With her signature wit and wisdom, Emily Levine meets her ultimate challenge as a comedian/philosopher: she makes dying funny. In this personal talk, she takes us on her journey to make friends with reality — and peace with death. Life is an enormous gift, Levine says: “You enrich it as best you can, and then you give it back.”
Even for an unwavering nonbeliever like myself, a couple of days last week were very close to a religious experience as we watched my wife’s mother, Ruth Aylward Pommer, 87, pass from this life into what she so fervently believed would be glory in the next.
Observing the initially distressful but finally serene end of a purposeful life robustly lived was both moving and humbling, a replaying of nature’s endless symphony of life and death far beyond any human capacity to halt or reverse it. Reality in perpetually unstoppable motion.
I come from a small family, but Ruth’s extended clan is relatively vast, so it was a beautiful and compelling thing to see the legions of daughters and sons, grand-kids and great-grandkids and great-greats, other relatives and friends filter into the room to hold vigil, voice rosary prayers, tell stories, and say their final good-byes.
It was particularly magnificent to see Ruth’s children closely arrayed around her bed, eyes red with anguished concern, stroking her hair, dabbing her brow, whispering soft encouragements into her ears, carefully watching her for signs of pain or distress so they could immediately do what was required to ease it. This is love expressed in its deepest, most primal, most authentic form.
Although I have spent long hours reading and writing about the unsubstantiality of supernatural ideas, as Ruth slipped quietly away I still realized once again what I already knew — that spiritual yearning is as universally human as rage against injustice. And it is powerful. So powerful.
When the kindly young priest from Ruth’s small farming community delivered the words of last rites in respectful, gentle tones, and anointed her forehead and palms with holy oil, it felt ancient, almost primordial. It felt natural to embrace any ritual, any hope that would make this not a sad end but a beginning of something profoundly better.
For many people, few things in life are as terrifying as its end, and the attendant possibility of immortal nothingness, or, worse, endless suffering. This is why most Christians, including, as Ruth was, Catholics, focus their lives on not displeasing God and improving their chances of being heartily welcomed by St. Peter in Paradise one blessed day.
I get it, especially after this past week, after seeing fervent faith up close in ways I rarely do, at a time of great angst and sadness over the passing of a woman much loved and honored in her lifetime. Even I mourn the end of her life in a personal way. Aside from the courtesy, respect and kindness she always showed me, the big-city alien grafted onto a small farming town by way of a happenstance meeting with her daughter in a far-away land, she also gave me another treasured gift: acceptance. From the beginning, she went out of her way to make me feel part of the large family she headed.
So, there I was at the end of her life, a most secular fellow in the midst of a most religious tribe, and I must say, it was terribly moving.
The funeral service in a breathtakingly lovely community church was fittingly transcendent, with its respectfully hushed tones, the great-grandchildren singing “Amazing Grace” in the choir loft, the candles and incense, readings from Ecclesiastes (“To every thing there is a season …”), the well-said sermon that honored and treasured Ruth’s long life. People came from far and wide to attend, some driving for days to reach the church.
And there was comfort food in church halls after the wake and funeral service and then the burial gathering the following day an hour away, where she was to be laid to rest with her husband. Food is part of the ritual of human passing, where pleasure and pain, good memories and sad immediacies, converge for sustenance of those who have been left behind.
As I went through this process, though from a further emotional remove certainly than Ruth’s immediate family, I still appreciated the essential value of such loving rituals and heavenly yearnings in helping survivors move on and face their next existential challenge. I tried to not focus on the reality that these painful passages also can bring out the worst in us.
So, although nonbelievers can often be antagonistic toward faith, I am reminded that it is pointlessly unkind and destructive to ever denigrate something so visceral and nurturing to people’s lives, whatever one’s philosophical differences.
I was thinking last week, as I waited patiently with others for the inevitable, that at such times theology and religious doctrine seem irrelevant, even as they precisely structure the final proceedings of a life lived out. What matters is love, remembrance and, as necessary, forgiveness.
My parents lived good lives and expected to die good deaths. They exercised daily, ate plenty of fruits and vegetables, and kept, in their well-organized files, boilerplate advance health directives. But when he was 79, my beloved and seemingly vigorous father came up from his basement study, put on the kettle for tea, and had a devastating stroke. For the next 6½ years, my mother and I watched, heartbroken and largely helpless, as he descended into dementia, near-blindness and misery. To make matters worse, a pacemaker, thoughtlessly inserted two years after his stroke, unnecessarily prolonged his worst years on Earth.
That was a decade ago. Last month I turned 70. The peculiar problems of modern death — often overly medicalized and unnecessarily prolonged — are no longer abstractions to me. Even though I swim daily and take no medications, somewhere beyond the horizon, my death has saddled his horse and is heading my way. I want a better death than many of those I’ve recently seen.
In this I’m not alone. According to a 2017 Kaiser Foundation study, 7 in 10 Americans hope to die at home. But half die in nursing homes and hospitals, and more than a tenth are cruelly shuttled from one to the other in their final three days. Pain is a major barrier to a peaceful death, and nearly half of dying Americans suffer from uncontrolled pain. Nobody I know hopes to die in the soulless confines of an Intensive Care Unit. But more than a quarter of Medicare members cycle through one in their final month, and a fifth of Americans die in an ICU.
This state of affairs has many causes, among them fear, a culture-wide denial of death, ignorance of medicine’s limits, and a language barrier between medical staff and ordinary people. “They often feel abandoned at their greatest hour of need,” an HMO nurse told me about her many terminally ill patients. “But the oncologists tell us that their patients fire them if they are truthful.”
I don’t want this to be my story.
In the past three years, I’ve interviewed hundreds of people who have witnessed good deaths and hard ones, and I consulted top experts in end-of-life medicine. This is what I learned about how to get the best from our imperfect health care system and how to prepare for a good end of life.
Have a vision. Imagine what it would take you to die in peace and work back from there. Whom do you need to thank or forgive? Do you want to have someone reading to you from poetry or the Bible, or massaging your hands with oil, or simply holding them in silence? Talk about this with people you love.
Once you’ve got the basics clear, expand your horizons. A former forester, suffering from multiple sclerosis, was gurneyed into the woods in Washington state by volunteer firefighters for a last glimpse of his beloved trees. Something like this is possible if you face death while still enjoying life. Appoint someone with people skills and a backbone to speak for you if you can no longer speak for yourself.
Stay in charge. If your doctor isn’t curious about what matters to you or won’t tell you what’s going on in plain English, fire that doctor. That’s what Amy Berman did when a prominent oncologist told her to undergo chemotherapy, a mastectomy, radiation and then more chemo to treat her stage-four inflammatory breast cancer.
She settled on another oncologist who asked her, “What do you want to accomplish?” Berman said that she was aiming for a “Niagara Falls trajectory:” To live as well as possible for as long as possible, followed by a rapid final decline.
Berman, now 59, went on an estrogen suppressing pill. Eight years, later, she’s still working, she’s climbed the Great Wall of China, and has never been hospitalized. “Most doctors,” she says, “focus only on length of life. That’s not my only metric.”
Know the trajectory of your illness. If you face a frightening diagnosis, ask your doctor to draw a sketch tracking how you might feel and function during your illness and its treatments. A visual will yield far more helpful information than asking exactly how much time you have left.
When you become fragile, consider shifting your emphasis from cure to comfort and find an alternative to the emergency room.
And don’t be afraid to explore hospice sooner rather than later. It won’t make you die sooner, it’s covered by insurance, and you are more likely to die well, with your family supported and your pain under control.
Find your tribe and arrange caregivers. Dying at home is labor-intensive. Hospices provide home visits from nurses and other professionals, but your friends, relatives and hired aides will be the ones who empty bedpans and provide hands-on care. You don’t have to be rich, or a saint, to handle this well. You do need one fiercely committed person to act as a central tent pole and as many part-timers as you can marshal. People who die comfortable, well-supported deaths at home tend to have one of three things going for them: money, a rich social network of neighbors or friends, or a good government program (like PACE, the federal Program of All Inclusive Care for the Elderly).
Don’t wait until you’re at death’s door to explore your passions, deepen your relationships and find your posse. Do favors for your neighbors and mentor younger people. It doesn’t matter if you find your allies among fellow quilters, bridge-players, tai chi practitioners, or in the Christian Motorcyclists Association. You just need to share an activity face-to-face.
Take command of the space. No matter where death occurs, you can bring calm and meaning to the room. Don’t be afraid to rearrange the physical environment. Weddings have been held in ICUs so that a dying mother could witness the ceremony. In a hospital or nursing home, ask for a private room, get televisions and telemetry turned off, and stop the taking of vital signs.
Clean house: Hospice nurses often list five emotional tasks for the end of life: thank you, I love you, please forgive me, I forgive you, and goodbye. Do not underestimate the power of your emotional legacy, expressed in even a small, last-minute exchange. Kathy Duby of Mill Valley was raised on the East Coast by a violent alcoholic mother. She had no memory of ever hearing, “I love you.”
When Duby was in her 40s, her mother lay dying of breast cancer in a hospital in Boston. Over the phone, she told Duby, “Don’t come, I don’t want to see you.” Duby got on a plane anyway.
She walked into the hospital room to see a tiny figure curled up in bed — shrunken, yellow, bald, bronzed by jaundice, as Duby later wrote in a poem. Duby’s mother said aloud, “I love you and I’m sorry.”
Duby replied, “I love you and I’m sorry.”
“Those few moments,” Duby said, “Cleared up a lifetime of misunderstanding each other.”
Think of death as a rite of passage. In the days before effective medicine, our ancestors were guided by books and customs that framed dying as a spiritual ordeal rather than a medical event. Without abandoning the best of what modern medicine has to offer, return to that spirit.
Over the years, I’ve learned one thing: Those who contemplate their aging, vulnerability and mortality often live better lives and experience better deaths than those who don’t. They enroll in hospice earlier, and often feel and function better — and sometimes even live longer — than those who pursue maximum treatment.
We influence our lives, but we don’t control them, and the same goes for how they end. No matter how bravely you adapt to loss and how cannily you navigate our fragmented health system, dying will still represent the ultimate loss of control.
But you don’t have to be a passive victim. You retain moral agency. You can keep shaping your life all the way to its end — as long as you seize the power to imagine, to arrange support and to plan.
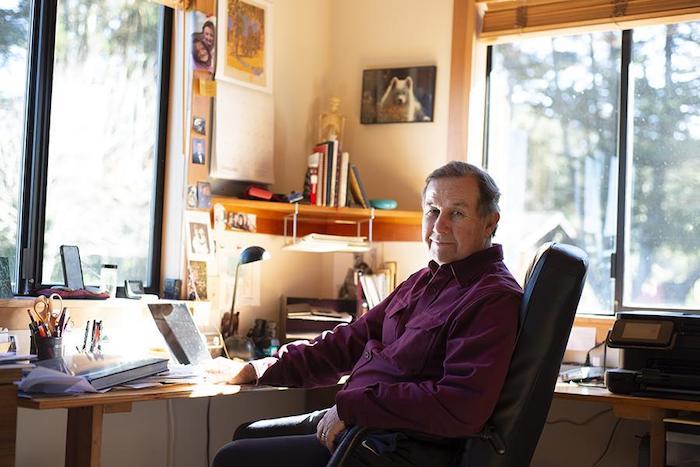
Dr. Steve Hadland learned over time to appreciate the “majesty and mystery” of death.
By Ellen Shehadeh
Dr. Steve Hadland began his medical career as an emergency room physician, fixing people and saving lives at all costs. These days he treasures his work as a hospice physician associated with Hospice of Petaluma, tending to the terminally ill and allowing them to die in comfort. Two extremes, one might say, but understandable given the intervening events in his life.
Steve’s practice melds a deep belief in social justice, reverence for life in all forms and enduring, self-described conservative views about end-of-life practices. His youthful face and genial manner, combined with an easy laugh and a soothing voice, belie the depth of his thinking, intellect and perceptions. He is informed not only by medical writings but also by psychology, literature, philosophy and classical music. One feels both calm and welcome in his presence.
Steve was the youngest in a conservative family growing up in Chicago. He attended university in Iowa City, studying astrophysics as a stepping stone to an astronaut program, and later majored in neuroscience. “University was a political and social awakening, as well as an intellectual one,” he says. He participated in marches and protests against the Vietnam War and for civil rights.
He longed to break out even further from his roots, however, and what better place than California, where “legend loomed for surfing and blondes.” He never quite managed the surfing thing, but wasted no time marrying his first wife, a blonde, during the summer of love, which coincided with his first year at Stanford Medical School. Their marriage of seven years included major involvements in the civil rights, anti-war and human potential movements.
All along, he had thoughts and profound feelings about end-of-life experiences, in part influenced by a Tolstoy novella, “The Death of Ivan Ilyich,” which he read in a death and dying course at Stanford. “It inspired me then, and continues to inspire me, year after year,” he says of the book, which he recommends “to anyone who really wants to know about what it’s like to die.”
Steve’s first job out of medical school, in 1972, was in a Kaiser emergency room. The nurses recognized his empathic nature and would steer the most difficult patients his way. Yet he recoiled at the Herculean efforts by staff to revive a dying patient, “all the excitement, the IVs,” and how quickly and “disrespectfully” staff abandoned a corpse when resuscitation efforts failed. At the time, there was no such thing as “do not resuscitate” or hospice.
Steve sought a different kind of medical experience and, in the fall of 1974, he arranged an interview with Dr. Michael Whitt in Point Reyes Station. He remembered the area from a drive many years before; “It cast a spell on me,” he says. Dr. Whitt’s liberal medical practice included home births, which at the time were popular in alternative communities, but Steve was stunned that he would deliver babies without liability insurance.
Steve’s conservative orientation and lack of maturity led him to decline a job offer by Dr. Whitt but, many years later, he would run a small integrative medical practice and pain management clinic out of his Point Reyes Station home. Ironically, he never secured liability insurance. “The influence of West Marin,” he quips.
Newly divorced in 1978, Steve encountered a single mother of three from Holland who was working as a Kaiser receptionist to pay her way through nursing school. They married two years later and, after 38 years, “it looks like it’s going the distance,” he says, laughing. Anneke van der Veen became an emergency room nurse, but they never worked together professionally, realizing the potential pitfalls of mixing business with pleasure.
Steve had traveled to England in 1978 to visit the first modern hospice. Although he was impressed with the approach, “I could tell I wasn’t ready for it,” he says. It was 12 years later that he helped start a hospice in Santa Clara, which he ran for five years along with an oncologist friend. He explains: “The world said, ‘You seem to be ready.’”
As society’s views about death and dying dramatically changed over the years, so clearly have Steve’s. Fifty years ago, death was a taboo subject and doctors rarely broached it with their terminal patients or even gave them an honest diagnosis. Now people take advantage of many choices, like refusing to eat and drink or using lethal medications now sanctioned by law. In California, the End of Life Option Act allows a patient to self-administer a lethal cocktail, but only after being judged by two physicians to be of sound mind and six months from death.
Some people object to the strictness of this law, which does not allow someone to assist in a patient’s suicide if the patient is physically or mentally unable to self-administer, even if it had been the patient’s expressed wish. In some states such assistance could be considered euthanasia or even murder.
Steve agrees with this self-described conservative view. “I don’t think it’s a bad thing; we don’t know what’s going on [inside their head]” or what kind of life these patients, some with Alzheimer’s and dementia, might have that we cannot fathom, he says. Surprisingly for a hospice worker, he was still opposed to the law when it was passed in July 2017, because “it’s a slippery slope.” How slippery? He cites a law in the Netherlands that now allows not only terminally ill patients but also depressed people to legally receive the fatal cocktail.
Steve explained that under California law, doctors may not legally list the cause of death as suicide when a patient has taken his or her own life. But the law “does allow a reference to the use of aid-in-dying meds as a contributing factor in the death, including the underlying fatal illness.” Steve, as a personal practice, does not include aid-in-dying medicines on the death certificate “to protect the patient from any backlash involving the choice of an induced death.”
Today Steve appreciates what he calls the “majesty and mystery” of death. Along with survivors, he participates in ancient rituals—“beautiful ceremonies” like washing and dressing the body—and finds it deeply humbling.
Steve is a spiritual man. He is influenced by the teachings of Jean Klein, a European who had an awakening in India. Although it is difficult to summarize Klein’s ideas, one important teaching is, “I am not identical with my thought process.” Steve believes that most of what one knows can be understood through other means, “coming from the heart and a sense of pure being.” This understanding has given him confidence to communicate with a dying person without words. “There is something in me that I know will make a difference. I am not anxious or worried, and am not in my head,” he explains.
About society’s recent openness to discussing death and dying, Steve cannot be more positive. It used to be, “If I don’t talk about it, it won’t happen.” The effect of the hospice movement has been to “lift the lid about frank, open discussions about death and dying. It helps people plan and frees them from living in a false reality, or a web of lies,” he says.
Naturally, one so intimate with death has opinions and thoughts about what awaits us all in the end. And what is the best death, to go quickly or to linger for a while? Not surprisingly, Steve believes that for himself, the ideal death would be when you know it is coming. “You get to finish your life, and say your goodbyes,” he says.
Steve also believes in a “continuity of consciousness.” This idea came to him intuitively years ago, after the death of his beloved dog, Misha, whose picture is prominently displayed on his office wall among other family photos. He tells this story, choking back tears.
“As I stood over the grave, I called out loud, ‘Where have you gone?’
A small voice inside asked, ‘Did you love me?’
‘Yes.’ ‘Do you still love me?’
‘Yes.’
‘Then that’s where I am.’”
Steve says, “My co-workers, patients and families living with the experience of dying have taught me much of what I know about love. Not the romantic love, of course, but something more encompassing, a feeling of compassion and connection with others that grows into this deep feeling of commonality and love.”
School of Public Health symposium explores how we approach dying so we can live richer lives
SPH symposium panelist George Annas, a William Fairfield Warren Distinguished Professor, suggested that that people should consider prioritizing quality of life over quantity of years lived.
By Jillian McKoy
From anti-aging beauty regimens to strict diets and medical screenings, Western culture places immense value on the quality and preservation of life. Death, however, is a subject largely absent from daily conversation, and when raised, it evokes fear and anxiety.
But talking about death—and the policies and attitudes that shape it—is a healthy practice, speakers at the School of Public Health Dean’s Symposium Death and Dying: A Population Health Perspective concluded Tuesday. More than 150 people attended the daylong event, which gathered authors, scholars, professors, physicians, storytellers, and public health experts for a frank conversation about an inevitable part of being human.
“The data is clear that 100 percent of us will die,” Sandro Galea, Robert A. Knox Professor and dean of the SPH, said at the start of the program, to the amusement of the audience. “And that’s okay,” he continued. “Our goal should be to think about how we approach death and dying at the population level, so we can live the healthiest, fullest, richest lives we can until such time.”
The notion of a good death—what it constitutes and if it even exists—was a central component of the day’s conversation.
“Death and dying is an issue that is characterized by a great disconnect between the universal experience we all share witnessing the deaths of our loved ones and a reluctance to discuss honestly and publicly the policies and attitudes that have gotten in the way of ensuring the good deaths that we all no doubt seek,” said Jon Sawyer, executive director of the Pulitzer Center, which cohosted the symposium, along with BU’s College of Communication, College of Arts & Sciences Center for the Humanities, and Program for Global Health Storytelling.
Sallie Tisdale, a nurse at Providence ElderPlace, pushed back against the concept of a good death. She said the National Academy of Sciences, Engineering, and Medicine definition of a good death—one that is “free from avoidable pain and suffering and in general accord with patients’ and families’ wishes”—is a fantasy.
“Death is a solitary experience,” Tisdale said. “How can we as a group decide what avoidable distress and suffering is? Only the person in the deathbed knows what that means.” Instead, there is such a thing as a “mastered death,” she said, where people are able to “express themselves as long as possible.”
Many of the speakers’ analyses were informed by personal experience. Michael Hebb, author and founder of the Death Over Dinner movement, described how his initiative was born from a communication breakdown within his family after the death of his father. Hebb was 13, and his family members, unable to talk about the devastating loss, ate meals alone and mourned in silence.
But repression creates the perfect environment for disease, he said, while talking about death “makes you funnier, improves intimate relationships, and increases your capacity to love.”
Death and Dying: A Population Health Perspective panelists Barbara Moran (COM’96), WBUR senior producing editor (from left); George Annas, a BU William Fairfield Warren Distinguished Professor; Tracy A. Balboni, Harvard Medical School; author and physician Samuel Harrington; journalist Christopher de Bellaigue; and Amy Appleford, a CAS associate professor of English.
Jamila Michener, a Cornell University assistant professor of government, recounted how her mother’s battle with stage 3 pancreatic cancer was initially misdiagnosed as acid reflux years prior by doctors in her low-income Queens neighborhood. The cancer wasn’t discovered until she saw a doctor in a predominantly white neighborhood in Ithaca. (Michener’s mother survived the cancer and is still living.)
“My brother jokes that she lived because she fled where black people were,” Michener said. “The experience of dying wasn’t something she wanted to do in her own neighborhood.”
Other speakers explored ways that people can exercise some control over their own dying.
“Spirituality is a primary strategy for integrating death into the human identity,” said Tracy Balboni, a Harvard Medical School associate professor of radiation oncology. Citing oncology studies conducted at four academic centers in Boston, Balboni explained that 78 percent of participating cancer patients said that religion was an important factor in dealing with their illness and that it provided coping skills and a way to understand their illness and their life.
“We need a creative reintegration of spirituality into medicine in order to care for dying patients well,” she said.
Another speaker, journalist Christopher de Bellaigue, discussed the practice of physician-assisted death in the Netherlands, dubbed the “euthanasia capital of the world.” The practice is now widely supported therecafter it was legalized in 2002 for patients experiencing “unbearable suffering with no prospect of improvement.”
De Ballaigue noted that the majority of the Dutch population opposed euthanasia when it was first enacted into law: “What interests me is where legislation leads to a change in dynamic in character and narrative, or the other way around. Public attitudes follow legislation.”
George Annas, a William Fairfield Warren Distinguished Professor and an SPH professor of health law, ethics, and human rights, challenged the American cultural approach that humans have to do everything they can to live as long as possible.
“Avoiding death is the goal of modern medicine,” said Annas, director of the Center for Health Law, Ethics & Human Rights, arguing that people should instead consider prioritizing quality of life over quantity of years lived. He suggested that it would be valuable to shift a portion of research funding into “things that make life worth living, such as decent housing and public transportation.
“There is such a thing as dying healthy, and it can be a worthy public health goal,” Annas noted.
Author Barbara Ehrenreich (Nickel and Dimed: On (Not) Getting By in America and Natural Causes: An Epidemic of Wellness, the Certainty of Dying, and Killing Ourselves to Live Longer) was scheduled to be a panelist, but was unable to attend. Sharon Begley, senior science writer at the Boston Globe publication STAT, a morning session moderator, read a portion of Ehrenreich’s prepared statement to the audience: “I’m 77 years old and I love cheeseburgers and Popeye’s Fried Chicken. I exercise when I feel like it, and I refuse to submit to medical tests and screenings recommended to all people over 50.”
This approach to her health, she explained, makes her an “outlier in our culture…where death is seen as some kind of failure.”
Panelists also discussed dealing with grief after a loved one dies, and the lack of resources available to properly treat mourning family members and friends. Katherine Keyes, a Columbia University Mailman School of Public Health associate professor of epidemiology and codirector of its Psychiatric Epidemiology Training Program, detailed how unexpected loss can lead to symptoms such as depression and to post-traumatic stress disorder.
“There’s something very specific to the loss experience itself,” said Keyes, who lost her ex-husband to suicide. “Losing someone close to us is very destabilizing.”
Afternoon session moderator Diane Gray, Acclivity Health Solutions chief innovation and advocacy officer and a board member of the Elisabeth Kübler-Ross Foundation, urged the audience to “become more engaged in the community of healing, empathetic, compassionate, caring individuals.
“There is no reason in our country for us to continue the legacy of shame and stigma that surrounds grief,” Gray said.
Alexis Flemming has dedicated herself to giving terminally ill animals the best last days of their lives – despite recently almost dying herself.
The animal lover, who lives with autoimmune diseases, was recently given only a few days to live before an operation helped control her condition.
Now recovering, she is back giving care to the variety of animals she has taken in at her animal hospice and sanctuary in Scotland.
She was inspired to set up the Maggie Flemming Animal Hospice in 2016 after her beloved bullmastiff Maggie died suddenly at the vets.
Alexis’s beloved bullmastiff Maggie died while away from her at the vets in 2016.
“Not being able to be with someone you love when they die can be quite traumatic,” she says.
As she walks through the sanctuary to the hospice, she knows every pig, sheep and chicken by name.
She wants all the animals to have a dignified end.
“They come here to spend however long they have left, a few days, a few weeks – sometimes even a few years – and I do end-of-life care to give them peace, comfort and friendship,” she says.
Alexis works hard to see which activities the animals enjoy most.
At the hospice, situated just outside Kirkcudbright in Dumfries and Galloway, Alexis makes a point of discovering what the animals like.
For some it’s sweets and reading. For her 19-year-old pal Bran, it’s adventures in the car.
“Bran was dumped on the street when he was about 17, he had a tumour on his spleen. Bran came to us with just six weeks to live and that was two and a half years ago,” she explains.
Bran is still going strong at 19, defying the terminal prediction of vets two years ago.
Bran is still going strong but Alexis admits her own health problems have made it harder to keep up with the care demands.
“It’s very hard to deal with that much grief. There was a time last year when I did 10 end-of-life cares in one month, that really took its toll. I was really ill at the end of that because my health isn’t very good anyway,” she says.
Inevitably her own recent doomed diagnosis – while thankfully avoided – has made her re-evaluate her life and work.
Bran enjoys a new lease of life, after being taken in by Alexis, that involves adventures out in the car.
“I almost died twice. Even if you think you’re the most life-grabbing, go-getting person, when you’re told you’ve only got a few days left and you survive that, every day is just… you make the most of it,” she says.
On dealing with the mortality of her farmyard friends, she says: “I know how I felt thinking it was almost my end and I know it’s almost their end so let’s just make the most of it, let’s not hang around and think of the sadness.”
She is now developing what is the first purpose-built animal hospice in the UK. She believes it could be one of the first of its kind in the world.
“We try to never turn anyone away if we can help it, but it’s very important to do end-of-life care properly, so we have very small numbers [and] we only do end-of-life for three animals at any time,” she says.
The passionate animals rights advocate believes “most animals in our society are denied a peaceful life and death”.
But she says she remains focused on helping the animals living out their final days in her care.
“Doing this kind of work you realise anything can happen at anytime and it could be today, it could be tomorrow, it could be a month from now, I just don’t know,” she says. “I try not to dwell on it too much.”
From DIY funeral services to death doulas, B.C. is on the leading edge of a trend that wants to make death a part of life, and a better experience for everyone. Meet the women leading the trend.
There may be no table more full of life than the corner booth at Paul’s Omelettery on Granville Street, where a group of women are talking over breakfast about death.
Three of the women are licensed funeral directors, two specialize in end-of-life planning, one is a celebrant, another an apprentice death doula — someone who assists families before and after death, the way a midwife does with a birth.
They call themselves the D’Posse.
The name is a playful nod to the word “death,” but their aim is thoughtful and resolute: to transform the way we commemorate and bury our dead, to bring death back to life.
Glenn Hodges, manager of Vancouver’s Mountain View Cemetery, has dubbed them “the disruptors” — part of what he says is a growing number of end-of-life workers, many of them women, who are quietly, respectfully, and often joyfully, working to take death out of the hands of the corporate monopolies, and give it back to families.
Although many funeral homes in B.C. still bear the names of the families that originally established them, many of these are owned by Service Corporation International, a conglomerate headquartered in Texas. SCI owns 45 funeral homes in B.C., about a third of the funeral service providers in the province. (SCI, which trades on the New York Stock Exchange, has repeatedly tangled with consumer advocates over everything from its pricing to sales techniques.)
Funeral director Ngaio Davis spent 20 years working for a number of providers in the corporate funeral industry before breaking away to start Koru Cremation, Burial and Ceremony (korucremation.com), which she runs out of a cheerful space on Kent Avenue in Vancouver.
Like the other women at this monthly breakfast, Davis says she was drawn to the funeral industry because she wanted meaningful work. “I wanted to do something that felt worthwhile,” says Davis.
Coming face to face with death never made Davis uneasy — but the funeral industry did.
“There are a lot of wonderful, compassionate people in the corporate funeral homes,” says Davis. What bothered her, she says, was the focus on profit: “What’s the bottom line?”
Davis says one funeral home she worked for stipulated that commissioned sales staff be in every meeting with grief-stricken clients to have the “face time” to push extras. At another job interview, she was grilled on what her average sales “per call” were — this was not the work she wanted to be doing.
Lisa Hartley is a ‘celebrant’ who officiates at weddings as well as funerals.
‘What can I help you do?’
Despite decades of scrutiny, the North American funeral industry has changed little since Jessica Mitford’s 1963 expose, The American Way of Death, in which she called the funeral industry a “huge, macabre, and expensive practical joke on the American public.”
A big part of that macabre joke is the cost.
The average traditional funeral in Canada costs $10,000, according to Stephen Garrett of the Memorial Society of B.C., and GoFundMe counts funerals among its fastest-growing fundraising categories.
“From a basic cremation at about $1,200, costs range up to $15,000 or $20,000 — which is fine if it’s in line with your budget. But that’s where we get into problems with funeral homes pushing that on people,” said Garrett.
In addition to basics, such as registration of death, transportation, sheltering and disposition of the remains, costs — and funeral home profits — skyrocket once the bells and whistles are added: the expensive casket, which may be incinerated days later, embalming (not a legal necessity in B.C.), makeup, hairdressing, flowers, grief counselling, memorial, and follow-up house calls to sell products, such as future burial services, to survivors.
Five years ago, Davis decided to do something different.
Davis says her approach to death is informed by her Maori heritage. “Maori practices around death and dying are very strong. You are with your dead. You don’t just let them be taken away and be controlled by others. The family is the one who is crafting and planning what happens, and what will be the final ceremony.”
At Koru, the reception room is simply decorated with none of the trappings of a traditional funeral home: no sombre music, heavy curtains, or staff in dark suits.
Clients can plan as elaborate or as simple a funeral, ceremony and cremation or burial as they wish. Koru also specializes in green burials — biodegradable casket or a simple shroud, and no embalming — and will facilitate DIY, family-led or “home funerals.”
“This week, I’m looking after a family that wants to take their father and husband back home to his condo in North Vancouver. They want to have him there, they want to give him a sponge bath, dress him, and let him spend his last night there with his wife,” Davis explains.
Davis will transport the man and bring a special table so he can be laid out in his own home. “We will move him onto the table so it’s more comfortable for them to bathe him and dress him,” said Davis.
The next day, Davis will return with the casket, which will be placed in the condo’s common room because it won’t fit in the elevator.
“They are lining the casket with sheep wool that one of the kids brought from Scotland, and then we will go to the cemetery,” said Davis.
“His wife knows what she wants. They’ve been married for 60-plus years — they want those last moments together.”
At Paul’s Omelettery, over the warm clatter of breakfast dishes, cups and spoons, Lisa Hartley, a celebrant who officiates at weddings as well as funerals, recalls meeting Davis when her father-in-law died unexpectedly in his West End apartment.
His death had come quickly and the family was unprepared.
“We didn’t know what to do. Someone said, ‘Call Ngaio,’” says Hartley. “Her first question to us was, ‘What can I help you do?’”
They didn’t have to go to a funeral home, something Hartley was uncomfortable with.
“Ngaio came over to the apartment, and sat on the sunny balcony with her checklist, and we went through all the options.”
The family chose to keep Hartley’s father-in-law at home for a short period, and her husband decided he wanted to participate in the washing of his father’s body. “I never expected him to do something like that,” says Hartley. “But it really helped him.”
While the family gathered in the apartment, Davis completed the preparations.
“When she had him ready, she wrapped his body in a beautiful red velvet cloth, but she came to us first and said, ‘Peter is ready to go now.’”
Hartley was deeply moved by the experience, and now works closely with Davis and other alternative providers as a funeral celebrant. “My special interest is in sustainability in death care,” says Hartley. That means being more hands-on, in DIY and home funerals.
Hartley’s ceremony design process includes in-depth meetings with the client and family and friends to talk about the person. “It’s quite beautiful, and it’s often the start of the healing process. People get to tell stories about the person that has died. I recently had one person who said, ‘I feel better already,’” says Hartley.
Jennifer Mallmes is a death doula who founded the End-of-Life Doula program at Douglas College.
When death is expected, a death doula can help the family prepare for what Jennifer Mallmes, founder of the End-of-Life Doula program at Douglas College, calls “a gold-star death.”
“Planning really does help with the death and bereavement process, even when people don’t want to die,” said Mallmes. “Barring sudden or unexpected deaths, you can have some choice in how you go. Who do you want around? Who do you not want around?”
A death doula will help individuals and families faced with an illness or a diagnosis that a death is coming plan home care or hospice care, work with funeral services. They can also help with making what life is left fulfilling: “We can help with a life review, ask what are the things I still want to do? We might look at services to help them accomplish those things.”
Death isn’t just a business, it’s a way of life
Garrett said that although the funeral business is slow to change, Baby Boomers are pushing the trend toward the “reclamation” of death and dying.
“The Boomers demographic changed the world they lived in — they questioned authority, lived through the Summer of Love, built the environmental movement,” says Garrett. “We’re on our way out, and that’s going to change things, if only because of the large numbers.”
About 34,000 to 35,000 people a year die in B.C. “That death rate in the next 10 to 12 years is going to head north of 45,000,” says Garrett. “We’ve got 916,000 Baby Boomers living in British Columbia with only one way off the planet.”
Glen Hodges is the manager at Mountain View Cemetery in Vancouver.
Although Statistics Canada doesn’t keep numbers on the kinds of funerals people hold, Glen Hodges says he has seen changes in people’s attitude toward death. Part of that has been the renaissance of the city’s only cemetery.
Mountain View shut down briefly after running out of grave space in 1986, but a new master plan created more space. Mountain View built columbaria (condos for cremains) to house niches for cremated remains, and reclaimed unused graves from families — a complex and provincially regulated process that applied to plots purchased at least 50 years ago and never used by family members in that time.
Hodges says the city has also been working to re-establish the cemetery as a place for the living.
“A cemetery is not just a utilitarian place for disposal of the dead and keeping of public records,” said Hodges. “(It is also) a sacred place to remember and commemorate, and it has a larger role within the community.”
That includes family oriented community events, such as its annual All Souls Night, which draws up to 2,000 people.
“We invite people to wander into the cemetery to light candles and leave mementos for their loved ones and be in a contemplative atmosphere filled with candles and music and in a place that is safe for them to speak of the dead and talk with others.”
Mountain View doesn’t require grave liners, so green burials are possible, as well as reburials, an option that allows families to open the grave and reposition any remains still there so a new casket can be added.
Hodges regularly hosts free workshops hosted by D’Posse members Reena Lazar and Michelle Pante of Willow EOL (end of life).
The workshops, says Pante, are designed to help people figure out how embracing their mortality can change the way they live. “Our lives are limited, they are precious and finite, so we ask how does that fact affect how we live?” said Lazar.
The workshops help people explore their thoughts and feelings about death and guide them through the process of creating what Pante calls “heart wills,” or love letters for the family and friends who will survive them.
Their clientele ranges through all age groups, says Pante, although many are healthy and in the Boomer demographic.
Boomers may be fuelling the trend toward a more compassionate, affordable, personalized experience after their final exits, but for Davis and her growing network, death isn’t just a business — it’s a way of life.
Many find their way to Koru after a negative experience elsewhere, says Davis — whether it was sales pressure that shamed them into overspending, a service that didn’t reflect their loved one’s personality, or a makeup job that made them look like a stranger.
“Here was this very important moment in their lives, and they were robbed of it. It could be a special time, or it could be something you never want to go through again. So I’m just doing my little bit to change that.”
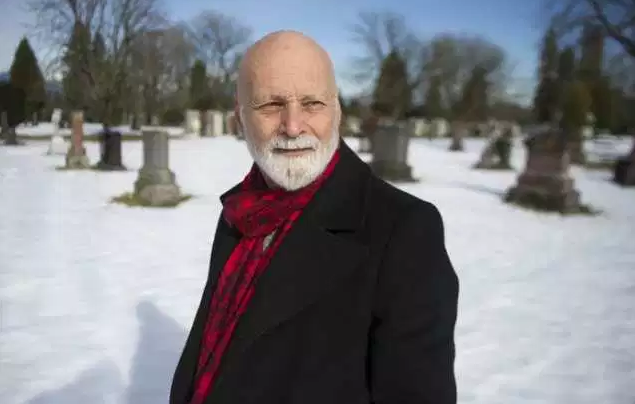
Stephen Garrett, seen here at Mountain View Cemetery in Vancouver, is the executive-director of the Memorial Society of British Columbia.
The Planner
Stephen Garrett, executive director of the Memorial Society of B.C., a non-profit society serving 240,000 members, believes that much of the expense and discomfort families inherit when a loved one dies can be avoided with good planning. To help people making final arrangements, Garrett has designed the “All Ready To Go Binder” to help with the death planning process.
“When my sons were 21 and 23, I invited them over for beer and pizza. I had the death binder in the middle of the table,” said Garrett. “They were a bit shocked — they didn’t want to think about me being dead and I didn’t want to think about it either — but as a responsible parent, this was my gift to them.”
The mood changed as he went through his wishes and let them know that he would be throwing in a family holiday: an all-expenses-paid trip to India, where he wants his ashes to be sprinkled in the Ganges River. Making a plan that’s personal, that includes opportunity for meaning, is part of what can make the process fun, said Garrett.
The binder is available on the society’s website for a nominal fee, and Garrett would like to see every family in B.C. have one.
The All Ready to Go Binder is a place for everything from your last will and testament, to advanced care directives, funeral arrangement forms, and other details such as people to call, copies of personal identification, and celebration-of-life plans.
The purpose of the Memorial Society is to help families prepare for and plan affordable services by partnering with ethical providers. The Memorial Society of B.C. offers lifetime membership for a one-time $50 fee. Members receive discounted prices of 15 to 30 per cent with participating funeral providers and access to support, advocacy and planning.
By The Numbers
$7,181: Average Cost of a traditional funeral (includes viewing, burial, embalming, transport of body)
28.6%: Percentage increase in average traditional funeral costs between 2004-2014
87%: Percentage increase in average traditional funeral costs between 1980-1989