‘Diagnosing death’ would prevent unnecessary distress at the end of life.
Doctors need to be trained in the art of “diagnosing” death to prevent unnecessary distress at the end of life, an expert has claimed.
Dr Erna Haraldsdottir, a senior lecturer at Queen Margaret’s University, in Musselburgh, called for a shake-up of thinking on medical intervention for the dying after watching her elderly father-in-law die in hospital.
The 84-year-old had been diagnosed with dementia five years beforehand and his family watched his gradual decline until he was admitted to hospital. Although he was elderly and very frail, doctors attempted to discharge him at one point and tried to resuscitate him as a “do not resuscitate” note had not been arranged.
Doctors were also reluctant to issue a death certificate as they were unsure of his cause of death.
Writing in the European Journal of Palliative Care, Dr Haraldsdottir said doctors need to change their mindsets over when patients need medical intervention and try to “diagnose” death.
Dr Haraldsdottir, who also leads a pioneering research programme at St Columba’s Hospice in Edinburgh, said: “In my own experience, our family believed my father-in-law had a good death, however what was noticeable was the staff’s lack of insight into the situation and understanding of what was happening.
“This caused the family unnecessary upset and distress – which could have been avoided if the medical team had applied the principles of palliative care to the assessment and care.”
Ministers unveiled a five-year plan to put palliative care at the heart of the NHS in December and to ensure a greater openness around death and dying.
It comes after a Glasgow researchers found falling numbers of Scots were dying at home, despite many saying it was what they wanted.
It is more important than ever for hospices to be leading the way when it comes to developing care around death and dying, said Dr Duncan Brown, medical director at St Columba’s Hospice.
I’ve been with the dying many times, both in a personal capacity and as a health care professional. As an end-of-life doula my work is centred around supporting people and their families at end of life. My experiences have led me to agree wholeheartedly with the BMA in its recent report: hospitals are not the best place to die.
An overwhelming majority of us want to die at home, yet statistics show the reality is that 54% of us will die in hospital. But in my opinion, hospices are for the dying. Home is for the dying. Hospitals are not. The raison d’etre of end of life care is to help people experience a ‘good death’. We will remember how someone we love dies forever. The impact of a bad death is far-reaching. Candy Chang, creator of the ‘Before I Die‘ wall, a global art project that invites people to reflect on their lives and share their personal aspirations on a public wall, describes the fallout as creating ‘circles of mayhem’ for generations.
What is a good death?
Every person will have a different idea about what would constitute a good death for themselves or their family. Much of the debate over end-of-life care comes down to two questions:
Is a good death one where the medical team did everything to save a life?
Is this still true if there is little chance or no of a happy outcome?
Culturally, we have always seen a good death as one we have ‘fought’ against. It may be time to consider otherwise. Many treatments are aggressive and futile, robbing the last remaining quality of life a patient has.
Perhaps a good death is the accepted one. One where the dying person is in control, can be at home, can have their pain and symptoms managed. End of life care must be entirely individualised and person-centred, only then can we begin to offer the excellent end of life care that everyone deserves.
The refusal of a medical team to end active treatment to the detriment of the patient was exemplified in the death of a very close friend of mine. They threw everything they had at giving him longer than his twenty-something years. They didn’t give up ‘actively’ treating him until the end. He died clinging to the belief that he was going to live. That last precious year of his life was a tragic mess of chemotherapy, life-prolonging operations and colourless hospital wards. The treatment had destroyed the very essence of who he was, long before his heart played out its final beats.
I believe if we discussed end of life issues regularly, we wouldn’t find them so tricky to broach. Issues about death and dying should be taught in schools as part of the PSHE syllabus from primary and onwards. During Year 13 tutor time when we teach young adults to fill in job application forms, we should also be filling in advance directives with them.
Issues with control at the end
In a study by the Economist Intelligence Unit, the UK was crowned the best in the world for provision of end-of-life care. The author of the report, however, said that there is room for improvement, especially in symptom control and communication. Could this improvement be guided not by government policy or hospital administration, but by changing the way we look at death?
The recent BMA report concluded that some doctors continue to treat the dying when active treatment is no longer of any benefit. One reason it suggested was because of pressure from the patient and their loved ones. This is understandable – it is often too difficult to let go of the ones we love. The report also stated it is because if doctors acknowledge there’s nothing more that can be done, that they’re admitting defeat.
I knew a woman worked with the dying so when she was dying, although she knew there was nothing that could be done, she didn’t want to die. She wasn’t ready: she had a life to lead, a world to see and children to watch grow and guide. She was looked after by the same medical team she had worked alongside for many years. They couldn’t let her die either. If they let her die, they would have failed one of their own. They had to try, even though they knew it was futile. They couldn’t give up, even though they knew the treatment she would most likely shorten her life, not extend it. Her original prognosis with palliative care had given her up to a year. She died two weeks into aggressive treatment, four weeks after her initial diagnosis.
We should not see the death of a dying patient as a failure. Death is not the loss of a battle. Death is a natural part of life. If we could see it that way, we might be able to approach it differently. Our goal should be helping someone live as good a life as possible right up until the very end. No one will ever experience a “good death” if our focus is active treatment at all costs.
The report set out that treatment at end-of-life should be ‘appropriate and proportionate’. Dying with care, deference and dignity, and on our own terms is the very least we should be able to offer. A lady I worked with lived an incredibly full life: alone and happy. She went dancing and played snooker. She cooked everything from scratch everyday. Her breathlessness became untenable and she finally went to the doctor. She had cancer, which was slow to progress even though she chose a palliative care pathway. She accepted her life-limiting prognosis with the wisdom of one who knew herself well and contemplated mortality more often than many. She died in a hospice, surrounded by her family. Hers was a peaceful death. Peaceful and on her own terms.
One aspect of the report that I feel most strongly about is that doctors should be receiving training and CPD on communication and how best to have difficult conversations. One junior doctor who was interviewed for the report said: “I found it very difficult to talk to patients about dying, prior to working in a hospice, because…as a junior doctor we’re not taught very much…”
A shift in thinking
We all have to take responsibility for communication and the decisions we make. It’s terribly difficult when we’re unwell and vulnerable to hear these truths. If we’ve never considered end-of-life until our own life’s end it’s no wonder we find it so hard. If we discussed these issues regularly we wouldn’t find them so hard. We need to break down the ingrained cultural barriers that prevent us from talking about death and dying
Let’s all take on that responsibility. Let’s talk about it: openly and without fear. It’s too much to have that conversation for the first time when we are facing death. It’s much easier to talk about it while we’re living a healthy life.
We need to ask ourselves what is a good death for us.
Why do we value quantity over quality of time? Why do we cling so dearly to the notion that a life well lived is the longest? Sometimes doing nothing is the most courageous path. Sometimes accepting there’s nothing left that can be done is the bravest choice. Some may describe such a decision as “giving up”. Pursuing treatment until the very end, on the other hand, is lauded as “being a fighter”.
Do these words,”battle” and “fight”, compound medical teams’ feelings of failure when an unavoidable and imminent death is in front of them? Changing our language may help us to change the way we think. Illness and death are a part of life. Loss is not a failure: not ours, and not our doctors’. Perhaps redesigning our expectations and language at end of life could begin with Paul Kalanithi’s beautiful words:“The physician’s duty is not to stave off death or return patients to their old lives, but to take into our arms a patient and family whose lives have disintegrated and work until they can stand back up and face, and make sense of, their own existence.” If they did, I believe death and dying could be a richer and better experience for everyone involved.
Children’s book author and illustrator Maurice Sendak, who died in 2012, spent much of his life obsessed with death. In 2011 he told Fresh Air’s Terry Gross: “There are so many beautiful things in the world which I will have to leave when I die, but I’m ready, I’m ready, I’m ready.”
Katie Roiphe’s preoccupation with death goes back to her childhood, when she contracted virulent pneumonia at the age of 12. She was sick for a year and thought she was going to die.
Her terror of death was reignited many years later when her father died. It was then that Riophe found herself turning to great minds to see how they confronted mortality.
She initially told herself that she wanted to “understand it better,” she tells NPR’s Melissa Block, but she soon realized that was a lie. “I was actually trying to see it,” she explains. “It sounds really simple, but it’s actually a very difficult thing to do. So that was my goal, to sort of focus in really closely on the final days of these writers and thinkers, and just look.”
In The Violet Hour, Roiphe describes the last days of Sigmund Freud, James Salter, Maurice Sendak, Susan Sontag, John Updike and Dylan Thomas. She talks with Block about how these writers and thinkers accepted, or railed against, their fate.
Interview Highlights
On John Updike, who wrote poems in the hospital after being diagnosed with lung cancer
It was amazing. He had very little time — just weeks before he was dead. I actually went up and looked at the manuscripts and you can see in his handwriting how arduous it was. At that last moment, when most people would just be watching television or railing against the universe, that was what he did and I found it very moving. …
The poems have a sort of quality of reporting — that he’s bringing news. And he talks about writing as turning pain into honey, which I find a really beautiful way to think about what writers do: taking this incredibly awful — maybe the most awful thing that can happen to you — and turning it into honey just with words.
On Susan Sontag, who endured brutal treatments for cancer
She had written so eloquently about the importance of not turning illness into a metaphor — of not embellishing and fantasizing and being really realistic and rational when it comes to your own illness — and she was unable to do that ironically in her own life. …
She thought to herself she would be the exception even to the rule of mortality. That somehow, as she had with her earlier cancers famously, she was going to defeat death in some way. And even though the odds were against her — she was 71-years-old getting a bone marrow transplant — even in those situations, she felt this time she wouldn’t die.
At the one hand, it’s the opposite of a good death, it’s almost the anatomy of how you don’t want to die. On the other hand, I did see something kind of heroic in the power and force of her will.
On how mortality was a constant companion for writer and illustrator Maurice Sendak
He was certainly preoccupied with death for his entire life, and one of the things that fascinated me about him is the way, in his art and famous children’s books, he worked on this problem year after year. Like when his parents died, or when his brother died, he just kept working on this problem and worked it through in drawing after drawing and draft after draft. And he sort of came out freeing himself to a certain extent from this obsession. He was very depressed at certain points of his life and he used his art as a way of countering that. It was a sort of medication for that almost.
On Sendak owning John Keats’ death mask
It’s really very beautiful. When I saw it — he has it in a guest room with a blue bedspread — there are kind of stuffed animals on the bed. It’s a very bizarre scene and very Sendak, and I thought to myself, “Who would ever want to own Keats’s death mask?”
And then I looked at it and I realized I knew exactly why you’d want to own Keats’ desk mask: Because in a way what I was doing in this book was writing death masks. That urge to preserve the moment, and Annie Leibovitz did it with her famous photographs of Sontag, and Sendak himself drew the people he loved: his partner of many, many years after he died, and his family members right before they died.
There’s something about capturing that moment in art that I actually do completely understand — both the reason you’d make Keats’ death mask and the reason you’d want to own it.
On her idea of what a “good” death would be
I feel like the thing that mostly happened with this book is I came away marginally less afraid, which sounds like not that a big deal. But given my panic about death at various points in my life, [this] was liberating to me. In terms of a good death, I did feel that this prolonged medical struggle of a Susan Sontag where you’re chasing after any possibility of medical salvation seemed like not a good idea, and the way of working your way into accepting what’s happening the way Sendak did and the way Updike did seems preferable to me.
But one doesn’t always have control, and that was one of the things I really realized in writing about these deaths.
Now I measure time in distinct chunks, focusing on events – a holiday or a party. Although it has been an intense few months, I’ve tried not to dwell on it
By Max Edwards
Max Edwards, summer 2015.
Five months ago, I was diagnosed with terminal cancer aged 16. It was rather as I’d pictured GCSE results day to be: a lot of stress waiting for potentially awful results, although, as it happened, GCSE results day was a pleasant surprise. But, like many whose grades came as a disappointment, I got over it soon enough. I think it’s surprisingly easy to adapt to this kind of news. After all, while I’m not going to deny its personal significance, it doesn’t really change anything important.
In the past, I have imagined terminal illness as the short and depressing period before a person’s premature death, but it somehow doesn’t feel nearly as dramatic or upsetting. I don’t feel as though normal life has ceased, or that my perception of it has changed drastically. In fact, if it weren’t for my loss of mobility following an operation, my life would have probably settled back to normal long before now. The assumed tide of unimaginable suffering that rests hand in hand with these kinds of situations is rather less dramatic in reality.
Being told you are going to die is a shock, but I was largely over it in a week, and as for breaking the news to friends and family around me, the guesswork on my part of trying to assess the other person’s emotional fragility, their guesswork at trying to assess mine, and the background danger – perhaps felt by both of us – that your partner in conversation is about to break down in tears, made the experience not so much sad as really quite awkward.
This isn’t to say that it hasn’t been an intense few months, but I can’t say that this experience has truly changed me as a person. People have told me how well I’m coping and how they couldn’t have done the same in this situation, as though I’ve faced an unimaginably horrendous set of circumstances and managed to do the impossible (remain positive), but I don’t see it that way.
While I understand why it may feel like that to those looking in from the outside, dying of cancer, in my experience, has been a succession of hospital visits, a lot of pills, and one or two pieces of bad news. But after that, there is an inevitable return to the way you were previously living. Pretty soon I came to realise that it doesn’t make any difference if you’ll be dead in 10 years or two months; you still get up, have a shower and make a cup of tea.
OK, so there are drawbacks – in my case, largely a lack of movement. After the operation on my spine, I was all but paralysed in my dominant hand, movement was compromised in the other and I could barely move my legs, all of which meant I could no longer write, walk, or play the guitar and clarinet. These limitations didn’t seem to matter when I was still in hospital, but as I left bed eight, ward 27 and returned home, I was confronted by all I could no longer do. At first, when the seriousness of my illness was still a new and shocking discovery, the issue of not being able to walk to the toilet seemed dwarfed by this drama, and it was only later that these kinds of problems started to irk me.
Nonetheless, I’ve found that these problems start to sort themselves after a while. For example, I was at first stretchered around the hospital. As my mobility improved, I spent more time in a wheelchair, which at least gave me the luxury of seeing where I was going. Currently, I walk with a stick, which of course resolves many difficulties, and I can now eat at a restaurant without having to sit half a mile from the table because the wheelchair won’t fit underneath.
Where there hasn’t been a significant improvement, such as in my right hand, I’ve tried to make up for the problem. Unable to play any instruments that require two hands, I’ve begun learning the blues harmonica (which only requires one – at least it does the way I play it) and, while practising writing left-handed, I now type on a touchscreen phone, this being how I continued to write my weekly blog and my recently published book. In addition to this, I’ve continued to write songs and music by composing on the computer. I suppose I can at least be glad to live in an era when technology makes this possible.
Religion has featured a lot in discussions since the diagnosis. I am told that many people are praying for me and I have prayed myself, though I never thought it would make a difference (I only did it on the off chance that something positive might happen – what’s to lose?). I don’t believe in God; I didn’t before my diagnosis and I don’t now. I can see how some in my position may want to turn to religion as a comfort, and I can also see how many may become disillusioned or even angry with the God they thought they believed in. But I have done neither. Most of my frustration has fallen on nurses and medical staff for the most trivial of reasons.
Max Edwards with his sister Esme, 14, and brother Toby, seven, decorating the Christmas tree, 2015.
As for comfort, I don’t feel I need comforting. The initial shock wears off very quickly, and after that, life seems to become quite ordinary. The satisfaction of daily routines is enough in the way of comfort.
One thing I have started to do is measure time in distinct chunks. Ordinarily, I would allow days to blur into weeks, weeks into months and months into years. After my operation, however, I’ve found myself focusing on certain events. A holiday, for example, or a day trip, or a party. Perhaps my perception of time has changed, or maybe it comes from a lack of ways to fill the day, although that’s becoming less of a problem now that I’m more mobile and have been able to get more done, such as schoolwork (AS-level history), which I’ve just restarted.
In terms of where I want to be, my main hopes for the future are life-expectancy-related. This is one thing that still gets to me: I’ve more or less made peace with the idea of death, but it’s the question of when that is still a daunting thought. The (almost) inevitable growth of my cancer means it is likely to come some time soon, but I still don’t know when exactly, and I’m not sure I want to.
Regular MRI scans will probably give me an indication of how bad the situation is as and when that becomes the case, which means there is more bad news in store for me. I considered not having any further scans, but then I’m sure I’d panic with every slight pain or possible symptom of tumour growth, and given that I already interpret a headache as, “OH MY GOD, IT’S SPREAD TO THE BRAIN AND I’LL BE DEAD WITHIN A WEEK!”, I’d rather not venture any further down this route.
I am sure the expectation of death is worse than death itself. True, they say death is the worst single thing that can happen to you, and given that I can’t trick myself into believing there is an afterlife, I imagine it leads only to an empty void, but I’ve found ways to accept such an idea. First, I look on my life, which I believe has been a modest success, and remember that it could not have occurred in any other way. The only possible way I could have had my unique set of experiences is by living my life as it is, and that means dying when I die. Even if I’m wrong, and there has been more unhappiness than I care to remember (rendering my life “unsuccessful”), death – the absence of pain or pleasure – should then logically be seen as an improvement.
I also remind myself that the experience of dying is not unique to me. Whether it happens aged 16 or 95, experiencing the end of everything you know is the same process – it’s just that I and those around me are forced to come to terms with this fact prematurely.
Finally, I feel it has helped to process the whole issue selflessly. Some people might find it helpful to know that they are loved, that people care about them and that they won’t be forgotten when they die. I can understand this and I see how it’s comforting, but I also find it consoling to take the opposing view: stop dwelling on personal suffering and carry on as before.
This approach seems to help deflate the hype that terminal diagnoses carry. Pity, grief and sympathy are all natural emotions, and they certainly have their place, but I’ve found the message of “Stop whining and get on with it” far more effective. Stoicism, I feel, is more effective than grief: a simple reality-check helps to set my perspectives in place.
It helps to remind myself that even if I’m dying, it’s not all about me. At the end of the day I’m one in seven billion, a number that – like my cancer – will continue to grow and multiply over the coming months and years. While my life may be all I know, I’m nothing more than a dot on this planet. When you take into account the dozens of people I know, the billions I don’t, the thousands of miles that separate us, and the ever running river of time on which we all finitely float, you may come to the inevitable and strangely comforting realisation that we are all going to die: me, you and everyone else. Get over it.
Claudia Biçen, an artist based in San Francisco and London, spent the past two years interviewing and sketching hospice patients. She was convinced, she said, that dying people could help answer the question of how to live.
The result is a new multimedia exhibit, “Thoughts in Passing,” featuring nine sketched portraits and brief audio narratives in which the patients reflect not only on what it’s like to be dying, but on the lives they led.
The exhibit, completed in recent weeks and which will be shown in San Francisco, has already generated a passionate response. It is likely to be shown in other cities, and can also be seen online.
“Doing this felt like shining a light into this very dark, scary area for me and I’m sure for lots of people,” Biçen said in an interview. “It’s made me feel in my life more. I’m more in each moment.”
Born 30 years ago in London to a mother who brought home orphaned kittens and puppies for foster care, Biçen often held the animals as they died, and she grew accustomed to “the idea of death being close by.”
She earned degrees in psychology, philosophy, and anthropology before romance brought her to San Francisco, where she sketched portraits of family members. The work earned the attention of local galleries, but failed to deliver lasting satisfaction. Deeper wisdom, she thought, might be found in subjects facing death.
Biçen asked Bay Area hospices to find patients to sit for portraits and reflect on life and death, and in 2014 the first candidates emerged. She met several times with each, posing the question: What does it feel like to be dying? They had never been asked the question, they told her, and they had much to say.
She retreated to a studio, where she surrounded herself with photographs of her subjects and audio recordings from their meetings. Just 400 words would make the final audio cut. In the portraits, she would embed words taken from fragments of their conversations.
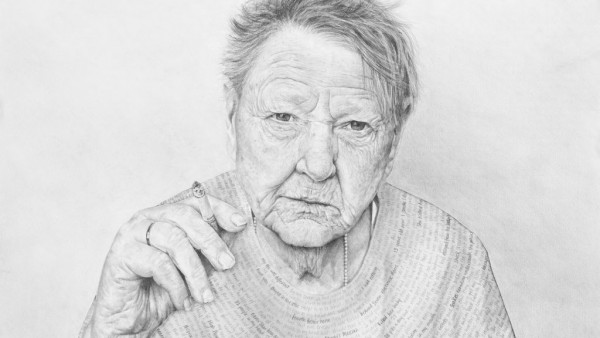
One subject, Jenny, is an artist herself. Written on her blouse are allusions to time spent locked in a mental institution with the criminally insane. In her audio recording, she tells of a childhood of being kept in an attic by foster parents, the terror of shock therapy, her later discovery of art, and the peace she found in it.
“I wonder about people who never ever know high peace,” Jenny says. “And I felt lucky that I knew. Little old nobody me could get high peace.”
Biçen’s pencil sketch of Jenny will hang in the Smithsonian’s National Portrait Gallery starting March 12 — a significant achievement for an artistic project, but one that doesn’t in itself speak to Biçen’s more spiritual achievements.
Experiencing her exhibit, even online, is like stumbling onto an exquisite, futuristic cemetery: portraits that capture the subjects’ essence; spoken words that distill their feelings on life and death; written words that hint at experiences that shaped them.
On screen, the portraits fade to black before their voices go silent, leaving viewers to confront their own reflection on the screen as patients offer their final thoughts.
The exhibit begs the question: How will you be when the time comes?
A nurse in end-of-life care shares the most common regrets of the dying
When you are on your deathbed, what others think of you is a long way from your mind.
For many years I worked in palliative care. My patients were those who had gone home to die. Some incredibly special times were shared. I was with them for the last three to twelve weeks of their lives.
People grow a lot when they are faced with their own mortality. I learned to never to underestimate someone’s capacity for growth. Some changes were phenomenal. Each experienced a variety of emotions, as expected, denial, fear, anger, remorse, more denial and eventually acceptance. Every single patient found their peace before they departed though, every one of them.
People grow a lot when they are faced with their own mortality
When questioned about any regrets they had or anything they would do differently, common themes surfaced again and again. Here are the most common five:
1. I wish I’d had the courage to live a life true to myself, not the life others expected of me.
This was the most common regret of all. When people realize that their life is almost over and look back clearly on it, it is easy to see how many dreams have gone unfulfilled. Most people had not honoured even a half of their dreams and had to die knowing that it was due to choices they had made, or not made.
It is very important to try and honour at least some of your dreams along the way. From the moment that you lose your health, it is too late. Health brings a freedom very few realize, until they no longer have it.
2. I wish I didn’t work so hard.
This came from every male patient that I nursed. They missed their children’s youth and their partner’s companionship. Women also spoke of this regret. But as most were from an older generation, many of the female patients had not been breadwinners. All of the men I nursed deeply regretted spending so much of their lives on the treadmill of a work existence.
By simplifying your lifestyle and making conscious choices along the way, it is possible to not need the income that you think you do. And by creating more space in your life, you become happier and more open to new opportunities, ones more suited to your new lifestyle.
We often regret the things we didn’t say
3. I wish I’d had the courage to express my feelings.
Many people suppressed their feelings in order to keep peace with others. As a result, they settled for a mediocre existence and never became who they were truly capable of becoming. Many developed illnesses relating to the bitterness and resentment they carried as a result.
We cannot control the reactions of others. However, although people may initially react when you change the way you are by speaking honestly, in the end it raises the relationship to a whole new and healthier level. Either that or it releases the unhealthy relationship from your life. Either way, you win.
4. I wish I had stayed in touch with my friends.
Often they would not truly realize the full benefits of old friends until their dying weeks and it was not always possible to track them down. Many had become so caught up in their own lives that they had let golden friendships slip by over the years. There were many deep regrets about not giving friendships the time and effort that they deserved. Everyone misses their friends when they are dying.
It is common for anyone in a busy lifestyle to let friendships slip. But when you are faced with your approaching death, the physical details of life fall away. People do want to get their financial affairs in order if possible. But it is not money or status that holds the true importance for them. They want to get things in order more for the benefit of those they love. Usually though, they are too ill and weary to ever manage this task. It all comes down to love and relationships in the end. That is all that remains in the final weeks, love and relationships.
Many don’t realize til the end that happiness is a choice
5. I wish that I had let myself be happier.
This is a surprisingly common one. Many did not realise until the end that happiness is a choice. They had stayed stuck in old patterns and habits. The so-called ‘comfort’ of familiarity overflowed into their emotions, as well as their physical lives. Fear of change had them pretending to others, and to their selves, that they were content. When deep within, they longed to laugh properly and have silliness in their life again.
When you are on your deathbed, what others think of you is a long way from your mind. How wonderful to be able to let go and smile again, long before you are dying.
Life is a choice. It is YOUR life. Choose consciously, choose wisely, choose honestly. Choose happiness.