In recent years, many Americans have begun looking for new ways to approach death. The death-positive movement supports people who prefer to die at home, and even those who wish to care for the bodies of loved ones the way many families did before the rise of the funeral industry. Historian Karol K. Weaver took a close look at that earlier approach, studying the business of death in early nineteenth century Pennsylvania, when care for the dying and dead fell mostly to women.
In those years, Weaver writes, watchers or watch-women—sometimes also referred to with the more generic term “nurse”—tended to the dying. These might be friends, family members, or hired help.
The watchers offered physical care and prayer, and organized visits by clergy and loved ones. Another important part of their job was observing the attitude of the dying person. If they could report a Good Death—characterized by courage and faith—it would comfort the other survivors. On the other hand, a Bad Death filled with struggle and pain could make for a cautionary tale aimed at the insufficiently pious.
Weaver writes that the final and most important job of a watcher was to verify that her charge was dead, observing the cessation of breath and even shaking the body to be sure no life remained.
Once the watcher’s work was done, “layers out of the dead” would wash, dress, and groom the body. They would also close the mouth of the deceased, using a tied cloth or a stick propped between the chin and breastbone, and use coins or other objects to keep the eyes closed. Layers out might also perform the skilled jobs that would later fall to undertakers, such as removing internal organs, blocking orifices, and slowing putrefaction by applying alum-covered cloth or filling body cavities with charcoal.
Like watchers, some layers out were unpaid family members or friends, but others were paid professionals. Looking at Philadelphia city directories from the early nineteenth century, Weaver found business listings for these women. Sometimes, they also advertised themselves as nurses or midwives—jobs that involved intimate care in a domestic setting just as laying out the dead did. Some listed themselves as “widows” in the directories. Weaver writes that this title suggested their connection with death and also explained the lack of a husband’s income that forced them to work for money.
Over the following decades, women’s death work declined. Increasingly, people died in hospitals rather than at home. With the Civil War came the need to transport Union soldiers’ bodies home, inspiring the rapid growth of undertaking as a business—often a father-and-sons affair. Now, families had a one-stop shop for coffin, burial plot, hearse, and the care and preservation of the body.
By 1867, the Philadelphia directory listed 125 male undertakers, one female undertaker, and four female layers out of the dead. The death industry as we know it today had been born.
Where do you see yourself in five years? Ten? Twenty? It’s not an unusual question to hear, though answering it is never easy.
But what if you knew you weren’t going to live that long? What if you knew your death was coming in a matter of months — or even sooner?
End-of-life care is, generally speaking, the care that someone receives after being diagnosed with a terminal illness, such as cancer or Alzheimer’s disease. While some diseases may be treatable and even curable, terminal diseases are typically those for which there are no cures, and decisions regarding end-of-life care prioritize making the most of an individual’s time left.
Max Vergo, a palliative care doctor and assistant professor at the Geisel School of Medicine, explained that end-of-life care is highly individualized, and not all treatments are appropriate for a patient’s wishes. For example, some patients prioritize extending their lifespans as much as possible, perhaps to be able to attend a special event like someone’s graduation. But opting to live longer might come at the cost of a lesser quality of life, such as being bound to a hospital bed.
Other patients, however, would rather prioritize different treatments that would allow them to maintain a certain quality of life — say, being able to walk freely or live at home — even if that means their death may arrive sooner.
“For some people, [prioritizing living longer] feels like the quality would be so poor, it wouldn’t really be valuable time,” Vergo said. “Knowing that their time is limited anyway, they may choose a [different] path. … At least they’ll have some control over what the quality [of life] looks like.”
End-of-life decisions, while incredibly individual, often involve an entire of team of medical professionals. Kathryn Kirkland, the director of palliative care at Dartmouth-Hitchcock Medical Center and a professor at Geisel, spoke about how her patients interact with an interdisciplinary team of doctors and nurses, social workers, chaplains, creative writing specialists, artists and other volunteers, all of whom work to take care of “the whole person.”
Kirkland also explained how her team works with patients’ families and loved ones as well. For example, patients with terminal issues often experience feeling like a burden to their families. In those cases, patients and their families go through counseling to discuss those feelings and identify ways to alleviate them.
“Taking care of somebody who is very sick is a hard thing to do sometimes,” Kirkland said. “Most family members end up reassuring the person with [the] illness that they want to help, that the patient is not being a burden, but unless you have those conversations, it can be hard to influence people’s decision making.”
Among the many options that patients sometimes have, one of the most controversial is physician-assisted dying, also known as physician-assisted suicide. Ann Bumpus, who taught the course Philosophy 5, “Philosophy and Medicine” last fall, explained how physician-assisted suicide is different from euthanasia because patients take a drug that they know will cause their deaths, whereas euthanasia is when a physician administers the drug, usually via an injection.
Euthanasia is illegal in all 50 states, but physician-assisted suicide is legal in a handful of states. It became legal for Vermont residents in 2013 with Act 39, the Vermont Patient Choice and Control at the End of Life Act; physician-assisted suicide is still illegal in New Hampshire.
Cristine Maloney is the hospice medical director for Visiting Nurse and Hospice for Vermont and New Hampshire, meaning that she sees patients in both states. She noted that, given the difference between the law between Vermont and New Hampshire, she’s always cognizant of which side of the border she’s on when working with patients.
Maloney noted that when discussing the option with patients in Vermont, she tried to understand why they are considering it in the first place. Many patients are unfamiliar with the process, which requires two different physicians — one consulting and one prescribing — and a waiting period of at least two and a half weeks. Another misconception is that patients receive a shot or intravenons treatment to end their life, when in reality, it’s a powder that dissolves in water that patients must be able to take by themselves.
When asked about the emotional aspect of physician-assisted dying, Maloney said that many of her discussions with patients revolve around their desire to have control over this aspect of their life, as well as the expected nervousness about what dying is like. She noted that family members, and even the doctors who prescribe the medicine, often feel intense emotions too.
“After a patient takes medication like this, they die, but their caregivers or family members live with that experience, and so they often have also had some strong opinions … or feel nervous or concerned about it as a family member,” Maloney said. “I think the same is true for the [physicians]. Most of them are doing this for the first time, and it’s very different than anything a physician usually does. We’re usually doing the opposite, giving folks medications to not end their lives.”
How does physician-assisted dying enter into the broader topic of suicide as a whole? The name of the process itself is controversial. While the terms “physician-assisted dying” and “physician-assisted suicide” seem interchangeable in everyday discourse, Vergo expressed a strong preference toward the former.
“In our profession, [we don’t use] ‘suicide’ because these are rational decisions that people make,” Vergo said.
Bumpus spoke about how some of the arguments against physician-assisted dying include the possibility that it leads to a rise in suicide rates in young people and terminally ill people, acknowledging that there is not yet good evidence to prove or disprove the concern. She also touched upon the use of the word “suicide” instead of “dying.”
“Calling it suicide emphasizes the similarity, and the similarity is just that, technically, the person takes their own life,” Bumpus said. “I think using the word suicide for both overstates the similarities. I’m not saying that suicide is always irrational or always wrong, but I think these cases are really special end-of-life cases and ought to be looked at separately.”
Another compelling concern with physician-assisted suicide that Bumpus brought up was that vulnerable populations, including individuals without good health insurance or a strong understanding of the medical system, may be pressured — however subtly — to choose physician-assisted dying without exploring other options as much as they would have otherwise. While we, as a society, often believe that more options leads to more freedom, that’s not always the case, and offering physician-assisted suicide could end with patients feeling obligated to take it.
So, what can students do? For students who are interested in the medical field and may one day have end-of-life care conversations with patients and families, Vergo spoke about how much of his teaching work involves perspective training. It’s essential for physicians to understand how, given the same information, different people can have different perspectives, and none of them are wrong. He also acknowledged that having these conversations can be emotionally taxing for health care professionals as well, and a tried-and-true “scaffold” to fall back on during these conversations can help.
Vergo emphasized that no one is born having mastered these skills, but instead they are gained gradually with practice and training.
“It’s just like in sports,” Vergo said. “You don’t just become an awesome soccer player on your own. You usually have a team and then a coach that helps you figure out how you can take the next step in your skills. We do a lot of coaching.”
For students who aren’t necessarily interested in the medical field, these topics can still be important to think about, especially since many patients in end-of-life care couldn’t have anticipated their current situations. Kirkland, who has taken care of students who have gotten into car crashes or skiing accidents, has even seen friends enter positions where they had to make important decisions. While these topics aren’t always easy to talk about, having conversations early about what you value most in life is a valuable investment.
“Even though students don’t really want to think about how they’re mortal like everyone else, it is probably worthwhile to think about who you would want making decisions for you if you couldn’t make them for yourself,” Kirkland said. “Having conversations with families is important to do.”
Under current law, people who have made every life decision based on their personal values and faith suddenly become, due to a terminal illness, a victim of someone else’s theology.
By Harlan Limpert
My Uncle Don died in his mid-60s after a two-year struggle with cancer. He was one of my favorites, an adult with whom I could discuss topics I couldn’t even mention to my parents. As a kid I’d often ride my bike to his home in Richfield with assurance of getting some cookies, Rice Krispies bars or a similarly unhealthful snack.
So when in college I learned he had lung cancer, I was heartbroken. Like so many cancer patients, he “fought the good fight” — chemo, surgery, radiation. Despite all the treatments, the disease was winning.
One day, after returning from one of countless doctor appointments, he walked into his bedroom, pulled out a gun and shot himself. My aunt, hearing the shot from the kitchen, lived another 20 years with that horrendous memory.
My uncle accepted some comfort care but would not succumb to the cancer robbing him of his humanity. He wanted to die as he had lived, on his own terms. But at that time, medical aid in dying (MAID) wasn’t legal. I have no doubt that, after realizing the futility of further treatment, Uncle Don would have taken advantage of MAID, which enables a mentally competent adult suffering from a terminal illness to request from their physician medication that will end life peacefully. Medical aid in dying has been legal in Oregon for 20 years since that state’s’ passage of its Death with Dignity law and is now legal in seven more states, including California.
Many of us know of someone suffering from a terminal illness. Most often they are willing to fight like hell for as long as possible but in the end pray for a gentle, painless death.
For decades, Gallup Polls have shown that a majority of Americans support medical aid in dying as an end-of-life option. Twenty state legislatures, including Minnesota’s, have introduced bills similar to Oregon’s Death with Dignity law. But, despite widespread support, lawmakers are reluctant to act. Why? Despite the overwhelming support of people of faith, some religious leaders are fighting it, insisting that Americans die by what they call a “natural death.” Suffering, they argue, is redemptive (“to change for the better”). Even the loved ones surrounding the dying person, it is believed, are changed — redeemed — by the experience.
Other people of faith — me included — see nothing redemptive about needless suffering. In fact, needless suffering is cruel and pointless. The proper religious response to suffering is to alleviate it, to show compassion to the one who is suffering. And there is nothing “natural” about being connected to numerous tubes injecting futile drugs into a dying person’s veins when that person would prefer her suffering to end. There is nothing natural about a respirator providing oxygen to a person whose clear intention was to have a good death, one surrounded by loved ones and absent of unnecessary suffering.
National Religious Freedom Day was Jan. 16. For at least 25 years, U.S. presidents have issued annual proclamations acknowledging and celebrating the many faiths that exist within our country. They have reminded us of our cherished legacy of religious liberty. They recall how Thomas Jefferson penned the Virginia Statute of Religious Freedom in 1786, which inspired the words of the First Amendment to the Constitution guaranteeing the free exercise of religion.
But when it comes to end-of-life care, an individual’s personal religious freedom is limited by current law. People who have made every life decision for decades based on their personal values and faith suddenly become, due to a terminal illness, a victim of someone else’s theology. The arena of life that is most personal and profound often has people with different religious values determine our options. At end of life, one’s personal values and spiritual beliefs ought to take priority over everything else.
Passing legislation to allow medical aid in dying in Minnesota will enable end-of-life options to be decided by an individual’s values and spiritual beliefs and no one else. Those who choose medical aid in dying can do so. Those who do not would not be affected.
As National Religious Freedom Day is celebrated, let us remember to honor religious freedom and show compassion to those wishing to end their suffering.
In 2016, a small group of doctors gathered in a Seattle conference room to find a better way to help people die. They included physicians at the forefront of medical aid in dying—the practice of providing terminal patients with a way to end their own life. And they were there because the aid-in-dying movement had recently run into a problem. The two lethal medications used by most patients for decades had suddenly become either unavailable or prohibitively expensive. When doctors briefly tried a substitute, some patients had rare but troubling experiences.
The Seattle group hoped to discover a different drug. But the practicalities of aid in dying, a controversial policy still illegal in most of the United States, are not like those in other medical fields. “There’s lots of data on stuff that helps people live longer, but there’s very little data on how to kill people,” says Terry Law, a participant at the meeting and one of the most frequently used aid-in-dying doctors in the U.S.
Seven states—including Hawaii, where a law took effect on January 1—and the District of Columbia now allow doctors to write lethal prescriptions for qualifying, mentally capable adults who have a terminal illness. And support for the practice has gained new national momentum after the widely publicized death of Brittany Maynard, a young cancer patient who moved to Oregon in 2014 to take advantage of that state’s aid-in-dying law.
But the public remains deeply conflicted about the laws—as does the medical community itself. No medical association oversees aid in dying, and no government committee helps fund the research. In states where the practice is legal, state governments provide guidance about which patients qualify, but say nothing about which drugs to prescribe. “Nowhere in the laws is there any sort of guidance for how to do it. There is no oversight to make sure that it’s happening in a safe way, apart from annual reports and kind of a face-value annual hearing,” says Laura Petrillo, a palliative-care physician who opposes legalized aid in dying.
The meeting of the 2016 group set in motion research that would lead the recipe for one of the most widely used aid-in-dying drugs in the United States. But the doctors’ work has taken place on the margins of traditional science. Despite their principled intentions, it’s a part of medicine that’s still practiced in the shadows.
On the surface, figuring out protocols for hastening death doesn’t seem complicated. Lonny Shavelson, a California physician who specializes in aid in dying, says that when he explains to patients it might take an hour or more for them to die, they’re often shocked. They tell him, “When I put down my dog, it took 10 minutes,” he says.
But veterinarians can use lethal injections on pets. In the U.S., aid-in-dying drugs must be ingested by the patient. The first proposed aid-in-dying law in Washington State would have allowed physicians to inject medications, but that legislation failed to pass. In 2008, a modified law was voted in, with an added requirement that patients self-ingest to help protect them from the possibility of family coercion.
For years, the two barbiturates widely considered the best drugs for hastening death in terminally ill patients were secobarbital and pentobarbital. These medications were painless, fast-acting, and relatively affordable. But since 2015, they’ve been largely unavailable. U.S. pharmacies stopped carrying pentobarbital approved for human use, and the price of secobarbital doubled from an already historic high after Valeant Pharmaceuticals (today known as Bausch Health) bought the manufacturing rights. A few years ago, a lethal dose cost about $200 or $300; now it can cost $3,500 or more.
To help patients who could no longer afford the drug, aid-in-dying groups sought a fix. In Washington, an advocacy organization called End of Life Washington briefly advised prescribing a drug mixture with the sedative chloral hydrate to about 70 patients. “We know this is going to put you to sleep, and we’re pretty sure it’s going to kill you,” Robert Wood, a medical director at the organization, says they told the patients. It worked, but with a tragic catch: In a few cases, the chloral hydrate burned people’s throats, causing severe pain just at the time they expected relief.
The End of Life gathering was born out of the need for a better solution. Wood enlisted three others affiliated with End of Life Washington: Law, its president; Tom Preston, a former medical director; and Carol Parrot, a retired anesthesiologist who, like Law, is one of the most experienced aid-in-dying doctors in the U.S. Others joined that meeting or later ones by telephone: a toxicologist in Iowa, a veterinarian, a pharmacologist, another anesthesiologist. The group had three main criteria, Parrot says: They wanted “a drug that would: number one, put a patient to sleep and keep them asleep; and, number two, make sure there was no pain involved; and number three, ensure that they would die, and, hopefully, die relatively quickly.” Plus, it had to be cheap. They aimed for $500 a dose.
The doctors considered a malaria medicine known to be lethal in large doses, but read that it caused severe muscle spasms in some patients. They discussed the synthetic opioid fentanyl, but were deterred by the drug’s newness and dangerous reputation. So the group decided to use a combination of medications, and eventually settled on high doses of three: morphine, diazepam—also known by its early brand name, Valium—and propranolol, a beta-blocker that slows the heart. They called the mixture DMP.
Next, the group had to test the drug. But they still didn’t have a way to follow standard procedure: There would be no government-approved clinical drug trial, and no Institutional Review Board oversight when they prescribed the concoction to patients. The doctors took what precautions they could. Patients could opt in or out, and for the first 10 deaths, either Parrot or Law would stay by the bedside and record patients’ and families’ responses.
The first two deaths went smoothly. But the third patient, an 81-year-old with prostate cancer, took 18 hours to die, Parrot says. In Oregon, where aid in dying has been legal for 20 years, the median time from taking the medication until death is 25 minutes. Patients themselves typically become unconscious in five or 10 minutes, so they are not affected by protracted times, Parrot, Wood, and Law all emphasize. But longer waiting periods can be nerve-racking for families and other caregivers, especially in the exceptional cases where these have persisted for a day or more.
Parrot and Law halted the DMP trial. The informal research group met again, this time by teleconference, and Law dug through the literature and found an article about people who purposely overdosed on digoxin, a cardiac drug. The group added it to the prescription, and the drug became DDMP.
At first, Parrot gave patients latitude in how they took this new drug combination. “One guy chugged a half a cup of Bailey’s Irish Cream, his favorite thing, after he had his medicine,” she says. “He probably took five or six hours to die.” She suspects that the fat particles in the Bailey’s slowed his gastric emptying. So the researchers checked in with each other again, and decided to increase the doses to what Parrot calls “blue-whale-sized doses.” They dubbed the modified formula DDMP2.
The drug is not a perfect aid-in-dying solution. Secobarbital is faster-acting and remains the drug of choice when patients can afford it, Wood says. Just as in the case of the barbiturates, a few outlier patients on DDMP2 take hours longer to die. And the mixture tastes extremely bitter. “Imagine taking two bottles of aspirin, crushing it up, and mixing it in less than half a cup of water or juice,” Parrot says.
Still, DDMP2 has become the low-cost solution the Seattle group set out to discover. In 2017, secobarbital was still the most commonly prescribed drug in Washington and Oregon, but in Colorado, DDMP2 was more commonly prescribed. The drug consistently accomplishes its purpose in hastening death, Parrot says: “It always works. It always, always works.”
Parrot and Wood keep track of patient data, and they continue to make discoveries. By examining medical histories of the patients who took longer to die, they’ve learned about certain risk factors for longer deaths: being on extremely high doses of painkillers such as fentanyl or morphine; being very athletic; having a compromised digestive tract. For patients who are especially risky, Parrot or Wood will sometimes offer the choice of chloral hydrate, the drug that burned some patients’ throats, although they say they carefully discuss potential problems with patients and families.
Together, Parrot and Law have written perhaps 300 lethal prescriptions over the years and observed the effects of medications on numerous patients. Neither set out to be an aid-in-dying advocate; they turned to End of Life Washington after witnessing the suffering of some dying patients. About eight years ago, Law says she was asked to prescribe lethal medications for a dying woman whose regular doctors had refused. She agreed to see the woman, and realized how difficult it was for some aid-in-dying patients to find doctors. Parrot says she was profoundly affected by the deaths of two close friends who asked her to help hasten their dying, but who lived in states where the practice was illegal. She was unable to help them, and began volunteering as an aid-in-dying doctor soon after she retired.
Most medical professionals don’t participate in aid in dying. Some physicians are concerned that their Hippocratic oath prohibits intentionally helping someone die, or that aid-in-dying requests originate from treatable pain or depression. Some worry about the broader repercussions for a society that accepts medically aiding the deaths of the terminally ill. The American Medical Association remains officially opposed.
Without the support of the rest of the profession and much of society, aid-in-dying research methods don’t fit the model of good medical research, says Matthew Wynia, the director of the Center for Bioethics and Humanities at the University of Colorado. There’s no standard protocol, no standardized data collection or independent group that monitors data and safety—all of which are intended to protect patients and help ensure the quality of the research.
The Belmont Report, which guides federal recommendations for research on human subjects, recognizes that sometimes, no satisfactory options exist for some patients, Wynia points out. In those rare cases, a doctor may want to try an innovative treatment, something for which there’s no approved research protocol. While that’s legal, clinicians are supposed to avoid turning that innovation into established practice, or doing unapproved research on numerous patients, according to Wynia. Some of the same issues exist with medical marijuana, which is legal in several states but still illegal federally. “There’s no way to fix this at the individual level,” Wynia says. “There’s no immediate answer.”
That leaves researchers like Law and Parrot in a bind. They don’t have good ways to do research and communicate what they learn. But they’ve witnessed the suffering some dying people experience, and contrast that with many peaceful deaths of patients who choose aid in dying. “These are not hard deaths,” argues Shavelson, the California physician. “These are lovely deaths.”
Shavelson says he tries to be at the bedside on the day of his aid-in-dying patients’ death. “It’s a lighter atmosphere than you think,” he says. The patient takes the first drug, which Shavelson separates out from the rest of the mixture, and then Shavelson sits down at the bedside and reads aloud questions from the state’s required report. After about 30 minutes, he asks: “Are you ready to take the medications?” He mixes the drug cocktail and the patient drinks it.
“Usually, they go silent after taking the medication,” he says. “They’ve said what they’re going to say by that time.” For a few minutes, patients usually continue to sit silently, their eyes open. “And then, very, very slowly, they’ll close their eyes.”
Shavelson asks intermittently, “Are you still there?” At first, patients usually say yes, or nod. Within five or 10 minutes, they stop responding to the question. Then Shavelson will gently touch their eyelids. “When people aren’t deeply unconscious, they’ll sort of have a twitching response,” he explains. Within 10 or 15 minutes, the twitching response disappears, and patients enter a deep coma.
Using a heart monitor, Shavelson tells caregivers as a patient’s pulse slows and oxygen levels drop. “We wait a little while, and then I say, ‘Ah, the patient’s now dead.’”
This is the first generation of patients who have consciously hastened their death with medications in this way, Shavelson says. He tells them they’re pioneers. “What a different thing, to be able to say, ‘This is the day I die,’” he says.
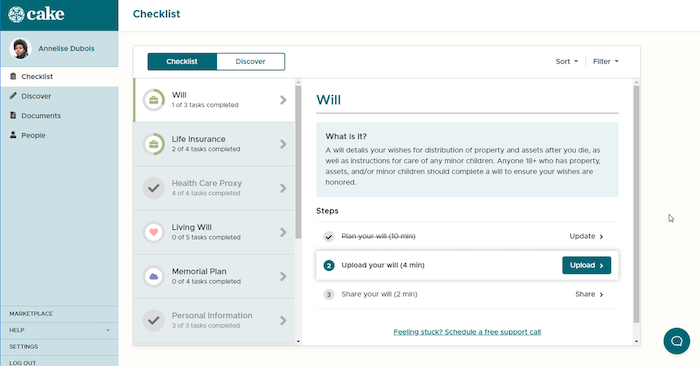
These days, your last will and testament needs to cover more than just who gets your money and random tchotchkes. Cake takes a no-nonsense and pleasant approach to planning your inevitable demise; no gloom and doom here. Founder Suelin Chen explains.
A few years ago, ahead of a scheduled operation, I had to hire an attorney to draw up my last will and testament. Per the hospital’s instructions, I was also told to bring a copy of my Advance Directive, or instructions on when to pull the plug. It was scary, grown-up stuff.
As a digital native, it all felt a bit too real. I would have much preferred to sit on my couch, laptop at the ready, with an on-screen AI to talk me through the whole decision-making process and pop it up on the cloud. And that’s exactly what former healthcare executive Suelin Chen built in her Boston-based startup, Cake.
Aware that no one is thrilled about planning for the final exit—or having to talk loved ones through their own wishes—Cake is a no-nonsense online tool. You can lay out: how you’d like to go (hospice versus at home or maybe a remote cabin in the woods); who gets your stuff; the music you’d like at your memorial; and more.
You can also specify how you want to be remembered digitally. Perhaps you want to allocate funds for annual site management fees, domain registration, or deputizing someone to ensure a Wiki-profile is factually accurate.
I spoke to Chen to find out more. Here are edited and condensed excerpts from our conversation.
Suelin, how did you come up for the idea behind Cake?
With my background in healthcare and business, I saw not only the high costs involved in end-of-life care, but that in our country people often default to enduring more and more medical procedures without fully understanding the value, or the trade-offs. Three out of four people don’t plan for end-of-life, and I get why—the barriers to planning can be really high. Simply put, I saw an opportunity to help people plan better, to make their desires known, before it’s too late.
Because they’re too incapacitated to make their views known?
Right, it’s often brought up too late. Because, when surveyed, 80 percent of people would prefer to die at home—and yet, today, 80 percent of people die in medical facilities.
Planning for the final exit is a space ripe for disruption, then.
I knew there could be good digital tools for doing this but I couldn’t find any, so I found a great team and built Cake.
Is there also a generational shift? Due to social media, we get to ‘see’ people die, many of whom we might have lost touch with over the years. Death is going to happen to us all. But it feels more ‘visible’ now.
Absolutely. We have a lot of millennials on our platform, and we see that this generation is very pragmatic and perceives less stigma about death than older generations. Previous generations have been remembered through a gravestone or something similar. In time, those degrade. But our digital footprint, the traces of our lives, will persist online. I ask people, when your great-grandchildren search online for you in the future, what do you want them to find?
That’s a deeply unsettling and yet curiously interesting thought. You must have worked with many different partners to bring Cake to life.
Yes, we’ve spent hundreds of hours consulting with experts to develop all our online tools including: estate attorneys, funeral planners, physicians, social workers, and wealth managers.
How does Cake work? This is more than a basic will, right?
Yes, many of our users have done estate planning and have a will but realize that they still have gaps. We provide a personalized, comprehensive, and detailed checklist that helps people understand what planning they still need to do. It’s hard to know what legal fees are reasonable, because there’s a lack of transparency. Many of our users have seen an attorney but want more visibility into the process. It’s not just avoiding taxes on your assets after death (though of course this is very important). It’s also managing how you want to be remembered, your funeral or memorial service, your digital footprint, your digital assets (Bitcoin, etc.)—certainly doing more than putting all your passwords in an Excel doc and locking it (which has been recommended to several of our users).
How many data points is your AI gathering as it takes a Cake user through personal planning?
It’s fluid [and] really depends on the individual. Our Cake AI prompts you with questions, to capture data around many decisions that need to be made. But there’s also a freeform section for more personal wishes. Some of our users write (almost) novel-length answers to those.
What are some of the more ‘out there’ requests?
Well, every employee at Cake has gone through the process and one of my team members loves the idea of having a tree planted for him. A lot of our users, including me, feel they’d rather have a celebration of life than a somber funeral. One of our users wants to be buried with a 6-pack of Bud Lite. Someone else I know has left instructions to rent out a movie theater for his. Your last wishes should be a true expression of who you are.
How many people have signed up so far?
We don’t reveal exact user numbers.
Fair enough. It’s free to users, so what’s your revenue model?
We make money from affiliate links and from enterprise partners who distribute to their population. For example, we’ve built a Cake back-end for a large healthcare provider, an insurer, a bank, and other institutions. A premium product is also in the works.
You don’t share data with ‘interested parties’ who might want to sell fancy urns then?
No, trust is the most important thing to us. We will never sell or share personally identifiable information with any third party without our users consent.
Why the name Cake?
It’s a warm, inviting symbol of celebrating and honoring life. Planning is a positive act, a true gift to your loved ones.
You’ve build a web-based service, rather than a mobile app. Why?
It’s much faster to iterate and improve the platform, and doesn’t require any download. We also know that many of our user base is more comfortable with web apps than downloading native applications.
Do you have a tech team in-house or are you partnering with a digital agency on this build?
All in house! We actually have more female than male techies, who span several generations, which I’m very proud of.
Are you wedded to any particular tech tools?
Choosing Microsoft Azure as our hosting platform made it easy for us to implement excellent security and scalability for our product early on, and our code base heavily utilizes the Microsoft .NET stack as well. We recently also switched our internal IT to Office 365 and were early adopters of Microsoft Teams; so I guess we’re fans of Microsoft technologies.
Why are you based in Boston rather than any of the other Silicon cities?
I love Boston. There’s a lot of activity in FinTech, MedTech, and healthcare here. It’s a great place to be, with plenty of talent and financial support from big institutions.
Finally, what’s next for you?
We have an exciting growth plan for 2019, and a number of new partners in the financial sector that will provide new avenues for growth and new opportunities to add features that enable our users to plan and have peace of mind. Cake is in the FinTech cohort of Mass Challenge 2019, which kicks off orientation on Jan. 18. The initiative is aimed at startups which have an enterprise-ready solution, and helps them partner with large organizations. Cake will be working with MassMutual, Fidelity, and AARP Innovation Labs.
Mort Felix liked to say that his name, when read as two Latin words, meant “happy death.” When he was sick with the flu, he used to jokingly remind his wife, Susan, that he wanted Beethoven’s “Ode to Joy” played at his deathbed. But when his life’s end arrived at the age of 77, he lay in his study in his Berkeley, California, home, his body besieged by cancer and his consciousness cradled in morphine, uninterested in music and refusing food as he dwindled away over three weeks in 2012. “Enough,” he told Susan. “Thank you, and I love you, and enough.” When she came downstairs the next morning, she found Felix dead.
During those three weeks, Felix had talked. He was a clinical psychologist who had also spent a lifetime writing poetry, and though his end-of-life speech often didn’t make sense, it seemed to draw from his attention to language. “There’s so much so in sorrow,” he said at one point. “Let me down from here,” he said at another. “I’ve lost my modality.” To the surprise of his family members, the lifelong atheist also began hallucinating angels and complaining about the crowded room—even though no one was there.
Felix’s 53-year-old daughter, Lisa Smartt, kept track of his utterances, writing them down as she sat at his bedside in those final days. Smartt majored in linguistics at UC Berkeley in the 1980s and built a career teaching adults to read and write. Transcribing Felix’s ramblings was a sort of coping mechanism for her, she says. Something of a poet herself (as a child, she sold poems, three for a penny, like other children sold lemonade), she appreciated his unmoored syntax and surreal imagery. Smartt also wondered whether her notes had any scientific value, and eventually she wrote a book, Words on the Threshold, published in early 2017, about the linguistic patterns in 2,000 utterances from 181 dying people, including her father.
Despite the limitations of this book, it’s unique—it’s the only published work I could find when I tried to satisfy my curiosity about how people really talk when they die. I knew about collections of “last words,” eloquent and enunciated, but these can’t literally show the linguistic abilities of dying people. It turns out that vanishingly few have ever examined these actual linguistic patterns, and to find any sort of rigor, one has to go back to 1921, to the work of the American anthropologist Arthur MacDonald.To assess people’s “mental condition just before death,” MacDonald mined last-word anthologies, the only linguistic corpus then available, dividing people into 10 occupational categories (statesmen, philosophers, poets, etc.) and coding their last words as sarcastic, jocose, contented, and so forth. MacDonald found that military men had the “relatively highest number of requests, directions, or admonitions,” while philosophers (who included mathematicians and educators) had the most “questions, answers, and exclamations.” The religious and royalty used the most words to express contentment or discontentment, while the artists and scientists used the fewest.
MacDonald’s work “seems to be the only attempt to evaluate last words by quantifying them, and the results are curious,” wrote the German scholar Karl Guthke in his book Last Words, on Western culture’s long fascination with them. Mainly, MacDonald’s work shows that we need better data about verbal and nonverbal abilities at the end of life. One point that Guthke makes repeatedly is that last words, as anthologized in multiple languages since the 17th century, are artifacts of an era’s concerns and fascinations about death, not “historical facts of documentary status.” They can tell us little about a dying person’s actual ability to communicate.
Some contemporary approaches move beyond the oratorical monologues of yore and focus on emotions and relationships. Books such as Final Gifts, published in 1992 by the hospice nurses Maggie Callanan and Patricia Kelley, and Final Conversations, published in 2007 by Maureen Keeley, a Texas State University communications-studies scholar, and Julie Yingling, professor emerita at Humboldt State University, aim to sharpen the skills of the living for having important, meaningful conversations with dying people. Previous centuries’ focus on last words has ceded space to the contemporary focus on last conversations and even nonverbal interactions. “As the person gets weaker and sleepier, communication with others often becomes more subtle,” Callanan and Kelley write. “Even when people are too weak to speak, or have lost consciousness, they can hear; hearing is the last sense to fade.”
I spoke to Maureen Keeley shortly after the death of George H. W. Bush, whose last words (“I love you, too,” he reportedly told his son, George W. Bush) were widely reported in the media, but she said they should properly be seen in the context of a conversation (“I love you,” the son had said first) as well as all the prior conversations with family members leading up to that point.
At the end of life, Keeley says, the majority of interactions will be nonverbal as the body shuts down and the person lacks the physical strength, and often even the lung capacity, for long utterances. “People will whisper, and they’ll be brief, single words—that’s all they have energy for,” Keeley said. Medications limit communication. So does dry mouth and lack of dentures. She also noted that family members often take advantage of a patient’s comatose state to speak their piece, when the dying person cannot interrupt or object.
Many people die in such silence, particularly if they have advanced dementia or Alzheimer’s that robbed them of language years earlier. For those who do speak, it seems their vernacular is often banal. From a doctor I heard that people often say, “Oh fuck, oh fuck.” Often it’s the names of wives, husbands, children. “A nurse from the hospice told me that the last words of dying men often resembled each other,” wrote Hajo Schumacher in a September essay in Der Spiegel. “Almost everyone is calling for ‘Mommy’ or ‘Mama’ with the last breath.”
It’s still the interactions that fascinate me, partly because their subtle interpersonal textures are lost when they’re written down. A linguist friend of mine, sitting with his dying grandmother, spoke her name. Her eyes opened, she looked at him, and died. What that plain description omits is how he paused when he described the sequence to me, and how his eyes quivered.
But there are no descriptions of the basics of last words or last interactions in the scientific literature. The most linguistic detail exists about delirium, which involves a loss of consciousness, the inability to find words, restlessness, and a withdrawal from social interaction. Delirium strikes people of all ages after surgery and is also common at the end of life, a frequent sign of dehydration and over-sedation. Delirium is so frequent then, wrote the New Zealand psychiatrist Sandy McLeod, that “it may even be regarded as exceptional for patients to remain mentally clear throughout the final stages of malignant illness.” About half of people who recover from postoperative delirium recall the disorienting, fearful experience. In a Swedish study, one patient recalled that “I certainly was somewhat tired after the operation and everything … and I did not know where I was. I thought it became like misty, in some way … the outlines were sort of fuzzy.” How many people are in a similar state as they approach death? We can only guess.
We have a rich picture of the beginnings of language, thanks to decades of scientific research with children, infants, and even babies in the womb. But if you wanted to know how language ends in dying people, there’s next to nothing to look up, only firsthand knowledge gained painfully.
Lisa Smartt at her father, Mort Felix’s bedside
After her father died, Lisa Smartt was left with endless questions about what she had heard him say, and she approached graduate schools, proposing to study last words academically. After being rebuffed, she began interviewing family members and medical staff on her own. That led her to collaborate with Raymond Moody Jr., the Virginia-born psychiatrist best known for his work on “near-death experiences” in a 1975 best-selling book, Life After Life. He has long been interested in what he calls “peri-mortal nonsense” and helped Smartt with the work that became Words on the Threshold, based on her father’s utterances as well as ones she’d collected via a website she called the Final Words Project.
One common pattern she noted was that when her father, Felix, used pronouns such as it and this, they didn’t clearly refer to anything. One time he said, “I want to pull these down to earth somehow … I really don’t know … no more earth binding.” What did these refer to? His sense of his body in space seemed to be shifting. “I got to go down there. I have to go down,” he said, even though there was nothing below him.
He also repeated words and phrases, often ones that made no sense. “The green dimension! The green dimension!” (Repetition is common in the speech of people with dementia and also those who are delirious.) Smartt found that repetitions often expressed themes such as gratitude and resistance to death. But there were also unexpected motifs, such as circles, numbers, and motion. “I’ve got to get off, get off! Off of this life,” Felix had said.
Smartt says she’s been most surprised by narratives in people’s speech that seem to unfold, piecemeal, over days. Early on, one man talked about a train stuck at a station, then days later referred to the repaired train, and then weeks later to how the train was moving northward.
“If you just walk through the room and you heard your loved one talk about ‘Oh, there’s a boxing champion standing by my bed,’ that just sounds like some kind of hallucination,” Smartt says. “But if you see over time that that person has been talking about the boxing champion and having him wearing that, or doing this, you think, Wow, there’s this narrative going on.” She imagines that tracking these story lines could be clinically useful, particularly as the stories moved toward resolution, which might reflect a person’s sense of the impending end.
In Final Gifts, the hospice nurses Callanan and Kelley note that “the dying often use the metaphor of travel to alert those around them that it is time for them to die.” They quote a 17-year-old, dying of cancer, distraught because she can’t find the map. “If I could find the map, I could go home! Where’s the map? I want to go home!” Smartt noted such journey metaphors as well, though she writes that dying people seem to get more metaphorical in general. (However, people with dementia and Alzheimer’s have difficulty understanding figurative language, and anthropologists who study dying in other cultures told me that journey metaphors aren’t prevalent everywhere.)
Even basic descriptions of language at the end of life would not only advance linguistic understanding but also provide a host of benefits to those who work with dying people, and dying people themselves. Experts told me that a more detailed road map of changes could help counter people’s fear of death and provide them with some sense of control. It could also offer insight into how to communicate better with dying people. Differences in cultural metaphors could be included in training for hospice nurses who may not share the same cultural frame as their patients.
End-of-life communication will only become more relevant as life lengthens and deaths happen more frequently in institutions. Most people in developed countries won’t die as quickly and abruptly as their ancestors did. Thanks to medical advances and preventive care, a majority of people will likely die from either some sort of cancer, some sort of organ disease (foremost being cardiovascular disease), or simply advanced age. Those deaths will often be long and slow, and will likely take place in hospitals, hospices, or nursing homes overseen by teams of medical experts. And people can participate in decisions about their care only while they are able to communicate. More knowledge about how language ends and how dying people communicate would give patients more agency for a longer period of time.
But studying language and interaction at the end of life remains a challenge, because of cultural taboos about death and ethical concerns about having scientists at a dying person’s bedside. Experts also pointed out to me that each death is unique, which presents a variability that science has difficulty grappling with.
And in the health-care realm, the priorities are defined by doctors. “I think that work that is more squarely focused on describing communication patterns and behaviors is much harder to get funded because agencies like NCI prioritize research that directly reduces suffering from cancer, such as interventions to improve palliative-care communication,” says Wen-ying Sylvia Chou, a program director in the Behavioral Research Program at the National Cancer Institute of the National Institutes of Health, who oversees funding on patient-doctor communication at the end of life.
Despite the faults of Smartt’s book (it doesn’t control for things such as medication, for one thing, and it’s colored by an interest in the afterlife), it takes a big step toward building a corpus of data and looking for patterns. This is the same first step that child-language studies took in its early days. That field didn’t take off until natural historians of the 19th century, most notably Charles Darwin, began writing down things their children said and did. (In 1877, Darwin published a biographical sketch about his son, William, noting his first word: mum.) Such “diary studies,” as they were called, eventually led to a more systematic approach, and early child-language research has itself moved away from solely studying first words.
“Famous last words” are the cornerstone of a romantic vision of death—one that falsely promises a final burst of lucidity and meaning before a person passes. “The process of dying is still very profound, but it’s a very different kind of profoundness,” says Bob Parker, the chief compliance officer of the home health agency Intrepid USA. “Last words—it doesn’t happen like the movies. That’s not how patients die.” We are beginning to understand that final interactions, if they happen at all, will look and sound very different.
Nursing requires hands-on training. But research has found that university curriculum often goes light on one of life’s universal experiences — dying. So some colleges have gone to new lengths to make the training more meaningful.
There’s a sound near the end — the death rattle. People stop swallowing. The lungs fill up. There can be involuntary moaning.
“So you get all that noise. And that’s really distressing for family members,” Professor Sara Camp of Nashville’s Belmont University says.
Camp and other nursing instructors at Belmont wear headsets and watch video monitors in a dark closet. The sounds they make emerge from realistic robots lying in hospital beds on the other side of the wall. The instructors also control the stats for the robots’ breathing, pulse and blood pressure.
Other than administering morphine, there’s no exact prescription for students to follow. A review of nursing textbooks found many make no mention of this standard part of the job. And studies of professional nurses find that many feel unprepared.
Belmont adjunct nursing instructor Morgan Bryant mimics the “death rattle” in her headset, also controlling the pulse, breathing and blood pressure of the simulated patients in the lab.
“They’re really comfortable in their skills, like putting in IVs and giving medications,” Camps says. “In this one, they have to focus on communication, when there’s not that much to do. It challenges them.”
There are family dynamics to navigate, like explaining to grown children how their mother signed a do-not-resuscitate order. They have to balance caring for the dying patient and attending to the patient’s family.
In response to surveys showing anxiety about death among young nurses, Belmont started hiring actors to make these end-of-life interactions as realistic as possible.
“That old cancer … didn’t want it to come back,” says Vickie Bailey, who has embraced her role as a grieving daughter.
The student, senior Sara Lindsay, sits on the bedside and puts a hand on Bailey, warning that the end is near.
“Now would be a good time if you have prayers or anything you want to say,” she tells Bailey.
“I’ve been praying all morning,” Bailey responds, in character.
The monitors stop beeping. Everyone sits in silence.
Once the simulation ends, Lindsay marvels at how real the moment felt.
Half a dozen beds are going at the same time in this simulation lab. And all the students gather to debrief afterward. Senior Zacnite Vargas volunteers that she second-guessed herself.
“Should I say she’s dying? She’s dead? She’s passed?” she asks. “I don’t know how to be straight-forward with it.”
Camp tells the class to be cautious, especially about predicting when a patient will die, but also show compassion.
“They may not remember what you say, but they’ll remember how they feel when you were there, because you were there.”
It’s such important work, Camp says, that more students should get the chance to rehearse.