Some people focus their fear of death on smaller and more manageable threats.
Awareness of our mortality is part of being human. As author and existential philosopher Irvin Yalom said, we are “forever shadowed by the knowledge that we will grow, blossom and, inevitably, diminish and die”.
There is growing research exploring the overwhelming anxiety that the inevitability of death, and our uncertainty about when it will occur, has the power to create. A social psychological theory, called terror management theory (TMT), is one way to understand how this anxiety influences our behaviour and sense of self.
Coping mechanisms
According to this theory, we manage our fear of death by creating a sense of permanence and meaning in life. We focus on personal achievements and accomplishments of loved ones; we take endless photos to create enduring memories; and we may attend church and believe in an afterlife.
These behaviours bolster our self-esteem and can help us feel empowered against death. For some, however, periods of stress or threats to their health, or that of loved ones, may result in ineffective and pathological coping mechanisms.
These people might focus their real fear of death on smaller and more manageable threats, such as spiders or germs. Such phobias may appear safer and more controllable than the ultimate fear of death.
We might take endless photographs to create a sense of permanence.
This makes sense because when we look closely at the symptoms of several anxiety-related disorders, death themes feature prominently.
When children experience separation anxiety disorder, it is often connected to excessive fear of losing major attachment figures – such as parents or other family members – to harm or tragedy from car accidents, disasters or significant illness.
People with panic disorder frequently visit the doctor because they’re afraid of dying from a heart attack. Meanwhile, those with somatic symptom disorders, including those formerly identified as hypochondriacs, frequently request medical tests and body scans to identify serious illness.
Finally, specific phobias are characterised by excessive fears of heights, spiders, snakes and blood – all of which are associated with death. Phobic responses to seeing a spider, for instance, typically involve jumping, screaming and shaking. Some researchers argue these extreme responses could actually represent rational reactions to more significant threats, such as seeing a person with a weapon.
Priming death
More evidence for the TMT hypothesis comes from studies showing that death anxiety is capable of increasing anxious and phobic responding.
Compulsive hand washers
These studies use a popular “mortality salience induction” technique to prime death anxiety in people with other anxiety disorders. The technique involvesparticipants writing down the emotions that the thought of their own death arouses, as well as detailing what they think will happen as they die and once they are dead.
Spider phobics primed like this had increased reactions to spiders, such as avoiding looking at spider-related images, when compared to spider phobics not primed with death. And compulsive hand washers spent more time washing their hands and used more paper towels when primed with death.
Given that we are all going to die at some point, death anxiety is a normal part of the human experience. For many of us, thinking about death can evoke fears of separation, loss, pain, suffering and anxiety over leaving those we love behind.
According to terror management theory, this fear has the power to motivate a life well lived. It stimulates us to cherish those we love, create enduring memories, pursue our hopes and dreams and achieve our potential.
Death anxiety is a normal part of human experience.
Death anxiety becomes abnormal when it forms the basis of pathological thoughts and behaviours that interfere with normal living. Many obsessive-compulsive hand washers and checkers spend significant amounts of time each day in ritualistic behaviours designed to reduce the threat of dirt, germs, fire, home invasion or threats to themselves and loved ones.
Similarly, those with phobias may go to extreme lengths to avoid what they fear and react with extreme distress when confronted with it. When these thoughts and behaviours lead to impaired functioning, anxiety is no longer considered “normal”.
Treatments, such as cognitive behaviour therapy, for a range of disorders may need to incorporate new strategies that directly address death anxiety. Without such innovation, the spectre of death may tragically haunt the anxious across their lifespan, until it is too late.
Communications skills training in medicine is patchy, undervalued and not a clinical imperative – but 90% of doctors say it should be mandatory
‘Promoting better communication can signal to every doctor that the difficult skill of really listening to patients is one that can be learned in the same way as suturing a wound.’
The new patient is an elderly, diabetic lady whose heart has been teetering on the edge of failure for the past two years. She likes saying that her husband’s death broke her heart – it might have been so but at age 80, diabetes, uncontrolled hypertension and a series of heart attacks have also taken their toll. The last little while has been particularly eventful, with practically a hospital admission each month despite maximal therapy.
She sees a different physician every time to tackle her immediate problem – fluid overload on one visit, diuretic-induced dehydration the next; sky high sugars one month, dangerously low ones the next. There are short-term solutions but no overarching intent of management. Everyone, including the patient, simply skids from one disaster to the next. She looks defeated and miserable. This time, her exhausted son pulls me aside and says, “I know you are the expert, but am I alone in thinking that treatment is futile?”
He was being sensible, not cruel, as he feared. He was right that treatment was futile and what was missing was a narrative of his mother’s long illness that included death as an end point. Avoiding even the mention of mortality, we were doing the patient, her family and ourselves a disservice.
His words brought home two truths. First, that patients are entitled to more thorough explanations and better conversations about their health. Second, that we are seeing an emerging theme in medicine, where patients and families are seeking to define the boundaries of care when doctors either don’t or won’t.
In fact, the timeless business of dying has never had a higher profile, which is why the results of a recent survey by the Royal Australasian College of Physicians make for sobering reading.
The RACP end of life working party, of which I was a member, surveyed more than 1,500 physicians to identify their knowledge and practice of advance care planning and end of life care. Unsurprisingly, the majority reported routinely caring for patients who were likely to die within 12 months. On a weekly basis, one third of doctors observed provision of treatments inconsistent with known patient wishes and one-third observed treatment with little chance of benefit.
And while doctors overwhelmingly agreed that discussing end of life care was important, only a minority actually translated the intention into action. Barriers included a lack of time but just under half of the physicians felt insufficiently trained to undertake what is easily one of the most consequential conversations in the doctor-patient relationship. As a result, a dismal 17% of physicians expressed confidence in knowing the end of life preferences of their patients.
More than any other group, apart from general practitioners, physicians are expected to conduct difficult and sensitive conversations with chronically ill patients to define goals, and hence, boundaries, of care. A surgeon’s adroitness with the scalpel is best paired with the wider perspective of a physician who deliberates whether the patient will survive the operation. A tricky biopsy is within the radiologist’s reach but it’s the physician who asks whether it’s the right thing to do. This is not to diminish one speciality or elevate another but merely to acknowledge that our combined skills are necessary to provide appropriate and judicious healthcare.
When it comes to sustained communication with hospitalised patients about complex and chronic illness and helping them navigate the end of life, the burden on physicians has always been higher, which is why it’s a worry when as a group, they express uncertainty about their ability to provide this core component of care.
At the end of life, physicians are typically the doctors expected to explore your deepest longings and regrets, your strongest convictions and worst fears. In between, they deliberate resuscitation status, stop antibiotics, encourage palliation and provide counsel to the frazzled resident who says, “He is dying but the family wants everything done. How should I respond?”
No matter how prepared one is for the end of life, for most of us there is accompanying consternation, grief and anxiety. One might reasonably expect a physician to be the custodian of good health but also the guarantor of comfort and dignity in death. It’s clear that physicians aspire to be that doctor but confess to needing help. In the survey, a staggering 90% of physicians thought that communication skills training should be mandatory.
It isn’t, you ask. No, and it has never been. Such training in medicine, especially when it pertains to end of life care, is patchy, undervalued and considered an optional extra rather than a clinical imperative. In an era where we have mapped the human genome and talk about cancer moonshots we have consistently failed to provide not just physicians, but all doctors, with the tools to be effective communicators.
It’s often feared that in discussing mortality a doctor will extinguish hope – and there is indeed a tension between maintaining hope and telling the truth – but patients tell us they value honesty and doctors know it’s the right thing to do.
Becoming a tactful, sensitive and honest communicator is a lifelong process but it’s important enough that it shouldn’t be left to chance. But this is exactly what medical schools and hospitals largely do. And then we lament that despite all the advances in medicine, doctor-patient communication remains a fraught problem that underpins a significant majority of healthcare complaints.
Hospitals hate removing doctors from the floor because it costs money. Many are dubious that communications training can alter a doctor’s fundamental approach to patients, so they end up dealing reactively with problems.
But promoting better communication can influence organisational culture by signalling to every doctor that the difficult skill of really listening to patients is one that can be learned in the same way as suturing a wound or interpreting an ECG.
Doctor-patient communication has long been viewed as an indulgence that comes at the cost of service delivery. Fire training is mandatory as is training in cultural sensitivity. It is mandatory to know how to resuscitate a patient but not how to broach end of life care.
Patients are increasingly taking charge of their needs and concerns at the end of life and physicians will be forced to listen and respond accordingly. It’s hard to find nine out of 10 doctors agreeing over anything. If they are clamouring to become better communicators, it’s time we took note.
After you’ve decided on a funeral home and are ready to begin the process of planning a funeral, your funeral director will ask you to come into the facilities for a visit. This personal contact with the people in charge of your loved one’s remains is an important step in the grieving process. Not only will you get to benefit from face-to-face interaction, but you’ll also be walked through each decision ahead of you.
Although every funeral home operates differently, most visits take on a fairly similar format. Expect yours to look something like this.
Initial Telephone Contact: Almost all funerals begin with a phone call to the funeral home of your choice. Your funeral director will tell you where to come to make the arrangements, set up an appointment, and let you know what types of items to bring with you. These often include financial papers as well as personal effects.
Meet the Staff: Your funeral director will be there to greet you when you arrive. This individual will become your primary point of contact for all the funeral plans you have ahead of you—and he or she will also become your partner in grief. Don’t be afraid to ask questions and accept support when you need it. That’s what the funeral director is there for.
Make Arrangements: After you arrive at the funeral home, you’ll most likely be led to a consultation room. Offering privacy and comfort, this room is where your funeral director will walk you through the process of making final arrangements. Even if the deceased had everything pre-planned or laid out in a will, the next-of-kin will be responsible for solidifying all decisions.
View Caskets/Options: While catalogs exist to help you visualize the details of the funeral, many funeral homes also have showrooms where you can see the caskets, linings, and urns for yourself. Many people find it comforting to make a tactile connection to these types of items.
Go Over Payment Plans: Paying for a funeral is a costly affair, even if the deceased set aside money for the final arrangements. Once you’ve decided on the type of funeral you’d like to hold, your funeral director will go over your payment options. No matter how difficult, this is a necessary conversation, and you will have to sign contracts before things can be set in motion.
A Moment to Reflect: It can be difficult to make these kinds of decisions all at once, so never be afraid to ask for a moment to yourself. No decisions have to be made during this initial consultation, so if you want time to talk to family members, have the contract looked over by a lawyer, or to slow down and think things through, you have every right to ask for time.
You also are not obligated to sign up for any services at all if you feel like the funeral home might not be a good fit. Although you may have to pay for transportation and service fees if you choose to have the body transferred to another home, you’re never locked into a funeral provider you don’t like until the contracts are signed.
The influx of for-profit companies into the hospice field has benefited patients, advocates say, because the commercial companies made big investments in technology, focused on efficiency and made care more accessible.
But a Washington Post analysis of hundreds of thousands of U.S. hospice records indicates that, as those companies transformed a movement once dominated by community and religious organizations into a $17 billion industry, patient care suffered along the way.
On several key measures, for-profit hospices as a group fall short of those run by nonprofit organizations.
The typical for-profit hospice:
Spends less on nursing per patient.
Is less likely to have sent a nurse to a patient’s home in the last days of life.
Is less likely to provide more intense levels of care for patients undergoing a crisis in their symptoms.
Has a higher percentage of patients who drop out of hospice care before dying. High rates of dropout are often viewed as a sign that patients were pushed out of hospice when their care grew expensive, left dissatisfied or were enrolled for hospice even though they were not close to death.
The quality of individual hospices varies widely. In some cases, for-profit hospices provide service at levels comparable to nonprofits, according to the review. But the data analysis, based on hundreds of thousands of Medicare patient and hospice records from 2013, shows that the gap between the for-profits as a whole and nonprofits is striking and consistent, regardless of hospice size.
Hospice profits vs. quality care
“Unfortunately, a lot of people have come into the business for the wrong reasons,” said Michael Girard, who with his wife Deb owns the Circle of Life for-profit hospice in Reno, Nev. “A lot of the problems we have in hospice today have happened with the entry of what I call the ‘vulture capitalists.’ ”
About half of Americans of retirement age will employ a hospice service before death, but public information about the agencies is meager, and many consumers are unaware whether a hospice operates as a nonprofit or for-profit.
The federal government has been trying — for years — to develop a way to measure and report hospice quality, but the effort has lagged behind other health-care industries. The Washington Post has published an online hospice guide that provides detailed information on more than 3,000 hospices.
The findings on for-profit hospices come amid repeated complaints within the industry that pressure to cut costs, combined with sparse government oversight, has led some companies to focus on the bottom line to the detriment of patients.
Hospice operators have an economic incentive to provide less care because they get paid a flat daily fee from Medicare for each of their patients. That means that the fewer services they provide, the wider their profit margin.
Industry advocates warned against using the findings to rule out care from a for-profit hospice.
“There are many, many factors in making a decision about what hospice to choose,” said Theresa M. Forster, vice president of the National Association for Home Care & Hospice, which represents for-profit and nonprofit hospices. “National trends may not apply at the local level. The key issues are the hospice’s ability to provide good end-of-life care.”
Through a spokesman, the National Hospice and Palliative Care Organization, another industry group, declined to comment on the findings.
Dave Williams, the chief financial officer of Chemed, which owns the largest U.S. hospice chain, said that for-profits offer several advantages for patients: They can more easily raise money for investments in equipment and expansion; they can achieve a size that offers them economies of scale; and, pushed by investors, they are encouraged to be more efficient.
He emphasized that size and scale matter because a large hospice can afford to lose money on some patients who may need extraordinary care.
“For large hospices that have been around a long time, the quality of care is going to be the same, whether they are for-profit or nonprofit,” Williams said. “The only way you can compete for patients and referrals over a long period of time is to provide the best possible care.”
***
The rise in hospice usage — today roughly half of older Americans who die have received some hospice care — has created a boom in the industry. In 2012, Medicare spent more than $15 billion on hospice care, which offers terminally ill patients treatment that focuses on providing comfort rather than aggressive methods aimed at a cure.
The number of hospice firms has risen rapidly, and over the past decade the growth has come almost entirely from new for-profit operations. Between 2000 and 2012, the number of for-profit hospices tripled to 2,196, according to federal figures, compared with about 1,500 nonprofit hospices, including those run by local governments.
The industry growth has been accompanied by remarkable turbulence, too. Between 1999 and 2009, more than 40 percent of hospices experienced one or more changes in ownership, according to researchers.
The expansion has been driven in large part by investors, including private equity firms, hedge funds and entrepreneurs. More than a dozen private equity firms have invested in businesses that provide hospice care, including giants such as The Carlyle Group, Kohlberg & Company, Summit Partners and GTCR.
“Hospice [mergers and acquisitions] market is red hot (peak valuation levels),” according to a presentation by financial analysts at Cain Brothers last year, which cited, among other things, the favorable U.S. demographics — more old people.
“Hospice continues to be of robust interest to Wall Street,” said Carsten Beith, a managing director at Cain Brothers.
He said the influx of private equity money has allowed the industry to expand and to fund investments in technology. The demands of investors have also pushed hospices to provide good care at lower costs and a hospice that spends less on nursing is not necessarily providing less care, he said.
“An operating model that is more efficient doesn’t translate into patient care deficiencies,” Beith said.
But some in the industry — often those in the traditional nonprofit hospices — have questioned whether the goals of a for-profit company and a dying patient are easily aligned.
“If you think as a businessman and you want to make money, you will cut and cut and cut,” said Helen Zebarth, who cofounded the nonprofit Blue Ridge Hospice in Winchester, Va., in 1979.
A former cardiac nurse, Zebarth decided to create a hospice after visiting the famed St. Christopher’s hospice in London in the mid-’70s.
Back in Winchester, she and colleagues operated the fledgling operation on a shoestring budget out of a hospital basement. At the time, hospice services had to be paid for by donations because insurance and Medicare didn’t cover it.
“It was free for everyone,” she said. “And the community supported it.”
She credits the beginning of Medicare and insurance coverage with allowing far more people in the United States to receive hospice services.
But it also turned hospice into a big business, which operates side-by-side with the visionaries remaining from the movement’s early days.
Today, the amount the Blue Ridge Hospice spends on nursing per patient is more than 50 percent higher than the state average. It offers an array of extra services, including music therapy. It accepts patients with no insurance coverage. It also built its own inpatient unit.
It pays for the extras with donations from the community and a string of thrift shops it operates.
“We really want to take care of people — that’s our goal,” Zebarth said. “That’s where we are focused.”
***
The debate over the role of for-profit companies has come up before in health care, most often with hospitals. Within that field, some researchers have found generally negligible differences between the care provided by for-profits and nonprofits.
“When simple measures of quality are used — such as mortality — we have not seen differences between the quality of for-profit and nonprofit hospitals,” said Frank Sloan, a Duke University health and economics professor.
Where the two vary, he said, is in business practices, with for-profit hospital chains more aggressively marketing other services to patients.
By contrast, significant differences appear to distinguish for-profit and nonprofit hospices.
The Post analysis is based on the 2013 cost reports and other billing data that hospices are obliged to file if they accept Medicare patients. Medicare pays for the vast majority of hospice care in the United States.
While they are not audited, the reports are supposed to reflect what the hospice spends each year in caring for patients.
The key findings:
Nonprofit hospices typically spent about $36 a day per patient on nursing visits; for-profit hospices spent $30 per day, or 17 percent less. The gap between for-profits and nonprofits remains whether the hospices are old or new.
Nonprofit hospices are much more likely to provide the more intense services — continuous nursing and inpatient care — required by patients whose symptoms are difficult to control. Nonprofits offered about 10 times as much of this per patient-day as did for-profits.
While hospices of both kinds usually dispatch a nurse to see a patient at some point during the last two days of life, for-profit hospices are more likely to fail in this regard, according to the analysis. A typical patient at a for-profit hospice is 22 percent less likely to have been visited by a nurse during this window than a patient at a nonprofit hospice, the numbers show, a sign that for-profit hospices may be less responsive during this critical time.
Patients at for-profit hospices are much more likely to drop out of hospice care than patients at nonprofit hospices.
The proportion of patients leaving a for-profit hospice is typically 22 percent, while it is only 14 percent at nonprofits.
The rate at which patients leave a hospice alive is a closely watched measure of quality.
“An extraordinarily high live discharge rate is indicative of financial motivations driving a hospice rather than patient care,” said Rich Chesney, chief executive of Healthcare Market Resources, a market research company that provided 2012 live discharge rates to the Post. (For its analysis, the Post obtained current data on discharge rates from the federal government.)
Patients may be leaving such hospices because “patients are dissatisfied with hospice or didn’t understand what they were getting into in the first place — that is, the hospice failed in the admissions process.”
The gap between for-profits and nonprofits was generally consistent even when geography, age of the hospice and diagnoses were taken into account. Older hospices of both kinds — for-profit and nonprofit — appeared to perform better than new hospices, according to the statistics.
Some previous academic studies have found other differences between for-profits and nonprofits.
Elizabeth Bradley, a Yale health policy professor, has conducted several such studies and found that for-profit hospices appear to offer less for patients: that nursing staffs at for-profit hospices had a smaller proportion of registered nurses; that patients at for-profit hospices received a narrower range of services; and that for-profit hospices were more likely to restrict enrollment of patients with potentially high-cost care.
Bradley notes that in at least one respect, for-profits do better than nonprofits: she and her colleagues found that for-profits are more likely to engage in outreach to low-income communities.
“I’m delighted that the for-profit hospices are expanding access by reaching low-income and minority communities,” Bradley said. “But someone needs to be watching to make sure that their strategies for maximizing their returns don’t end up compromising the quality of care.”
***
The differences between for-profits and nonprofits even show up in what kinds of pain relief are available.
Take, for example, a specific cancer treatment known as palliative radiation.
While the treatment is not intended to cure a patient, it can shrink tumors and ease pain. It is, however, expensive to provide and hospices often lose money when they do so — in other words, it cuts into profits.
Research has shown that nonprofit hospices are much more likely to offer the treatment to patients. The odds that a nonprofit hospice uses palliative radiotherapy are 2.5 times greater than the rate for a for-profit hospice, according to the 2009 research from the University of Minnesota. The Post analysis also found such differences.
Geoff Coleman, chief medical officer at Montgomery Hospice, a nonprofit group, said that he sometimes recommends palliative radiation at times. But when he worked at a for-profit hospice, the staff was not allowed to give patients palliative radiation, he said.
“Essentially I was told, ‘We’re not going to do those kinds of therapies,’ ” he said, a decision he said he disagreed with. “The administrators were adamant that it was not in their purview. Sometimes, the smaller hospices just don’t have the funds.”
Anna Williams, 82, last year received palliative radiation as a patient of Montgomery Hospice after her oncologist recommended it.
Her daughter said that because Williams’s condition was deteriorating rapidly, it was hard to tell what effect it had on her mother, a former nurse she described as a “gentle spirit.”
“We knew it wasn’t going to save her,” said her daughter, Edie Gordon. “But the doctor said the radiation could bring her some relief. We just wanted to make her comfortable. It was something hopeful.”
Montgomery Hospice is better able to afford such care because, like other nonprofits, it receives a large portion of its operating budget from donations. About 11 percent of its $22 million budget comes from donations every year.
Given the budget pressures facing hospices, oversight is critical to making sure that financial demands do not trump patient care.
But regulatory scrutiny of hospices has lagged behind those of other health-care institutions, though Congress has recently called for more frequent inspections. And without as much oversight, hospice operators can operate in ways that benefit shareholders more than patients.
“With hospitals, whatever financial motivations to provide less or inappropriate care is more likely to be blunted by regulation and oversight and quality measures,” said Harold Miller, president of the Center for Healthcare Quality and Payment Reform. “We’re not there yet with hospices.”
In “How Doctors Die,” a powerful essay that went viral in 2011, a physician described how his colleagues meet the end: They go gently. At the end of life, they avoid the mistakes — the intensive, invasive, last-ditch, expensive and ultimately futile procedures that many Americans endure until their very last breath.
“Of course, doctors don’t want to die; they want to live. But they know enough about modern medicine to know its limits,” Ken Murray wrote.
A new study reveals a sobering truth: Doctors die just like the rest of us.
“We went into this with the hypothesis we were going to see very large differences,” said Stacy Fischer, a physician who specializes in geriatrics at the University of Colorado School of Medicine. “What we found was very little difference to no difference.”
The study in the Journal of the American Geriatrics Society examined 200,000 Medicare beneficiaries to bring some hard data to the question. They found that the majority of physicians and non-physicians were hospitalized in the last six months of life and that the small difference between the two groups was not statistically significant after adjusting for other variables. The groups also had the same likelihood of having at least one stay in the ICU during that period: 34.6 percent for doctors vs. 34.4 percent for non-doctors. In fact, doctors spent slightly longer in the ICU than non-doctors, the study found — not enough time to signify a clinical difference, but suggesting that, if anything, doctors may be using medicine more intensively.
In one regard, doctors seemed to die slightly better than non-doctors: 46.4 percent of doctors used hospice during their last six months compared with 43.2 percent of non-doctors. Doctors also spent nearly 2½ more days in hospice than non-doctors.
But these differences are small, and overall, they are far from the powerful mythology that doctors are dying better than the rest of the populace.
“Doctors are human, too, and when you start facing these things, it can be scary, and you can be subject to these cognitive biases,” said Daniel Matlock of the University of Colorado School of Medicine.
This is striking because it is the opposite of what doctors say they’d prefer. Onesurvey asked doctors and their patients what treatment course they would choose if they were faced with a terminal illness. Doctors said they would choose less medicine than their patients in almost all cases.
Many people have witnessed a death that seemed to be exacerbated by modern medicine: a drug that came with side effects but never seemed to halt the disease’s progress, the surgery that was totally unnecessary and might even have sped up someone’s death. Doctors have seen that happen even more often.
“Patients generally are not experts in oncology, and yet they have to make decisions without knowing what the whole course of their illness will be,” wrote Craig C. Earle in the Journal of Clinical Oncology. “We, on the other hand, have shepherded many patients through this journey toward death.”
That’s why powerful anecdotes about doctors who die better, whose last moments are spent peacefully and with family, give us hope: There is a better way.
But Matlock and Fischer think that their data may reveal the odds against the patient, even when the patient is a doctor. The health-care system may simply be set on a course to intervene aggressively.
“These things that encourage low-value care at the end of life are big systems issues,” Matlock said. “And a strong, informed patient who knows the risks and benefits — maybe even they have a hard time stopping the train.”
There are definite limits to the study: It could not control for differences in education or income among people in the sample. The doctors who died were mostly white men.
But the findings may reveal a deep bias that lies at the root of medicine. Fischer pointed out that the entire health-care system is aimed at fixing problems, not giving comfort. For example, a hip replacement the day before someone dies is something the medical system is equipped to handle: Surgeons can schedule it, and health insurance will pay for it. But, Fischer pointed out, if a patient needs less-skilled home care — such as help with feeding and bathing at home, it’s much harder to write a prescription.
Lonny Shavelson is consulting with doctors who have questions about California’s “End of Life Option Act.” He will also see patients after the law takes effect next week.
Few people have the unusual set of professional experiences that Lonny Shavelson does. He worked as an emergency room physician in Berkeley for years — while also working as a journalist. He has written several books and takes hauntingly beautiful photographs.
Now he’ll add another specialty. Just as California’s End of Life Option Act, a law legalizing physician aid-in-dying for people who are terminally ill, is set to take effect next week, Shavelson has become a consultant aimed at answering questions from physicians and patients about the practice — even becoming a physician to terminally ill patients seeking to end their lives.
Oregon was the first state to approve the practice, and in 1996 the law was held up in court. I turned to Shavelson as he had published “A Chosen Death,” a moving book following five terminally ill people over two years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue of assisted suicide closely for several years more, but ultimately moved on to other major projects — among them a book about addiction and a documentary about people who identify as neither male nor female.
Now he’ll add another specialty. Just as California’s End of Life Option Act, a law legalizing physician aid-in-dying for people who are terminally ill, is set to take effect next week, Shavelson has become a consultant aimed at answering questions from physicians and patients about the practice — even becoming a physician to terminally ill patients seeking to end their lives.
Oregon was the first state to approve the practice, and in 1996 the law was held up in court. I turned to Shavelson as he had published “A Chosen Death,” a moving book following five terminally ill people over two years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue of assisted suicide closely for several years more, but ultimately moved on to other major projects — among them a book about addiction and a documentary about people who identify as neither male nor female.
Now he’ll add another specialty. Just as California’s End of Life Option Act, a law legalizing physician aid-in-dying for people who are terminally ill, is set to take effect next week, Shavelson has become a consultant aimed at answering questions from physicians and patients about the practice — even becoming a physician to terminally ill patients seeking to end their lives.
Oregon was the first state to approve the practice, and in 1996 the law was held up in court. I turned to Shavelson as he had published “A Chosen Death,” a moving book following five terminally ill people over two years as they determined whether to amass drugs on their own and end their lives at a time of their choosing. He was present at the death of all of them.
He followed the issue of assisted suicide closely for several years more, but ultimately moved on to other major projects — among them a book about addiction and a documentary about people who identify as neither male nor female.
The wall of Lonny Shavelson’s office, lined with covers of the books he has written.
Shavelson decided he had to act, although he feels “quite guilty” about having been away from the issue while others pushed it forward.
“Can I just sit back and watch?” Shavelson told me from his cottage office in his backyard in Berkeley. “This is really an amazing opportunity to be part of establishing policy and initiating something in medicine. This is a major change … [that] very, very few people know anything about and how to do it.”
His website, Bay Area End of Life Options, went up in April, and he’s outlined the law at “grand rounds” at several Bay Area hospitals this spring. His practice will be focused on consulting not only with physicians whose patients request aid-in-dying, but also with patients themselves, including offering care to patients who choose him as their “attending End-of-Life physician,” as he indicates on his site.
Shavelson is adamant that this is “something that has to be done right.” To him, that means starting every patient encounter with a one-word question: “Why?”
“In fact, it’s the only initial approach that I think is acceptable. If somebody calls me and says, ‘I want to take the medication,’ my first question is, why? Let me talk to you about all the various alternatives and all the ways that we can think about this,” he predicts he will say.
Shavelson worries that patients may seek aid-in-dying because they are in pain, so first, he would like all his patients to be enrolled in hospice care.
“This can only work when you’re sure that the patients have been given the best end-of-life care, which to me is most guaranteed by being a part of hospice or at least having a good palliative care physician. Then this is a rational decision. If you’re doing it otherwise, it’s because of lack of good care.”
California is the fifth state to legalize aid-in-dying, joining Oregon, Washington, Vermont and Montana. The option is very rarely used. For example, in 2014 in Oregon, 155 lethal prescriptions were written under the state’s law, and 105 people ultimately took the medicine and died, a death rate under this method of less than 0.5 percent.
Under the law, two doctors must agree that a mentally competent patient has six months or less to live. One of the patient-doctor meetings must be private, between only the patient and the physician, to ensure the patient is acting independently. Patients must be able to swallow the medication themselves and must state, in writing, within 48 hours before taking the medication, that they will do so.
Shavelson says he has been surprised by the lack of understanding he hears from some health care providers about the law. One person insisted the law was not taking effect this year; another asked how the law would benefit his patients with Alzheimer’s disease. To be clear, the law takes effect next week, and patients with dementia cannot access the law because they are not mentally competent.
The law does not mandate participation by any health care providers. Many physicians are “queasy” with the new law, Shavelson says he’s hearing, and are unwilling to prescribe to patients who request the lethal medication — even though they tell him they think the law is the right thing to do.
Renee Sahm, one of five terminally ill people followed by Lonny Shavelson in his 1995 book “A Chosen Death.”
“My response to that is as health care providers, you might have been uncomfortable the first time you drew blood. You might have been uncomfortable the first time you took out somebody’s gall bladder,” he says. “If it’s a medical procedure you believe in and you believe it’s the patient’s right, then it’s your obligation to learn how to do it — and do it correctly.”
Shavelson said he predicts that many physicians who are initially reluctant to provide this option to their patients may become more comfortable after the law goes into effect and they see how it works.
Burt Presberg, an East Bay psychiatrist who works specifically with cancer patients and their families, said a talk he attended by Shavelson sparked a conversation at his practice. Yet, in my own talk with him, he peppered his statements with “on the other hand,” as he clearly wrestled with his own comfort level of handling patient requests.
Presberg spoke of his concern that patients suffer from clinical depression at the end of life, sometimes feeling they are a burden to family members who could “really push for the end of life to happen a little sooner than the patient themselves.” He spoke from his experience of successfully treating terminally ill patients with clinical depression.
“Depression is something that’s really undertreated,” Presberg said. “I often talk to people about the difference between normal sadness and normal grieving at the end of life.”
He said he believes Shavelson will be aware of treating depression, “but I do have concerns about other physicians,” he said. “On the other hand, I think it’s really good that this is an option.”
Shavelson says he’s already received a handful of calls from patients, but he’s mostly spent this time before the law takes effect talking to other physicians. He needs a consulting physician and a pharmacist that will accept prescriptions for the lethal dose of medicine.
Then he returns to the patient. “It’s important … that we’re moving forward,” he says. “It’s crucial that we do that because this is part of the rights of patient care to have a certain level of autonomy in how they die.”
To many of the doctors who feel “queasy” about moving to end a patient’s life, this type of care “isn’t so tangibly different to me,” Shavelson says, than other kinds of questions doctors address.
“I’m just one of those docs who sees dying as a process, and method of death is less important than making sure it’s a good death.”
“Things were a little ghostly,” wrote a reporter for the Philadelphia Times, setting the scene for a morbid public spectacle. The press had been invited to the first “modern” cremation performed in the United States. It was December 6, 1876.
The Times reporter was among a crowd of journalists and townspeople gathered at the top of a hill in Washington, Pennsylvania to witness the first run of a new crematory built by Dr. Francis Julius LeMoyne. The furnace, designed by LeMoyne and built on his own property, was based on a working model presented at the Vienna Exposition in 1873. The remains to be cremated were those of Joseph Henry Louis Charles, Baron de Palm, a Theosophist who was fascinated by “Eastern” philosophy, and besides that had once known a woman who had been buried alive, and was terrified by the prospect.
Burning the dead is an ancient practice, and in some cultural traditions, it’s a thousands-year-old norm. Today, cremation in the U.S. is soaring in popularity; by 2018, the Cremation Association of North America predicts that over 50 percent of Americans will choose to have their bodies cremated.
Dr. Francis Julius LeMoyne.
But in late 19th-century America, cremation was a radical, tradition-bucking idea. LeMoyne and other cremation advocates believed that burying the dead in the ground allowed germs to seep into the soil, thus contributing to the spread of diseases like cholera, typhus, and yellow fever. Cremation promised to sterilize human remains and bypass the altogether slow and icky process of decomposition. When performed in a state-of-the-art indoor furnace, it was a sanitary and high-tech alternative to burial.
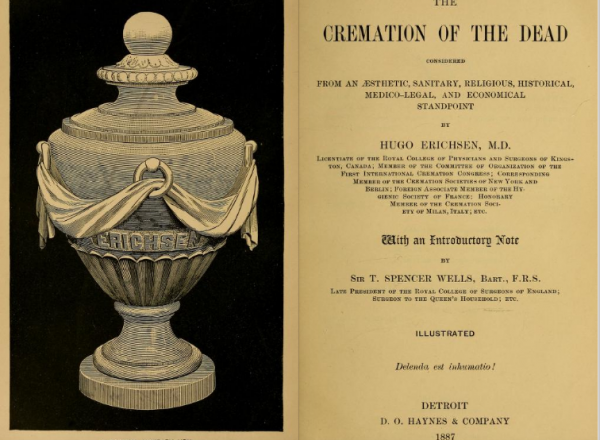
Cremation was also a solution to an urban problem. As cities expanded, they surrounded burial grounds that had once been miles away from town—and rested on prime real estate. “In and about New York, Brooklyn, and Jersey City, 4,000 acres of valuable land are taken up by cemeteries,” wrote Hugo Erichsen in his 1887 pro-cremation treatise The Cremation of the Dead. “It is calculated that with the probable increase of population in the next half a decade, 500,000 acres of the best land in the United States will be enclosed by graveyard walls. … It is an outrage!”
But cremation didn’t catch on with the masses right away. LeMoyne had first approached a local cemetery with an offer to build the crematory on their land; they dismissed him with disgust. The Times reporter who witnessed the de Palm cremation was horrified: “If [de Palm] could have foreshadowed the startling scenes his poor bones would have to go through he would have thought twice before he jumped into the fire.” Anti-cremationists put aside their religious discomfort with cremation to argue that burning bodies would encourage crime—you can’t exhume a cremated corpse!—and dismissed the public health claims of cremationists as unfounded fear-mongering. (They weren’t wrong; there’s no evidence that in-ground burial encouraged the spread of epidemics.)
Cremation was also a solution to an urban problem. As cities expanded, they surrounded burial grounds that had once been miles away from town—and rested on prime real estate. “In and about New York, Brooklyn, and Jersey City, 4,000 acres of valuable land are taken up by cemeteries,” wrote Hugo Erichsen in his 1887 pro-cremation treatise The Cremation of the Dead. “It is calculated that with the probable increase of population in the next half a decade, 500,000 acres of the best land in the United States will be enclosed by graveyard walls. … It is an outrage!”
But cremation didn’t catch on with the masses right away. LeMoyne had first approached a local cemetery with an offer to build the crematory on their land; they dismissed him with disgust. The Times reporter who witnessed the de Palm cremation was horrified: “If [de Palm] could have foreshadowed the startling scenes his poor bones would have to go through he would have thought twice before he jumped into the fire.” Anti-cremationists put aside their religious discomfort with cremation to argue that burning bodies would encourage crime—you can’t exhume a cremated corpse!—and dismissed the public health claims of cremationists as unfounded fear-mongering. (They weren’t wrong; there’s no evidence that in-ground burial encouraged the spread of epidemics.)
Inside the Detroit Crematorium columbarium at Woodmere Cemetery.
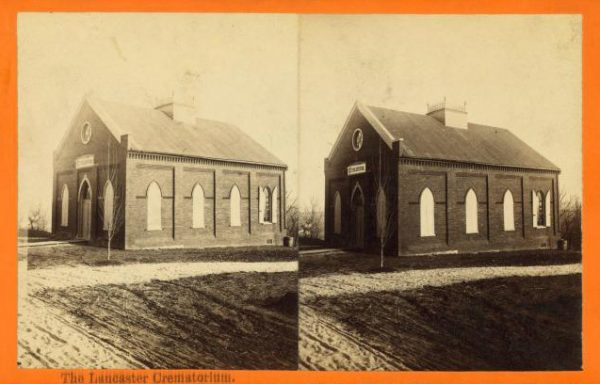
Throughout the 1870s and ’80s, as debates about cremation raged in the papers, local cremation societies were organized to argue their case and — more importantly—to raise funds to build crematories. The first public crematory in the U.S., at Lancaster, Pennsylvania—funded by the Lancaster Cremation and Funeral Reform Society—was built in 1884. By 1887, Cincinnati, Buffalo, Los Angeles, and Detroit had all built crematories, many of them designed to look like chapels, with stained glass and stonework. These crematories operated independently of cemeteries, which saw cremationists as competitors.
A few of these early crematories still exist; in Cincinnati, the building is hiding behind deceptive new construction.
The opening pages to 1887 book The Cremation of the Dead.
Sometimes the dead traveled hundreds of miles to have their last wishes fulfilled. When Barbara Schorr died in Millersburg, Ohio in 1887, her family honored her wish to be cremated by sending her body to the Detroit Crematorium—nearly 200 miles away, it was nonetheless the closest crematory. But it was still under construction, so Barbara Schorr lay in state for several weeks while it was completed.
Today, a portrait of Barbara Schorr, commissioned by her sons, hangs in the columbarium at Woodmere Cemetery, honoring her as a pioneer of the cremation movement in Detroit.
A stereoscope view of Lancaster Crematorium, Pennsylvania.
Because cremation was a moral crusade for the betterment of public health, it attracted sympathizers from other moral causes to its ranks, including no small number of women activists. The suffragist Lucy Stone was the first person cremated at the Forest Hills Crematory in Boston in 1893. Frances Willard—suffragist, temperance activist, and avid bicyclist—was also a vocal advocate of cremation. In 1900, the New York Times ran a satirical news item about the cremation of Willard’s cat: “Each of Toots’s human friends will sprinkle a little myrrh or frankincense over the body, and while it is being consumed the incense will counteract any odor which might be emitted through the furnace chimney.”
By the early 20th century, the sensationalism of cremation had waned, and the practical case for cremation was winning minds. After all, cremation, which requires no elaborate monument marker or plot purchase, is significantly less expensive than in-ground burial. Eventually, cemetery directors realized they might be better off joining the cremationists than trying to beat them. In 1899, Mount Auburn Cemetery—famously one of the original rural cemeteries in the U.S.—hired an architect to renovate an existing chapel on the grounds into a crematory. It was the first cemetery crematory in the state of Massachusetts, and it marked a turning point in the history from what was once a “ghostly” spectacle to an agreeably American way of death and burial.