Like taxes, death is still a certainty. But in America, the end of life isn’t what it used to be.
Today, one in five Americans lives in a state that permits medical aid in dying, sometimes simply called assisted dying. The idea is terminally ill individuals who have six months or less to live can apply for a medically assisted death to limit their suffering. And if they meet the criteria, they can have some say when they will take their last breath.
It’s been nearly 25 years since the country’s first assisted death law — Oregon’s Death With Dignity Act — went into effect. And since then, eight other states — Washington, Vermont, California, Colorado, Hawaii, New Jersey, Maine and New Mexico, as well as Washington, D.C., have enacted their own versions. What all jurisdictions with medical aid in dying have in common is the requirement that the patients must be of sound mind, have less than six months to live and they must be able to self-administer the lethal medication, prescribed by a physician, to end their lives.
Eleven other states have introduced medical aid in dying bills during the 2021-22 legislative session. It’s a growing movement that’s largely under the radar, much as death is in this society.
Assisted death is “not the path of least resistance. For many it’s the path of most resistance.”
In the latest survey by Susquehanna Polling & Research, two out of three voters (67%) said if they “had an incurable, terminal illness, still had a sound mind but less than six months to live and met the legal requirements,” they would want the option of medical aid in dying.
As the baby boomers age, medical aid in dying is expected to be an even bigger issue in the years ahead.
Anita Hannig, associate professor of anthropology at Brandeis University in Waltham, Massachusetts, says assisted death is “not the path of least resistance. For many it’s the path of most resistance.”
Indeed, the assisted dying laws in the ten U.S. jurisdictions are among the most restrictive in countries with such laws. That hasn’t stopped opposition from some religious and right-to-life groups, among others.
For her new book, “The Day I Die: The Untold Story of Assisted Dying in America,” Hannig spent hundreds of hours over five years on the frontlines of assisted dying in the Pacific Northwest, including witnessing several deaths among those who availed themselves of the law.
Next Avenue: You’ve taken a very deep dive into assisted dying in America, a world few families have experienced. As a cultural anthropologist, you’ve gone from researching birth and the beginning of life in Ethiopia to the opposite end of the life cycle. Why the shift?
Anita Hannig: I was showing a film called ‘How to Die in Oregon’ in my Medicine and Religion class at Brandeis. It’s such a lovely documentary about the law in Oregon and about all those assisted dying volunteers who go and help people die. And I was immediately hooked and thought, wow, birth and death are like bookends. You have home births and home deaths. And so I was curious to go over to the other side. I was very surprised by what I found.
You must have a unique perspective on birth and death as an anthropologist studying assisted dying and as a new mother who also lost a child during an earlier pregnancy.
Definitely. We’re so used to thinking about birth and death as opposites when they’re actually very similar. One of the main figures in my book, a former nurse and longtime assisted dying volunteer in Oregon, Derianna Mooney, taught me that birth and death are both sacred transitions — from one state of being to another, from nonbeing into being and being into nonbeing. And culturally we revere one, but we shun the other.
“I think part of the issue is that we have all the technology now, but our ethical and moral compass hasn’t really caught up with how we should use it.”
As a new mother, I can see people’s eyes light up when they watch us stroll by with our oversized pram. There’s so much positive attention. And all of this has to do with the fact that we love the beginning. It holds so much promise.
And yet we’re so afraid of the end. Similar to a birth, people do need help at the end of life. I love when Derianna says, “You’re going to the gate with them and you are letting them go, but you’re nurturing them through the gate.” What a beautiful vision.
One of the vexing issues surrounding death in our country especially is the role high-tech medicine plays in extending life — even when a longer life doesn’t always promise more quality. Is the assisted dying movement a sign that technology is frequently not making our final years better?
Yes. I think part of the issue is that we have all the technology now, but our ethical and moral compass hasn’t really caught up with how we should use it. And it’s not just in the United States. My 87-year-old grandmother, who passed away in Germany in March, underwent radiation for her breast cancer when she was two weeks away from dying. I’m flabbergasted when I think about why we offer this extremely invasive treatment to somebody who is close to dying. Thankfully, she was soon admitted to a beautiful hospice by a lake to spend what became her final days.
I got interested in this topic when a friend’s husband, suffering from Parkinson’s and no longer able to feed himself, was forced to starve himself to death since he lived in Maryland, a state without a medical aid in dying law. For people consigned to such a horrific death, can a doctor truly say they are following the Hippocratic Oath that tells physicians to do no harm?
That’s exactly the conclusion that a lot of doctors who help patients die come to because in that case doing nothing — such as not helping somebody die — is doing harm. Physicians who are at the forefront of assisted dying say their task is to prevent suffering. And how you prevent suffering in many of these cases is to help somebody die. I always come back to this question: Who is telling these patients that they need to hang on? For what? For whom? Sometimes they themselves are ready to go, but they want to stick around for the family or because there’s a societal expectation to fight.
At the beginning of your book, you almost took my breath away when you were helping one of the volunteers opening the capsules of Seconal and pouring powder into a bowl in one room while the patient, Ken, was waiting in the next room to receive the lethal medication. What were your thoughts as you prepared the medicinal mix that you knew would end a man’s life?
It’s a really good question. Anthropologists have a tool in our toolbox called “participant observation.” And that means you’re never just an impartial observer because your presence alone already changes what’s happening in the room. In order to really relate and put ourselves and the reader into the shoes of these people, you have to bring yourself into the situation wholeheartedly and authentically. And often that means becoming a participant in what is happening.
It’s an extreme privilege to be invited into that kind of intimate space. So, it would have felt very off- putting to just be sitting in the corner taking notes. Everybody in the room is carrying this person over the threshold together. And so you just kind of take your cues from what’s happening.
You don’t want to feel like a voyeur?
Exactly. You want to be in the moment and going through all the emotions other people are going through. It’s a different way of being present that allows you to faithfully experience the death alongside the people whose loved one is dying.
But this must have been a difficult moment for you. In your book, you described “a heavy sense of transgression rise up inside” of you as prepared the lethal medication.
You know what I think it is? It’s the feeling of internalizing some of the stigma that we carry and some of the taboo with which we treat death. And so being part of somebody’s death in this participatory way makes you ask, ‘Am I doing something wrong? Am I, in some bizarre way, enabling that person to die?’
But even if I hadn’t been there, things would have gone probably in a very similar way. I think it’s the cultural baggage that we feel around what it means to hasten the end of your life. Everyone there knew this is what Ken wanted. He chose this with one-hundred percent of his cognitive abilities. His wish was to be delivered from this world and you are enabling that transition.
Among the deaths you researched but didn’t witness was that of Louis, who was an outlier. His experience turned into a nightmare for the person who supervised his assisted death. Louis actually woke up after taking the lethal medication. What happened?
“Everybody in the room is carrying this person over the threshold together.”
Medicine is a human art and as an art, is prone to failure. And it just goes back to the ways the laws are written. They insist on self-administration. But when you are limited that way, you’re going to run into a bunch of problems such as people with gastrointestinal issues who can’t quite absorb the medication. And then you have people who can’t physically self-administer, like a lot of folks with ALS or other illnesses that affect their mobility or their hand range or who can’t drink something on their own or push the syringe on their feeding tube.
And people are getting a little more innovative with things like rectal catheters now, but there’s still a requirement that this has to be an act of volition — you have to be the one to push the plunger on your feeding tube or catheter, what have you. And in almost all other countries, you don’t have that requirement. A doctor can administer if you’re unable to administer yourself.
So after immersing yourself in this world of assisted dying for five years, what‘s your takeaway from this experience?
As a society, we have to make a concerted effort to become less alienated from death and dying. Of course, one could ask how alienated are we when the biggest newspaper in the country, the New York Times, can post images of corpses in Ukraine on its front page? But that doesn’t create closeness or connection. That just creates more fear.
Ideally, I think everybody should have to take a class on death and dying that could cover estates, hospice, and what life-extending procedures there are. In my death and dying class, I talk about people in South Korea who fill an entire gymnasium with coffins and the public comes in and gets inside the coffin to simulate what it would be to die. And they come out of this experience with a totally new zest for life.
This is what contemplating our mortality can do for us. It can take away some of the fear and some of the surprise when a loved one passes away because you will have thought about it in advance. I’m not saying assisted death is the way to go for everyone. We really need to pay more attention to end-of-life issues and prepare for the inevitable and have all of that be less stigmatized.
As the country’s pandemic death toll inches toward one million, has America’s attitude toward death changed at all?
Certainly it’s brought death into the lives of lots of people but not in a way to make them feel more connected to death. Many people weren’t able to see their loved ones in assisted living homes or couldn’t go to the funeral or they weren’t allowed to be present at a nursing home.
When I see the way that we’re tumbling back into life as it was before the pandemic, I don’t know that we’ve really thought critically about death. We just have this big fear-based relationship with death and it’s not lifting the curtain, really. I think people are thrilled to have escaped the pandemic. They see themselves on the other end of that mostly unscathed.
They dodged a bullet?
That’s exactly what it is. But I don’t think it’s made us really contemplate our mortality that much more.
So what will give you a signal that something has shifted in the American attitude toward death?
That people don’t automatically associate the topic of death with fear. And when people begin to realize what I witnessed and write about in the book — some of the empowerment that can come from determining the end of your life and even some of the joy. I hope I’m not out of line to call it joy. When I think of the deaths I witnessed, they weren’t unambiguously sad. There were also serene and heartfelt moments, some laughter and families felt at ease because their loved one wanted to die and they were helping them.
And those who chose to end their lives wanted their death to resonate beyond themselves and their families. Jean, one of the people whose death I witnessed, unbelievably spent the last few minutes of her life promoting her chosen way to die. I still remember her words:
“There are all these baby boomers who will want a better way to die. Our society doesn’t recognize that yet. They will someday.”
After more than a decade of argument, psychiatry’s most powerful body in the United States added a new disorder this week to its diagnostic manual: prolonged grief.
The decision marks an end to a long debate within the field of mental health, steering researchers and clinicians to view intense grief as a target for medical treatment, at a moment when many Americans are overwhelmed by loss.
The new diagnosis, prolonged grief disorder, was designed to apply to a narrow slice of the population who are incapacitated, pining and ruminating a year after a loss, and unable to return to previous activities.
Its inclusion in the Diagnostic and Statistical Manual of Mental Disorders means that clinicians can now bill insurance companies for treating people for the condition.
It will most likely open a stream of funding for research into treatments — naltrexone, a drug used to help treat addiction, is currently in clinical trials as a form of grief therapy — and set off a competition for approval of medicines by the Food and Drug Administration.
Since the 1990s, a number of researchers have argued that intense forms of grief should be classified as a mental illness, saying that society tends to accept the suffering of bereaved people as natural and that it fails to steer them toward treatment that could help.
A diagnosis, they hope, will allow clinicians to aid a part of the population that has, throughout history, withdrawn into isolation after terrible losses.
“They were the widows who wore black for the rest of their lives, who withdrew from social contacts and lived the rest of their lives in memory of the husband or wife who they had lost,” said Dr. Paul S. Appelbaum, who is chair of the steering committee overseeing revisions to the fifth edition of the D.S.M.
“They were the parents who never got over it, and that was how we talked about them,” he said. “Colloquially, we would say they never got over the loss of that child.”
Throughout that time, critics of the idea have argued vigorously against categorizing grief as a mental disorder, saying that the designation risks pathologizing a fundamental aspect of the human experience.
They warn that there will be false positives — grieving people told by doctors that they have mental illnesses when they are actually emerging, slowly but naturally, from their losses.
And they fear grief will be seen as a growth market by drug companies that will try to persuade the public that they need medical treatment to emerge from mourning.
“I completely, utterly disagree that grief is a mental illness,” said Joanne Cacciatore, an associate professor of social work at Arizona State University who has published widely on grief, and who operates the Selah Carefarm, a retreat for bereaved people.
“When someone who is a quote-unquote expert tells us we are disordered and we are feeling very vulnerable and feeling overwhelmed, we no longer trust ourselves and our emotions,” Dr. Cacciatore said. “To me, that is an incredibly dangerous move, and short sighted.”
“I completely, utterly disagree that grief is a mental illness,” said Joanne Cacciatore, an associate professor of social work at Arizona State University who operates the Selah Carefarm, a retreat for bereaved people.
‘We don’t worry about grief’
The origins of the new diagnosis can be traced back to the 1990s, when Holly G. Prigerson, a psychiatric epidemiologist, was studying a group of patients in late life, gathering data on the effectiveness of depression treatment.
She noticed something odd: In many cases, patients were responding well to antidepressant medications, but their grief, as measured by a standard inventory of questions, was unaffected, remaining stubbornly high. When she pointed this out to psychiatrists on the team, they showed little interest.
“Grief is normal,” she recalls being told. “We’re psychiatrists, and we don’t worry about grief. We worry about depression and anxiety.” Her response was, “Well, how do you know that’s not a problem?”
Dr. Prigerson set about gathering data. Many symptoms of intense grief, like “yearning and pining and craving,” were distinct from depression, she concluded, and predicted bad outcomes like high blood pressure and suicidal ideation.
Her research showed that for most people, symptoms of grief peaked in the six months after the death. A group of outliers — she estimates it at 4 percent of bereaved individuals — remained “stuck and miserable,” she said, and would continue to struggle with mood, functioning and sleep over the long term.
“You’re not getting another soul mate and you’re kind of eking out your days,” she said.
In 2010, when the American Psychiatric Association proposed expanding the definition of depression to include grieving people, it provoked a backlash, feeding into a broader critique that mental health professionals were overdiagnosing and overmedicating patients.
“You’ve got to understand that clinicians want diagnoses so they can categorize people coming through the door and get reimbursement,” said Jerome C. Wakefield, a professor of social work at New York University. “That is a huge pressure on the D.S.M.”
Still, researchers kept working on grief, increasingly viewing it as distinct from depression and more closely related to stress disorders, like post-traumatic stress disorder. Among them was Dr. M. Katherine Shear, a psychiatry professor at Columbia University, who developed a 16-week program of psychotherapy that draws heavily on exposure techniques used for victims of trauma.
By 2016, data from clinical trials showed that Dr. Shear’s therapy had good results for patients suffering from intense grief, and that it outperformed antidepressants and other depression therapies. Those findings bolstered the argument for including the new diagnosis in the manual, said Dr. Appelbaum, who is chair of the committee in charge of revisions to the manual.
In 2019, Dr. Appelbaum convened a group that included Dr. Shear, of Columbia, and Dr. Prigerson, now a professor at Weill Cornell Medical College, to agree on criteria that would distinguish normal grief from the disorder.
The most sensitive question of all was this: How long is prolonged?
Though both teams of researchers felt that they could identify the disorder six months after a bereavement, the A.P.A. “begged and pleaded” to define the syndrome more conservatively — a year after death — to avoid a public backlash, Dr. Prigerson said.
“I have to say that they were kind of politically smart about that,” she added. The concern was that the public was “going to be outraged, because everyone feels because they still feel some grief — even if it’s their grandmother at six months, they are still missing them,” she said. “It just seems like you’re pathologizing love.”
Measured at the year mark, she said, the criteria should apply to around 4 percent of bereaved people.
The new diagnosis, published this week in the manual’s revised edition, is a breakthrough for those who have argued, for years, that intensely grieving people need tailored treatment.
“It’s kind of like the bar mitzvah of diagnoses,” said Dr. Kenneth S. Kendler, a professor of psychiatry at Virginia Commonwealth University who has played an important role in the last three editions of the diagnostic manual.
“It’s sort of an official blessing in the world,” he said. He compared it to astronomers deciding on a definition of planet. “This one’s in, and Pluto we kick out.”
If the diagnosis comes into common use, it is likely to popularize Dr. Shear’s treatment and also give rise to a range of new ones, including drug treatments and online interventions.
Dr. Shear said it was difficult to predict what treatments would emerge.
“I don’t really have any idea, because I don’t know when the last time there was a really brand-new diagnosis,” she said.
She added, “I really am in favor of anything that helps people, honestly.”
Dr. M. Katherine Shear, a psychiatry professor at Columbia University and a founding director of the Center for Prolonged Grief, has been studying the condition since 1995.
A loop of grief
Amy Cuzzola-Kern, 54, said Dr. Shear’s treatment helped her break out of a terrible loop.
Three years earlier, her brother had died suddenly in his sleep of a heart attack. Ms. Cuzzola-Kern found herself compulsively replaying the days and hours leading up to his death, wondering whether she should have noticed he was unwell or nudged him to go to the emergency room.
She had withdrawn from social life and had trouble sleeping through the night. Though she had begun a course of antidepressants and seen two therapists, nothing seemed to be working.
“I was in such a state of protest — this can’t be, this is a dream,” she said. “I felt like I was living in a suspended reality.”
She entered Dr. Shear’s 16-session program, called prolonged grief disorder therapy. In sessions with a therapist, she would narrate her recollection of the day that she learned her brother had died — a painful process, but one that gradually drained the horror out of the memory. By the end, she said, she had accepted the fact of his death.
The diagnosis, she said, mattered only because it was a gateway to the proper treatment.
“Am I ashamed or embarrassed? Do I feel pathological? No,” she said. “I needed professional help.”
Yet, others interviewed said they were wary of any expectation that grief should lift in a particular period of time.
“We would never put a time frame around when someone should or shouldn’t feel that they have moved forward,” said Catrina Clemens, who oversees the victim services department of Mothers Against Drunk Driving, which provides services to bereaved relatives and friends. The organization encourages bereaved people to seek mental health care, but has no role in diagnosis, said a spokesperson.
Filipp Brunshteyn, whose 3-year-old daughter died after an automobile accident in 2016, said grieving people could be set back by the message that their response was dysfunctional.
“Anything we inject into this journey that says, ‘that’s not normal,’ that could cause more harm than good,” he said. “You are already dealing with someone very vulnerable, and they need validation.”
To set a year as a point for diagnosis is “arbitrary and kind of cruel,” said Ann Hood, whose memoir, “Comfort: A Journey Through Grief,” describes the death of her 5-year-old daughter from a strep infection. Her own experience, she said, was “full of peaks and valleys and surprises.”
The first time Ms. Hood walked into her daughter Grace’s room after her death, she saw a pair of ballet tights lying in a tangle on the floor where the little girl had dropped them. She screamed. “Not the kind of scream that comes from fright,” she later wrote, “but the kind that comes from the deepest grief imaginable.”
She slammed the door, left the room untouched and eventually turned off the heat to that part of the house. At the one-year mark, a well-meaning friend told her it was time to clear out the room — “nothing worse than a shrine,” he told her — but she ignored him.
Then one morning, three years after Grace’s death, Ms. Hood woke up and returned to the room. She sorted her daughter’s clothes and toys into plastic bins, emptied the bureau and closet and lined up her little shoes at the top of the stairs.
To this day, she is not sure how she got from one point to the other. “All of a sudden, you look up,” she said, “and a few years have gone by, and you’re back in the world.”
Sit shiva for seven days. Spend another 30 in sheloshim — a secondary mourning period — and say the Mourner’s Kaddish for a year. Between all of its mourning rituals, Judaism offers plenty of structure to mourners, which can offer comfort and a structured space in which to grieve.
But as many rituals as there are, there are even more ways to make them one’s own.
“There’s so many ways that grief and mourning are aligned from person to person, and it is so unique and personal,” said Naomi Less, an associate director at Lab/Shul, a New York Jewish community that welcomes members who don’t believe in God. With a significant number of people who identify as Jewish also identifying as not religiously observant, that adaptability in ritual has begun to prove key to ensuring that age-old rituals stay relevant — and that even the nonreligious find comfort in spaces where those rituals are observed.
“Your own experience of grief is wildly different for each loss,” Less said.
Even with religion taken out of the equation, it can be hard to negotiate your own grief along other people’s ways of grieving. When different approaches to religion come into play, especially within a family or communal group all mourning the same loss, it can be particularly tricky.
A recent study from the Pew Research Center found that about a quarter of Jews do not identify with the Jewish religion, meaning they consider themselves culturally and ethnically Jewish, but may also identify as atheists or agnostic. That number gets higher for Jews under the age of 50, with four of every 10 Jews aged 18-29 identifying as nonreligious.
The need for common practices for handling family divides is therefore increasing. To cope with this challenge, Less suggests adding practices that feel right, rather than subtracting ones that don’t.
“If they’re doing a more traditional funeral service, maybe there’s a piece of poetry you can bring in, maybe there’s a song as people are entering the space that evokes a memory,” she said.
That approach can help make sure there’s room in mourning rituals for everyone.
Rabbi Tzemah Yoreh of the City Congregation for Humanistic Judaism in Manhattan, which also welcomes secular Jews, offers similar advice.
“Find the reading, find the piece, find the memory that you’d like to bring to the occasion,” Yoreh said. For example, many of the secular mourners he works with like to recite the Torah passage that begins, “To everything there is a season, and a time to every purpose under heaven.”
When there’s real disagreement within families over how to observe mourning rituals for a loved one, it can be helpful to bring in a rabbi or someone else who can mediate. “Sometimes it’s helpful to have somebody to sit with you to talk about these things, because the emotions are running so high,” Less said. “It’s just nice to have somebody sit with you, actively listen, share back, and try to find commonalities for families.”
When the pandemic hit, Lab/Shul, where Less works, compiled a guide to mourning for its congregants, consistent with its emphasis on artistic expression.
The guide, which is available online, is largely geared toward adapting traditions for social distancing. But it also offers ways to mix up traditions that might be more palatable to those who aren’t religious, such as making a playlist of songs the loved one liked or volunteering to honor their memory.
“It’s kind of a glossary of Jewish mourning and the cycles of mourning,” Less said. “And then it offers different kinds of ideas for creative ways to make it your own, ways to make it more personal.”
Lab/Shul also offers a weekly virtual Kaddish call that usually attracts about 20 people. She says it has been a meaningful way for mourners from all walks of Jewish life to create community.
“These folks who came because they heard about this call are now wanting to connect in person,” Less said. “There are groups that have connected in different parts of the country because folks call in from everywhere.”
For people who want to say Kaddish but don’t believe in God, the synagogue also offers alternatives to the prayer in English that use nonreligious language.
Of course, there’s no one set of customs that all secular Jews will want to follow when it comes to mourning.
“Secular Jews tend to be individualistic and are not seeking those unifying rituals, necessarily,” Yoreh said. For them, resisting structure might be part of the point.
Olena Koval found out that her husband was dead via text message. He was shot by Russian soldiers inside their home in Bucha while she was sheltering nearby, their neighbors told Human Rights Watch. In the days that followed, despite the brutal cold and her spinal disability, she made repeated attempts to recover his body but was turned back each time by the soldiers’ threats.
As the atrocities escalated, Olena fled Bucha to save her remaining family. Before their departure, she left a note with a neighbor that marked where her husband’s body was, hoping someone could give him a burial.
War is synonymous with death, but its emotional toll extends beyond the loss of life. The inability to say farewell to one’s loved ones and lay them to rest can often be just as painful.
Humans have always cared for their dead – so much that archaeologists often consider mortuary rites among the traits that distinguish Homo sapiens from other species. In other words, it is a fundamental part of being human.
Paying respect
Humans’ close relatives also showed concern for the dead. The Neanderthals practiced burials, and other extinct hominids probably did too. Even chimpanzees appear to grieve over deceased relatives. But no other species goes to such extraordinary lengths to care for its dead.
As an anthropologist, I have spent two decades studying rituals, particularly those that can seem “extreme.” At first glance, these customs seem puzzling: They appear to have no direct benefits but can feel utterly meaningful. A closer look, however, shows that these seemingly senseless acts express deeper, profoundly human needs.
Take funerary rites. There is a practical need to dispose of a dead body, but most burial customs go far beyond that requirement. Among the Toraja people of Indonesia, for example, deceased family members are kept in their homes for months or even years. During that time, their relatives treat them as if they were still living: They offer them food, change their clothes, and bring them the latest gossip. Even after their funeral, their mummified bodies are exhumed, dressed up, and paraded around town on ceremonial occasions.
Residents participate in a funeral procession to honor ancestors in Tana Toraja Regency, South Sulawesi, Indonesia.
The Toraja are not alone. In Madagascar, I have visited communities where people lived in fragile reed huts, at the mercy of frequent deadly cyclones, as the only robust brick-and-mortar buildings in the area were used as tombs. And in the ancient city of Petra in Jordan, the architectural masterpieces carved into the rock by the Nabataeans two millennia ago were resting places for the dead.
Those practices may seem like outliers, but they are not. In all cultures, people clean, protect, embellish and carefully deposit their dead. Muslims wash and shroud the body before interring it. Hindus may bathe it with milk, honey and ghee and adorn it with flowers and essential oils before cremation. Jews keep watch over the deceased from the time of death until the burial. And many Christians hold wakes at which family members gather to pay tribute to the deceased.
Creating closure
Funerary rites are ostensibly about the dead. But their importance lies in the roles they play for the living: They allow them to grieve, seek comfort, face the reality of death and find the strength to move on. They are deeply human acts, which is why being deprived of them can feel devastating and dehumanizing.
This is what is happening in Ukraine.
In besieged cities, people cannot retrieve the bodies of their loves ones from the streets out of fear of being killed. In other cases, Ukrainian officials have accused the Russian army of burying victims in mass graves to hide war crimes. Even when they are retrieved, many of the corpses have been mutilated, making them difficult to identify. To people who have lost their loved ones, the lack of a proper send-off can feel like a second loss.
Tanya Nedashkivs’ka, 57, mourns the death of her husband at the site where he was buried in Bucha, on the outskirts of Kyiv, Ukraine, Monday, April 4, 2022.
The need for closure is widely recognized to be indispensable – not only by anthropologists and psychologists, but also first responders, governments and international organizations. This is why armies go to great lengths to return the remains of fallen soldiers to their families, even if that takes decades.
The right to a burial is acknowledged even for one’s foes. The Geneva Convention stipulates that belligerents must ensure that the bodies of enemies are “honorably interred” and that their graves are respected and “properly maintained and marked so that they may always be found.”
Given the importance of those rites, it is also striking that the Russian defense ministry has reportedly been reluctant to bring their own dead back home, because they are concerned with covering up the scale of the losses. This seeming indifference to the suffering of Russia’s own people and their need for closure may be yet another act of dehumanization.
The older we get, the more life and death tangle. In this poem, the speaker occupies the liminal space of transition, where the child and the parents begin to switch roles. This poem toggles among birth, life and death seamlessly — it starts with objects remaining after a recent death, and eventually turns to the speaker running errands with his aging parents. This final unannounced shift is what gives this poem gravity — changes are always happening, and time’s movement is constant, but our awareness of these changes arrives at the most mundane moments: buying cupcakes at a bakery, or picking up cold medicine at the pharmacy. Selected by Victoria Chang
Of Errands
By Rick Barot
On a table in the living room
there is a gray ceramic bowl that catches
the light each afternoon, contains it.
This is the room we turned into
the room of her dying, the hospital bed
in the center, the medical equipment
against the walls like personnel.
In Maine, once, I rented a house hundreds
of years old. One room had been
the birthing room, I was told, and I sat
in that room writing towards the bright
new world I am always trying
to write into. And while I could stop
there, with those two recognitions
of endings and beginnings, I’m thinking
of yesterday’s afternoon of errands.
My father and mother were in the backseat,
my sister in the passenger seat,
and I driving. It was like decades ago
but everyone in the wrong places,
as though time was simply about
different arrangements of proximity.
Sometimes someone is in front of you.
Or they are beside. At other times
they are behind you, or just elsewhere,
inconsolably, as though time was
about how well or badly you attended
to the bodies around you. First, we went
to the bakery. Then the hardware.
The pharmacy, the grocery. Then the bank.
STEPPING BACK FROM THE LEDGE A Daughter’s Search for Truth and Renewal
By Laura Trujillo
When a loved one dies by suicide, it can reverberate through the family for generations. In some instances, the emotional toll is worse than that of a murder. If — and this is a crucial “if” — the murderer is convicted and the motives and circumstances of the crime are aired, the family can at least clothe its grief in a conclusive story. In the case of most suicides, family members are left with the agony of guessing, and the guilt that ensues — I could have saved her, if only I’d heeded the signs — can lead them to imagine that they are inadvertently the killers themselves.
In her moving memoir, “Stepping Back From the Ledge,” a veteran journalist takes readers to this difficult place. Here’s the history, painful as it will be to read: On April 26, 2012, Laura Trujillo’s mother killed herself by jumping from the edge of the Grand Canyon. Mother and daughter were extremely close, and the circumstances surrounding the suicide make the web of Trujillo’s emotions a challenge to untangle.
Several months earlier, a visit to her stepfather at a rehab center where he was recovering from a stroke provoked vivid memories of his repeated intrusions into her bedroom to rape her from the time she was 15. The abuse continued throughout her adolescence, and to protect her mother, who seemed rejuvenated by her new marriage, Trujillo bore it in frozen silence. “She had her confidence now, joy, and I couldn’t ruin that, I told myself, no matter what he did to me.”
Trujillo was a happily married mother of four, with a fulfilling job as managing editor of The Cincinnati Enquirer. Recollections of her stepfather’s abuse shook the foundation of her life, to say the least, so her therapist suggested that she tell her mother what happened. Shock and guilt followed the revelation and their rich relationship became fraught and strained. Hoping to repair the rift and unburden herself of her trauma, Trujillo sent a long email to her mother, expressing all that she had felt and experienced. One of the haunting questions is whether her mother knew what was happening with her stepfather. “I told her I didn’t forgive her, because I didn’t need to forgive her. It wasn’t her fault. It was his.”
Two days after receiving the email, her mother killed herself. “I was certain I was responsible,” writes Trujillo. To make matters worse, her maternal grandmother and her mother’s siblings blamed her for the tragedy. They ostracized her and her children at the funeral, embracing the abuser, now a hobbled, elderly man, seemingly incapable of the crimes he had committed decades ago.
The loss of her mother plunged Trujillo into a deep depression. She plotted her own death, writing (and rewriting) goodbye notes to her husband and children. Trujillo ably describes the pernicious logic of suicidal depression. Ending it all became the only reasonable solution: “I truly believed at the time that my children would be better off without me — it seemed so normal and obvious.” The decision provoked a temporary sense of relief and calm. Enveloped by this feeling, she headed toward the Grand Canyon to join her mother.
How the author stepped back from this ledge constitutes the heart of the story. The process is slow, almost imperceptible at first. In a memoir like this, the author must be both scientist and lab rat, painstakingly dissecting her mother’s behavior and her own under duress. When Trujillo struggles to convey the most trying experiences, her inarticulateness becomes a form of eloquence. Among her realizations is that suicide is a mysterious and unknowable aspect of being human.
As mysterious are the ways we find to heal. Trujillo inherits a bracelet that her mother wore on her right arm on the day of her death. The bracelet is bent, and Trujillo wants to know if this is because of the impact of the fall. In the course of her investigative work, she reads the medical examiner’s autopsy report, which indicates she fell on the left side of her body. The “bend in the bracelet must have been simply from my mother squeezing it to fit on and off her wrist.” In the irresoluble shadow of suicide this fact offers comfort.
The most enduring pain is in the impossibility of understanding why. Trujillo’s mother had bouts of depression throughout her life. Is this knowledge enough to alleviate her daughter’s agony of self-blame? With suicide, Trujillo writes, “only one person ‘gets’ an ending; the rest of us are left with a story abandoned midsentence.” Fearlessly, Trujillo attempts to complete the sentence. For many who have been touched by suicide, her hard-earned story will be a helpful companion.
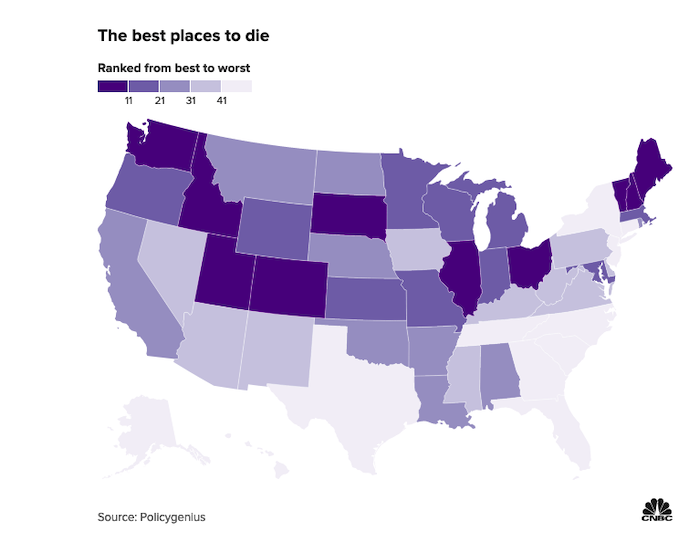
Your end-of-life experience may be very different depending on where you live, according to a Policygenius report.
The report ranks the best and worst U.S. places to die based on funeral costs and services, green burials, palliative care, Medicare providers, at-home deaths and probate shortcuts.
Your end-of-life experience may be very different depending on where you live, according to a Policygenius report that ranks the country’s best and worst places to die.
The report gave each state and the District of Columbia a numerical score based on seven factors, including funeral costs and services, green burials, palliative care, Medicare providers, at-home deaths and probate shortcuts.
“I think the big takeaway of this project is to get people thinking about the costs associated with the end of life,” said Logan Sachon, senior managing editor of research at Policygenius. “Because some of them can be mitigated through planning.”
“If you look at the top 10 and bottom 10, there aren’t any specific things they all have in common,” Sachon said. “They are each kind of unique in their own way.”
Indeed, Vermont, ranked as the No. 1 place to die, was among the most expensive for funeral costs but scored highest for palliative care, which focuses on pain relief, management and emotional support.
Florida, known for its high population of retirees, came in last place, with the fewest Medicare providers per capita, and scored low for at-home deaths and palliative care.
The best places in the U.S. to die
Vermont
Utah
Idaho
Ohio
South Dakota
Maine
Colorado (tie)
Illinois (tie)
New Hampshire
Washington
The worst places in the U.S. to die
Florida
Alaska
Texas
Hawaii
New York
Georgia
New Jersey
North Carolina
South Carolina
Connecticut
It’s never too early for older Americans to prepare for end of life, Sachon said.
Experts recommend an advanced directive, also known as a living will, covering your medical care preferences. You’ll also need a health-care proxy or power of attorney, naming someone to make medical decisions on your behalf if needed.
Estate planning
The report also focuses on each state’s probate process, which determines the cost and time it takes to settle your estate.
As of June 2021, only 17 states and the District of Columbia have an estate or inheritance tax, according to the Center on Budget and Policy Priorities.
With different laws in every state, a local estate planning attorney may share some options to protect your assets and carry out your wishes, depending on where you live.
There’s no federal estate tax on wealth below $12.06 million for individuals in 2022, and with proper planning, married couples can transfer their unused exemption to their surviving spouse, effectively doubling it to $24.12 million.
However, this reverts to an estimated $6 million exemption in 2026 when provisions from the Tax Cuts and Jobs Act sunset.