On this day, I was at Mount Sinai Hospital, in the oncology ward. The receptionist I usually check in with wasn’t at her desk. I was being greeted by a volunteer. Dark hair, wide eyes and a smile like a child’s doll. High school co-op student, maybe?
I handed over my health card and told her my doctor’s name.
“I’m sorry, I don’t know who she is. What are you here for?”
Her smile widens.
“Because I’m a patient?” I retort.
I know I’m being rude. But it’s an oncology ward. What does she think I’m here for? To discuss the weather? The shortage of wheelchair-accessible parking spaces in the lot?
What I really want to say is, my doctor is a palliative-care specialist. I’m seeing her because I have cancer. I’m preparing for my death.
I don’t look like I have cancer, let alone the incurable kind. I have all my hair. My friends and husband assure me my colour is good. Dressed in my normal clothes and not the pajamas I currently favour, I look reasonably well – for a middle-aged woman who also has spinal muscular atrophy, a congenital neuromuscular condition.
I rely on a motorized wheelchair to get around and need personal support workers to assist me in all aspects of daily living. It’s been this way forever, but now I have colon cancer, and two external abdominal bags to collect various bodily fluids.
This, to put it mildly, complicates things.
My palliative-care doctor is a compassionate young woman who wouldn’t look out of place in a medical drama. She has been guiding me through my own recent hospital drama: I was readmitted to hospital a couple of weeks earlier, for yet another emergency.
I’ve been fighting off a major abdominal abscess for more than a year now. At one point, my abscess was so large, one of my doctors admitted surprise that I was upright. This is what initially led to my cancer diagnosis. A colon biopsy confirmed the cancer was malignant. In October, I was told my cancer was inoperable, despite 28 rounds of radiation.
At least it’s not metastatic. Localized, but nowhere else. For now, anyway. Plus, my surgeon tells me, I likely have years with this cancer. Not months or weeks, like some of his other patients.
The challenge now is the infection associated with the abscess. During this current crisis, antibiotics are working. What my surgeon can’t tell me is when the next infection will hit, or when antibiotics may fail.
Some patients reinfect every month, he tells me. I’ve done well, he adds. I tell him I couldn’t handle being hospitalized every month. He acknowledges I would need to evaluate my quality of life, if this became my reality. In that moment, my decision to seek palliative care early seems the smartest decision I’ve made in a while.
Like most Canadians, I had limited understanding of palliative care before I had cancer. To me, “palliative care” was synonymous with “you are about to die.”
That’s not the case. On my first palliative visit, the doctor explains the word is Latin for “to cloak.” She personally likes that, seeing her role as guide and protector to patients who are coping with the most difficult time of their lives.
I need her guidance. There is no clear path around how to deal with cancer while living with a disability. I’m used to being disabled. It’s my normal. My quality of life up to now has been exceptional, complete with a husband I adore, a sweet, sassy daughter and a brand-new career.
Like everyone else diagnosed with cancer, my life has suddenly imploded. I find myself in this new world, navigating how to continue while knowing the end is coming much sooner than I’d like.
That’s why I’ve sought out palliative care. My own research leads me to studies showing that having a palliative-care expert can help me prolong my quality of life through the management of symptoms, such as pain that I know will likely worsen over time. My family doctor concurs, telling me outright that I need this.
This new relationship has enabled me to talk about my greatest fears. After my conversation with my surgeon, I fear dying slowly of sepsis, waiting for my organs to fail. I’ve agreed to a Do Not Resuscitate order, which ensures I won’t be hooked up to machines in the ICU, prolonging The End.
During this particular admission to hospital and based on what my surgeon has said, my choices seem stark. Down the road, I could die slowly from an infection that will shut down my organs, or sign up for a medically assisted death.
Then, my palliative-care doctor arrives at my bedside. She points out I have bounced back from severe, acute episodes before. She also knows I don’t want an assisted death and takes the time to explain there are options available, such as palliative sedation, a process where I can have large doses of morphine to keep me comfortable. She firmly tells me I am not close to needing this. My goal needs to be focused on getting better and getting home, to my daughter.
As she explains this, I start to relax. She’s given me the window I need to live my life, as compromised as it now is. It is not the life I would have chosen, but it still has meaning. My task now is to figure out what that meaning is. And her task is to help me to define my priorities while maximizing the quality of my life with medical therapies and emotional support.
It’s an interesting time to be thinking of my life as a person who is both disabled and has cancer. Less than two years ago, the federal government enacted a new law enabling Canadians with incurable conditions, whose death is foreseeable and are suffering irremediably, to ask a doctor to end their lives.
It’s been called “dying in dignity,” but for me, that’s not the way I want to go, at the hands of a doctor, wielding a poisoned syringe.
I believe no one with a terminal illness should be forced to endure suffering – but, if there is one lesson for me in the past year, death is not the only way to alleviate suffering. Managing physical suffering feels like traveling a winding road. Some days, it feels never-ending; other days, manageable, almost like the life I had before. Some days are so bad, I’m convinced death really is the only relief, but I’m brought back to reality when I think of what I could miss out on.
My life is definitely smaller now. I doubt I will ever work full-time again. I barely leave my apartment. Thanks to my father’s financial generosity, my husband has been able to take unpaid leave from his work to be with me. The time we spend together is precious. Even in its ordinariness, it is meaningful.
I appreciate the world differently now. It is as though time has slowed for me to see the small details of life, whether it be the softness of my bed sheets or watching snow drift down through my apartment window.
I’m trying to live with dignity, as I always have, despite the very real medical indignities I have been subjected to.
Which is why it dismays me greatly there are continuing attempts to make it easier for people without terminal conditions to ask a doctor to end their life. It dismays me that a lobby organization calling itself Dying With Dignity is not actively lobbying for increased access to palliative and hospice care, or advocating for more community supports for people with disabilities to live as productively as possible. In other words, to live with dignity.
We are all going to die, but before we do, each one of us has a right to a good quality of life, even to the very end. Yet too many Canadians do not have adequate access to palliative and hospice care. The lobbying efforts of those to equalize this are rarely discussed in our media.
I’ve chosen my path, thanks to the help of empathetic doctors and my own advocacy. My hope now is that more Canadians have the right to do the same, without the implied suggestion there is only one real way to die with dignity.
Most people who’ve used lethal prescriptions under Washington’s Death with Dignity Act were white, college-educated and lived in Western Washington. They ranged in age from 20 to 101; most were dying of cancer.
[O]n a cold winter morning, Phil Estes gets into the private ambulance he’s hailed for the more than two-hour journey to Spokane, all 99 pounds of the former Hanford engineer clinging to his frail 6-foot-tall frame as his gurney is secured in the vehicle.
He’s taking this trip not to save his life, but to be able to end it. As weak as Estes is, this is his last resort.
The 81-year-old is several years into his fight against colon cancer. He can barely sit up for five minutes at a time, let alone take care of himself. He’s in pain, it’s hard to breathe and the cancer that has riddled his body is going to kill him. So he’s done.
He wants to take “the pill.”
“I’ve lived a long life, a happy life,” Linda Estes recalls her dad telling her family at the time. “I want you to go on with your life, but I’ve thought it all through, and this is the best option.”
But as his family would soon learn, getting a lethal dose of medication, which is legal under Washington’s Death with Dignity Act, involves much more than a single pill. And in Eastern Washington, it can mean long roadtrips to find doctors and pharmacies willing to validate a patient’s terminal illness and fill a fatal prescription.
In the 10 years since voters passed the Death with Dignity Act, the vast majority of terminal patients who have opted to die under the law lived in Western Washington — more than 90 percent of cases most years — despite Eastern Washington accounting for more than 20 percent of the state population.
The discrepancy between the two sides of the Cascades, experts say, is largely due to access: Even those who can cover thousands of dollars in out-of-pocket costs aren’t guaranteed to live in an area where a doctor or hospital system is willing to participate.
In Estes’ case, Dr. David Jones had been working with him for years and was willing to learn how to sign off as the attending physician and write him a prescription. That meant Estes just needed another consulting doctor to agree he was mentally competent, deathly ill and not being coerced to get the life-ending medication.
But Jones learned that participating would violate policy at Kadlec, the Tri-Cities hospital system where he works, and he feared he might lose his job. The previously secular system had recently been acquired by Providence, a Catholic health-care system that generally doesn’t allow its employees to participate under the rules of the act.
So the family scrambled to find other doctors.
“We called everybody we could think of,” Linda Estes recalls. “At one point my mother was carrying all the cellphones and the house extension in a bag with her, so whoever called, she could answer them.”
Eventually, with assistance from End of Life Washington, a Seattle-based organization that helps people navigate end-of-life options, they got in touch with a Spokane doctor willing to sign the attending paperwork, and a local physician agreed to handle the consulting role. But the Spokane doctor wanted to diagnose Estes in person, spurring the $1,400 contracted ambulance ride from Richland to Spokane.
After an exhausting day of appointments, Estes got his prescription.
“I got out to the ‘cabulance,’ and I put the bag in dad’s hands,” Linda Estes says. “He grabbed that little [prescription] bag and his whole body relaxed. He’d been so afraid that at the last minute, that this decision that was his to make would be snatched from him.”
Estes took the medication at home Jan. 4, 2016, fell asleep and died peacefully with his daughter holding his hand.
But Linda Estes questions why it was so difficult to access something that was legal, especially when her father’s doctor was OK with the decision.
“My mom and I were able to accomplish this because we had the financial means and educational resources,” she says. “What do people do who don’t have these kind of resources? It shouldn’t be this hard.”
So she’s joining efforts to make the process easier for others and ensure physicians who want to sign off can do so.
Voter support for Initiative 1000 — Washington’s Death with Dignity Act — crossed typical ideological boundaries, with counties on both sides of the Cascades approving the measure.
TERMINAL CHOICES
Washington’s role in nationwide right-to-die efforts has a complicated history. In 1997, the U.S. Supreme Court reviewed a Washington state law that made physician-assisted suicide a felony. The court held that the law was fine, but also left the door open for states to pass laws allowing the practice if it wouldn’t violate their own constitutions.
That same year, Oregon became the first in the nation to enact its Death with Dignity Act.
A decade later, nearly 58 percent of Washington state voters approved their own version of the act, making Washington the second state in the country to allow the practice. Assisted suicide is still illegal under state law, but under the Death with Dignity Act, people who are already dying and meet the qualifications are not considered to be committing suicide — their underlying illnesses are listed as the cause of death on death certificates.
Since then, three other states — Vermont (in 2013), Colorado (2016) and California (2016) — and the District of Columbia (2017) have also legalized it. Opponents have filed various challenges in court, but each of the laws have been allowed to move forward. Montana hasn’t passed a similar law, but the state’s Supreme Court determined in a 2009 case that nothing in Montana law prohibits physicians from participating. That means about a sixth of the U.S. population lives in a state where the process is legal, and several states are currently considering similar bills.
The majority of American adults believe that someone has a moral right to end their life if they are suffering great pain with no chance for improvement (62 percent), or have an incurable disease (56 percent), according to a 2013 Pew Research survey on end of life. However, only 47 percent approved of laws allowing doctors to prescribe lethal medication to terminal patients.
How that process is referenced largely depends on viewpoint: Opponents typically refer to it as “physician-assisted suicide” or “euthanasia” (mercy killing), while proponents tend to use “death with dignity” or “physician aid-in-dying.”
Many opponents, including large sectors of the medical field and religious organizations, consider the act a crime or immoral. Some worry there could be a slippery slope: If patients think they are a burden on their families, they may feel pressured to die sooner; or insurance companies could decide it is cheaper to pay for fatal medication than further treatment. In summer 2016, Pope Francis told medical leaders that physician-assisted suicide was “false compassion.”
“Frailty, pain and infirmity are a difficult trial for everyone, including medical staff. They call for patience, for ‘suffering-with.’ Therefore, we must not give in to the functionalist temptation to apply rapid and drastic solutions, moved by false compassion or by mere criteria of efficiency or cost effectiveness,” the Catholic News Agency reported Francis saying. “The dignity of human life is at stake.”
But proponents point to very specific protections written into the law. More than one physician needs to determine someone is terminally ill and not being coerced. At least one witness to the request for medication must not be related or stand to gain financially from the person’s death. There are mandatory waiting periods and the chance to rescind a request before a prescription is filled.
In states where it is not legal, people sometimes take extreme measures to die on their own terms.
Lacie Agidius was drinking coffee with her father in Lewiston, Idaho, when he received the worst call of his life.
Her grandfather was on the other end. He’d dressed in his best Sunday suit, organized important documents and was calling to make sure someone knew where a few things were on the family farm before taking his own life.
“He had told [my dad], ‘I want you to know, I don’t want to freak you out: Today is the day. I’m getting ready to walk down to the car,'” Agidius says. “He said, ‘This is not a call for help. This is absolutely what I want to do.'”
After being diagnosed with prostate cancer, her grandfather chose not to treat it. For months, he’d told his family he was getting his affairs in order and planned to take things into his own hands if it came to the point where he was in too much pain and couldn’t care for himself, but they’d largely brushed him off or were in denial, Agidius says.
Then came the call. In an awful shock to Agidius’ father, not only did her grandfather warn him not to call authorities, but he also said if he wasn’t successful, he wanted them to “finish the job.” A half-hour drive away, her father refused and said, “You don’t need to do this.”
“The whole conversation was awful,” Agidius says. “That long car ride for my dad and brothers, not knowing what they were going to find, that whole experience was so traumatic.”
By the time they arrived, it was too late.
Agidius, who now works in hospice care in the Spokane-Coeur d’Alene area, says she wishes that life-ending meds would have been an option for her grandfather, as it would’ve made things easier on everyone to know what was coming, and would have been less frightening for him, as it would have provided certainty.
She still lives in Idaho, where lawmakers made physician-assisted suicide a felony in 2011, partly in response to efforts similar to those that legalized the practice in neighboring states.
“It is something that is hard for people on the Idaho side to think we wouldn’t have that option,” she says. “You plan that date, then you can have time with that person, you know it’s happening. You can say those things you want to say and not have a shocking situation.”
PLANNING FOR THE UNKNOWN
Jessica Rivers, an End of Life Washington volunteer
Aside from the planning required by mandatory waiting periods, people with life-ending meds tend to plan out the process with family, and in each of the cases volunteer client adviser Jessica Rivers has worked on, they tried to say meaningful goodbyes to their loved ones.
Rivers, who lives near Palouse, Washington, has been a volunteer with End of Life Washington for about four years, working with families in Pullman, Spokane and rural communities in the region.
In the first case she worked, she and other End of Life volunteers arrived on the date their client selected to find his home full with family, friends and neighbors.
“They had food and drink and had all been having his celebration of life that morning,” Rivers says. “It was really remarkable, because we just let them take their time and do what they needed to do.”
The man, dying of aggressive cancer, gave his own eulogy, and everyone surrounded him as he lay down in bed, took the medication and talked them through how he felt before falling asleep. In the quiet, someone started singing “Amazing Grace,” and everyone cried.
“It was very powerful for me, and it was very gentle and very peaceful for him,” Rivers says.
For her, the choice to get involved in end-of-life care started about 20 years ago, when she cared for her mother, who was dying of pancreatic cancer.
“I remember my mom looking at herself in the mirror one morning, and the cancer had just ravaged her body,” Rivers says. “She was actually, amazingly enough, OK with dying, but she wasn’t OK with the process of getting there, and I think that’s true for most of the folks I’ve been with at End of Life.”
Of the 25 cases she’s been involved with through the organization, each patient died, though only six of them decided to take the medication.
“The majority of them told me, ‘I may or may not use this, but it gives me peace of mind,'” Rivers says. “And one of the things I tell them on that first visit when I meet them is ‘I’m not invested at all in whether they take this or not.'”
As a volunteer, she typically meets with families a few times, offering information on what the process may look like, encouraging clients to get on hospice care, and talking about death and the dying process, which is new to many people.
“I think that helps reduce fear,” she says. “My little piece of advice to family members is try not to let the fear and grief interfere in the days to come that you have left with your loved one. Try to really balance that fear and grief with love and gratitude.”
Rivers, who spent several years working in hospice, feels people aren’t supported enough through the end of their lives, which can be distressing. One dying man Rivers spoke to last year blurted out in front of his adult children that if he couldn’t for some reason access lethal medication under Washington’s law, he had hunting guns in his basement.
“The fear and distress this caused his children was so obvious and apparent,” Rivers says. “But the reality is people who are desperate can do dramatic things, and that’s one of the reasons this law is so important. People should not have to feel desperate.”
Artist Melinda Hannigan fought cancer for years before deciding to take life-ending medication at her home in Twisp.
EAST SIDE, WEST SIDE
Of the more than 1,100 people who are known to have died after getting prescriptions for lethal medication under Washington’s law from 2009 through 2016, fewer than 150 lived east of the Cascades, according to data compiled by the Washington State Department of Health. Not all of those people took the medication.
About three-quarters of people who got prescriptions had cancer, while the rest were mostly people with neurodegenerative diseases such as Lou Gehrig’s disease or respiratory or heart disease.
People who use the law account for only about two of every 1,000 deaths in Washington, says Sally McLaughlin, executive director of End of Life Washington. Of the more than 54,000 people who died in the state in 2015, 166 used the medication, putting the number of deaths in that category slightly above the 141 people who died from the flu the same year.
“It’s not like it’s a rampant number of people, but the issues with access have to do with several things,” she says. “One is access to physicians who can or are able to prescribe life-ending medications in a more conservative environment. There are a lot of physicians who don’t even want to think about administering life-ending medications.”
Secondly, many doctors are not allowed to participate under the rules of their employers. Patients often have to form new relationships with doctors when they’ve got little time left.
Aside from the population size accounting for part of the difference, many people east of the mountains just don’t know the law exists, says Dr. Raleigh Bowden, who lives in Twisp and works as a volunteer medical adviser with End of Life.
“In my personal experience, a lot of people don’t know about the law,” Bowden says. “In fact I talked to one pharmacist [last] year who didn’t know we had a law.”
Patients need both a prescribing doctor and a consulting physician, who ensures the person isn’t being coerced. To be eligible, the patient must be a Washington resident, have about six months or less to live, and understand that there are other options, Bowden says.
Ideally consulting physicians see someone in person, but in rural areas, sometimes they have to use other options like electronic communication. From Twisp, Bowden will sometimes serve in the consulting role via Skype, as that part of the process mostly involves going over a checklist with the patient.
Attending doctors almost always want to see the patient in person, Bowden says, and it’s better if they’ve already had a relationship. Jones, Estes’ doctor, says it was the fact he’d known him for eight years that made him comfortable with the idea of supporting his decision.
“It was the perfect situation for me to say, ‘Wow, how could I deny this?'” Jones says. “Whatever my beliefs were, I was a physician in the state of Washington where this was legal. It took the politics out of it for me until the very end when I realized I might be at risk of losing my job.”
Aside from physicians, the medication itself can pose problems.
End of Life Washington recommends one of two prescriptions. The first and cheapest runs about $700, but needs to be made in a compounding pharmacy, which often isn’t available in rural areas, Bowden says.
The second and most expensive option involves opening up about 100 capsules of Seconal, once regularly prescribed as a sleeping pill, and mixing the contents with juice or something the patient can drink. With only one manufacturer making the drug anymore, the price for that dosage has gone up from a few hundred dollars when Washington’s law started to more than $3,000.
“If you’re poor — and I have yet to see an insurance company pay for this, though I hear some will — then the cost falls into the lap of the patient or their family,” Bowden says. “That’s a barrier if you come from a poor part of the state.”
The most common reasons Washington patients told their doctors they wanted life-ending meds was because they were losing autonomy and the ability to engage in activities that make life enjoyable, with 84 percent to 100 percent of patients citing those two reasons every year from 2009 to 2016, the most recent for which state data has been released.
In contrast, inadequate pain control or concern about it was cited by 25 percent to 41 percent of patients, and only 2 percent to 13 percent cited concerns about the cost of medical treatment.
For many years, Pat and Melinda Hannigan lived in Seattle, where Melinda was an artist and Pat worked as a tanker pilot in Puget Sound. Melinda was hanging some of her paintings for a show in Tacoma when she had a shooting pain go through her head and half of her face became paralyzed. What they initially thought was a stroke was actually due to a tumor, part of an aggressive cancer that would spread to other parts of her body.
Hannigan tried every treatment available, but after years of radiation, chemotherapy and other therapies destroying her body, her quality of life was awful, Pat Hannigan says.
She could barely swallow or speak, was put on a feeding tube for more than a year and was confined to a wheelchair. After going on hospice care in the home the couple had built in Twisp, she decided to take the medication.
When it came time, Pat had to drive an hour to Omak to get the pills, which cost them about $4,400 out of pocket.
Hannigan shared a final dinner with her kids and grandkids and was surrounded by family when she took the lethal dose in July of 2016.
Pat Hannigan says it was the right decision for his wife and was in keeping with her choices to accept or decline treatment at every step of her illness. Still, he hasn’t spoken to many people about the experience, in part because he doesn’t want to influence others, who need to make that choice for themselves. However, he thinks those who oppose the law don’t understand what it’s like.
“I hear people criticize it and I think to myself, ‘They have never been through an experience like this in their lives,'” Hannigan says. “It’s really easy for them talk based on their religious beliefs or their philosophical principles, but if you live through four years of absolute, total hell, with no hope, Death with Dignity is an awesome thing.”
NOT FOR EVERYONE
Policies about physician participation under the act vary even within the same system.
For example, Providence physicians in Spokane are not allowed to participate under the rules of the act in any way, even though physicians at Swedish, a Providence-affiliated hospital in Seattle, are allowed to if they choose.
“We respect the rights of patients and their care team to discuss and explore all treatment options and believe those conversations are important and confidential. As part of a discussion, requests for self-administered life-ending medication may occur, but our providers do not participate in any way in assisted suicide,” writes Liz DeRuyter, director of external communications for Providence Health & Services. “We provide all other requested end-of-life and palliative care and other services to patients and families.”
MultiCare, the other large service provider in Spokane, does allow its physicians to participate as attending and consulting physicians, and they may write prescriptions. However, no MultiCare physicians or pharmacies can help patients fill the prescriptions, meaning they need to find another pharmacy to fill it.
In her efforts to increase access, Linda Estes is working with Providence to change the policy at its Tri-Cities affiliate hospital to allow physicians to participate under the law, even if that means doing so outside of the scope of the hospital system. She’s been in contact with a Providence attorney about helping draft that policy, which is under consideration.
Estes says she’s passionate about making that change because when a family member is dying, the last thing people need is additional stress around end-of-life decisions.
“When you’re grieving so hard, you don’t have brain cells left to deal with this,” Estes says. “Having been through it myself, and having been put completely through the ringer, I want to make sure this is an easier process to do. Not to say it’s the right choice for everyone, it’s just our choice.” ♦
A lethal prescription under Oregon’s Death with Dignity law.
[O]n the last morning of their lives, Charlie and Francie Emerick held hands.
The Portland couple, married for 66 years and both terminally ill, died together in their bed on April 20, 2017, after taking lethal doses of medication obtained under the state’s Death With Dignity law.
Francie, 88, went first, within 15 minutes, a testament to the state of her badly weakened heart. Charlie, 87, a respected ear, nose and throat physician, died an hour later, ending a long struggle that included prostate cancer and Parkinson’s disease diagnosed in 2012.
“They had no regrets, no unfinished business,” said Sher Safran, 62, one of the pair’s three grown daughters. “It felt like their time, and it meant so much to know they were together.”
In the two decades since Oregon became the first state to legalize medical aid-in-dying, more than 1,300 people have died there after obtaining lethal prescriptions. The Emericks were among 143 people to do so in 2017, and they appear to be the only couple to ever take the drugs together, at the same time, officials said.
The pair, early members of the 1980s-era Hemlock Society, had supported the choice for years, and, when their illnesses worsened, they were grateful to have the option for themselves, family members said.
“This had always been their intention,” said daughter Jerilyn Marler, 66, who was the couple’s primary caretaker in recent years. “If there was a way they could manage their own deaths, they would do it.”
Before they died, the Emericks agreed to allow Safran and her husband, Rob Safran, 62, founders of the Share Wisdom TV Network, of Kirkland, Wash., to record their final days and hours. At first, the video was intended just for family, but then Safran asked her parents for permission to share it publicly.
“I think it can help change the way people think about dying,” she said.
The result is “Living & Dying: A Love Story,” a 45-minute documentary that details the background of the Emericks’ final decision and their resolve in carrying it out.
Shot mostly with handheld smartphones, the video captures the intimate moments of the couple’s preparations in their last week of life.
Charlie Emerick was a former medical missionary in India and chief of ENT at a Portland-area Kaiser Permanente hospital. (Kaiser Health News is not affiliated with Kaiser Permanente.) He was diagnosed with Parkinson’s disease in 2012, after dealing with symptoms of the disease for years. He suffered from prostate cancer and heart problems and learned in early 2017 that he had six months or less to live. In the documentary, he described his thoughts as he pondered whether to use aid-in-dying.
“You keep going, Charlie, you’re going to get worse and worse and worse,” he explained to Sher Safran, in a quavering voice. “The other can’t be worse than this.”
Francie Emerick, who handled marketing and public relations for the hospital in India, appears vital and articulate in the video. Her daughters, however, say that her energy was fleeting and that it masked years of decline following multiple heart attacks and cancer.
In the video, Francie acknowledged that she could have survived a bit longer than her husband. But, she said, she didn’t want to.
“Charlie and I have a rather unique relationship in that we have done and been so much to each other for 70 years,” she said.
The pair carefully followed the specifics of the law, which requires examinations by two different doctors to determine a prognosis of six months or less to live, multiple confirmations of intent and the ability of patients to ingest the lethal drugs themselves. The process takes a minimum of 15 days.
“We do want it to be legal,” Francie said.
The video traces the arc of the couple’s lives. The Emericks met as college students in Nebraska, married on April 4, 1951, and spent years in the 1960s as medical missionaries in Miraj, India. Dr. Emerick’s career took them to Southern California and then to Washington state, to India and ultimately to Oregon, all while raising three girls. In 2004, they moved into an apartment in a retirement community in Portland.
That’s where the Emericks died on a cloudy Thursday last spring, six days after a family celebration that included their children and grandchildren — and, at Francie’s request, root beer floats. The gathering was happy, but bittersweet, family members said.
“There were moments that they expressed great sadness at the goodbye that was coming,” Marler recalled.
The Emericks sought help from Linda Jensen, a veteran team leader with End of Life Choices Oregon, a nonprofit agency that supports people seeking to use the state’s Death With Dignity law.
“They were pretty well informed,” said Jensen, who has assisted with dozens of deaths in 13 years. “What they wanted to understand was what a planned death really looks like.”
The video includes a meeting between Jensen and the Emericks two days before they died. It would be nothing like dying on TV, she told them.
“You do not lose control of your bowel or bladder. You do not gasp for breath,” she explained. Instead, she said, they would simply go to sleep.
The Emericks went over the plan: no breakfast, just pills to calm their stomachs at 9 a.m., followed by the lethal drugs an hour later.
Safran and Marler appear calm and determined as they help finalize their parents’ arrangements.
“There was a lot of grieving ahead of time because we knew it was coming,” Marler said.
Some members of the family disagreed with the couple’s decision, but the Emericks were determined.
“You two have never wavered?” Safran asked her mom.
“We have not,” Francie replied.
The video captured details of the final morning: Charlie saluting the camera farewell as he’s wheeled down the hall, Safran’s tearful last hug from her mother, Charlie and Francie clasping hands after they swallow the drugs.
“It just takes such a huge amount of internal strength and self-knowing to face that choice, to make that choice and then bring along all the people that love you and are going to miss you,” Jensen said.
There was no funeral after the deaths. The Emericks had donated their bodies for research through a program at the Oregon Health & Science University and any remains wouldn’t typically be returned for two or three years, a spokeswoman said.
In the interim, the video has become comforting and precious to the family, said Safran.
“It’s very lovely, just to hear their voices,” she said.
The documentary also serves a larger purpose: helping others to understand how aid-in-dying works, she said.
Carol Knowles, 70, was a member of Francie Emerick’s book club. The Emericks didn’t tell other residents about their plans. Knowles said she was surprised when they died the same day — until she saw the documentary.
“I thought it was brave and beautiful,” she said. “You could see the care with which Charlie and Francie had made that decision.”
Another member of the group expressed concern, however, saying her religion prohibited any efforts to hasten death. Knowles said she plans to take the documentary to the retirement center’s social worker before showing it more widely.
“We want to do it in a way that will not scare them or make them feel uncomfortable,” she said.
Stephen Drake, research analyst for the disability rights group Not Dead Yet, had serious reservations about making the video public. He worried that presenting aid-in-dying in a positive light “changes the expectations; this romanticizes the idea of not just suicide, but a double suicide,” Drake said.
Safran said she expects strong reactions — including criticism — for chronicling her parents’ final days. But she said the documentary honors the Emericks’ belief that, if possible, everyone should have a say in when and how they die.
“We have a faith that says life is not to be worshipped,” Francie said. “It’s the quality of life that counts.”
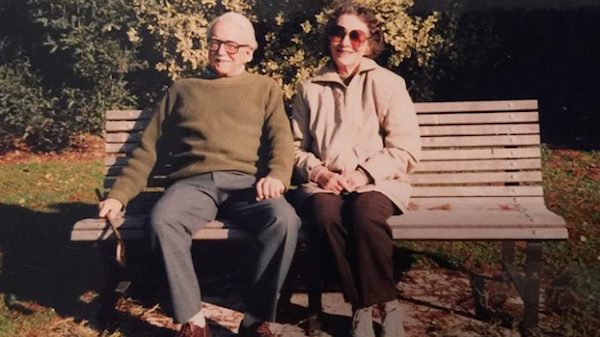
The author’s parents enjoying their retirement in New Zealand, 1991.
By Jane Peterson
[M]y mother’s last words were “It’s not working.” She slurred them before she fell into a deep sleep. Just prior to that, after ingesting medication mixed with applesauce, she had placed a plastic bag over her head and secured it. According to her meticulous research, this would hasten her passing.
Her death had been planned for months, if not years. Both my parents were members of The Voluntary Euthanasia Society in New Zealand, where they had retired from England to be close to my eldest sister and her children. Even though I had married an American and moved to rural Colorado, I was fortunate enough to be able to visit them every year and stay maybe two or three months.
Contemplating end of life
Our end-of-life discussions had been ongoing for many years, and both my parents were determined to die with dignity at a time of their choosing and before any needless and expensive medical procedures. Their wish was to pass away at home, as peacefully and as inexpensively as possible. As a family we agreed, with no hesitation. Now I pray that my sister and I can end our lives, legally, with the help of an enlightened physician, when quality of life is no longer an option.
My parents generally were in good health until my mother was diagnosed with rheumatoid arthritis at 82. This horrible disease was rampant on her side of the family—her beloved sister became ill in her 20s. She suffered mightily, without today’s wonder drugs that can alleviate some of the unpleasant symptoms, and died in her early 50s.
My mother had obtained a supply of Seconal from her doctor in London and had guarded her “stash,” with a mind to her eventual death. Despite the capsules being several years old, Mother did valuable research, including obtaining a prescription for anti-nausea pills, as well as taking six 10-mg Valium, with a glass of wine, before ingesting the lethal dose of Seconal. She had written separate goodbye notes to my father and to my sister and me. This was necessary to exonerate her family members in aiding and abetting her demise.
The final weeks of her life were filled with joy and laughter, and the planning took on a military aspect that my father, a lieutenant colonel in India during World War II, reluctantly took part in. I can honestly say that we had never laughed so much, despite the looming event that was ever present.
My mother’s pain was becoming increasingly unbearable and even sitting up in bed caused her appalling agony. The family doctor (they still made house calls in New Zealand) had given her Prednisone and Methotrexate. However, throughout her life, my mother had been unable to tolerate strong medications and she was terrified that the Prednisone was making her blind. The Methotrexate, on the other hand, messed with her mind. To our horror, a few weeks before, we found her lying outside in the driveway, in the pouring rain at 3 a.m., crying softly for help.
Goodness knows how long she had been there, and thank God I needed to use the bathroom in the middle of the night. When I checked her room and she was not in bed, I alerted my father. She was taken by ambulance to the nearest hospital and she remained there to be stabilized for a week.
Dying with dignity
Trying to keep on an even keel the morning of her death, I heard her speaking with my father who was asking her (again) if this was what she really wanted. I was cleaning up in the kitchen, and I am not ashamed to say that I lost it. I was privileged to have exceptional doctors in America and was prescribed suitable medication to help me through difficult times. This was definitely one of those occasions and I make apologies to no one.
Darling, darling Mother! So adamant that she could leave my sister and me as much money as she was able. She needed relief from her torture and, thanks to a long relationship with her family doctor in England, she was able to obtain it, in her own bed, surrounded by loving family. My sister and I monitored her pulse. It became weaker and weaker, until it was apparent that she had passed. The whole process took less than one hour.
It remains the most spiritual experience of my life, and I was similarly affected when my father died at home, just over a year later. Desolate after my mother’s death, he lost the will to live and had even asked my sister about getting a gun.
He passed away a week after being placed in a morphine-induced coma by his physician, so there was no verbal contact in his last days. Although he did not have to resort to my mother’s method, he succumbed to an illness that had no name since any diagnosis, advice or procedures that might have prolonged his life were adamantly refused. I suspect it was pancreatic cancer that prevailed.
He died around 11 a.m. on September 1, 1996, with me by his side, holding his hand and professing my love.
The right to make our own choices
As before, with my mother’s death, the funeral director who came to the house was incredibly disappointed when my sister and I firmly rejected his top of the line caskets. My parents always said that they wished to be cremated in matchboxes, a standing joke in our family for many years.
I give thanks every day for my parents’ decisions. My friends are coping with family members suffering from Alzheimer’s, dementia and worse. Their loved ones die in hospitals and nursing homes, lives needlessly prolonged. It results in loss of dignity, immeasurable suffering and devastating financial consequences.
I am so encouraged that more states have passed laws enabling physician-assisted dying (end-of-life options). To those of a similar persuasion, I urge you to become members of Compassion and Choices, based in Denver and available at 800-247-7421 or www.CompassionAndChoices.org. This progressive organization endorses Death With Dignity, and was instrumental in the Colorado voters passing the End-of-Life Options Act, now legalizing medical aid in dying. They continue their efforts in all states.
We should all be so fortunate to have the legal right to pass as we wish, and I say no state or federal agencies have any right to dictate how we make personal medical decisions.
[I]n May of 2016, Judith Dale was diagnosed with incurable Stage IV colorectal cancer that had metastasized to her liver and lungs. Having taken care of her mother when she was dying of cancer and witnessing its ravages, Ms. Dale wanted to die with dignity, something the California legislature permits patients with a terminal illness to do.
California, like several other states, has an End of Life Option Act (EOLOA) which “allows patients who have a terminal disease (with a life expectancy of six months or less) to request a life-ending drug prescription from their doctor.” Ms. Dale sought to avail herself of her rights under California law.
Sadly, she was denied that opportunity.
Ms. Dale would not have chosen her physician and medical center where she was treated unless they agreed to “respect and help facilitate her right to a more peaceful death via aid in dying,” according to the lawsuit filed against the physician and medical center. That lawsuit claims that the medical center and physician committed elder abuse/neglect, misrepresentation/fraud, negligent infliction of emotional distress, and negligence by failing to assist Ms. Dale with her final wish as it promised it would do.
As a result of the defendant’s failure, Ms. Dale’s “final weeks were brutal” and she suffered a “horrific death,” according to the lawsuit. This unfortunate story, which will be resolved in the courts, presents an opportunity for long-term care owners/operators and all healthcare practitioners to learn from it.
If not, they fail to do so at their peril, risking legal liability, among other adverse consequences.
States with End of Life Options Acts
Currently, five states and the District of Columbia have a Death with Dignity Act or End of Life Options Act. Those states are: California, Colorado, Oregon, Washington and Vermont. Montana does not have a statute regarding physician aid in dying, but its supreme court has ruled that state law does not prohibit a physician from honoring the wishes of a competent and terminally ill patient to receive a prescription that will hasten death.
In the states noted above, in order to receive a prescription for a lethal dose of medication, the patient must be at least 18 years old, be a resident of that state and have a terminal illness. Additionally, the patient must make two separate requests from his/her physicians at least 15 days apart.
As a safeguard, in the states that permit physicians to aid in dying, the physician must certify that the patient is medically competent to make that decision. In some states, such as Colorado, the patient must be referred to a consulting physician to confirm the diagnosis of competency.
The Colorado experience
Mount Evans Home Health & Hospice, in Evergreen, Colorado, was one of the Colorado hospices that had to determine its position and develop a policy and procedure after voters in Colorado passed the State’s first End of Life Options Act last year.
“The Mount Evans Home Health Care & Hospice Board of Directors felt it was important to engage in careful and thoughtful dialogue into the many complexities of this important issue,” said Charley Shimanski, President and CEO of Mount Evans. “This included elements such as supporting our clinical staff, weighing the differing board member viewpoints, and considering other support mechanisms available to patients/families.
“At the same time,” he adds, “we feel strongly that regardless of the path a patient chooses, we respect their choice and will provide the same comprehensive compassionate hospice services to all of our patients.”
Intersection of law, medicine, ethics
The issue of physician aid in dying is controversial at best and implicates the intersection of law, medicine and ethics. While the law allows for physician aid in dying in the states noted above, not all professional organizations have embraced or supported this growing movement.
For example, the American College of Physicians notes in its position paper that it “does not support legalization of physician-assisted suicide” in part because it “fundamentally alters the medical profession’s role in society.” Likewise, the Society for Post-Acute and Long-Term Care Medicine/American Medical Directors Association’s (AMDA) official position is that “AMDA opposes any physician involvement in assisted suicide or active euthanasia of any person regardless of age.”
Notably, professional organizations seem to have an evolving position on the issue of physician aid in dying. For example, the American Academy of Hospice & Palliative Medicine takes a position of “studied neutrality on the subject of whether PAD [physician assisted death] should be legally regulated or prohibited.” The Colorado Medical Society also took a “neutral” position when the issue was on the ballot, noting, “Ultimately, Proposition 106 [Colorado’s EOLOA] represents the most personal of decisions that must be left to our patients to determine.”
Mona’s final journey
Last Thanksgiving, I exchanged holiday greetings with Mona, a lifelong and dear friend. Days later, Mona’s sister called to say that Mona had had emergency surgery the day after Thanksgiving and then chose to be in hospice due to a terminal prognosis. I flew to the hospital/hospice facility in Nevada where my dear friend from childhood lay unconscious and slowly dying.
The “terminal morphine drip,” as it is referred to in medical community, kept Mona barely breathing and essentially unconscious for days. In spite of her decision for a hasty and dignified death given her terminal prognosis, she lingered in that unconscious state for days until she gasped her last breath.
As I held her hand, feeling completely helpless, I wondered if this slow ending was what Mona really wanted. Understandably, we may be reluctant to “let go” of loved ones but in the final analysis, each competent adult has the right to choose if he or she wants to die with dignity or soldier on and fight as long as possible.
In Mona’s case, she did not have the luxury of living in a state with an End of Life Options Act. And so it is with most terminally ill patients.
Recommendations
The most salient recommendation for long-term care providers is to have a well-reasoned policy and procedure, consistent with state law. If you are in the majority of states, the policy is straightforward: The law does not currently permit physician aid in dying, although that might change.
Consider how rapidly states began to legalize medical marijuana once that train left the station. For providers who are in states where physician aid in dying is legal, it is essential to have a policy that comports with your mission statement and values while respecting patients’ right. For example, hospice agencies in states with an EOLOA may choose to be “all in” and allow their medical directors and attending physicians to write the final prescription. Or, they may want no part of that process. Many hospices take a position in between the two extremes.
Few, if any decisions are as personal and far-reaching as the decision to end one’s life. Long-term care providers should be aware that it is likely that more state legislatures will enact End-of-Life-Options Acts. Until then, terminally ill patients will rely on the incredibly caring and competent long-term care providers, including hospices, physicians, nurses, and social workers, to ease their final journey.
[C]alifornia voters passed a law two years ago that allows terminally ill people to take lethal drugs to end their lives, but controversy is growing over a newer rule that effectively bans that option in the state’s eight veterans’ homes.
Proponents of medical aid-in-dying and residents of the Veterans Home of California-Yountville — the largest in the nation — are protesting a regulation passed last year by the California Department of Veterans Affairs, or CalVet, that requires that anyone living in the facilities must be discharged if they intend to use the law.
That’s a position shared by most — but not all — states where aid-in-dying is allowed. As more U.S. jurisdictions consider whether to legalize the practice, the status of terminally ill veterans living in state-run homes will loom large.
“It would be a terrible hardship, because I have no place to go,” said Bob Sloan, 73, who suffers from congestive heart failure and other serious cardiac problems. He said he intends to seek medical aid-in-dying if doctors certify he has six months or less to live.
“I’m not going to be a vegetable,” said Sloan, a Vietnam War-era veteran who moved into the Yountville center five years ago. “I’m not going to end up living in so much pain it’s unbearable.”
A CalVet official said the agency adopted the rule to avoid violating a federal statute that prohibits using U.S. government resources for physician-assisted death. Otherwise, the agency would jeopardize nearly $68 million in federal funds that helps run the facilities, said June Iljana, CalVet’s deputy secretary of communications.
California is not alone. Three other states where aid-in-dying is legal — Oregon, Colorado and Vermont — all prohibit use of lethal medications in state-run veterans’ homes.
In Montana, where aid-in-dying is allowed under a state Supreme Court ruling, officials didn’t respond to multiple requests about whether veterans would be able to use the law in the residences. However, Dr. Eric Kress, a Missoula physician who prescribes the lethal medication, says he has transferred patients to hospice, to relatives’ homes, even to extended-stay hotels to avoid conflict.
In Washington, D.C., where an aid-in-dying law took effect last summer, the Armed Forces Retirement Home won’t assist patients in any way. Those who wish to use the law would be referred to an ethics committee for individual consideration, spokesman Christopher Kelly said in an email.
Only Washington state has a policy that allows veterans to remain in government-run residences if they intend to ingest lethal medications.. At least one veteran has died in a state-run home using that law, said Heidi Audette, a spokeswoman for the state’s Department of Veterans Affairs.
Paul Sherbo, a spokesman for the U.S. Department of Veterans Affairs, said the choice is up to the states.
“VA does not mandate how states comply with federal law,” Sherbo said in an email. “There are a number of ways individual states can choose to handle such situations and still be in compliance.”
To date, none of the 2,400 residents of California’s veterans homes has formally requested medical aid-in-dying, said Iljana. That includes the more than 900 residents of the Yountville center, located about 60 miles north of San Francisco.
“We would respectfully and compassionately assist them in transferring to a hospice, family home or other location,” Iljana said in an email. “We will readmit them immediately if they change their minds.”
But Kathryn Tucker, executive director of the End of Life Liberty Project, an advocacy group that supports aid-in-dying, said that CalVet is interpreting the federal regulations too broadly and denying terminally ill veterans the right to choose a “peaceful death” through medical assistance.
“Nothing exists in the federal statute’s language that would prohibit a resident from receiving aid-in-dying services at state homes, so long as they are not provided using federal funds or employees,” she said.
Ed Warren, head of the Allied Council, a group representing veterans at the Yountville site, co-signed a letter to CalVet officials protesting the ruling.
“My point of view is that it is inhumane to expect people in the last stages of dying to go through the hullabaloo of leaving their homes,” he said.
In Washington state, a 60-year-old man diagnosed with terminal chronic obstructive pulmonary disease, or COPD, died in June 2015 after ingesting lethal drugs at the Washington Soldiers Home in Orting, where he lived.
“It was all done very much in the open,” said Chris Fruitrich, a volunteer with the group End of Life Washington, which assisted the man.
There has been no indication that the policy jeopardizes the nearly $47 million the agency receives each year in federal funds, said Audette, the state VA spokeswoman.
In California, additional protests have centered on allegations that CalVet suppressed information about the aid-in-dying law.
Critics at the Yountville home contend that CalVet passed the discharge rule quietly, with little public input. Then the agency refused to broadcast a public meeting about medical aid-in-dying on KVET, the center’s state-run, closed-circuit television station.
Iljana said the Aug. 21 meeting, led by Tucker and Dr. Robert Brody, also a supporter of aid-in-dying, violated state rules that prohibit using public resources to promote political causes.
“Free speech is great and criticizing the government is great, but not using the government’s own resources and paid staff to advocate for a change in the law,” Iljana wrote in an email to prohibit the broadcast.
That decision, however, prompted Jac Warren, 81, who has been KVET’s station manager for eight years, to resign last month in protest, citing censorship.
“What is at issue is whether a state may completely suppress the dissemination of concededly truthful information about entirely lawful activity,” Warren wrote in an email to CalVet.
The hour-long meeting, attended by about 50 people, was not propaganda, Tucker said, but “an educational event with information provided by an attorney and a physician who both specialize in their respective fields in end-of-life care.”
Bob Sloan, who works as an engineer at KVET for a $400 monthly stipend, disagreed with the decision not to broadcast the meeting on the system that serves residents of the Yountville home.
Sloan said he knows other residents who would like to be able to use California’s aid-in-dying law if their illnesses progress.
“The only other option that people have in this state is committing suicide,” he said. “If I can’t find some way of doing it legally, I’ll do it illegally.”
[W]hen my mother was in her final months, suffering from a heart failure and other problems, she called me to her bedside with a pained expression. She took my hand and asked plaintively, “How do I get out of this mess?”
As a physician, I dreaded the question that might follow: Would I help her end her life by prescribing a lethal drug?
Fortunately for me, my mother tolerated her final weeks at home, with the help of hospice nurses and occasional palliative medication. She never raised the thorny question of what is variously termed “medical aid in dying” or “physician-assisted suicide.”
As a son and family member who has witnessed the difficult final days of parents and loved ones, I can understand why support for MAID/PAS is growing among the general public. But as a physician and medical ethicist, I believe that MAID/PAS flies in the face of a 2,000-year imperative of Hippocratic medicine: “Do no harm to the patient.”
Studies point out that even many doctors who actually participate in MAID/PAS remain uneasy or “conflicted” about it. In this piece, I explore their ambivalence.
Assisted suicides
In discussing end-of-life issues, both the general public and physicians themselves need to distinguish three different approaches.
MAID/PAS involves a physician’s providing the patient with a prescription of a lethal drug that the patient could take anytime to end life. In contrast, active euthanasia or “mercy killing” involves causing the death of a person, typically through a lethal injection given by a physician. Finally, the term “passive euthanasia” refers to hastening the death of a terminally ill person by removing some vital form of support. An example would be disconnecting a respirator.
Increasing international acceptance
In the U.S. some form of legislatively approved MAID/PAS (but not active euthanasia) is legal in five states and the District of Columbia. In my home state – following a passionate debate – the Massachusetts Medical Society recently decided to rescind its long-held opposition to the practice. MMS has taken a position of “neutral engagement,” which it claims will allow it to “serve as a medical and scientific resource … that will support shared decision making between terminally ill patients and their trusted physicians.”
Physician-assisted suicide is finding more acceptance.
In a few countries, MAID/PAS has grown increasingly common. In Canada, for example, MAID/PAS was legalized in 2016. In Belgium and the Netherlands, both active euthanasia and physician-assisted suicide are permitted by law, even for patients whose illnesses may be treatable, as with major depression; and whose informed consent may be compromised, as in Alzheimer’s disease. In the Netherlands, a proposed “Completed Life Bill” would allow any persons age 75 or over who decide their life is “complete” to be euthanized – even if the person is otherwise healthy.
Perhaps this trend is not surprising. After all, what sort of physician would want to deny dying patients the option of ending their suffering and avoiding an agonizing, painful death?
But this question is misleading. Most persons requesting PAS are not actively experiencing extreme suffering or inadequate pain control. Data from the Washington and Oregon PAS programs show that most patients choose PAS because they fear loss of dignity and control over their own lives.
Some physicians feel conflicted
Physicians who carry out assisted suicide have a wide variety of emotional and psychological responses. In a structured, in-depth telephone interview survey of 38 U.S. oncologists who reported participating in euthanasia or PAS, more than half of the physicians received “comfort” from having carried out euthanasia or PAS.
“Comfort” was not explicitly defined, but, for example, these physicians felt that they had helped patients end their lives in the way the patients wished. However, nearly a quarter of the physicians regretted their actions. Another 16 percent reported that the emotional burden of performing euthanasia or PAS adversely affected their medical practice.
For example, one physician felt so “burned out” that he moved from the city in which he was practicing to a small town.
Other data support the observation that MAID/PAS can be emotionally disturbing to the physician.
Kenneth R. Stevens Jr., an emeritus professor at Oregon Health and Science University, reported that for some physicians in Oregon, participation in PAS was very stressful. For example, in 1998, the first year of Oregon’s “Death with Dignity Act,” 14 physicians wrote prescriptions for lethal medications for the 15 patients who died from physician-assisted suicide.
The state’s annual 1998 report observed that:
“For some of these physicians, the process of participating in physician-assisted suicide exacted a large emotional toll, as reflected by such comments as, ‘It was an excruciating thing to do … it made me rethink life’s priorities,’ ‘This was really hard on me, especially being there when he took the pills,’ and ‘This had a tremendous emotional impact.’”
As a physician and medical ethicist, I am opposed to any form of physician assistance with a patient’s suicide. Furthermore, I believe that the term “medical aid in dying” allows physicians to avoid the harsh truth that they are helping patients kill themselves. This is also the view of the very influential American College of Physicians.
I believe that the ambivalence and discomfort experienced by a substantial percentage of PAS-participating physicians is directly connected to the Hippocratic Oath – arguably, the most important foundational document in medical ethics. The Oath clearly states:
“I will neither give a deadly drug to anybody if asked for it, nor will I make a suggestion to this effect.”
In 5th century BC Greece, Hippocrates was something of a revolutionary in this respect. As the classicist and medical historian, Ludwig Edelstein has pointed out some non-Hippocratic physicians probably did provide poisons to their dying patients, in order to spare them protracted suffering. Hippocrates opposed this practice, though he did not believe that terminally ill patients should be exposed to unnecessary and futile medical treatment.
“From its very inception, the profession of medicine has formally prohibited its members from using their special knowledge to cause death or harm to others. This was – and is – a necessary protection so that the power of medicine is not used against vulnerable people.”
Indeed, when patients nearing the end of life express fears of losing control, or being deprived of dignity, compassionate and supportive counseling is called for – not assistance in committing suicide.
To be sure, comprehensive palliative care, including home hospice nursing, should be provided to the subset of terminally ill patients who require pain relief. But as physician and ethicist Leon Kass has put it: