In “How Doctors Die,” a powerful essay that went viral in 2011, a physician described how his colleagues meet the end: They go gently. At the end of life, they avoid the mistakes — the intensive, invasive, last-ditch, expensive and ultimately futile procedures that many Americans endure until their very last breath.
“Of course, doctors don’t want to die; they want to live. But they know enough about modern medicine to know its limits,” Ken Murray wrote.
A new study reveals a sobering truth: Doctors die just like the rest of us.
“We went into this with the hypothesis we were going to see very large differences,” said Stacy Fischer, a physician who specializes in geriatrics at the University of Colorado School of Medicine. “What we found was very little difference to no difference.”
The study in the Journal of the American Geriatrics Society examined 200,000 Medicare beneficiaries to bring some hard data to the question. They found that the majority of physicians and non-physicians were hospitalized in the last six months of life and that the small difference between the two groups was not statistically significant after adjusting for other variables. The groups also had the same likelihood of having at least one stay in the ICU during that period: 34.6 percent for doctors vs. 34.4 percent for non-doctors. In fact, doctors spent slightly longer in the ICU than non-doctors, the study found — not enough time to signify a clinical difference, but suggesting that, if anything, doctors may be using medicine more intensively.
In one regard, doctors seemed to die slightly better than non-doctors: 46.4 percent of doctors used hospice during their last six months compared with 43.2 percent of non-doctors. Doctors also spent nearly 2½ more days in hospice than non-doctors.
But these differences are small, and overall, they are far from the powerful mythology that doctors are dying better than the rest of the populace.
“Doctors are human, too, and when you start facing these things, it can be scary, and you can be subject to these cognitive biases,” said Daniel Matlock of the University of Colorado School of Medicine.
This is striking because it is the opposite of what doctors say they’d prefer. Onesurvey asked doctors and their patients what treatment course they would choose if they were faced with a terminal illness. Doctors said they would choose less medicine than their patients in almost all cases.
Many people have witnessed a death that seemed to be exacerbated by modern medicine: a drug that came with side effects but never seemed to halt the disease’s progress, the surgery that was totally unnecessary and might even have sped up someone’s death. Doctors have seen that happen even more often.
“Patients generally are not experts in oncology, and yet they have to make decisions without knowing what the whole course of their illness will be,” wrote Craig C. Earle in the Journal of Clinical Oncology. “We, on the other hand, have shepherded many patients through this journey toward death.”
That’s why powerful anecdotes about doctors who die better, whose last moments are spent peacefully and with family, give us hope: There is a better way.
But Matlock and Fischer think that their data may reveal the odds against the patient, even when the patient is a doctor. The health-care system may simply be set on a course to intervene aggressively.
“These things that encourage low-value care at the end of life are big systems issues,” Matlock said. “And a strong, informed patient who knows the risks and benefits — maybe even they have a hard time stopping the train.”
There are definite limits to the study: It could not control for differences in education or income among people in the sample. The doctors who died were mostly white men.
But the findings may reveal a deep bias that lies at the root of medicine. Fischer pointed out that the entire health-care system is aimed at fixing problems, not giving comfort. For example, a hip replacement the day before someone dies is something the medical system is equipped to handle: Surgeons can schedule it, and health insurance will pay for it. But, Fischer pointed out, if a patient needs less-skilled home care — such as help with feeding and bathing at home, it’s much harder to write a prescription.
Lonny Shavelson is consulting with doctors who have questions about California’s “End of Life Option Act.” He will also see patients after the law takes effect next week.
Few people have the unusual set of professional experiences that Lonny Shavelson does. He worked as an emergency room physician in Berkeley for years — while also working as a journalist. He has written several books and takes hauntingly beautiful photographs.
Now he’ll add another specialty. Just as California’s End of Life Option Act, a law legalizing physician aid-in-dying for people who are terminally ill, is set to take effect next week, Shavelson has become a consultant aimed at answering questions from physicians and patients about the practice — even becoming a physician to terminally ill patients seeking to end their lives.
Oregon was the first state to approve the practice, and in 1996 the law was held up in court. I turned to Shavelson as he had published “A Chosen Death,” a moving book following five terminally ill people over two years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue of assisted suicide closely for several years more, but ultimately moved on to other major projects — among them a book about addiction and a documentary about people who identify as neither male nor female.
Now he’ll add another specialty. Just as California’s End of Life Option Act, a law legalizing physician aid-in-dying for people who are terminally ill, is set to take effect next week, Shavelson has become a consultant aimed at answering questions from physicians and patients about the practice — even becoming a physician to terminally ill patients seeking to end their lives.
Oregon was the first state to approve the practice, and in 1996 the law was held up in court. I turned to Shavelson as he had published “A Chosen Death,” a moving book following five terminally ill people over two years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue of assisted suicide closely for several years more, but ultimately moved on to other major projects — among them a book about addiction and a documentary about people who identify as neither male nor female.
Now he’ll add another specialty. Just as California’s End of Life Option Act, a law legalizing physician aid-in-dying for people who are terminally ill, is set to take effect next week, Shavelson has become a consultant aimed at answering questions from physicians and patients about the practice — even becoming a physician to terminally ill patients seeking to end their lives.
Oregon was the first state to approve the practice, and in 1996 the law was held up in court. I turned to Shavelson as he had published “A Chosen Death,” a moving book following five terminally ill people over two years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue of assisted suicide closely for several years more, but ultimately moved on to other major projects — among them a book about addiction and a documentary about people who identify as neither male nor female.
The wall of Lonny Shavelson’s office, lined with covers of the books he has written.
Shavelson decided he had to act, although he feels “quite guilty” about having been away from the issue while others pushed it forward.
“Can I just sit back and watch?” Shavelson told me from his cottage office in his backyard in Berkeley. “This is really an amazing opportunity to be part of establishing policy and initiating something in medicine. This is a major change … [that] very, very few people know anything about and how to do it.”
His website, Bay Area End of Life Options, went up in April, and he’s outlined the law at “grand rounds” at several Bay Area hospitals this spring. His practice will be focused on consulting not only with physicians whose patients request aid-in-dying, but also with patients themselves, including offering care to patients who choose him as their “attending End-of-Life physician,” as he indicates on his site.
Shavelson is adamant that this is “something that has to be done right.” To him, that means starting every patient encounter with a one-word question: “Why?”
“In fact, it’s the only initial approach that I think is acceptable. If somebody calls me and says, ‘I want to take the medication,’ my first question is, why? Let me talk to you about all the various alternatives and all the ways that we can think about this,” he predicts he will say.
Shavelson worries that patients may seek aid-in-dying because they are in pain, so first, he would like all his patients to be enrolled in hospice care.
“This can only work when you’re sure that the patients have been given the best end-of-life care, which to me is most guaranteed by being a part of hospice or at least having a good palliative care physician. Then this is a rational decision. If you’re doing it otherwise, it’s because of lack of good care.”
California is the fifth state to legalize aid-in-dying, joining Oregon, Washington, Vermont and Montana. The option is very rarely used. For example, in 2014 in Oregon, 155 lethal prescriptions were written under the state’s law, and 105 people ultimately took the medicine and died, a death rate under this method of less than 0.5 percent.
Under the law, two doctors must agree that a mentally competent patient has six months or less to live. One of the patient-doctor meetings must be private, between only the patient and the physician, to ensure the patient is acting independently. Patients must be able to swallow the medication themselves and must state, in writing, within 48 hours before taking the medication, that they will do so.
Shavelson says he has been surprised by the lack of understanding he hears from some health care providers about the law. One person insisted the law was not taking effect this year; another asked how the law would benefit his patients with Alzheimer’s disease. To be clear, the law takes effect next week, and patients with dementia cannot access the law because they are not mentally competent.
The law does not mandate participation by any health care providers. Many physicians are “queasy” with the new law, Shavelson says he’s hearing, and are unwilling to prescribe to patients who request the lethal medication — even though they tell him they think the law is the right thing to do.
Renee Sahm, one of five terminally ill people followed by Lonny Shavelson in his 1995 book “A Chosen Death.”
“My response to that is as health care providers, you might have been uncomfortable the first time you drew blood. You might have been uncomfortable the first time you took out somebody’s gall bladder,” he says. “If it’s a medical procedure you believe in and you believe it’s the patient’s right, then it’s your obligation to learn how to do it — and do it correctly.”
Shavelson said he predicts that many physicians who are initially reluctant to provide this option to their patients may become more comfortable after the law goes into effect and they see how it works.
Burt Presberg, an East Bay psychiatrist who works specifically with cancer patients and their families, said a talk he attended by Shavelson sparked a conversation at his practice. Yet, in my own talk with him, he peppered his statements with “on the other hand,” as he clearly wrestled with his own comfort level of handling patient requests.
Presberg spoke of his concern that patients suffer from clinical depression at the end of life, sometimes feeling they are a burden to family members who could “really push for the end of life to happen a little sooner than the patient themselves.” He spoke from his experience of successfully treating terminally ill patients with clinical depression.
“Depression is something that’s really undertreated,” Presberg said. “I often talk to people about the difference between normal sadness and normal grieving at the end of life.”
He said he believes Shavelson will be aware of treating depression, “but I do have concerns about other physicians,” he said. “On the other hand, I think it’s really good that this is an option.”
Shavelson says he’s already received a handful of calls from patients, but he’s mostly spent this time before the law takes effect talking to other physicians. He needs a consulting physician and a pharmacist that will accept prescriptions for the lethal dose of medicine.
Then he returns to the patient. “It’s important … that we’re moving forward,” he says. “It’s crucial that we do that because this is part of the rights of patient care to have a certain level of autonomy in how they die.”
To many of the doctors who feel “queasy” about moving to end a patient’s life, this type of care “isn’t so tangibly different to me,” Shavelson says, than other kinds of questions doctors address.
“I’m just one of those docs who sees dying as a process, and method of death is less important than making sure it’s a good death.”
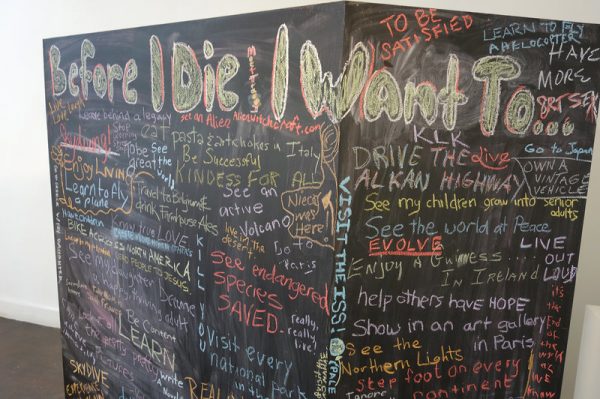
A chalkboard “bucket list” stirred imaginations and got people talking at an Indianapolis festival designed to help make conversations about death easier.
In a sunny patch of grass in the middle of Indianapolis’ Crown Hill Cemetery, 45 people recently gathered around a large blackboard. The words “Before I Die, I Want To …” were stenciled on the board in bold white letters.
Sixty-two-year-old Tom Davis led us through the thousands of gravestones scattered across the cemetery. He’d been thinking about his life and death a lot in the previous few weeks, he told us. On March 22, he’d had a heart attack.
Davis said he originally planned to jot, “I want to believe people care about me.” But after his heart attack, he found he had something new to write: “I want to see my grandkids grow up.”
Others at the event grabbed a piece of chalk to write down their dreams, too, including some whimsical ones: Hold a sloth. Visit an active volcano. Finally see Star Wars.
The cemetery tour was part of the city’s Before I Die Festival, held in mid-April — the first festival of its kind in the U.S. The original one was held in Cardiff, Wales, in 2013, and the idea has since spread to the U.K., and now to Indianapolis.
The purpose of each gathering is to get people thinking ahead — about topics like what they want to accomplish in their remaining days, end-of-life care, funeral arrangements, wills, organ donation, good deaths and bad — and to spark conversations.
“This is an opportunity to begin to change the culture, to make it possible for people to think about and talk about death so it’s not a mystery,” said the festival’s organizer Lucia Wocial, a nurse ethicist at the Fairbanks Center for Medical Ethics in Indianapolis.
The festival included films, book discussions and death-related art. One exhibit at the Kurt Vonnegut Memorial Library had on display 61 pairs of boots, representing the fallen soldiers from Indiana who died at age 21 or younger.
These festivals grew out of a larger movement that includes Death Cafes, salon-like discussions of death that are held in dozens of cities around the country, and Before I Die walls — chalked lists of aspirational reflections that have now gone up in more than 1,000 neighborhoods around the world.
“Death has changed,” Wocial said. “Years ago people just died. Now death, in many cases, is an orchestrated event.”
Medicine has brought new ways to extend life, she says, forcing patients and families to make a lot of end-of-life decisions about things people may not have thought of in advance.
“You’re probably not just going to drop dead one day,” she said. “You or a family member will be faced with a decision: ‘I could have that surgery or this treatment.’ Who knew dying was so complicated?”
With that in mind, the festival organizers held a workshop on advance care planning, including how to write an advance directive, the document that tells physicians and hospitals what interventions, if any, you want them to make on your behalf if you’re terminally ill and can’t communicate your wishes. The document might also list a family member or friend you’ve designated to make decisions for you if you become incapacitated.
“If you have thought about it when you’re not in the midst of a crisis, the crisis will be better,” Wocial said. “Guaranteed.”
About a quarter of Medicare spending in the U.S. goes to end-of-life care. Bills that insurance doesn’t cover are usually left to the patients and their families to pay.
Jason Eberl, a medical ethicist from Marian University who spoke at the festival, said advance directives can address these financial issues, too. “People themselves, in their advance directive will say, ‘Look, I don’t want to drain my kids college savings or my wife’s retirement account, to go through one round of chemo when there’s only a 15 percent chance of remission. I’m not going to do that to them.’ ”
The festival also included tour of a cremation facility in downtown Indianapolis. There are a lot of options for disposing of human ashes, it turns out. You can place them in a biodegradable urn, for example, have them blown into glass — even, for a price, turn them into a diamond.
“It’s not inexpensive,” Eddie Beagles, vice president of Flanner and Buchanan, a chain of funeral homes in the Indianapolis area, told our tour group. “The last time I looked into it for a family, “it was about $10,000.”
A crematorium tour was part of the festival, too. Metal balls, pins, sockets and screws survive the fire of cremation.
“Really, when it comes to cremation, there’s always somebody coming up with a million dollar idea,” Beagles added. “If you can think of it, they can do it.”
Beagles showed us a pile of detritus from cremated human remains. He picked up a hip replacement — a hollow metal ball — then dropped it back into the ashes.
I’m a health reporter, so I know a fair amount about the things that could kill me, or are already killing me. But watching this piece of metal that used to be inside a human be tossed back onto the heap gave me pause. I’m thinking about what I might write on a “Before I Die” wall. I still don’t know — there are many things to do before I go. But I’m thinking about it a lot harder now.
After I was diagnosed with brain cancer, I developed a desire to have really tough conversations about death and dying with my family so that I could share my thoughts with them and feel less alone on this journey that’s been full of uncertainty. At first, this was quite challenging for me and my family, but one of the things that has really helped us to be able to have these tough conversations was my realization that this topic was not something unique and exclusive to me and people like me, but rather a conversation we all should be having regardless of age, health, and condition.
Nobody lives forever and even though some people may seem to have better odds than others, tomorrow is not guaranteed to anyone. Unfortunately, our society makes death and dying very frightening because the only time people get asked about their wishes and end of life care is when death seems to be looming directly over them. This prevents us from developing any level of familiarity, comfort, and acceptance with this topic.
In an effort to confront this problem and try to combat this societal barrier, I began advocating for my entire family to have these conversations and revisit them regularly so that when the time comes we are each able to revisit this topic as a familiar concept opposed to completely foreign and devastatingly unbelievable circumstances.
While there are very real emotional and social challenges associated with addressing this topic, I’ve become incredibly empowered by the idea that there are still things out there that I have a choice over. This has been a very rewarding and welcomed realization after struggling to manage the overwhelming feelings of uncertainty and loss of control that formed after my diagnosis.
My intention is not to instill paranoia about death or dying, but rather begin to open a door for each of you to have those tough conversations about your future wishes regarding being comforted, supported, treated, and remembered when the time arises. At no point are you giving up hope by talking about this topic. You are simply ensuring that your wishes regarding the eventually inevitable circumstance that everyone will face are communicated and respected.
WANT a better 2016? Try thinking more about your impending demise.
Years ago on a visit to Thailand, I was surprised to learn that Buddhist monks often contemplate the photos of corpses in various stages of decay. The Buddha himself recommended corpse meditation. “This body, too,” students were taught to say about their own bodies, “such is its nature, such is its future, such its unavoidable fate.”
Paradoxically, this meditation on death is intended as a key to better living. It makes disciples aware of the transitory nature of their own physical lives and stimulates a realignment between momentary desires and existential goals. In other words, it makes one ask, “Am I making the right use of my scarce and precious life?”
In fact, most people suffer grave misalignment. In a 2004 article in the journal Science, a team of scholars, including the Nobel Prize winner Daniel Kahneman, surveyed a group of women to compare how much satisfaction they derived from their daily activities. Among voluntary activities, we might expect that choices would roughly align with satisfaction. Not so. The women reported deriving more satisfaction from prayer, worship and meditation than from watching television. Yet the average respondent spent more than five times as long watching TV as engaging in spiritual activities.
If anything, this study understates the misalignment problem. The American Time Use Survey from the Bureau of Labor Statistics shows that, in 2014, the average American adult spent four times longer watching television than “socializing and communicating,” and 20 times longer on TV than on “religious and spiritual activities.” The survey did not ask about hours surfing the web, but we can imagine a similar disparity.
This misalignment leads to ennui and regret. I’m reminded of a friend who was hopelessly addicted to British crossword puzzles (the ones with clues that seem inscrutable to Americans, such as, “The portly gentleman ate his cat, backwards”). A harmless pastime, right? My friend didn’t think so — he was so racked with guilt after wasting hours that he consulted a psychotherapist about how to quit. (The advice: Schedule a reasonable amount of time for crosswords and stop feeling guilty.)
While few people share my friend’s interest, many share his anxiety. Millions have resolved to waste less time in 2016 and have already failed. I imagine some readers of this article are filled with self-loathing because they just wasted 10 minutes on a listicle titled “Celebrities With Terrible Skin.”
Some might say that this reveals our true preferences for TV and clickbait over loved ones and God. But I believe it is an error in decision making. Our days tend to be an exercise in distraction. We think about the past and future more than the present; we are mentally in one place and physically in another. Without consciousness, we mindlessly blow the present moment on low-value activities.
The secret is not simply a resolution to stop wasting time, however. It is to find a systematic way to raise the scarcity of time to our consciousness.
Even if contemplating a corpse is a bit too much, you can still practice some of the Buddha’s wisdom resolving to live as if 2016 were your last year. Then remorselessly root out activities, small and large, that don’t pass the “last-year test.”
There are many creative ways to practice this test. For example, if you plan a summer vacation, consider what would you do for a week or two if this were your last opportunity. With whom would you reconnect and spend some time? Would you settle your soul on a silent retreat, or instead spend the time drunk in Cancún, Mexico?
If this year were your last, would you spend the next hour mindlessly checking your social media, or would you read something that uplifts you instead? Would you compose a snarky comment on this article, or use the time to call a friend to see how she is doing? Hey, I’m not judging here.
Some might think that the last-year test is impractical. As an acquaintance of mine joked, “If I had one year to live, I’d run up my credit cards.” In truth, he probably wouldn’t. In a new paper in the science journal PLOS One, two psychologists looked at the present value of money when people contemplated death. One might assume that when reminded of death, people would greatly value current spending over future spending. But that’s not how it turned out. Considering death actually made respondentsless likely to want to blow money now than other scenarios did.
Will cultivating awareness of the scarcity of your time make you grim and serious? Not at all. In fact, there is some evidence that contemplating death makes you funnier. Two scholars in 2013 published an academic paperdetailing research in which they subliminally primed people to think about either death or pain, and then asked them to caption cartoons. Outside raters found the death-primed participants’ captions to be funnier.
There’s still time to rethink your resolutions. Forget losing weight and saving money. Those are New Year’s resolutions for amateurs. This year, improve your alignment, and maybe get funnier in the process: Be fully alive now by meditating on your demise. Happy 2016!
In Australian nursing homes, older people are increasingly frail and being admitted to care later than they used to be. More than half of residents suffer from depression, yet psychiatrists and psychologists aren’t easily accessible, and pastoral or spiritual care is only available in a subset of homes.
Depression at the end of life is often associated with loss of meaning. Research shows people who suffer from such loss die earlier than those who maintain purpose. This can be helped by nurturing the “spirit” – a term that in this setting means more than an ethereal concept of the soul. Rather, spiritual care is an umbrella term for structures and processes that give someone meaning and purpose.
Caring for the spirit has strength in evidence. Spiritual care helps people cope in grief, crisis and ill health, and increases their ability to recover and keep living. It also has positive impacts on behaviour and emotional well-being, including for those with dementia.
Feeling hopeless
Many people have feelings of hopelessness when their physical, mental and social functions are diminished. A 95-year-old man may wonder if it’s worth going on living when his wife is dead, his children don’t visit anymore and he’s unable to do many things without help.
The suffering experienced in such situations can be understood in terms of threatening one’s “intactness” and mourning what has been lost, including self-identity.
Nursing home residents are increasingly frail and more than half experience depression.
Fear is also common among those facing death, but the particular nature of the fear is often unique. Some may be afraid of suffocating; others of ghosts. Some may even fear meeting their dead mother-in-law again.
What plagues people the most though is the thought of dying alone or being abandoned (though a significant minority express a preference to die alone). Anxiety about dying usually increases after losing a loved one.
But such losses can be transcended by encouraging people to pursue their own purpose for as long as they can; in other words, by caring for the spirit.
What is spiritual care?
Spiritual care has religious overtones that make it an uncomfortable concept in a secular health system. But such care can be useful for all – religious and non-religious – and can be provided by carers, psychologists and pastoral specialists alike.
Spirituality can be defined as “the way individuals seek and express meaning and purpose and the way they experience their connectedness to the moment, to self, to others, to nature, and to the significant or sacred”. Perhaps the Japanese term “ikigai” – meaning that which gives life significance or provides a reason to get up in the morning – most closely encompasses spirituality in the context of spiritual care.
Guidelines for spiritual care in government organisations, provided by the National Health Services in Scotland and Wales, note that it starts with encouraging human contact in a compassionate relationship and moves in whatever direction need requires. Spiritual needs are therefore met through tailoring components of care to the person’s background and wishes.
Spiritual care can involve having your dog nearby or being surrounded by your favourite sports team regalia.
For instance, one person requested that her favourite football team regalia be placed around her room as she was dying. Another wanted her dog to stay with her in her last hours. Supporting these facets of identity can facilitate meaning and transcend the losses and anxiety associated with dying.
Spiritual care can include a spiritual assessment, for which a number of tools are available that clarify, for instance, a person’s value systems. Such assessments would be reviewed regularly as a person’s condition and spiritual needs can change.
Some people may seek religion as they near the end of their lives, or after a traumatic event, while others who have had lifelong relationships with a church can abandon their faith at this stage.
Other components of spiritual care can include allowing people to access and recount their life story; getting to know them, being present with them, understanding what is sacred to them and helping them to connect with it; and mindfulness and meditation. For those who seek out religious rituals, spiritual care can include reading scripture and praying.
Spiritual care in the health system
Psychologists or pastoral care practitioners may only visit residential homes infrequently because of cost or scarce resources. To receive successful spiritual care, a person living in a residential home needs to develop a trusting relationship with their carer.
For those who seek out religious rituals, spiritual care can include reading scripture and praying.
This can best be done through a buddy system so frail residents can get to know an individual staff member rather than being looked after by the usual revolving door of staff.
Our reductionist health care model is not set up to support people in this way. Slowing down to address existential questions does not easily reconcile with frontline staff’s poverty of time. But health care settings around the world, including Scotland and Wales, the United States and the Netherlands, are starting to acknowledge the importance of spiritual care by issuing guidelines in this area.
In Australia, comprehensive spiritual care guidelines for aged care are being piloted in residential and home care organisations in early 2016.
People with chronic mental illness, the elderly, the frail and the disabled have the right to comprehensive health care despite their needs often being complex, time-consuming and expensive.
Finding meaning at all stages of life, including during the process of dying, is a challenging concept. It seems easier to get death over with as quickly as possible. But the development of new spiritual care guidelines brings us one step closer to supporting a meaningful existence right up to death.
Fear of dying – or death anxiety – is often considered to be one of the most common fears. Interestingly though, neither of the two widely used diagnostic psychiatric manuals, DSM-5 or ICD-10, has a specific listing for death anxiety.
Death is related in the manuals to a number of anxiety disordersincluding specific phobias, social anxiety, panic disorder, agoraphobia, post-traumatic stress disorder and obsessive compulsive disorder. Although many psychologists will argue that these fears are proxies for the larger fear of death.
Existential therapy directly targets death and the meaning of life. It’s practised by psychiatrist Irvin Yalom, a pioneer in understanding fear of death and how to treat it in therapy. He has written a popular book on the subject called Staring at the Sun: Overcoming the Terror of Death. Existential therapy is one way of treating death anxiety but no matter what psychological approach is used, the underlying theme is generally the same: acceptance.
What’s so frightening about death?
All life has death in common, yet it’s striking how little we actually talk about it. In Western cultures at least, the concept can be too much even to consider. But from a clinical psychology perspective, the more we avoid a topic, situation, thought or emotion, the greater the fear of it can become and the more we want to avoid it. A vicious cycle.
Fear of the unknown is one of the specific fears around death.
If presented with a client who has death anxiety, we would ask them to tell us exactly what they fear about death. Yalom once asked a client what bothered him most. The client replied, “The next five billion years with my absence.”
Yalom then asked, “Were you bothered by your absence during the last five billion years?”
The specific death fear will be different for everyone, but it can often be categorised into one of four areas: loss of self or someone else; loss of control; fear of the unknown – what will happen after death (nothingness, heaven, hell); and pain and suffering of dying.
Yalom suggests psychologists speak about death directly and early in therapy. The psychologist should find out when the client first became aware of death, who he discussed it with, how the adults in his life responded to his questions and whether his attitudes about death had changed over time.
In one of the first studies to examine death anxiety directly, cognitive-behaviour therapy (CBT), was found to be successful in treating it in those suffering from hypochondria. The strategies used included exposure (going to a funeral), relaxation strategies (breathing) and creating flexible thoughts around death, such as recognising that fearing death is normal.
Some researchers argue that CBT should include strategies that explore the probability of life events – such as calculating the chances of your parents’ meeting and having you. Such techniques can shift our perspective from a negative fear of dying to a positive realisation we are lucky to experience life at all.
We must learn to accept death. It’s not going away.
Existential therapy has been shown very useful in treating death anxiety. It focuses on ultimate existential concerns such as isolation. For instance, we have a deep need to belong and having family and friends means, in some way, we live on after death.
Treatment is directed at finding meaning and purpose in life, increasing psychological and social support, building relationships with friends and family and improving coping skills to manage anxiety in daily life.
In compassion focused therapy (CFT), the client is encouraged to descend into the reality of human experience. That means realising we only have about 25,000 to 30,000 days of life. Suffering is normalised and the emphasis is on the fact that the trajectory of life is the same for everyone: we come into this world, grow and flourish and then decay and die.
CFT discusses how the human brain has the fantastic ability to imagine and question our very existence – as far as we know a uniquely human quality. We will then say to clients: “Did you design your brain to have that capacity?” Of course the answer is a resounding no.
So we work on the principle that it is not the client’s fault they have death anxiety but that we must work with our brains so they don’t paralyse our ability to live now.
In CFT we will sometimes use the phrase, “Our brains were designed for survival not happiness”. Strategies arising form this include guided discovery (slowing down and giving clients opportunities to make their own insights) and soothing rhythm breathing.
Although subtly different in approach these therapies have a similar underlying theme. Death is something we must learn to accept. The key for us in the context of death anxiety is how we get out of our minds and into our life.
Some tips that could help
If you struggle with death anxiety, please consider seeing a psychologist. But for now, here are three tips that might be helpful.
Normalise the experience: We have tricky brains that allow us to question our existence. This is not your fault but is how the human brain was designed. It is perfectly normal to have a fear of death; you are not alone in this struggle.
Breathe: When you notice anxiety entering your body and mind, try to engage in some soothing breathing to help slow down your mind and physiological response.
Write your own eulogy as if you’re looking back over a long life: Pretend it is your funeral and you have to give the eulogy. What would you write? What would you have wanted your life to be about? This might provide some meaning and purpose for how to live your life now.