die, are you the same age forever?” Taylor Ann asked.
I thought about that carefully before saying “I think so,” though I also told them I was unsure. Then I asked what age they would want to be forever, and we all agreed we’d want to be somewhere in the teenage years, in the bloom of youth.
They picked the wild coreopsis that grows along the paths to put near L.J.’s gravesite. As we came upon the nearby grave of a 26-year-old man, his pensive portrait engraved on his stone, they wondered how he had died. I didn’t know, and that’s what I told them.
“My brother is going to die and come to Eloise Woods,” one of the girls said. At L.J.’s grave, their parents stood with a stroller into which was strapped their littlest brother. Jackie, their mother, looked only slightly overwhelmed and remarkably well put together. She was talking to Ellen about why she’d brought the girls. They’d been confused about L.J.’s future whereabouts, so Jackie thought it would be good for them to see the little 3-by-3-foot hole with the pile of dirt next to it. They laid rocks around the hole, and flowers inside of it.
The girls were fascinated by the wildlife of the park. It looks like a wooded campground, full of bugs, lizards and animals. Hoping to see a bunny, we walked a few more trails while they told me that L.J. slept a lot and no longer got in his wheelchair.
One of them asked me what happens when you die.
“Out here,” I said, pointing to some wildflowers, “you become a plant.”
“What!?” they yelped in confusion.
“Plants are going to grow out of his body?” Tori asked. I realized that I’d have to explain decomposition to complete the puzzle.
“Well, after we die, our bodies break down,” I stammered. I tried again: “They sort of fall apart.” It was no use. Looks of confusion and then boredom crossed their faces.
“Let’s go look for Mom,” said Taylor Ann. They took off, away from me.
They found their parents at the sheds and Ellen presented them with markers and rocks to scribble messages on for L.J. Tori wrote “Get Well Soon” on one. Texie drew a fairly sophisticated cat on another.
The more they colored, the more evident it became that L.J.’s death was an event they were preparing for in much the same way they would prepare for a birthday. To add extra excitement, the date would be a surprise, no matter how ready they thought they were.
Ellen’s cat apron was overshadowed by other sartorial matters once L.J.’s family arrived for his burial. Taylor Ann jumped out of the van barefoot and ran over to me. She had been too distracted to put on shoes before they’d left their house that morning. After parking the van, Jackie opened the door with a mixture of confusion and exhaustion on her face. She caught sight of the bare feet and became annoyed. “Where are your shoes? I told you to put on shoes!” she yelled.
Taylor Ann’s face suddenly reflected the gravity of the day, a collision of sadness and anger at having been yelled at by her mother, who had just lost a child. She burst into tears. Ellen quickly offered some extra sneakers she kept in the shed. Tori and Texie hopped out of the van wearing matching handmade black dresses with white cats on them and pink-and-blue cowboy boots. Taylor Ann stomped down Cardinal Trail toward L.J.’s grave wearing the same cat-pattern dress and borrowed sneakers five sizes too big.
The small group of guests held armfuls of sunflowers and babies. Kids ran wild while their parents alternated between quiet grief and chirping baby talk. The back door of the van remained open and unattended under a bright early-afternoon sun. Inside was a simple pine box about 4 feet long.
Jason, L.J.’s stepfather, and another man got inside the grave with shovels provided by Ellen and finished the digging that we’d been unable to complete that morning. The sisters posed with their sunflowers while I took pictures on my phone, and then they colored pictures to place inside the casket with L.J. After about half an hour, Jackie and Jason went to the van for the casket. Jackie’s face carried a look of powerful intention as they brought it to the grave and set it on the path while we all gathered around. They opened the top and laid it perpendicular across the casket, revealing little L.J. lying on his side, wrapped in a white blanket.
Everyone took turns writing on the top of the casket. The girls laid their pictures next to L.J.
A pastor wearing a rainbow sash covered in peace signs and yin-yang symbols started the ceremony. Taylor Ann, not quite grasping the mood, interrupted with an enthusiastic observation and was reprimanded loudly by Jackie. Still stinging from her earlier scolding, Taylor Ann began to pout until the pastor asked her to stand next to her. Together, they began to read a children’s poem that attempted to explain death.
The girls’ 2-year-old brother, Junior, out of his stroller for the first time I had ever seen, began to stalk the woods. While everyone stood sweating and patient, listening to the poem, Junior squatted outside the circle and began to taste the dirt. Jason alternated between chasing him and standing near Jackie, his expression lightening and darkening between the two situations. When the service was over, everyone said their goodbyes before placing L.J.’s casket into the earth.
It’s hard to explain how it felt to watch the girls embrace their dead brother in his casket. How they kissed his face and stroked his hair then delightedly shoveled dirt onto his grave. If I had to try, I would say it was like hearing a child’s first attempt to pronounce a new word. Ever afterward you hear that word differently, spoken without apprehension and full of love.
The next time I saw them I was measuring and marking plots in an open field. The girls came running at me with arms spread wide like I was someone they loved. I was ripe from working in the sun all day, but Texie clung to me like she had the first day we met. We talked about the other kids who were buried there and walked to one of their graves. Jackie asked questions about him. All the parents do this. They want the story on the kids, looking for similarities that will pull them together. I didn’t know much about the kid’s story, so I asked about L.J.’s.
At the sheds, I gave the girls the coloring books I had brought that day. Junior, red-faced and awake, rolled in the dirt. Jackie gave me the long version of L.J. ’s situation, which started with his being diagnosed with spina bifida, which isn’t a life-threatening condition. The events that led to his death began with him toppling over in his wheelchair. The accident apparently created fissures in his skull, through which cerebrospinal fluid drained. Jackie says his doctors misdiagnosed L.J.’s resulting condition for years before she finally convinced them to perform a 12-hour surgery, but it was too late to save him. He didn’t have to die, she said. She showed me pictures on her phone: L.J. with purple, puffy eyes and a zig-zag incision across the top of his skull. Then she showed me pictures of L.J. when he was healthy, with big brown eyes and a shy smile.
Eloise Woods owner and operator Ellen MacDonald maps the coordinates of a grave in Dunyah Garden, just off Cardinal Trail. Some portions of Eloise Woods are specifically dedicated, like Teva Garden, an exclusively Jewish section, and Sweet Angel Garden, for infants. Rainbow Bridge holds pet remains, but many people interred at Eloise Woods chose to have their pets buried by their side.
They don’t have the energy to file a lawsuit, but they are angry. The constant hospital visits put a huge strain on the family. They were briefly homeless, sleeping in a van in the hospital parking lot.
“That was my favorite because I got to lie down,” Taylor Ann said, smiling and drawing out “liiiiie doooown” and spreading her arms. Jackie gave her an odd smile, unsure if it was safe to laugh at her daughter’s black humor in front of me. I told Taylor Ann that what she’d said was oddly comical, and Jackie broke into a relieved smile. She said that when L.J. died, the family finally had a laugh. Home funerals, like parenting, bring unpredictable joys.
Jackie explained that after L.J. died, as they were washing him, they had pulled out his gastrostomy tube, creating a leak. They scrambled for the Krazy Glue to close the hole. They all laughed as Jackie recounted this, and the girls became giddy as they clamored to offer their favorite silly moments of the death. They told me about how L.J.’s body went floppy after he died and the girls played with his limbs like a doll. Texie had waved his hand, mimicking a lecturing adult. “I’m Dr. George, and you’re not sick,” she mimicked. The sisters burst into giggles again. I could see very clearly how deeply they loved one another, how making their mother smile and laugh was the most important thing in their world.
Jackie, flushed from the laughter, said L.J. would pull at her hair to bring her closer, right until the end. She said the girls all slept with him in the living room the night after his death. Texie told us that now he’s in Eloise Woods in a silly voice that her sisters made her repeat over and over while they laughed.
When I left that day, I cried all the way home. Complete Article HERE!
A divisive national debate over whether dying patients should have the power to end their own lives will sweep into Maine this week when the Republican-controlled state Senate begins to consider so-called “death-with-dignity” legislation.
Sen. Roger Katz’s bill, which the Republican from Augusta says the Senate could take up as early as Monday, is modeled after legislation passed in Vermont two years ago that allows physicians to provide lethal doses of medication to terminally ill patients who want to hasten their death. Katz and other supporters say those who are suffering should be free to end their lives on their terms.
“Why not have the right to say, ‘I want to go, I’ve had it’?” said 85-year-old June Wagner, whose daughter died in 2012 at the age of 54 after suffering from ovarian cancer. Her daughter lived in Washington state, which has such a law, and obtained a prescription to end her own life, but Wagner said she doesn’t know if she ultimately used it.
Maine would become the sixth state in the country with such a law if Katz’s bill passes this year, but it faces an uphill battle. Lawmakers here have repeatedly rejected similar measures and voters defeated a ballot referendum on the issue in 2000.
It has been met with fierce opposition from some religious and medical groups, including the Maine Medical Association and the American Nurses Association of Maine, who say lawmakers should focus instead on ensuring that all residents have access to proper health care that can make them comfortable in the final months of their lives. Others say they fear patients will feel the need to end their own life because they believe they’re a burden on their families.
Suzanne Lafreniere, director of the office of public policy for the Roman Catholic Diocese of Portland told lawmakers earlier this year that a person’s life must be protected “at every stage and in every condition.”
“A law permitting assisted suicide would demean the lives of vulnerable patients and expose them to exploitation by those who feel they are better off dead,” she said in her written testimony.
Brittany Maynard thrust the issue back into the national spotlight last year she ended her own life just before her 30th birthday in Oregon, the first state to legalize the practice. Maynard, who was dying of brain cancer, advocated for aid-in-dying laws in videos shared widely online.
Kandyce Powell, who opposes the bill and is executive director of the Maine Hospice Council, said she believes the proposal wouldn’t resurface so frequently if more people in Maine had proper access to end-of-life care.
Vast rural parts of the state lack hospice or palliative care that can ease a person’s suffering in the final stages of their life, Dr. James VanKirk, medical director of palliative care services at Eastern Maine Medical Center.
“I am not against people having choice. That’s what we’re all about in this country,” VanKirk said. “But I think if we’re going to give people this kind of choice … we need to make sure that they really have a choice. We need to make sure that they don’t feel like they are in a situation where there is only one option.”
Katz agreed that expanding access to health care is crucial, but palliative care may not make things bearable for everyone, he said. He stressed that his proposal includes many safeguards, including requirements that a second doctor has confirmed that the patient has a limited time to live.
He’s hopeful that the national discussion and the increased awareness of the issue over the last year will help propel his bill into law — if not this year, sometime soon.
“There are some people who have religious objections or other moral objections and I respect that,” Katz said. “But I think that most people have an open mind and are waiting to hear the debate.” Complete Article HERE!