Pictured with Vietnam War Veteran John Eilers are, from left, Marine Corps 1st Sgt. Jimmy Richard, Marine Corps Veteran Nicole Richard and Army Sgt. Daiana Wininger.
Nicole Richard is kind of in awe.
Well, as she is a former Marine Corps Staff Sergeant, maybe it is more appropriate to say shock and awe.
To provide a bit of background, Richard has a certain niche when it comes to volunteering. “Kids and the elderly, to me, are really close to God,” Richard said.
As a single woman serving in the Marine Corps in Okinawa, she would sign up through the chaplain to serve in the community. It was something she did throughout her 11-year military career, working with the elderly and school children overseas in Japan, Thailand and Korea. She left military service in 2012.
In 2015, she called Diane Sancilio, the Director of Volunteer Services at Hospice of the Chesapeake, to find a way to serve seniors. When Sancilio learned she was talking with a Marine Corps Veteran, she told her about the Veteran-to-Veteran volunteer program that pairs volunteers with military experience with hospice patients who also served. After her spiel, Sancilio heard nothing on the other end of the phone. She even had to ask if Richard was still on the line.
“I was in shock about this because I didn’t even know it existed,” Richard said. She couldn’t believe that there was an opportunity for her to not only care for elderly hospice patients – but also fellow Veterans. It was kismet.
The 33-year-old mother of three from Annapolis threw herself into volunteering. She has done much of her work performing Reiki therapy at the Inpatient Care Center in Pasadena. And though she has served many patients who aren’t Veterans, she said when she works with those who have served, they feel an instant connection, “We all hold those same values, even the families,” she said. “A lot of time, these Veterans, at the end of their life, all they need to transition is to share their story, and for us to give them that welcome home that they didn’t get. They have sacrificed so much.”
The Vet-to-Vet program is part of the We Honor Veterans Program, a collaboration of the National Hospice and Palliative Care Organization and Department of Veterans Affairs. Program partners like Hospice of the Chesapeake use resources and education provided by the NHPCO and the VA to help Veteran Volunteers care for Veteran patients and their families. With more than 25 percent of Hospice of the Chesapeake patients having served in the military the need for Patient Care Volunteers who also are Veterans is growing.
Many Veteran Volunteers take it to the next level of volunteer after performing an Honor Salute for a Veteran patient. The brief but moving ceremony takes place in the patient’s home or at his or her bedside. It demonstrates a tremendous respect for the patient while also serving as an intimate moment for all involved. Richard tells of her first Honor Salute. The patient’s daughter said he had become sullen and unresponsive, and she didn’t think he would talk. Upon learning the patient was a fellow Marine, she asked her husband to join them. Marine Corps 1st Sgt. Jimmy Richard is still in active duty, assigned to Marine Barracks Washington, D.C.
The minute he saw the Richards in their uniforms, the patient perked up.
“He talked so much. We used our terminology – oorah, semper fidelis — and he was smiling, telling us about his unit, where he served, and what he’s done,” Nicole said.
Before leaving, Jimmy removed the pin from his cover and gave it to the man. There were tears all around.
The moment cemented the purpose of having the program Nicole. “He wouldn’t talk to others, but he was open to talking to us because we understand, the terminology, the values — honor, courage and commitment” she said.
She said the families will sometimes roll their eyes as a patient starts telling “another” war story. “But (Veterans) get it. It heals us, too. We have our own mental and physical wounds. Just listening to somebody else kind of helps heal us, too.”
Nicole is still a bit in awe.
“I am still digesting this is here. And I am excited to be learning more. I thought it was amazing to volunteer at the Veterans Day event,” she said, adding that the Veterans she helped at the ceremony, which included an opportunity for Veterans to talk about their service, shared her surprise.
“They are in shock about it, too,” she said. “They are thinking, ‘they shared my story, they understand, they honor me’.”
‘Diagnosing death’ would prevent unnecessary distress at the end of life.
Doctors need to be trained in the art of “diagnosing” death to prevent unnecessary distress at the end of life, an expert has claimed.
Dr Erna Haraldsdottir, a senior lecturer at Queen Margaret’s University, in Musselburgh, called for a shake-up of thinking on medical intervention for the dying after watching her elderly father-in-law die in hospital.
The 84-year-old had been diagnosed with dementia five years beforehand and his family watched his gradual decline until he was admitted to hospital. Although he was elderly and very frail, doctors attempted to discharge him at one point and tried to resuscitate him as a “do not resuscitate” note had not been arranged.
Doctors were also reluctant to issue a death certificate as they were unsure of his cause of death.
Writing in the European Journal of Palliative Care, Dr Haraldsdottir said doctors need to change their mindsets over when patients need medical intervention and try to “diagnose” death.
Dr Haraldsdottir, who also leads a pioneering research programme at St Columba’s Hospice in Edinburgh, said: “In my own experience, our family believed my father-in-law had a good death, however what was noticeable was the staff’s lack of insight into the situation and understanding of what was happening.
“This caused the family unnecessary upset and distress – which could have been avoided if the medical team had applied the principles of palliative care to the assessment and care.”
Ministers unveiled a five-year plan to put palliative care at the heart of the NHS in December and to ensure a greater openness around death and dying.
It comes after a Glasgow researchers found falling numbers of Scots were dying at home, despite many saying it was what they wanted.
It is more important than ever for hospices to be leading the way when it comes to developing care around death and dying, said Dr Duncan Brown, medical director at St Columba’s Hospice.
I’ve been with the dying many times, both in a personal capacity and as a health care professional. As an end-of-life doula my work is centred around supporting people and their families at end of life. My experiences have led me to agree wholeheartedly with the BMA in its recent report: hospitals are not the best place to die.
An overwhelming majority of us want to die at home, yet statistics show the reality is that 54% of us will die in hospital. But in my opinion, hospices are for the dying. Home is for the dying. Hospitals are not. The raison d’etre of end of life care is to help people experience a ‘good death’. We will remember how someone we love dies forever. The impact of a bad death is far-reaching. Candy Chang, creator of the ‘Before I Die‘ wall, a global art project that invites people to reflect on their lives and share their personal aspirations on a public wall, describes the fallout as creating ‘circles of mayhem’ for generations.
What is a good death?
Every person will have a different idea about what would constitute a good death for themselves or their family. Much of the debate over end-of-life care comes down to two questions:
Is a good death one where the medical team did everything to save a life?
Is this still true if there is little chance or no of a happy outcome?
Culturally, we have always seen a good death as one we have ‘fought’ against. It may be time to consider otherwise. Many treatments are aggressive and futile, robbing the last remaining quality of life a patient has.
Perhaps a good death is the accepted one. One where the dying person is in control, can be at home, can have their pain and symptoms managed. End of life care must be entirely individualised and person-centred, only then can we begin to offer the excellent end of life care that everyone deserves.
The refusal of a medical team to end active treatment to the detriment of the patient was exemplified in the death of a very close friend of mine. They threw everything they had at giving him longer than his twenty-something years. They didn’t give up ‘actively’ treating him until the end. He died clinging to the belief that he was going to live. That last precious year of his life was a tragic mess of chemotherapy, life-prolonging operations and colourless hospital wards. The treatment had destroyed the very essence of who he was, long before his heart played out its final beats.
I believe if we discussed end of life issues regularly, we wouldn’t find them so tricky to broach. Issues about death and dying should be taught in schools as part of the PSHE syllabus from primary and onwards. During Year 13 tutor time when we teach young adults to fill in job application forms, we should also be filling in advance directives with them.
Issues with control at the end
In a study by the Economist Intelligence Unit, the UK was crowned the best in the world for provision of end-of-life care. The author of the report, however, said that there is room for improvement, especially in symptom control and communication. Could this improvement be guided not by government policy or hospital administration, but by changing the way we look at death?
The recent BMA report concluded that some doctors continue to treat the dying when active treatment is no longer of any benefit. One reason it suggested was because of pressure from the patient and their loved ones. This is understandable – it is often too difficult to let go of the ones we love. The report also stated it is because if doctors acknowledge there’s nothing more that can be done, that they’re admitting defeat.
I knew a woman worked with the dying so when she was dying, although she knew there was nothing that could be done, she didn’t want to die. She wasn’t ready: she had a life to lead, a world to see and children to watch grow and guide. She was looked after by the same medical team she had worked alongside for many years. They couldn’t let her die either. If they let her die, they would have failed one of their own. They had to try, even though they knew it was futile. They couldn’t give up, even though they knew the treatment she would most likely shorten her life, not extend it. Her original prognosis with palliative care had given her up to a year. She died two weeks into aggressive treatment, four weeks after her initial diagnosis.
We should not see the death of a dying patient as a failure. Death is not the loss of a battle. Death is a natural part of life. If we could see it that way, we might be able to approach it differently. Our goal should be helping someone live as good a life as possible right up until the very end. No one will ever experience a “good death” if our focus is active treatment at all costs.
The report set out that treatment at end-of-life should be ‘appropriate and proportionate’. Dying with care, deference and dignity, and on our own terms is the very least we should be able to offer. A lady I worked with lived an incredibly full life: alone and happy. She went dancing and played snooker. She cooked everything from scratch everyday. Her breathlessness became untenable and she finally went to the doctor. She had cancer, which was slow to progress even though she chose a palliative care pathway. She accepted her life-limiting prognosis with the wisdom of one who knew herself well and contemplated mortality more often than many. She died in a hospice, surrounded by her family. Hers was a peaceful death. Peaceful and on her own terms.
One aspect of the report that I feel most strongly about is that doctors should be receiving training and CPD on communication and how best to have difficult conversations. One junior doctor who was interviewed for the report said: “I found it very difficult to talk to patients about dying, prior to working in a hospice, because…as a junior doctor we’re not taught very much…”
A shift in thinking
We all have to take responsibility for communication and the decisions we make. It’s terribly difficult when we’re unwell and vulnerable to hear these truths. If we’ve never considered end-of-life until our own life’s end it’s no wonder we find it so hard. If we discussed these issues regularly we wouldn’t find them so hard. We need to break down the ingrained cultural barriers that prevent us from talking about death and dying
Let’s all take on that responsibility. Let’s talk about it: openly and without fear. It’s too much to have that conversation for the first time when we are facing death. It’s much easier to talk about it while we’re living a healthy life.
We need to ask ourselves what is a good death for us.
Why do we value quantity over quality of time? Why do we cling so dearly to the notion that a life well lived is the longest? Sometimes doing nothing is the most courageous path. Sometimes accepting there’s nothing left that can be done is the bravest choice. Some may describe such a decision as “giving up”. Pursuing treatment until the very end, on the other hand, is lauded as “being a fighter”.
Do these words,”battle” and “fight”, compound medical teams’ feelings of failure when an unavoidable and imminent death is in front of them? Changing our language may help us to change the way we think. Illness and death are a part of life. Loss is not a failure: not ours, and not our doctors’. Perhaps redesigning our expectations and language at end of life could begin with Paul Kalanithi’s beautiful words:“The physician’s duty is not to stave off death or return patients to their old lives, but to take into our arms a patient and family whose lives have disintegrated and work until they can stand back up and face, and make sense of, their own existence.” If they did, I believe death and dying could be a richer and better experience for everyone involved.
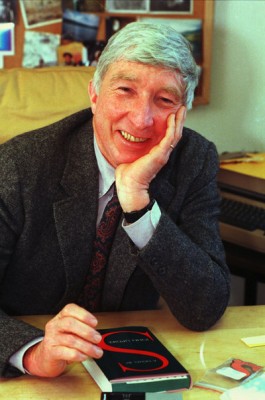
Children’s book author and illustrator Maurice Sendak, who died in 2012, spent much of his life obsessed with death. In 2011 he told Fresh Air’s Terry Gross: “There are so many beautiful things in the world which I will have to leave when I die, but I’m ready, I’m ready, I’m ready.”
Katie Roiphe’s preoccupation with death goes back to her childhood, when she contracted virulent pneumonia at the age of 12. She was sick for a year and thought she was going to die.
Her terror of death was reignited many years later when her father died. It was then that Riophe found herself turning to great minds to see how they confronted mortality.
She initially told herself that she wanted to “understand it better,” she tells NPR’s Melissa Block, but she soon realized that was a lie. “I was actually trying to see it,” she explains. “It sounds really simple, but it’s actually a very difficult thing to do. So that was my goal, to sort of focus in really closely on the final days of these writers and thinkers, and just look.”
In The Violet Hour, Roiphe describes the last days of Sigmund Freud, James Salter, Maurice Sendak, Susan Sontag, John Updike and Dylan Thomas. She talks with Block about how these writers and thinkers accepted, or railed against, their fate.
Interview Highlights
On John Updike, who wrote poems in the hospital after being diagnosed with lung cancer
It was amazing. He had very little time — just weeks before he was dead. I actually went up and looked at the manuscripts and you can see in his handwriting how arduous it was. At that last moment, when most people would just be watching television or railing against the universe, that was what he did and I found it very moving. …
The poems have a sort of quality of reporting — that he’s bringing news. And he talks about writing as turning pain into honey, which I find a really beautiful way to think about what writers do: taking this incredibly awful — maybe the most awful thing that can happen to you — and turning it into honey just with words.
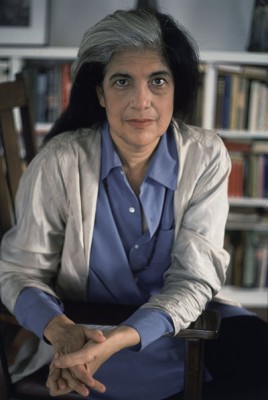
On Susan Sontag, who endured brutal treatments for cancer
She had written so eloquently about the importance of not turning illness into a metaphor — of not embellishing and fantasizing and being really realistic and rational when it comes to your own illness — and she was unable to do that ironically in her own life. …
She thought to herself she would be the exception even to the rule of mortality. That somehow, as she had with her earlier cancers famously, she was going to defeat death in some way. And even though the odds were against her — she was 71-years-old getting a bone marrow transplant — even in those situations, she felt this time she wouldn’t die.
At the one hand, it’s the opposite of a good death, it’s almost the anatomy of how you don’t want to die. On the other hand, I did see something kind of heroic in the power and force of her will.
On how mortality was a constant companion for writer and illustrator Maurice Sendak
He was certainly preoccupied with death for his entire life, and one of the things that fascinated me about him is the way, in his art and famous children’s books, he worked on this problem year after year. Like when his parents died, or when his brother died, he just kept working on this problem and worked it through in drawing after drawing and draft after draft. And he sort of came out freeing himself to a certain extent from this obsession. He was very depressed at certain points of his life and he used his art as a way of countering that. It was a sort of medication for that almost.
On Sendak owning John Keats’ death mask
It’s really very beautiful. When I saw it — he has it in a guest room with a blue bedspread — there are kind of stuffed animals on the bed. It’s a very bizarre scene and very Sendak, and I thought to myself, “Who would ever want to own Keats’s death mask?”
And then I looked at it and I realized I knew exactly why you’d want to own Keats’ desk mask: Because in a way what I was doing in this book was writing death masks. That urge to preserve the moment, and Annie Leibovitz did it with her famous photographs of Sontag, and Sendak himself drew the people he loved: his partner of many, many years after he died, and his family members right before they died.
There’s something about capturing that moment in art that I actually do completely understand — both the reason you’d make Keats’ death mask and the reason you’d want to own it.
On her idea of what a “good” death would be
I feel like the thing that mostly happened with this book is I came away marginally less afraid, which sounds like not that a big deal. But given my panic about death at various points in my life, [this] was liberating to me. In terms of a good death, I did feel that this prolonged medical struggle of a Susan Sontag where you’re chasing after any possibility of medical salvation seemed like not a good idea, and the way of working your way into accepting what’s happening the way Sendak did and the way Updike did seems preferable to me.
But one doesn’t always have control, and that was one of the things I really realized in writing about these deaths.
Now I measure time in distinct chunks, focusing on events – a holiday or a party. Although it has been an intense few months, I’ve tried not to dwell on it
By Max Edwards
Max Edwards, summer 2015.
Five months ago, I was diagnosed with terminal cancer aged 16. It was rather as I’d pictured GCSE results day to be: a lot of stress waiting for potentially awful results, although, as it happened, GCSE results day was a pleasant surprise. But, like many whose grades came as a disappointment, I got over it soon enough. I think it’s surprisingly easy to adapt to this kind of news. After all, while I’m not going to deny its personal significance, it doesn’t really change anything important.
In the past, I have imagined terminal illness as the short and depressing period before a person’s premature death, but it somehow doesn’t feel nearly as dramatic or upsetting. I don’t feel as though normal life has ceased, or that my perception of it has changed drastically. In fact, if it weren’t for my loss of mobility following an operation, my life would have probably settled back to normal long before now. The assumed tide of unimaginable suffering that rests hand in hand with these kinds of situations is rather less dramatic in reality.
Being told you are going to die is a shock, but I was largely over it in a week, and as for breaking the news to friends and family around me, the guesswork on my part of trying to assess the other person’s emotional fragility, their guesswork at trying to assess mine, and the background danger – perhaps felt by both of us – that your partner in conversation is about to break down in tears, made the experience not so much sad as really quite awkward.
This isn’t to say that it hasn’t been an intense few months, but I can’t say that this experience has truly changed me as a person. People have told me how well I’m coping and how they couldn’t have done the same in this situation, as though I’ve faced an unimaginably horrendous set of circumstances and managed to do the impossible (remain positive), but I don’t see it that way.
While I understand why it may feel like that to those looking in from the outside, dying of cancer, in my experience, has been a succession of hospital visits, a lot of pills, and one or two pieces of bad news. But after that, there is an inevitable return to the way you were previously living. Pretty soon I came to realise that it doesn’t make any difference if you’ll be dead in 10 years or two months; you still get up, have a shower and make a cup of tea.
OK, so there are drawbacks – in my case, largely a lack of movement. After the operation on my spine, I was all but paralysed in my dominant hand, movement was compromised in the other and I could barely move my legs, all of which meant I could no longer write, walk, or play the guitar and clarinet. These limitations didn’t seem to matter when I was still in hospital, but as I left bed eight, ward 27 and returned home, I was confronted by all I could no longer do. At first, when the seriousness of my illness was still a new and shocking discovery, the issue of not being able to walk to the toilet seemed dwarfed by this drama, and it was only later that these kinds of problems started to irk me.
Nonetheless, I’ve found that these problems start to sort themselves after a while. For example, I was at first stretchered around the hospital. As my mobility improved, I spent more time in a wheelchair, which at least gave me the luxury of seeing where I was going. Currently, I walk with a stick, which of course resolves many difficulties, and I can now eat at a restaurant without having to sit half a mile from the table because the wheelchair won’t fit underneath.
Where there hasn’t been a significant improvement, such as in my right hand, I’ve tried to make up for the problem. Unable to play any instruments that require two hands, I’ve begun learning the blues harmonica (which only requires one – at least it does the way I play it) and, while practising writing left-handed, I now type on a touchscreen phone, this being how I continued to write my weekly blog and my recently published book. In addition to this, I’ve continued to write songs and music by composing on the computer. I suppose I can at least be glad to live in an era when technology makes this possible.
Religion has featured a lot in discussions since the diagnosis. I am told that many people are praying for me and I have prayed myself, though I never thought it would make a difference (I only did it on the off chance that something positive might happen – what’s to lose?). I don’t believe in God; I didn’t before my diagnosis and I don’t now. I can see how some in my position may want to turn to religion as a comfort, and I can also see how many may become disillusioned or even angry with the God they thought they believed in. But I have done neither. Most of my frustration has fallen on nurses and medical staff for the most trivial of reasons.
Max Edwards with his sister Esme, 14, and brother Toby, seven, decorating the Christmas tree, 2015.
As for comfort, I don’t feel I need comforting. The initial shock wears off very quickly, and after that, life seems to become quite ordinary. The satisfaction of daily routines is enough in the way of comfort.
One thing I have started to do is measure time in distinct chunks. Ordinarily, I would allow days to blur into weeks, weeks into months and months into years. After my operation, however, I’ve found myself focusing on certain events. A holiday, for example, or a day trip, or a party. Perhaps my perception of time has changed, or maybe it comes from a lack of ways to fill the day, although that’s becoming less of a problem now that I’m more mobile and have been able to get more done, such as schoolwork (AS-level history), which I’ve just restarted.
In terms of where I want to be, my main hopes for the future are life-expectancy-related. This is one thing that still gets to me: I’ve more or less made peace with the idea of death, but it’s the question of when that is still a daunting thought. The (almost) inevitable growth of my cancer means it is likely to come some time soon, but I still don’t know when exactly, and I’m not sure I want to.
Regular MRI scans will probably give me an indication of how bad the situation is as and when that becomes the case, which means there is more bad news in store for me. I considered not having any further scans, but then I’m sure I’d panic with every slight pain or possible symptom of tumour growth, and given that I already interpret a headache as, “OH MY GOD, IT’S SPREAD TO THE BRAIN AND I’LL BE DEAD WITHIN A WEEK!”, I’d rather not venture any further down this route.
I am sure the expectation of death is worse than death itself. True, they say death is the worst single thing that can happen to you, and given that I can’t trick myself into believing there is an afterlife, I imagine it leads only to an empty void, but I’ve found ways to accept such an idea. First, I look on my life, which I believe has been a modest success, and remember that it could not have occurred in any other way. The only possible way I could have had my unique set of experiences is by living my life as it is, and that means dying when I die. Even if I’m wrong, and there has been more unhappiness than I care to remember (rendering my life “unsuccessful”), death – the absence of pain or pleasure – should then logically be seen as an improvement.
I also remind myself that the experience of dying is not unique to me. Whether it happens aged 16 or 95, experiencing the end of everything you know is the same process – it’s just that I and those around me are forced to come to terms with this fact prematurely.
Finally, I feel it has helped to process the whole issue selflessly. Some people might find it helpful to know that they are loved, that people care about them and that they won’t be forgotten when they die. I can understand this and I see how it’s comforting, but I also find it consoling to take the opposing view: stop dwelling on personal suffering and carry on as before.
This approach seems to help deflate the hype that terminal diagnoses carry. Pity, grief and sympathy are all natural emotions, and they certainly have their place, but I’ve found the message of “Stop whining and get on with it” far more effective. Stoicism, I feel, is more effective than grief: a simple reality-check helps to set my perspectives in place.
It helps to remind myself that even if I’m dying, it’s not all about me. At the end of the day I’m one in seven billion, a number that – like my cancer – will continue to grow and multiply over the coming months and years. While my life may be all I know, I’m nothing more than a dot on this planet. When you take into account the dozens of people I know, the billions I don’t, the thousands of miles that separate us, and the ever running river of time on which we all finitely float, you may come to the inevitable and strangely comforting realisation that we are all going to die: me, you and everyone else. Get over it.
The writer Anita Brookner, who has died at the age of 87, requested that no funeral be held after her death. How common is this and what does it mean for friends and family?
When someone dies, the UK government’s advice is given in three simple steps. First, get a death certificate from a GP or hospital doctor. Second, register the death. Third, arrange the funeral.
But the writer Anita Brookner, best known for her 1984 Booker Prize-winning novel Hotel du Lac, requested that step three didn’t happen in her case, her death notice in the Times saying: “At Anita’s request there will be no funeral.”
This type of ending, where a coffin goes straight from the place of death to the cremator, where it is burned, is known as a “direct cremation”.
Catherine Powell, customer experience director at Pure Cremation, which offers services for England and Wales, estimates that 2,000 people a year are now making this choice.
The most common reason, she adds, is to enable a more “celebratory” event, such as a summer beach party or function at a golf club, to take place weeks or months later. However, some choose it for financial reasons – a direct cremation, including transport and coffin, costs just over £1,000, whereas an average funeral costs £3,600, according to research by Bath University’s Institute for Policy Research.
A direct cremation involves a company moving the body from a hospital, hospice or home to the crematorium. As with a conventional funeral, the coffin travels along the aisle of the chapel to the cremator, but no ceremony takes place.
However, families and friends can come to watch the coffin’s procession. They can touch it and request music to be played. One woman who attended alone “sang her heart out”, says Powell, while the procession of one man’s body was accompanied by his two daughters performing “air guitar”. But there is no eulogy or other ceremonial aspect.
Some Christians have used the direct cremation service, in one case with friends of the deceased reciting scripture as the coffin passed through the crematorium. A religious memorial service took place months later.
UK funerals, in which mourners traditionally have worn black, have become less conventional. In some cases there is now a party theme, with attendees dressing up as, among other things, clowns, Vikings and Dr Who characters. Some might regard this as flippant behaviour, but supporters say they involve thoughtful, personalised ceremony – a tribute and a send-off.
The US-based website What’s Your Grief offers “guilt-free alternatives” to funerals. These include erecting a “shrine” – a collection of photographs and mementos – in the home, holding birthday or anniversary memorials, planting a tree and setting up a memorial book. Of course, all of these can, and often do, happen if the deceased has a funeral too.
“What we offer isn’t a cheap funeral – it’s a simple cremation,” says Powell. “That’s not right for everybody, but it allows the later remembrance to be more personalised and planned. Often there’s no time for some relatives and friends to get to funerals, so it gives them a chance to attend a memorial when one takes place at a better time. It offers more flexibility.
“The body is the part of the funeral process that people find most difficult to deal with. This takes away that worry for people.”
A central question is whether seeing the body (in an open casket) or at least having it in the same room as the mourners is important. In recent years it’s become more common to refer to a corpse as “just a shell”, wrote William Hoy, clinical professor of medical humanities at Baylor University in Waco, Texas, but he questioned how widely this is actually believed.
He cited the concept of “liminality”, described by the early-20th Century anthropologist Arnold van Gennep – that the immediate period following physical death is a “threshold” in which people aren’t sure whether to describe them as dead or alive.
“The bereaved need support in two months, to be sure,” Hoy wrote, “but they most certainly need the support of personally meaningful ceremonies in the early days after death.”
There are no centrally held figures on funeral – or non-funeral – types in the UK, but the National Association of Funeral Directors estimates that direct cremations and the rarer burials without ceremonies follow less than 3% of the 480,000 or so annual deaths.
“This is largely because, despite high-profile examples such Anita Brookner and David Bowie, as a society we generally view the act of a committing a body to the ground or to the flames as a central part of the funeral service,” a spokeswoman says.
She acknowledges that those who opt out of funerals usually do so for personal rather than financial reasons. “While a funeral can be extremely distressing,” she says, “it can also be an important part of the grieving process for those left behind and so providing an option to allow people to come together in another way might be an important consideration in the planning process. ”
Brookner, who nursed her own mother until her death in 1969, said she had read the Bible as a child but had decided there would be “a lot of questions and no answers”. She described herself as a “pagan” and supported the use of euthanasia.
The author, who taught at London’s Courtauld Institute of Art and was the first woman to hold the Slade Professorship of Fine Art at Cambridge University before becoming an author, never married or had children.
It’s not been revealed whether she planned for her friends and family, and many thousands of fans, to hold a celebration of her life at a later date.
Dawn Gross interviews her first mentor, Jeffrey Mandel, a hospice and palliative medicine doctor, during the launch of her radio show Dying to Talk.
Dawn Gross ’89 knows how to talk about death.
“I’ve asked hundreds of terminally ill patients, ‘If I had a magic wand, what would you wish for?’ And not one of them has ever answered, ‘Cure me,’ which is staggering to me,” said Gross, a hospice and palliative care physician since 2007.
Instead, patients respond by asking for something that brings them closer to who they truly are, she said, whether it’s being with family or spending time in their gardens.
Gross, who earned her bachelor’s in psychology and neuroscience from the USC Dornsife College of Letters, Arts and Sciences, has years of experience supporting patients with life-threatening illnesses in their own homes. She is currently a member of a hospital-based palliative care team at the University of California, San Francisco.
Just listen
Her first job, she said, is to listen.
“People have a hard time articulating or even knowing what is most important to them when they’re struggling with uncontrolled symptoms,” she said, “whether it’s nausea, difficulty breathing or pain.”
Once those symptoms are brought under control, she helps patients plan their goals of care and helps them identify and realize what they really want to do with the time left to them.
Gross said she’s profoundly grateful for the opportunity to practice her chosen specialty.
“It’s not depressing,” she said. “It is sad, and I think to untangle the two is important for people to do. But what we do — being with people and supporting them in the things that matter most in their lives — is a gift. I fall in love with people immediately, so when they die, am I sad that they die? You’d better believe it. But what I’m left with is immense gratitude for having gotten to know them and be part of their lives, and hopefully for helping to make their lives the way they wanted.”
A new openness
In January, Gross began hosting Dying to Talk, a public radio show that aims to revolutionize the way people discuss death.
“People are averse to talking about death, but I’ve noticed that once you give them permission to do so, they really are dying to talk,” she said.
“It’s really exciting to have now been given a platform to try and make this conversation accessible to people in an unintimidating format that can also provide anonymity.”
Many forums now exist worldwide for conversations around death, including so-called “Death Cafes,” which bring total strangers together to sit down and discuss death. Gross noted that The New York Times recently ran a year-long series of op-ed pieces and stories about death titled “The End.”
“If you a look at any media outlet, there’s an article every week about death,” she said. “To me that suggests people are eager to talk about it and now we’re giving them permission to do so.”
A very personal inspiration
One of her greatest inspirations in pursuing a specialty in hospice and palliative care was her father, who had always been clear he wouldn’t seek aggressive, curative therapies to prolong his life. When he became terminally ill, he questioned traditional care options, asking, “Why is no one asking me what I want?”
Although her father was eventually able to die in his own home under hospice care, Gross said he taught her to want to ask those questions and to help the rest of the family try to listen to what he needed.
“Watching how my family learned to accompany him on his journey was eye-opening and made me more curious about how to support patients and families at such times.”
Alumna Dawn Gross’ love of end of life conversations shaped her decision to specialize in hospice and palliative care. (Photo/Gurusurya Photography).
While her father was sick, Gross’ mother was simultaneously confronted with a very serious illness.
“My mother has a very different approach to her life and therefore a very different outlook and approach to how she will die,” Gross said. “Seeing these two very different ways of navigating life has given me permission to discover new ways to raise this conversation.”
A fairy godmother
Born in Northern California, Gross spent her teenage years in Portland, Ore. After tagging along on a college tour of USC with her older brother, she decided she liked the university. At age 16, she joined her brother at USC as a resident honors scholar in her senior year of high school.
“I was intrigued by science but always hated the sight of blood,” she said. However, in her freshman year, she chose a biology option, “Introduction to Neuroscience: Man, Mind and Machine” taught by William McClure, now professor emeritus of biological sciences.
“I remember my first day in that class. Professor McClure began to map out on the board how the brain works. I was hooked immediately.”
Admitted into the psychology honors program, Gross focused on neuroscience research, helping map the circuitry of memory. She did a post-baccalaureate premed program at Mills College and an M.D., PhD at Tufts University in Boston.
“I wanted to be a scientist,” she said, “but medicine snuck up on me. It wasn’t until I was in fellowship at Stanford, training in hematology and bone marrow transplants that I realized I loved being a physician because I loved having end-of-life conversations. That was something completely unexpected, and it shaped my decision to go into hospice and palliative care.”
End-of-life conversations are something that many doctors — trained to heal, not to discuss death — find difficult. Why does Gross cherish the experience?
“In my USC admission essay, I talked about wanting to major in psychology and inspire people to reach their highest dreams and then reach higher still,” she remembered. “Now, that’s all I do everyday. I see myself as a fairy godmother. When you’re facing your own mortality, what becomes essential rises to the top and everything else melts away. All you’re dealing with then is what matters most. It’s an extraordinary conversation to get to be a part of.”