[H]awaii recently joined the growing number of states and countries where doctor-assisted dying is legal. In these jurisdictions, help to die is rarely extended to those who don’t have a terminal illness. Yet, increasingly, very old people, without a terminal illness, who feel that they have lived too long, are arguing that they also have a right to such assistance.
Media coverage of David Goodall, the 104-year-old Australian scientist who travelled to Switzerland for assisted dying, demonstrates the level of public interest in ethical dilemmas at the extremities of life. Goodall wanted to die because he no longer enjoyed life. Shortly before his death, he told reporters that he spends most of his day just sitting. “What’s the use of that?” he asked.
Research shows that life can be a constant struggle for the very old, with social connections hard to sustain and health increasingly fragile. Studies looking specifically at the motivation for assisted dying among the very old show that many feel a deep sense of loneliness, tiredness, an inability to express their individuality by taking part in activities that are important to them, and a hatred of dependency.
Of the jurisdictions where assisted dying is legal, some make suffering the determinant (Canada, for example). Others require a prognosis of six months (California, for example). Mainly, though, the focus is on people who have a terminal illness because it is seen as less of an ethical problem to hasten the death of someone who is already dying than someone who is simply tired of life.
Why give precedence to physical suffering?
Assisted dying for people with psychological or existential reasons for wanting to end their life is unlikely to be supported by doctors because it is not objectively verifiable and also potentially remediable. In the Netherlands, despite the legal power to offer assistance where there is no life-limiting illness, doctors are seldom convinced of the unbearable nature of non-physical suffering, and so will rarely administer a lethal dose in such cases.
Although doctors may look to a physical diagnosis to give them confidence in their decision to hasten a patient’s death, physical symptoms are often not mentioned by the people they are assisting. Instead, the most common reason given by those who have received help to die is loss of autonomy. Other common reasons are to avoid burdening others and not being able to enjoy one’s life – the exact same reason given by Goodall. This suggests that requests from people with terminal illness, and from those who are just very old and ready to go, are not as different as both the law – and doctors’ interpretation of the law – claim them to be.
Sympathetic coverage
It seems that the general public does not draw a clear distinction either. Most of the media coverage of Goodall’s journey to Switzerland was sympathetic, to the dismay of opponents of assisted dying.
Media reports about ageing celebrities endorsing assisted dying in cases of both terminal illness and very old age, blur the distinction still further.
One of the reasons for this categorical confusion is that, at root, this debate is about what a good death looks like, and this doesn’t rely on prognosis; it relies on personality. And, it’s worth remembering, the personalities of the very old are as diverse as those of the very young.
David Goodall died listening to Beethoven’s Ode to Joy.
Discussion of assisted suicide often focuses on concerns that some older people may be exposed to coercion by carers or family members. But older people also play another role in this debate. They make up the rank and file activists of the global right-to-die movement. In this conflict of rights, protectionist impulses conflict with these older activists’ demands to die on their own terms and at a time of their own choosing.
In light of the unprecedented ageing of the world’s population and increasing longevity, it is important to think about what a good death looks like in deep old age. In an era when more jurisdictions are passing laws to permit doctor-assisted dying, the choreographed death of a 104-year-old, who died listening to Ode to Joy after enjoying a last fish supper, starts to look like a socially approved good death.
Today we are talking about death, looking at philosophical approaches from Socrates, Epicurus, and Zhuangzi. We will consider whether it’s logical to fear your own death, or the deaths of your loved ones.
[T]he building that houses Milward Funeral Directors in Lexington, Kentucky has been around for 193 years. It’s a three-story maze that starts with a light-soaked, stone-floored entrance hallway. The hallway is home to an awfully regal cage of tiny, yellow-breasted finches, and they greet you as you walk in through the funeral home’s front doors. Even when they’re out of sight, you can hear their occasional, lively chirps, particularly if you’re in any of the nearby pastel-hued rooms on the first floor. Say, the powder blue chapel, the pink viewing room, the green family meeting room, or the front office where office associate Elaine Kincaid has found a way to answer the ever-ringing phone with a pressing sense of compassion.
By contrast, it’s nearly pin-drop-silent in the upstairs casket showroom, where, if you were preparing to bury a loved one, you would arrive to find a selection of 30-plus casket models in every variation of wood and steel. Should you be cremating your loved one, there’s an adjoining hall where you could select an urn, each one of them unique in presentation and name — “White Orchid” for the porcelain vase and “Solitude” for the simple, gold rectangle. You could also turn loved ones’ cremated remains into jewelry, a keychain, a bench or, in the words of Miranda Robinson, Milward’s youngest mortician, “pretty much anything you want.”
Like Milward funeral home, Miranda Robinson is polished and professional. Yet, at 30-years old, she both embodies and defies the stereotypes often associated with morticians. Yes, she has a fascination with death and dying. Yes, she loves the skeletal system, owns a black cat, and displays a ouija board on her apartment’s living room table — but she’s anything but morose. In fact, her bubbly Kentucky drawl is often interrupted by a burst of up-swinging giggles, even while discussing death. She used to be a cabaret performer and closely follows RuPaul’s Drag Race. Her most-used word is “lovely” and her retro-feminine personal aesthetic matches that same description.
At around 5 feet, 4 inches tall with an obvious flair for vintage, Miranda pays almost as much attention to her own presentation as she does to those on her embalming table. Robinson clips in hair extensions that she curls every morning. Her arms, which remain covered while at work, are decorated with tattoos. One of them is of a bottle of embalming fluid.
Still, at first blush you’d never guess that Robinson works with the dead on a daily basis. And, perhaps, you’d never guess how many women her age are actively entering the field, either. Frustrated by nursing school and looking for a change, Robinson shifted gears from aiding the living to preserving the dead, and enrolled in mortuary school in Cincinnati, Ohio. In doing so she joined the ranks of young women now outnumbering men in the mortuary education system. In fact, the National Funeral Directors Association reports that, “While funeral service has traditionally been a male-domination profession…today, 60% of mortuary science students in the United States are women.”
Once a male-dominated industry, after-life and funeral care is now becoming not only a budding, female-centric space but also one ripe for disruption. And no one knows this better than Miranda. “Even in mortuary school, I was taught that [funeral service] was still a different, difficult field for women.” She explains, “Women, so I’ve heard, were expected to wear skirts and heels still, so it seemed, before I got into the funeral home, that [the] funeral service [industry] hadn’t come a long way for women… but now that I’m here, I feel like I’ve made my mark and I’m really seeing women in funeral service emerge.” They’re emerging and they’re excelling, bringing with them calm, care, and attention to detail that may have long been lacking.
While embalming, Miranda says she feels like “both an artist and a scientist,” because her work combines aspects of both. Made prevalent during the Civil War, when bodies of fallen soldiers were shipped back home for viewings and funerals, embalming is a technique used to preserve the deceased by replacing a portion of their blood with chemicals (including formaldehyde). The body is also made up to look as it did in life — lipstick and all. But, while this method may long be favored in the United States, a new wave of green burial options seeks to challenge the traditional funeral industry. In fact, for the second year running, cremation is now more popular than burials, and the National Funeral Directors Association only expects this trend to continue.
That’s because green burials, alternative and eco-friendly practices are popularizing. Some of these green practices, like home funerals and vigils, pre-date the popularization of embalming, while others like bio-urn cremation (when the body’s cremated remains are buried and grow with the seeds of a plant) or aquamation (a proposed way of breaking down a body using water rather than fire) are brand new. Whether the increased options in funeral care signify an impending end of the traditional funeral industry that Miranda is a part of is a matter that may only be answered in time. For now, what it does mean is that this freshly energized attention to death care is bringing light to a space that, despite touching every single life on Earth, has largely been kept in the shadows.
Ultimately, it is not the method of end-of or after-life care that concerns women like Miranda, but rather the instinct to talk about death in a meaningful way, early and often. Miranda loves her job because what she does helps bring peace to grieving families. She explains, “The most beautiful thing about my job, is taking the loved one into my care from a removal, especially when family is gathered, just that intensity of how much they love that person. It’s an absolute honor to be in the worst possible moment in someone’s life. To be there and for them to look at me and just me to try to at least give them some answers, to try to give them some peace in that moment.”
And while it may seem strange to light up while talking about death, it’s a conversation everyone will someday need to have, regardless of personal preference or spiritual beliefs. Miranda has this conversation every day — at work, at home, with her 1,859 instagram followers — and in doing so helps to de-stigmatize a topic that’s long been off-limits.
As a mortician, Miranda believes that viewing the body is of the utmost importance. As she puts it, “I think it’s important to see the body because you face the reality of what’s actually happened.” But, it’s the trend toward personalization, transparency and increased discussion around death and dying that continues to be a universal priority for many women working in both alternative and traditional funerals.
For Miranda, part of this conversation means addressing the details of her own funeral. And, of course, she can’t imagine anything more fitting than a traditional embalming. Ever the enigma, while her choice to embalm may be traditional, her last look will be anything but. Robinson would like a “glitter casket” with a leopard interior. Dark brown extensions will be clipped and curled, her lips will be painted in the bright red pigment Ruby Woo by Mac. Years from now, when that day comes, Miranda may very well lay on the table that she works alongside every single day at Milward Funeral Directors, in the storied embalming room that she considers sacred. Perhaps somewhere beneath her in the entry hall, the finches will be singing.
“Death is inevitable. My life span is ever decreasing. Death comes whether or not I am prepared.” These are three of the nine contemplations on death written by Buddhist teacher Atisha — and Alua Arthur reads them to clients during death meditations. As a death doula and owner of Going With Grace, an end of life and death care company, Arthur (who graduated from law school before shifting to work in the death industry) facilitates these sessions to help people who are uncomfortable with the idea of death or dying.
“Death meditation is an opportunity for people that are struggling with some fears around death and dying to confront those fears head-on,” Arthur says. “It’s not for the faint of heart. It’s an opportunity to really think about the body’s eventual decline, and to go there to see what the discomfort is, so that we can then talk about that and process that. It’s intended to soften the fear around death.”
And, true to her claim, Arthur’s work is meant to soften fears around death. “Doula” is a word derived from a Greek term meaning, “women who serve.” As a death doula, she works with clients to plan for the final stage of their lives, holds space to support them emotionally through their deaths, and ensures their wishes are met.
Arthur developed a nine-part “Advanced Care Directive” that allows clients to list how they’d like to be cared for in the event of terminal illness. It includes everything from personal grooming preferences to thoughts on life support. By filling out Arthur’s document, a client can clearly state how they’d like their social media to be handled in the event of their death and whether they’d prefer to be embalmed, buried in a bio-urn (a seed pod for ashes that nourishes the earth and grows into a plant), or anything in between. She’s helped prepare for end of life with healthy millennials, large family groups, and even her own father.
Alua Arthur
Of course, when it comes to her own funeral, Arthur, who thinks about death “all day, every day” knows exactly what she wants. If possible, she’d prefer to die outside, at sunset. And she wants to be buried in a pink or orange raw silk shroud. Her funeral will be a party filled with music (Michael Jackson is a must on the playlist). She’d like her jewelry — an extensive collection of bangles and big earrings — hung on trees and for attendees to take the pieces they like. This tendency toward bright colors, generosity and liveliness mirrors Arthur’s sensibility in life. Her smile is contagious. Arthur’s yellow and magenta and green African-print frocks are a far cry from the drab, stereotypical wares one might associate with the death industry. In fact, there’s nothing grim about her or the work she does.
Yes, Arthur’s death consultations can be heartfelt and tearful to be sure, but, as she puts it, “death can definitely be funny.” And so, she approaches each conversation with a seemingly effortless but effective sense of levity. Arthur is part of a new trend in the death industry that favors pre-planning, personalization, and, ultimately, the normalization of death as a topic of conversation. In Arthur’s vision of the world, everyone over the age of 18 has an end of life plan and is willing to talk openly about death, she says.
“I think people don’t talk about death, because we’re not really comfortable with it,” she says. “Yet, whenever I talk about my work, people always talk to me about death… I think my work gives people permission to talk about this thing that we all want to talk about anyway, yet we’re just not doing.”
So, while many of us may not all be ready to recite the nine contemplations just yet, we can take comfort in the words Arthur uses to signs off on all of her Advanced Care Directives: “Yes, one day you and I will die, but before that day, let us live.” When she says those words out loud, she can’t help but smile.
Threshold Choir members pray before visiting a patient at the Halquist Memorial Inpatient Center in Arlington, Va.
by Debra Bruno
[I]t’s a quiet afternoon at the Halquist Memorial Inpatient Center, a hospice, as four women huddle close, talking quietly in a tight circle before walking through the doors to sing to men and women on the threshold of death.
These women are part of the Threshold Choir, a group that brings the comfort of song to dying people.
A thin woman, who is in the last weeks of life, is the choir’s first stop. She is sitting nearly upright in a hospital bed, her daughter beside her. Leslie Kostrich, the group’s leader for this day, asks the older woman if she would like to hear a few songs. She nods; the singers set up folding stools and pull up close to her bed.
“We sing in a circle of love,” the women sing, a cappella and in three-part harmony. “In music we are joined.” As they sing, the woman gazes off with a faraway look in her eyes, as if she’s trying to remember something.
The group sings another song, and as they finish, the older woman claps softly. “Thank you,” she says. “Nice.”
It takes sensitivity, situational awareness and a dash of emotional intelligence to sing to the dying. The sound of soft harmonious voices can be very comforting as life closes down, but the songs can also bring forward the immediacy of death to family members sitting nearby. Singing in such an emotional environment takes practice and a recognition that it is less a performance than a service.
For the dying and their families, the singers are hoping to bring peace, comfort and a feeling of love. “We call it kindness made audible,” says Jan Booth, who with Kostrich is co-director of the Washington-area Threshold group.
It is also very life-affirming for those who sing in this unusual choir.
“When I tell people I’m in a choir that sings at the bedside of the dying, they’ll say, ‘Oh girl, what a good thing,’ or ‘Girl, you must have lost your mind,’ ” says Kadija Ash, 66.
But the opposite is true. “Sometimes I run” to rehearsals, she says, “because of the healing.” In the two years she has been a member of Threshold, Ash says, she has gone from having a fear of death to an ability to be more accepting of life’s ups and downs.
Kostrich, 60, who has been with the group for three years, likewise says: “This has changed my life. That’s not an exaggeration. It gave my life a spiritual dimension that I was totally unprepared to receive.”
Threshold Choir — which has more than 200 groups around the world — seems to have tapped into something both primal and much-needed: a growing desire not to recoil from death or abandon the dying but to face that ultimate truth and figure out how to help ease the isolation of those near the end.
Bedside singing is a way of “normalizing death,” says Kate Munger, 68, who founded the first group in the San Francisco area 18 years ago. Many of the choirs are started and run by baby boomers, who are comfortable shaking up the accepted way of doing things, Munger says. “We’ve done that for childbirth, for education, and now for our impending death.” She says the number of people participating in Threshold Choir has grown to about 2,000.
Similar deathbed choirs have also surged, including Hallowell Singers, based in Vermont, which recently celebrated its 15th year, says founder Kathy Leo. She estimates that Hallowell has as many as 100 spinoffs, mainly in the United States.
Although they sing some requested songs, such as “Amazing Grace,” Threshold Choir mostly uses a repertoire designed for singing around a dying person. The pieces tend to be limited to just a few words, and sung without accompaniment in three-part harmony.
The idea is to keep things simple and not tied to any spiritual tradition — for instance, “Thank you for your love” and “We are all just walking each other home.” Complicated verses could intrude on the process of dying, which often involves people retreating from the day-to-day and reviewing their lives.
During the afternoon at Halquist, the four Threshold singers — Booth, Kostrich, Ash and Margo Silberstein — move out into a hallway after their first group of songs. One hospice staffer says, “I love working on Thursdays because I love listening to this group.”
The group slips into another large room with four beds separated by curtains. A frail woman with brilliant blue eyes smiles at the group. In another bed, someone is making noises that are halfway between breathing and groaning.
The blue-eyed woman asks, “Do you know ‘A Mighty Fortress?’ ” The group knows some of the words to the hymn but ends up mostly singing “oooo” to its tune. After they finish, Kostrich offers, “We do have ‘Amazing Grace.’ ” “Oh yes,” the woman answers and quietly sings along with them. After they finish, she says: “Oh, thank you. That was just wonderful.” They go on to sing “Simple Gifts” and “He’s Got the Whole World in His Hands” and then a few Threshold songs.
A TV next to a different bed blares.
After they finish, they approach a man sitting at the bedside of a woman. Can they sing?
“She’s pretty well gone out, but you can try,” he says.
As they sing “Hold this family in your heart,” the man’s eyes redden. He shifts in his seat. They sing, “Rest easy, let every trouble drift away.” His chin starts to tremble. As they begin to sing “You are not alone,” the woman begins to breathe more loudly but doesn’t move. The woman in the bed across the room, where they first sang, calls out, “Beautiful!”
An hour later, as the group gets ready to leave the hospice, Kostrich says that singing with Threshold has given her a way to process her own family’s experiences with death. When her parents were dying in the 1980s, Kostrich says, no one acknowledged they were close to death, which didn’t allow her and her family to come to terms with the losses themselves. The Threshold Choir has both helped her in a small way alleviate her own loss and help others avoid that kind of pain, she says.
There’s another thing that comes out of Threshold singing: community. And that feeling is evident when group members get together for a twice-a-month rehearsal, often in a church basement in the District. All but one singer at this rehearsal is female, but they range in age from 20-somethings to 70-somethings, African American, Chinese and white, those with tattoos and those with carefully coifed hairdos. There are a lot of hugs and laughter.
Olivia Mellon Shapiro, 71, says that group members are her “kindred spirits.” When she retired from her work as a psychotherapist, she told a friend, “Now I want to sing people out in hospices,” Shapiro says. “My father sang himself out — he died singing, and I was very moved by that.” Her friend said, “Oh, that’s the Threshold Choir.”
“Now I have a new group that feels like home to me. It really does,” she says. “I’ve also always been a little afraid of death and dying, but I’ve always loved the idea of hospices. So the idea of singing people out in hospices to get more comfortable with the idea of death and dying appealed to me.”
(The group sings several times a month at Halquist in Arlington and also at Providence Hospital in Northeast D.C. through the nonprofit hospice provider Capital Caring.)
One of the singers, Lily Chang, 28, notes that the choir is helping her confront her own fears of loss.
Chang says she’s very close to her grandmother and, given her age, worries about her. “I remember telling my mom, ‘I don’t know what I would do’ ” if she died. “Thinking about it, engaging with it in different ways makes me feel better.”
[C]are at the end of life should address all of the important elements that play a critical role in ensuring a positive end-of-life experience for patients and families. Therefore, quality end-of-life care extends beyond managing physical pain to include psychosocial and spiritual needs.
Not all long-term care professionals carry the same understanding of the issues.
Frequently, nurses serve as advocates to support patients and families in making care decisions based upon their goals and values. Ideally, physicians, nurses and other team members work together to create an atmosphere of care and compassion in accordance with patient and family wishes.
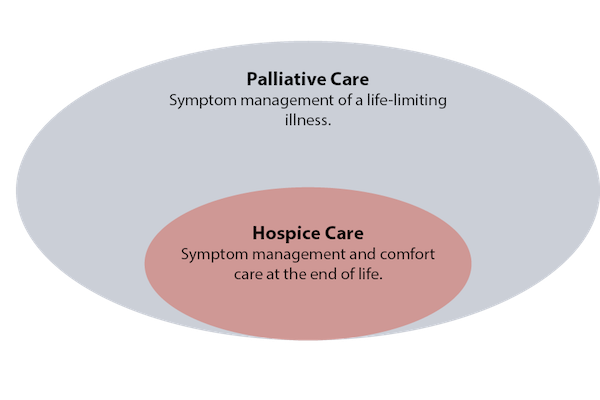
Although hospice and palliative care both aim to deliver quality holistic care, there are key differences.
The dimensions of hospice care
Hospice is the model for quality compassionate care for people facing a life-limiting illness. Hospice clinicians focus on pain and symptoms, and attend to the patient and family’s emotional and spiritual needs. Hospice is offered at a patient’s residence, such as their home or nursing home, or, if needed, in a hospice facility.
Hospice programs utilize an interdisciplinary team (IDT) approach to plan the care needed by patients and their families during the final weeks and months of life. The IDT is comprised of nurses, chaplains, social workers, physicians and medical directors, hospice aides, volunteers, bereavement specialists and other clinicians who develop and implement a plan of care that is formulated to relieve anxiety and suffering during the final months and weeks of a patient’s life. This approach allows the team to address physical, emotional, spiritual and social concerns that arise with advanced illness.
Hospice is available to people with all types of conditions and diseases, and focuses on comfort — not cure. Hospice provides care for the “whole person,” including physical care, counseling, spiritual needs, drugs, equipment and supplies related to the conditions that comprise the terminal prognosis. It also supports family caregivers, including bereavement support for up to a year after the patient’s death.
Financing hospice
Hospice care is reserved for people at the end of life who meet Centers for Medicare & Medicaid Services eligibility requirements and elect a comfort approach to care. The Medicare Hospice Benefit (MHB) requires that two physicians certify that a patient has less than six months to live if the disease follows its usual course. However, if a patient is still alive after six months, he or she can continue to receive hospice services if he or she meets eligibility requirements and demonstrates signs of progressive decline.
When a patient elects hospice, they sign off their Medicare Part A (hospital insurance) and enroll in hospice under the MHB. From that point on, hospice covers all services and care related to the terminal diagnosis and related conditions through Medicare, Medicaid and most commercial insurance.
The hospice IDT, together with the patient’s attending physician, is responsible for determining the plan of care. Under terms of the Medicare Hospice Benefit, the hospice agency is responsible for the plan of care and may not bill the patient for services. All costs related to conditions that affect the terminal prognosis are paid from a per diem rate that the hospice agency receives from Medicare. This per diem rate includes all drugs and equipment, nursing, social service, chaplain visits and other services deemed appropriate by the hospice agency. Care and medications not related to the terminal illness or related conditions continue to be paid for through original Medicare.
Distinctions of palliative care
The biggest differences between hospice and palliative care revolve around where the patient is in their illness related to prognosis, their goals/wishes regarding curative treatment, and how palliative care is financed.
Palliative care focuses on relief from physical suffering and caregiver burdens for individuals who are living with a chronic disease that may or may not be terminal, addressing their physical, mental, social and spiritual well-being. Atul Gawande recently defined palliative care “as the field devoted to providing people with serious life-limiting illness with expert care that serves their goals for quality of life, not just quantity of life.”
Similar to hospice, palliative care utilizes an interdisciplinary approach with highly trained professionals, including physicians, nurse practitioners, nurses, social workers, chaplains, and other disciplines.
Palliative care can be offered to people of any age, without restriction as to disease or prognosis. It may be appropriate for anyone with a serious, advanced illness, whether he or she is expected to recover fully, live with chronic illness for an extended time, or experience disease progression. Unlike hospice, patients receiving palliative care may continue to receive aggressive treatments, including life-prolonging therapies.
Conditions appropriate for palliative care include cancer, congestive heart failure, end stage renal or liver disease, chronic obstructive pulmonary disease, and dementia, among others. While palliative care is often appropriate earlier in the disease trajectory, referrals to palliative care clinicians are often not made until late in the disease process.
Palliative care focuses on relieving symptoms, such as pain, shortness of breath, fatigue, constipation, nausea, loss of appetite, difficulty sleeping and depression. Palliative care providers also support patients in carrying on with daily life so that they can tolerate medical treatments. In addition, patients receive support that empowers them to have more control over their care by improving communication so that they can better understand their choices for treatment. Helping patients and their caregivers coordinate care across care settings is a hallmark of palliative care.
Financing palliative care
Unfortunately, palliative care programs struggle financially because there is no reimbursement code specifically for palliative services and Medicare does not reimburse for interdisciplinary care management. Hospital-based palliative care is paid by the health system with some fee-for-service (FFS) billing for physician services. Medicare Part B covers physician and nurse practitioner (NP) fees for outpatient care delivered in the community or in clinics. Therefore, most community-based palliative care programs utilize NPs and physicians for home visits.
Other disciplines, such as nurses and social workers cannot bill Medicare for palliative home visits. Palliative care is also paid for through flexible bundled payments under Medicare Advantage, Managed Medicaid, ACOs and other commercial payers.
While Medicare doesn’t have a palliative care benefit, CMS has authorized demonstration projects that are testing different ways of meeting the needs of seriously ill patients. The Medicare Care Choices Model allows patients to receive hospice-like support services while concurrently being treated for their illness.
Demonstrated value
Costs for palliative care teams and programs are offset by fewer trips to emergency departments and lower hospitalization and rehospitalization rates. In addition, patients and families rate the value of palliative care services highly. This explains why 80% of hospitals with 50 beds or more have established palliative care teams and some are starting to consider outpatient palliative care programs. In addition, health plans and payers, including Accountable Care Organizations (ACOs), Integrated Delivery networks (IDNs) and other types of provider-driven managed care organizations, are beginning to offer community-based palliative care programs to their patients/members to extend the benefits of palliative care into the home.
Palliative care programs and advance care planning that include earlier conversations about patient and family goals of care are consistently demonstrating their value in helping patients live their final days in accordance with their wishes. Data shows that in communities that provide greater access to palliative care programs, patients are less likely to die in the hospital.
Furthermore, findings show that patients experience fewer admissions to the intensive care unit in the last six months of life and are less likely to die in an ICU
Today, palliative care is becoming recognized as option at any stage of advanced illness, not simply reserved for care at the end-stage of life. Its use should be driven by patient need, not disease prognosis. Hospice care remains the gold standard for end-of-life care. Together, hospice and palliative care offer compassionate care when it is needed most.
That sounds judgmental, but it’s more akin to wishful thinking.
While death is a certainty, it’s rarely a goal, so we tend to resist, to worry, to grasp at new treatments or old beliefs.
But the emerging death doula movement offers another option: We can’t change the destination, but we can improve the journey.
The term doula is more linked to childbirth, describing someone present during labor to help a mother feel safe and comfortable. There’s no medical role; doulas are companions and listeners. They attend.
End-of-life doulas, also called death doulas or death midwives, similarly are attuned to a dying person’s emotional needs.
“It’s about filling a gap that the system doesn’t acknowledge,” said Christy Marek, an end-of-life doula from Lakeville. “The system is designed to tend the body. But when you get into the lonely feelings, the mess of real life, the expectations and beliefs around dying — those things don’t fit into the existing system.”
In some ways, death doulas signal a return to earlier times, when ailing parents lived with children, when life-extending options were fewer.
“Death was more of a ritual, really laboring with someone as they were dying,” said Jeri Glatter, vice president of the International End of Life Doula Association (INELDA) in New Jersey.
Family and friends “felt a sense of acceptance and completion and a knowledge that they had fully honored someone,” she said. “It’s the most loving act that they could do.”
Over time, though, “we became a very medicated society — and thank God for that. I don’t want to diminish that,” Glatter said. But medical options can create a sense of disconnect with our inevitable mortality. When those options are exhausted, “we say we’ll house them, make sure they have medication and have a bed that goes up and down.
“But people are saying, ‘I don’t feel OK about this.’ ”
Marek is the first end-of-life doula in Minnesota certified by INELDA, credited with creating the first death doula program for hospitals and hospices in 2003. It offered its first public training in 2015; last year, 700 people attended 18 sessions. Several other groups in Minnesota and elsewhere offer training and doula directories.
Glatter said the trend has roots with those who used birth doulas in the 1980s.
“These people now are burying their parents. Just as with birth, as we labor into the world fully engaged in that process, they’re saying, ‘I want to be fully engaged in this process.’ Doulas are the bookends of life.”
How can we do this together?
What does it mean to be fully engaged? Whatever the dying person wants it to mean.
“Is the person having their own experience, instead of trying to meet the expectations of the family?” Marek asked. “I’m there to create a space for the person who is dying to ask, ‘How can we do this together?’ ”
One woman, for example, asked Marek to tell everyone that she wanted acknowledgment — a greeting — each time someone entered her room, “even though it may look like she’s sleeping.”
Marek added, “I have no agenda other than reflecting to that person what they are saying, what they are feeling. I can give directions to family and friends, which is a comfort to the dying person because then people around them know what to do — and they feel listened to.”
As part of a new field, doulas occupy a niche among doctors, family, hospice and other factors. Sometimes, doulas fill practical needs, gathering paperwork or helping with funeral plans, particularly if relatives are distant, either geographically or emotionally.
More often, though, their roles are more personal: creating a vigil environment, writing letters to loved ones, helping family members recognize the signs of dying such as a change in breath and, finally, helping survivors deal with their loss.
Glatter said that doctors or hospital personnel sometimes worry that a doula will infringe upon medical decisions. But doulas have no medical role, and may even be able to provide information that doesn’t come up in medical conversations, “such as, ‘Do you know there’s a son with a restraining order?’ ”
Doulas’ lack of medical standing also enables consistency. Doctors may change. Hospice care may be suspended. “But a doula provides a continuity of care no matter what treatments are being done or not,” Marek said.
Dying as a creative process
Marek, 47, appears to wear not a speck of makeup. The physical transparency mirrors her comfort with the emotions that dying can expose. But it took her years to reach this point.
With a degree in child psychology, she intended to work with youngsters. Then she met a child life specialist, a field of which she’d never heard, describing someone who works with children with acute, often fatal, illnesses.
“It was like a lightning bolt went through me,” she said. “I knew that someday I would work with people who are dying. And it scared the pants off me!”
She went on to do other work, in the course of which she explored yoga, shamanism, writing, painting and more. She studied to become an anam cara, from pre-Christian Celtic spirituality that translates as “soul friend.”
Every few years, the idea of working with dying people surfaced, but never took hold. Then, five years ago, she learned about applying doula principles to the dying process. This time, the idea came cast as “the creative process at the end of your life,” and her path was clear.
“I feel like this has been following me my whole life,” Marek said. She took the training through INELDA, which includes vigil planning, working with the survivors, and self-care for doulas themselves. She founded a business, Tending Life at the Threshold.
“As doulas, we’re trying to normalize the experience of death,” Marek said.
She recalled one woman who said that her mother would love it if Marek would read the book of Psalms or a Hail Mary. “And I told her, ‘I can certainly do that. But it would be more meaningful if you did.’ ”
Once family members and friends learn that it’s OK to “lean into the pain,” she said, they may find a sense of comfort and ease with dying that, in turn, proves a gift to their loved one.
Another support system
Karen Axeen had been sick for what seemed like forever, after years of breast cancer and ovarian cancer and other chronic illnesses.
After spending almost all of 2016 in the hospital, she decided to enter hospice care. She also decided that she wanted a doula at her side.
“She kind of fell into the idea, talking with the hospital social workers,” said her daughter, Laura Fennell, who lives in Marshall, Minn. “I don’t live close by, so I think it was really helpful for her.”
Working with Marek, Axeen developed what’s often called a legacy project. In this case, she wrote several letters to each of her six grandchildren, to be read as they grow older.
“She wrote letters to be read on their 16th and 18th birthdays, on their wedding days, on the first day they have kids of their own,” Fennell said.
“I think I probably would have been lost after my mom had passed away, but Christy had everything organized,” she added. “It’s definitely a great service for those who don’t have family in the area.”
End-of-life doulas “are another support system,” Fennell said. “It was important for Mom to be able to get to know someone closely and have them walk her through the final process of life.”
Axeen died on Sept. 23, 2017, at age 57.
‘We know how to die’
Some death doulas volunteer with hospices or churches. Others work in hospitals, while others set up private practices.
Glatter mentioned a California prison where inmates with life sentences became end-of-life doulas “because they wanted to be able to care for their own,” she said. “They’re really an extraordinary group of men who wanted to pay their debt to society by helping other inmates as they die.”
An article in Money magazine included death doulas among “seven new jobs that reflect what’s important in 2017.” Also listed, compost collectors and vegan butchers.
The death doula trend reflects gradually more open attitudes toward death. Surveys show that 80 percent of Americans would prefer to die at home if possible, but few are able to. Yet the landscape slowly is changing. Hospital deaths slowly declined from 2000 to 2010. In that time, deaths in the home grew from 23 percent to 27 percent. Deaths in nursing homes held steady at about 20 percent.
The Centers for Disease Control suggested that the shifts reflect more use of hospice care. As the dying process becomes, for some, more grounded in the home, end-of-life doulas may become more familiar and, in Marek’s vision, help make death a natural part of life.
She reached that vision, in part, during an outdoor meditation project she began in 2014. For 1,000 days, she meditated for 20 minutes outdoors, no matter the weather. (It’s on Instagram as wonderofallthings.)
“Sometimes I’d be thinking, ‘This is awful. But that’s OK,’ ” she said. “It helped me develop a tolerance for whatever is happening, and to stay close to the fact that none of us is immune to the cycles of nature, including death.
“If you can sit when it’s uncomfortable — to be able to sit in the unknown — that’s huge.”
While family members may not be at peace with someone’s death, she added, they can be at ease with it as a natural outcome of life.
“One thing I believe firmly is that we know how to do this,” she said. “We know how to die, like every creature of nature does. We just need to get out of our own way.”