Because it’s time to start thinking about death differently.

[W]hen Victoria Chang’s mother was diagnosed with pulmonary fibrosis, she didn’t have a single person she felt she could turn to. Six years earlier, her father had a stroke that led to significant neurological changes, and now the young poet realized she alone would have to care for them both. None of her friends had sick or elderly parents, so she felt completely isolated.
What followed was a decade of navigating America’s imperfect end-of-life health care system, without much guidance from the doctors and specialists she so frequently encountered. When asked what she would have done differently over the course of the stressful years, Chang says, frankly, “Everything.”
“Everything was a learning curve, everything new,” she says, noting how she wished there had been more help for people like her. “Emotions were high, and we needed a case manager or a consultant or something. Hospice seemed to help, but in the end, there was only so much they could do.”
Chang’s experience caring for seriously ill loved ones is sadly not unique. Thanks to a combination of denial, a lack of know-how and flawed systems, most Americans don’t have the support they need when it comes to end-of-life care. According to a study by the California HealthCare Foundation:
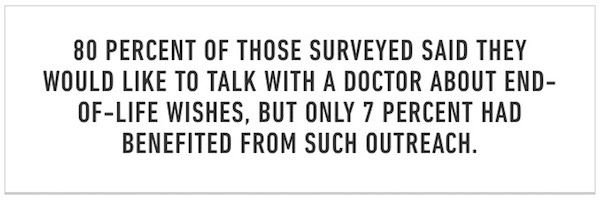
Furthermore, a majority of those surveyed had not even communicated their end-of-life wishes to the loved one they would want making decisions on their behalf. That’s where Dr. Ira Byock, chief medical officer of the Institute for Human Caring at Providence St. Joseph Health, comes in. A renowned expert in palliative care and the author of The Four Things That Matter Most: A Book About Living and The Best Care Possible, Byock wants to reimagine health care as a more personal, approachable system. He wants to boost the person-to-person communication and eradicate denial — an approach he and his colleagues call Whole Person Care.

“[Whole Person Care] attends not just to your medical problems, but to your personal priorities, values and preferences,” explains Byock. “You’re someone with bodily needs but also have emotional, relational, social and spiritual parts of your life, all of which need to be attended to.”
This perspective may not seem all that radical, but it is clearly not the current practice. American medicine is good in that it’s a “problem-based system,” Byock says. “It is organized around your problem list on your chart. Everything we do, by design, responds to a problem on your list.” But life isn’t just a set of problems to be solved; patients have lives that extend well beyond the walls of hospitals and waiting rooms. Health care, in Byock’s opinion, should address this reality at all stages of life.
Perhaps most importantly, Whole Person Care includes patients’ families at every level of care. Byock emphasizes the significance of the familial role in a patient’s comfort, as well as the ripple effects of a single individual’s illness on loved ones and their network of relationships. “Whenever one person gets a serious diagnosis, everyone who loves that person shares in the illness. It’s a family and community issue.”

Chang, for one, can attest to the need for a system like Whole Person Care. “Looking back, I can’t remember the past decade because I was so busy helping everyone around me,” she says.
When asked what advice she would give to those caring for a family member or spouse dealing with a serious illness, Chang emphasizes the importance of self-care and finding community support in whatever form that might take. Remember that “it is OK to think about yourself and to take care of yourself,” she says. “Seek out groups to share with and to get emotional support. I only did this toward the end when I started reading about and writing to people on the pulmonary fibrosis foundation website. Those forums saved my life.” She also encourages folks in similar positions to consider their options, including daycare, homecare and facilities, and weigh the pros and cons of each.
Byock also encourages those faced with these situations to manage their own health: “People can experience wellbeing even in the midst of serious illness.”
Complete Article ↪HERE↩!