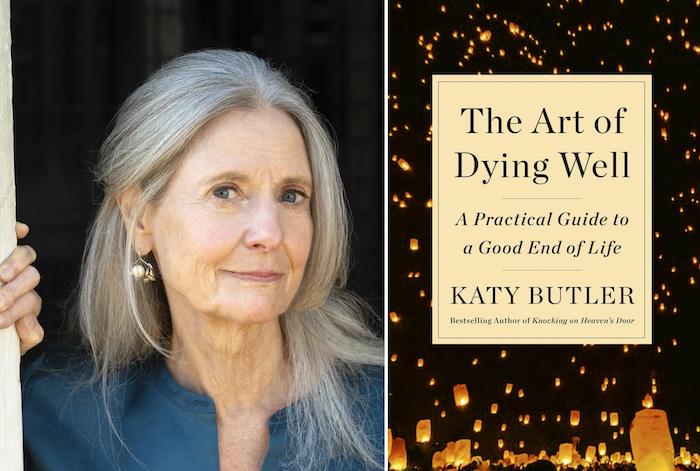
I have to confess that I am a Katy Butler fan. When I started the journey to become an End of Life Doula, her Knocking on Heaven’s Doorwas one of the first books that I read. I didn’t so much read the book as devoured it, often catching a sob in my throat as I read her deeply personal account of the horror show that became her fathers final years. I admired the courage and honesty of the parts of the book that were memoir, and the research on the current culture of American healthcare with respect to death. I agreed that our way of dying in the good ol’ USA has come to leave something to be desired.
In her newest work The Art of Dying Well – A Practical Guide to a Good End of Life, Katy picks up the narrative in a new and accessible way. She divides the process of moving toward the end into seven unique segments defined not so much by age but by ability and functionality. At the beginning of each of these chapters she has a list of statements and suggests that if many of these apply to you now, this might be where you find yourself. I found this approach fresh and, best of all, non-threatening. This might be just the way to start a conversation with a unwilling family member.
In the first segment, aptly titled Resilience, we learn that in this stage of well being we can still dramatically impact our health, longevity, and ultimately the quality of our death. By building reserves (aka altering what we eat and whether we’re active enough), finding allies in preventative medicine, and increasing our circle of friends and acquaintances, we are still in the drivers seat with regard to how things will go for us as our situation changes. This perspective gives lots of practical advice for those who may think there is plenty of time.
With each ongoing chapter comes an inevitable decline – not according to any decade of life or disease process – but according to naturally decreasing functionality. I like that she is careful to follow this definition, as people age as they darn well please, and I personally know 90 year olds who are still more capable than I am. This lets you find your home page, so to speak, without feeling like a failure or self fulfilling a prophecy to act your age. Every chapter offers practical advice; about healthcare, money, housing, and all those pesky details like advanced directives and wills. In nearly every chapter there are personal accounts of folks who managed things well, or not so well, and lots of food for thought.
There was a great deal of material that wasn’t new to me, but I work with dying people. In my every day life, I am always shocked at how hard working, responsible people don’t bother with a will or advanced directive… because? They aren’t going to die? Or they’re not going to die tomorrow? This book may be just the ticket to get you going, or to give to that parent who is dragging their feet about preparing for anything. With a helpful glossary and pages and pages of useful references included, this will certainly be a ‘go to’ book in my personal library and in my practice.
* Special correspondent, Trish Rodriguez, is an End of Life Doula and hospice vigil volunteer in Anacortes, WA.
Palliative care is a growing specialty that provides comfort care and that teaches patients and doctors how to talk about patients’ goals for life with serious disease and how to prepare for a good ending.
That’s what the family of a patient told Sunita Puri when she was a resident in internal medicine. They were chilling words for the young doctor as she took over the care of a very sick man on the overnight shift.
To Puri, the patient, who had widespread metastatic liver cancer, appeared to be dying. She tried to talk with the family about forgoing heroic measures, to let him have peace in his last hours. But they were adamant.
“Do everything,” they told her. Hours after admitting him to the intensive care unit, she was overseeing chest compressions to revive him after his heart stopped. “I was blinking back tears,” she recalls. The man died that night.
Few people would say they want to die while undergoing painful last-minute resuscitation or while hooked up to machines in a hospital. Yet it’s the death many Americans end up with. Now a palliative care doctor at the University of Southern California, Puri is fighting for an alternative.
In her new book, That Good Night: Life and Medicine in the Eleventh Hour, Puri writes about how palliative care specialists are working to change medicine from within — teaching other doctors how to talk to patients about their hopes and fears, not just their disease and treatment. Palliative care, she says, gives doctors, patients and their families a new vocabulary with which to talk about the way life’s goals can shift when you have a serious illness and how to plan for a good final chapter.
We spoke with Puri about the field of palliative care and what patients need to know.
This interview has been edited for clarity and length.
What is palliative care, and how is it different from hospice?
Palliative care is attending to the physical, emotional and spiritual suffering of patients and families who are dealing with a serious illness. Hospice is a type of palliative care that we provide in the last six months of life. And I would say hospice is even distinct from end-of-life care, which is really the care of patients in the last days and hours of their lives.
In our country, hospice is overwhelmingly provided in a patient’s home or in a nursing home, whereas palliative care is available at any stage of an illness. And so we can see people in the hospital; we can see people in clinics when they come to see their oncologist or their cardiologist. With palliative care, you can have us on your team just right alongside care like chemotherapy or dialysis — we’re meant to attend to your quality of life. And in an ideal circumstance, we will be there when you decide to transition to hospice.
How common is it now to have palliative care specialists available?
There’s actually very few of us, and many of us are concentrated in the big cities. So in rural areas or in nonacademic teaching hospitals, there’s definitely a shortage of palliative care docs around the country. Our presence and the need for us is growing though. So for example, the American Society of Clinical Oncology now has a recommendation that at the time of diagnosis of a serious illness, palliative care should be involved. Patients with a serious illness can ask for a consultation with the palliative care team if their other care providers don’t bring it up, either in a hospital or a clinic setting.
We have studies that show that for patients with, for example, metastatic lung cancer, if they got palliative care right alongside their cancer treatment — as opposed to just getting cancer treatment alone — the patients actually lived longer and had better quality-of-life scores.
What other advantages does palliative care offer?
I think the emotional and spiritual aspects of it are actually some of the most important supports that we can offer our patients.
One thing my patients tell me a lot is, “Thank you for listening.” And I think there is something about our field — focused on being silent and listening to people — that is deeply therapeutic for the vast majority of my patients. To say, “I’m going to be with you through this whole journey, no matter what the outcome with your treatment, and work with your other doctors to make sure we’re all on the same page about what therapies may or may not actually be helpful to you in the way that you define helpful.” I think there’s something pretty magical about that.
You wrote that when you found palliative care, you were finally able to become the kind of doctor you wanted to be. What did you mean by that?
I grew up the daughter of an anesthesiologist — she was always my first model for what a doctor should be. My mother is very technically skilled, but she is also deeply devoted to the idea that every human being is kind of an embodiment of the divine who she felt she was in service to. So, she really had this beautiful intertwining in her practice of being very scientific but also being very spiritual — being able to take people to the operating room and control their physiology to get them through an operation but also understanding that the body and nature has its limits.
And that’s what I wanted to be: somebody with the technical and scientific command of medicine but who understood that every human life is different from the other. In my medical training, there were so much focus on the technical and scientific aspects. But as I was learning those things, I was not also learning how to talk with someone who has a serious diagnosis. How do you explain to them how their life might change? How do you ask, if this is not something that we can cure, “What would be really important to you in the time that you have?” And this language was not given to me in medical training.
When people get a diagnosis like cancer, they sometimes talk about “being a fighter” or “fighting the disease.” Why do you find that kind of language problematic?
When we think of disease as a battle to fight, you kind of divide people into winners and losers — which is not a mentality I think benefits them.
What’s dangerous is that when we’re talking about a fight, if someone chooses not to “continue to fight,” then people will often tell me, “I feel like I’m giving up.” I have to reframe that for them to say, “You may be a fighter, but your body cannot fight this anymore. Can you hear that distinction between you and the natural limits of your body?” I have found that to be incredibly potent because people can see that this isn’t a personal thing.
You know, you did not deserve to get this horrible bout of heart failure, and your not “beating it” is not your fault.
What are the consequences for doctors and for the patient’s treatment of using this kind of language?
I think people feel an obligation, if they identify as a fighter, to keep trying any and every treatment offered to them — sometimes without a full appreciation of the risks of those treatments or whether those treatments might keep them in a place they don’t want to be, like an intensive care unit, instead of having the opportunity to go home. I think that sort of “fight or give up” mentality is such a toxic binary. And I’ve seen people suffer tremendously because they felt that if they said no to therapy, that they would be letting other people around them down.
From my perspective, when I was in my residency, when I heard those words, I then felt obligated to offer anything and everything to the patient or family — even when I knew that certain treatments were not going to help them but could very well hurt them. So I think hearing those words almost put a stop to any real in-depth conversation about what someone is hoping for and what realistically we as physicians can offer them to fulfill those hopes.
I still regret the ways that I offered therapies to patients that I knew would not be in their best interest. But I didn’t know how to talk about another way when I was in my training.
What kind of therapies might be harmful or not be in their best interest?
Being in a clinical trial is one example of a therapy people often feel they need to take but may not truly be in their best interests if it, for example, requires them to uproot their life and go elsewhere. Or if it has side effects that we may not really know about, because part of the trial is to figure out what the toxicities are.
And the other scenario I’ve seen is people in the ICU with an overwhelming infection or a set of post-surgical complications, and they’re suffering one complication after another, especially if they’re elderly. And we can keep trying to manipulate their physiology, using very powerful medications and machines, but we’re not always as attentive to what someone’s life would actually look like if we were successful in reversing some of the problems that they’re going through.
So when a palliative care team is involved and you have these kinds of difficult discussions early on in a serious diagnosis, what can a good outcome look like for the patient?
The advantage of getting to know people and their family early on when they first get a diagnosis is that we can really help them through their treatment. To think about and articulate what’s most important for them if a specific treatment doesn’t work or if it takes a huge toll on their quality of life. And when we can have those discussions, then a happy ending might be that they have their pain, their shortness of breath, their nausea, all of those things exquisitely well controlled. And they decide on their own terms when to transition, for example, to hospice.
When I was a hospice doctor, I think the best situations were when people were still able to be themselves and participate as much in living as they could — even though their bodies were failing. They could still be cognitively intact. Their symptoms were well controlled. They were in a place they wanted to be in. They were living their lives on their own terms for however long they had. And that to me is what a good ending can look like.
Even other doctors don’t always understand what palliative care is or embrace it. What do you think the obstacle is?
I think doing what we do in our field is a little bit of the rejection of our culture’s idea of what medicine exists to do. I think the public thinks of doctors as heroes that can beat diseases and extend lives. And in many important ways we are heroes. Surgery is safer. Childbirth is safer. We’ve eliminated certain infectious diseases almost entirely because of vaccines. But I think we are not good at knowing what to do when we can’t fix a problem.
For patients who have a terminal diagnosis, what advice would you give about how to decide whether or not to opt for some of the more extreme life-sustaining measures, like going on a ventilator or a feeding tube?
In planning ahead, I always encourage people to think about the quality of life that they value. What are the things that they would be OK not doing? And what are the things that if they couldn’t do them would make their life extremely difficult — maybe even not worth living? And if people can think about their values and their goals in broad strokes, the broad strokes can help inform the more specific question about CPR or a ventilator.
I encourage families to really look to their doctors to guide them. And to say, if there’s a question about going on a ventilator, “Is this for a reversible condition, as far as you can tell, doctor? Or am I taking a gamble, a big enough gamble that he may be stuck on the ventilator forever, and then I would have to make the decision to stop? Tell me more about that.” I think being able to ask your doctor openly and not feel alone in making some of these weighty decisions is extremely important. So there are those two components of it: thinking yourself, “What is the sort of life I value? What would be a life that would be too hard for me to live even with the help of medicine?” And to talk to your doctor, even if you’re healthy right now, because you want to prepare for the storm.
I am a gynecologic oncologist and I’m boarded in palliative care. As a result of my training and 20+ years of clinical experience, I feel strongly about caring for the whole patient throughout the clinical course: spiritually, emotionally, and physically. In those 20+ years, I have experienced the end of life with many patients and families. Although everyone handles it differently, I’ve observed some common themes. It is difficult to stop treatment, to accept the inevitable with dignity, to die “well”—not just for the patient and her family, but for her providers as well.
This past Christmas, I experienced the death of a loved one both as a family member and a health care provider, acting in the stead of the health care providers who were absent at the end of life. The experience of my father in law’s passing brought home to me that inappropriate aggressive measures at the end of life are not limited to patients with cancer, but affect us all.
I met my husband when we were freshmen in college, and we spent a lot of time at his father’s home together. My husband has a big Catholic family who are all rabid Eagles fans; I am a Jewish liberal girl raised on the Boston teams. They accepted me unconditionally. I shared Sunday dinner with his family, brought my laundry over, watched movies on his dad’s TV. When my husband and I were married in a Jewish ceremony in Boston, everyone in his family came to the wedding and thoroughly enjoyed the ceremony and dancing the hora at the reception.
My husband’s family, and particularly his father, were an important part of both of our lives. My father-in-law, Ron, was a philosophy professor and a brilliant man who loved to argue (he would say debate) with his children. While he and I disagreed about many things, I never felt judged by him, or by anyone else in the family.
In the last few years, I could tell that Ron was sick, but he was private about the details and I didn’t pry. I did know that he had multiple stents placed in his cardiac vessels. This past year, though, there had been a significant deterioration in his condition. He had to stop golfing due to fatigue, and he was in and out of the hospital with shortness of breath and chest pain.
In December, I visited the community hospital where Ron was receiving care; his third prolonged admission in as many weeks. I found him sitting in a chair wrapped in a heavy blanket in an overheated room. He had lost a lot of weight and looked frail. He had to lean forward to breathe. A few weeks before my visit, he had undergone another cardiac catheterization (there was nothing more to stent) and a renal artery catheterization that showed bilateral significant occlusion.
Ron told me he expected to get better and get back to the golf course. I told him I wished for him to get well enough to go home and stay out of the hospital.
I had spoken to his wife on the telephone before the renal artery catheterization. I talked with her about requesting a palliative care consult as Ron was clearly suffering. We discussed the hard questions I was hoping would be addressed. I don’t know if she asked these questions. I do know that the doctors convinced her that the renal artery catheterization might help him. I know that they didn’t offer a palliative care consultation and I know that they didn’t tell my in-laws that Ron would not get better—that his current state was the best they could hope for.
On Christmas morning, my husband and I received a panicked call from Ron’s wife. When we arrived, he was clearly in distress. An episode of melena (that apparently wasn’t new) needed to be managed urgently. I spoke to his primary physician on the phone, who suggested we bring him to the ED. I asked him if the ED was the best decision; wouldn’t hospice be a better option? Yes, he said, it would. In fact, he said he had been thinking about this for the past two months. This revelation shocked me. Why, I asked him, had he not said anything to the family? Why was he continuing to recommend and pursue aggressive care in this 81-year-old man who was clearly declining? There was no good answer to this question.
And so it fell to me to tell Ron’s wife that he wasn’t going to get better, and that she had to make a choice: take him to the ED, where he was likely to be admitted to the hospital for another prolonged—and futile—stay, or keep him at home and call hospice. I will admit that I supported avoiding the hospital, and for better or worse, I influenced that decision.
I talked to Ron that morning during the intermittent periods that he was awake. He asked me how I knew he was dying. (A good question, but I just knew, an instinct honed over two decades of caring for patients with cancer.) He seemed genuinely surprised to hear that his condition would not improve. He told me he wasn’t ready to die, he had a lot of things left to do. (I asked him to make a list, but he couldn’t stay awake long enough to accomplish this task.) He said he was afraid. He had only that one morning to process impending death, and he never really got to say all of his goodbyes.
Ron died early that afternoon. I was with him. His death was peaceful. He was in his own home, surrounded by his (completely oblivious) grandchildren. It was what we call in medicine a “good death.”
But his family was angry. They weren’t prepared, they hadn’t known, they didn’t realize it would happen so fast. For the most part, they had all believed that he would get better. More than half of them didn’t make it to the house to say goodbye before he died.
I was angry, too. I was furious at Ron’s care providers that day. They never communicated clearly with him or his wife that he was dying, that his chances of getting better were slim. They didn’t discuss quality of life or goals of care. They offered aggressive procedures that were potentially life shortening and unlikely to be helpful, and the family didn’t feel empowered to decline. Their approach was the opposite of everything I believe in as a palliative specialist, an oncologist, a fellow human being.
Unfortunately, this type of aggressive care at the end of life happens often. We live in “a very peculiar, death denying society.”1 As providers, we spend far too much money on procedures at the end of life (chemotherapy, ICU, catheterizations) that are unlikely to benefit our patients, and in fact are likely to decrease quality of life and hasten death.
Why do we do this? Are we afraid to tell patients the truth? Are we reluctant to admit to ourselves that sometimes medicine has nothing more to offer and that death is unavoidable (for all of us)? Maybe it feels too much like failing to say that there’s nothing more we can do, even when there are other options (such as palliative care and/or hospice) that are far preferable to aggressive medical procedures and prolonged hospital stays.
A few weeks after Ron died, his wife called me. She wanted to talk about the decision we made to keep him home. She wanted to know if this was the right choice: if she had taken him to the hospital that day, would things have been different?
I told her honestly that yes, things would have been different—they would have been horribly worse. Ron would not have lived longer, and he certainly wouldn’t have died at home, in his bedroom, in his recliner, surrounded by his family. We could have painfully prolonged the dying process, by a few hours or a few days at most, but we could not have stopped it. She had made the right decision.
Here is the fact that we cannot avoid: We are all going to die. Whether we cheer for the Eagles or the Patriots, whether we are philosophy professors or medical professionals (yes, even us). I believe it is fair to say that most of us want to die that “good death,” surrounded by our family and friends, not attached to machines in a sterile hospital environment.
As providers, we must take that extra step to be honest with our patients and prepare them for the truth. To do less—to gloss over the inevitable end of life and deny them the opportunity for a good death—is to do our patients a profound disservice. For myself and for my family, I hope that our own health care providers will be honest with us about what medicine can and cannot accomplish in improving all aspects of health.
My pain at losing Ron is mitigated in a small way by knowing that I helped to spare him from discomfort and loss of dignity in the final hours of his life. I am so glad that, as a palliative care provider and cancer physician, I had the training and experience to do this small thing for the man who welcomed me so wholeheartedly into his family.
But she says that fear of those late-stage declines can prevent us from helping our loved one make the most of the days when they are still able to spend time with family and friends, enjoy activities, and be part of the wider world.
Powell is the director of the Montefiore Einstein Center for Bioethics in New York and her expertise includes dementia treatment and end of life care.
Powell’s own grandmother and mother died from dementia. In her research, she came across a phrase that resonated with her: Every remaining day should be a good day.
“I love the sound of that,” she says.
Here are seven ways you can help your loved one with dementia find joy in their remaining days:
1. Look forward, not back
So many people are grieving the loss of the person their loved one used to be. “We think, ‘This is so terrible, my mother is no longer a great mathematician,’” Powell says.
As difficult as it is, you need to try to accept that your loved one isn’t the person they once were and try to embrace who they are, she says.
When you’re focused on who your loved one used to be, you can inadvertently shame them. If you say things like, “That’s not like you,” or “You don’t need help with that” you can end up embarrassing your loved one, she says.
2. Think beyond safety
When your loved one is in the earlier stages of dementia, you may think they can safely stay home alone. But safety isn’t the only concern. Your loved one might be spending hours staring out the window or watching TV.
“Family members get into denial and don’t want to address the fact that it’s not really okay to leave them home alone all day,” Powell says.
You don’t necessarily have to look at residential placements. Your loved one could get out and do things with other people in a day program a couple of times a week, she says.
3. Get care for other medical conditions
To help people with dementia get the most out of every day, it’s important to make sure other medical conditions are well controlled.
A family member or companion might need to accompany your loved one to medical appointments.
That’s because a person with dementia might not accurately report problems. They may forget that they fell recently, or not notice that they are getting out of breath more easily than they used to.
And, a person with dementia might forget what the doctor says. If their doctor changes their medication, for example, they need to remember to both stop the old prescriptions and start the new ones.
“They need someone to be external memory for them,” Powell says.
4. Boost joy with good food
“Food is often one of the last remaining pleasures,” Powell says. Plus, food can be an important part of family celebrations and culture. She feels that as people with dementia age, it’s time to lighten up on the food rules.
“If I’m 94 and have dementia, I don’t really care about my cholesterol,” she says. “I want to order up an ice cream sundae if I feel like it.”
“When you’re younger and worried about protecting your cognition, I think it’s appropriate [to make healthy food choices],” she says. “Once [dementia] is moderate to severe I would not overly restrict. I think then you can make some tradeoffs.”
5. Help them keep moving
“Exercise is one of the few things that everybody agrees helps prevent speeding of cognitive delays,” Powell says. “And it’s another way to get that happy feeling.”
My mother used to be addicted to the thrift store. She went every week for no purpose other than to browse for deals. Of course she found deals, being the shrewd and careful shopper that she is — gold earrings, fine china sets, silverware, high-quality linens, kitchen appliances, to name a few. The problem was that these deals came home. They filled the house, packing shelves and occupying counter space, to the point of feeling cramped.
Several years ago, I said to my mother in frustration, “It would be a nightmare to have to deal with all this stuff if you died tomorrow.” She looked at me, stunned. Up until then, I suspect she’d assumed that everyone appreciated her junk-treasures as much as she did. What ensued, mercifully, was a house purge. Mom removed much of her stuff and ceased her weekly pilgrimages to the thrift store, avoiding temptation.
That conversation revealed to me the importance of discussing the long-term intentions for one’s belongings. If I hadn’t said anything, I suspect it would have been decades before my 50-something-year-old mother realized what a burden her stuff would be on the family someday — and just think of all the additional things she could’ve accumulated in that time. It makes me shiver.
Enter “Swedish Death Cleaning.” (I’m not joking. This is for real.)
The first time I heard the term, I thought it meant some kind of hardcore Scandinavian house-cleaning routine (they take a lot of things seriously there), where you scour your home from top to bottom to the point of physical collapse, as in “working yourself to the bone.” Well, I was wrong.
The first time I heard the term, I thought it meant some kind of hardcore Scandinavian house-cleaning routine (they take a lot of things seriously there), where you scour your home from top to bottom to the point of physical collapse, as in “working yourself to the bone.” Well, I was wrong.
In Swedish, the word is “dostadning” and it refers to the act of slowly and steadily decluttering as the years go by, ideally beginning in your fifties (or at any point in life) and going until the day you kick the bucket. The ultimate purpose of death cleaning is to minimize the amount of stuff, especially meaningless clutter, that you leave behind for others to deal with.
A woman by the name of Margareta Magnusson, who says she’s between 80 and 100, has written a book titled “The Gentle Art of Swedish Death Cleaning: How to free yourself and your family from a lifetime of clutter.” She says she has moved house 17 times over the course of her lifetime, which is why “I should know what I am talking about when it comes to deciding what to keep and what to throw away”. Reviewer Hannah-Rose Yee, who practiced some Swedish death cleaning herself, describes it as being “like Marie Kondo, but with an added sense of the transience and futility of this mortal existence.”
Magnusson says that the first secret to effective death cleaning is to speak about it always. Tell others what you’re doing so they can hold you accountable. Yee writes: “If you vocalise it, it will come. Or something like that.” Pass on your belongings in order to spread the happy memories.
The second key point is not to fear death cleaning:
“Death cleaning isn’t the story of death and its slow, ungainly inevitability. But rather the story of life, your life, the good memories and the bad. ‘The good ones you keep,’ Magnusson says. ‘The bad you expunge.'”
Finally, Magnusson encourages those engaging in Swedish death cleaning to reward their efforts with life-enhancing pleasures and activities, such as going to watch a movie, spending time in the garden, or eating an enjoyable meal. (Need I say no shopping?)
Who can possibly resist a decluttering philosophy with the name of ‘Swedish death cleaning’? Watch your friends’ eyebrows skyrocket when you pull this one out as an excuse for not wanting to go out next weekend. “Sorry, but I must engage in my Swedish death cleaning routine…”
George and Shirley Brickenden, who are 95 and 94, respectively, decided they didn’t want to wait any longer for death to arrive. They’d been married for 73 years and their bodies weren’t faring so well. Shirley had a heart attack in 2016 and nearly died; she now had rheumatoid arthritis and was in constant pain. George was found passed out, unconscious, on his birthday and his heart was also failing.
Under Canadian law, both of them qualify for what’s known as physician-assisted death. They’re older than 18, Canadian citizens, mentally competent, suffering from a “serious and incurable disease, illness or disability,” and in an “‘advanced state of irreversible decline,’ with enduring and intolerable suffering.” Furthermore, there was no coercion involved. They checked off all the boxes.
And both of them decided to end their lives together, in peace, at the same time last week.
Shortly before 7 p.m., Mrs. Brickenden turned to her husband. “Are you ready?”
“Ready when you are,” he replied.
They walked into their bedroom and lay down together, holding hands. The two doctors, one for each patient, inserted intravenous lines into their arms.
…
Angela rubbed her mom’s feet. [Pamela] rubbed her dad’s. “They smiled, they looked at each other,” Pamela said. Then Mr. Brickenden looked at his children, standing at the end of the bed.
“I love you all,” he said.
This is exactly why the law was passed. Forcing people to live in pain is a form of torture. The Brickendens were able to get their lives in order, say goodbye one last time to their children, and end life hand in hand with the person they love most. If you were to imagine your own perfect death, it would probably look something like that.
And yet there are many religious groups that oppose letting people make that decision because it’s thwarting God’s plan for their lives. They’re so “pro-life,” they would rather see people suffer than die on their own terms. In some cases, like when a dying patient ends up at a Catholic hospital that doesn’t allow the procedure, the result is even more cruelty.
In Canada, however, this is now a legal procedure with sensible hurdles in place to prevent people from abusing it. It was made for situations like these. There may be certain situations where the moral thing to do isn’t always obvious, but this isn’t one of them.
As age and overwhelming infirmities overtook them, on a beautiful spring day, after 73 years of marriage, they toasted each other with family and good champagne, held hands and left this life gently and together, on their own terms. This was their final act of love, hoping their act will pave the way for others who are suffering. They were fully at peace with this decision and had the support of their four devoted children who have always known this was how they wanted it to be when the time came. We are all forever grateful for the compassionate assistance of Dying with Dignity. They have blessed this earth together for 73 years and it’s time for them to bless the stars.
Instead of flowers, they asked for supporters to make donations to Dying with Dignity.
In the United States, death with dignity is only legal in six states and Washington, D.C. That leaves a lot of places where people who are ready to end life are forced to prolong it against their will. That needs to change.
Many of us are so used to living in the past or the future that we have no awareness of what being in the present means. Recent research has shown that we are not as conscious as we think we are. In fact, we are unconscious most of the time as we move about our day, with […]
Many of us are so used to living in the past or the future that we have no awareness of what being in the present means. Recent research has shown that we are not as conscious as we think we are. In fact, we are unconscious most of the time as we move about our day, with only specific decisions making their way into our consciousness. Because of this, we struggle to live in the present because our mind swings from thought to thought, only briefly settling somewhere that captures our truest form of attention. To become more mindful and present in your life, focus on these three areas.
Unselfconsciousness
Thinking about yourself and how you appear to others takes you out of the moment. When in a situation you already feel anxious about, focusing on the anxious feeling worsens it. Instead of focusing on what’s going on in your head, think instead of what’s happening around you and how you are a part of that. Mindfulness blurs the line that exists between yourself and others. Without feelings of self-consciousness, you’re able to witness the passing of feelings and perception of being evaluated by others without feeling threatened and taking it personally.
Savoring
Being so caught up in our thoughts prevents us from truly experiencing and enjoying our own lives. Instead of appreciating what we’re experiencing, we think of when the next time we’ll get to experience this again is or how the experience could be better. Learning how to direct your attention allows you to become an expert at savoring the present moment. No matter what the moment is, take note of how you’re feeling in all of your senses. Taking a few extra minutes to savor daily activities helps you to feel more joy and happiness and fewer depressive symptoms. Savor the taste of food, rather than gulping it down. Savor the feeling of fresh air as you walk to your car rather than re-playing what happened in your meeting. Savor the smell of your favorite cologne, perfume or lotion to bring yourself into the moment. Because the majority of negative thoughts involve the past or future, thinking in the present forces you to stop ruminating on the past and stop catastrophizing about the future.
Acceptance
When faced with pain or discomfort, our natural reaction is to avoid it. Resisting unpleasant feelings and thoughts means you don’t have to face them. Humans have two types of emotions: primary and secondary. Secondary emotions are ones that we feel around other feelings. When we feel stressed out about being busy at work, the primary emotion is the stress surrounding your workload. The secondary emotion is hating feeling stressed. Instead of fighting these emotions, allow yourself to take them in. Be open to how you feel in the present moment without judging your feelings or trying to push them away. Focusing on your secondary emotions instead of feeling your primary ones actually prolongs the negative feelings. Accepting these emotions doesn’t mean you like them and want to feel this way forever. It instead means that there are some things you can’t change, and how you feel right now is one of those things. Accepting your feelings doesn’t mean resigning to them.
Applying these three techniques will help you develop PRESENCE. When you are able to bring your presence to each situation in your life, be it at work, in your relationship, or even when hanging out with friends, the quality of your life experience will increase dramatically.