The right reader of a good poem can tell the moment it strikes him that he has taken a mortal wound — that he will never get over it.
-Robert Frost
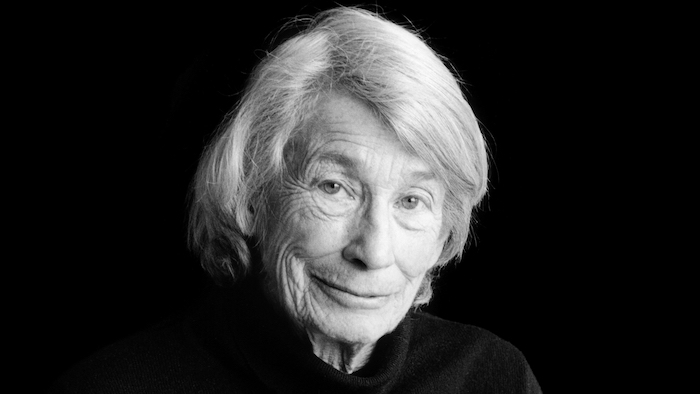
Mary Oliver has received many honors for her poetry, including the Pulitzer Prize and The National Book Award
By Ken Trainor
There should be a national day of mourning when our best and most loved poets die. But most of those poets probably wouldn’t want that. Mary Oliver, who died on Jan. 17, was one of them. But she would probably approve of a national day of reading poetry in her honor, so let’s make that day today.
Oliver never took life for granted. She celebrated the daily discipline of paying attention to the world around us, which is essential to conscious living.
For our national day of reading Mary Oliver, I’ve collected some of my favorite passages.
I dedicate them to Joanne Cella-Easton, friend and kindred spirit, who died much too young on Jan. 9.
I go down to the shore in the morning / and depending on the hour the waves / are rolling in or moving out, / and I say, oh, I am miserable, / what shall — / what shall I do? And the sea says / in its lovely voice: / Excuse me, I have work to do.
“I Go Down to the Shore” A Thousand Mornings
Mary Oliver was very good at asking challenging questions in her poems, such as this one from “Have You Ever Tried to Enter the Long Black Branches?”
Listen, are you breathing just a little, and calling it a life?
One of her most popular poems focuses on discerning where we stand in relation to the world:
Whoever you are, no matter how lonely, / the world offers itself to your imagination, / calls to you like the wild geese, harsh and exciting — / over and over announcing your place / in the family of things.
from “Wild Geese” New and Selected Poems, Vol. 1
This is from my favorite Oliver poem — and the most meaningful at a crucial point in my own journey:
But little by little, / as you left their voices behind, / the stars began to burn / through the sheets of clouds, / and there was a new voice / which you slowly / recognized as your own, / that kept you company / as you strode deeper and deeper / into the world, / determined to do / the only thing you could do — / determined to save / the only life you could save.
from “The Journey” New and Selected Poems, Vol. 1
I quoted the following lines in my mother’s eulogy in 2015:
To live in this world / you must be able / to do three things: / to love what is mortal; / to hold it / against your bones knowing / your own life depends on it; / and, when the time comes to let it go, / to let it go.
from “In Blackwater Woods” New and Selected Poems, Vol. 1
She let go of the love of her life, Molly Malone Cook, who died in 2005. Here is Oliver’s prose poem on falling in love:
Listen to me. Lift the oars from the water, let your arms rest, and your heart, and heart’s little intelligence, and listen to me. There is life without love. It is not worth a bent penny, or a scuffed shoe. It is not worth the body of a dead dog nine days unburied. When you hear, a mile away and still out of sight, the churn of the water as it begins to swirl and roil, fretting around the sharp rocks — when you hear that unmistakable pounding — when you feel the mist on your mouth and sense ahead the embattlement, the long falls plunging and steaming — then row, row for your life toward it.
from “West Wind #2” New and Selected Poems, Vol. 2
More challenging questions to keep you awake at night Tell me, what else should I have done? / Doesn’t everything die at last, and too soon? / Tell me, what is it you plan to do / with your one wild and precious life?
from “The Summer Day” New and Selected Poems, Vol. 1
Mary Oliver considered the end with some frequency in her work. When she died last month at the age of 83, I hope she realized she had, indeed, made something of her life.
When it’s over, I want to say: all my life / I was a bride married to amazement. / I was the bridegroom, taking the world into my arms. / When it’s over, I don’t want to wonder / if I have made of my life something particular, and real. / I don’t want to find myself sighing and frightened, / or full of argument. / I don’t want to end up simply having visited this world.
from “When Death Comes” New and Selected Poems, Vol. 1
And she certainly did more than visit the world:
The little sparrow / with the pink beak / calls out, over and over, so simply — not to me / but to the whole world. All afternoon / I grow wiser, listening to him, / soft, small, nameless fellow at the top of some weed, / enjoying his life. If you can sing, do it. If not, / even silence can feel, to the world, like happiness, / like praise, / from the pool of shade you have found beside the everlasting.
from “Just Lying on the Grass at Blackwater”
New and Selected Poems, Vol. 2
“Poetry,” Mary Oliver wrote in A Poetry Handbook, “is a life-cherishing force. For poems are not words, after all, but fires for the cold, ropes let down to the lost, something as necessary as bread in the pockets of the hungry. Yes indeed.”
If someone you love has died in a hospital, you may have seen modern death at its worst: overly medicalized, impersonal, and filled with unnecessary suffering. The experience can be a bitter lesson in Buddha’s most basic teaching: the more we try to avoid suffering (including death), the worse we often make it.
Even though roughly half of Americans die in hospitals and other institutions, most of us yearn to die at home, and perhaps to experience our leavetaking as a sacred rite of passage rather than a technological flail. You don’t have to be a saint, or be wealthy, or have a Rolodex of influential names to die well. But you do need to prepare. It helps to be a member of at least one “tribe,” to have someone who cares deeply about you, and to have doctors who tell you necessary truths so that you can decide when to stop aggressive treatment and opt for hospice care. Then those who care for you can arrange the basics: privacy, cleanliness, and quiet, the removal of beeping technologies, and adequate pain control. They can listen and express their love, and provide the hands-on bedside care hospice doesn’t cover.
From then on, a more realistic hope for our caregivers, and for ourselves when we are dying, may not be an idealized “good death” by a well-behaved patient, but a “good enough death,” where we keep the dying as comfortable and pain-free as possible, and leave room for the beautiful and the transcendent—which may or may not occur.
Hospice professionals often warn against high expectations. Things will probably not go as planned, and there comes a point when radical acceptance is far more important than goal-oriented activity. They don’t like the idea, inherent in some notions of the “good death,” of expecting the dying to put on a final ritual performance for the living, one marked by beautiful last words, final reconciliations, philosophical acceptance of the coming of death, lack of fear, and a peaceful letting go.
“In It Together” by Nancy Borowick. Nancy Borowick’s photo series (January 2013 through December 2014) depicts the experiences of Howie and Laurel Borowick, partners for over 30 years, who found their lives consumed by doctor appointments and the shared challenges of chemotherapy.“The Calm before the Storm”“His and Hers”
“I don’t tell families at the outset that their experience can be life-affirming, and leave them with positive feelings and memories,” said hospice nurse Jerry Soucy. “I say instead that we’re going to do all we can to make the best of a difficult situation, because that’s what we confront. The positive feelings sometimes happen in the moment, but are more likely to be of comfort in the days and months after a death.” This is what it took, and how it looked, for the family of John Masterson.
John was an artist and sign painter, the ninth of ten children born to a devout Catholic couple in Davenport, Iowa. His mother died when he was 8, and he and two of his sisters spent nearly a year in an orphanage. He moved to Seattle in his twenties, earned a black belt in karate, started a sign-painting business, and converted to Nichiren Shoshu, the branch of Buddhism whose primary practice is chanting. He never left his house without intoning three times in Japanese Nam Myoho Renge Kyo (“I Honor the Impeccable Teachings of the Lotus Sutra”).
He was 57 and living alone, without health insurance, when he developed multiple myeloma, an incurable blood cancer. He didn’t have much money: he was the kind of person who would spend hours teaching a fellow artist how to apply gold leaf, while falling behind on his paid work. But thanks to his large extended family, his karate practice, and his fierce dedication to his religion, he was part of several tribes. He was devoted to his three children—each the result of a serious relationship with a different woman—and they loved him equally fiercely. His youngest sister, Anne, a nurse who had followed him to Seattle, said he had “an uncanny ability to piss people off but make them love him loyally forever.”
When he first started feeling exhausted and looking gaunt, John tried to cure himself with herbs and chanting. By the time Anne got him to a doctor, he had a tumor the size of a half grapefruit protruding from his breastbone. Myeloma is sometimes called a “smoldering” cancer, because it can lie dormant for years. By the time John’s was diagnosed, his was in flames.
Huge plasma cells were piling up in his bone marrow, while other rogue blood cells dissolved bone and dumped calcium into his bloodstream, damaging his kidneys and brain function. He grew too weak and confused to work or drive. Bills piled up and his house fell into foreclosure. Anne, who worked the evening shift at a local hospital, moved him into her house and drove him to various government offices to apply for food stamps, Social Security Disability, and Medicaid. She would frequently get up early to stand in line outside social services offices with his paperwork in a portable plastic file box.
Medicaid paid for the drug thalidomide, which cleared the calcium from John’s bloodstream and helped his brain and kidneys recover. A blood cancer specialist at the University of Washington Medical Center told him that a bone marrow transplant might buy him time, perhaps even years. But myeloma eventually returns; the transplant doesn’t cure it. The treatment would temporarily destroy his immune system, could kill him, and would require weeks of recovery in sterile isolation. John decided against it, and was equally adamant that he’d never go on dialysis.
After six months on thalidomide, John recovered enough to move into a government-subsidized studio apartment near Pike Place Market. He loved being on his own again and wandered the market making videos of street musicians, which he’d post on Facebook. But Anne now had to drive across town to shop, cook, and clean for him.
The health plateau lasted more than a year. But by the fall of 2010, John could no longer bear one of thalidomide’s most difficult side effects, agonizing neuropathic foot pain. When he stopped taking the drug, he knew that calcium would once again build up in his bloodstream, and that he was turning toward his death.
An older sister and brother flew out from Iowa to help Anne care for him. One sibling would spend the night, and another, or John’s oldest daughter, Keely, a law student, would spend the day.
Christmas came and went. His sister Irene returned to Iowa and was replaced by another Iowa sister, Dottie, a devout Catholic. In early January, John developed a urinary tract infection and became severely constipated and unable to pee. Anne took him to the University of Washington Medical Center for what turned out to be the last time. His kidneys were failing and his bones so eaten away by disease that when he sneezed, he broke several ribs. Before he left the hospital, John met with a hematologist, a blood specialist, who asked Anne to step briefly out of the room.
Anne does not know exactly what was said. But most UW doctors are well trained in difficult conversations, thanks to a morally responsible institutional culture on end-of-life issues. Doctors at UW do not simply present patients with retail options, like items on a menu, and expect them to blindly pick. Its doctors believe they have an obligation to use their clinical experience to act in their patients’ best interests, and they are not afraid of making frank recommendations against futile and painful end-of-life treatments. When the meeting was over, the doctor told Anne that her brother “wanted to let nature take its course.” He would enroll in hospice. Anne drove him home.
John knew he was dying. He told Anne that he wanted to “feel everything” about the process, even the pain. He took what she called “this Buddhist perspective that if he suffered he would wipe out his bad karma. I said, ‘Nah, that’s just bullshit. You’ve done nothing wrong. The idea that we’re sinners or have to suffer is ludicrous.’” She looked her brother in the eye. She knew she was going to be dispensing his medications when he no longer could, and she wasn’t going to let him suffer. She told him, ‘You’re not going to have a choice.’”
The drive to treatment takes half an hour, and Howie and Laurel Borowick take turns, resting and driving, depending on who’s getting treatment that day. “The Drive to Chemo”In Laurel’s final moments, her family assured her that all would be OK. “Last Touch”
Anne said she “set an intention”: not to resist her brother’s dying, but to give him the most gentle death possible and to just let things unfold. On January 15, her birthday, she and John and a gaggle of other family members walked down to Pike Place Market to get a coffee and celebrate. John was barely able to walk: Anne kept close to him so that she could grab him if he fell. It was the last time he left the house.
The next morning, a Sunday, while Anne was sitting with John at his worktable, he looked out the window and asked her, “Do you think I’ll die today?” Anne said, “Well, Sundays are good days to die, but no, I don’t think it’s today.” It was the last fully coherent conversation she had with him.
He spent most of his last nine days in bed, as his kidneys failed and he grew increasingly confused. He didn’t seem afraid, but he was sometimes grumpy. He had increasing difficulty finding words and craved celery, which he called “the green thing.” He would ask Anne to take him to the bathroom, and then forget what he was supposed to do there. His daughter Keely took a leave of absence from law school, and Anne did the same from her job at the hospital. Fellow artists, fellow chanters, former students to whom he’d taught karate, nephews, nieces, and sign-painting clients visited, and Anne would prop him up on pillows to greet them.
Anne managed things, but with a light hand. She didn’t vet visitors, and they came at all hours. If she needed to change his sheets or turn him, she would ask whoever was there to help her, and show them how. That way, she knew that other people were capable of caring for him when she wasn’t there. “The ones that have the hardest time [with death] wring their hands and think they don’t know what to do,” she said. “But we do know what to do. Just think: If it were my body, what would I want? One of the worst things, when we’re grieving, is the sense that I didn’t do enough,” she said. “But if you get in and help, you won’t have that sense of helplessness.”
Each day John ate and spoke less and slept more, until he lost consciousness and stopped speaking entirely. To keep him from developing bedsores, Anne would turn him from one side to the other every two hours, change his diaper if necessary, and clean him, with the help of whoever was in the room. He’d groan when she moved him, so about a half an hour beforehand, she’d crush morphine and Ativan pills, mix them with water as the hospice nurse had showed her, and drip them into John’s mouth.
One morning her distraught brother Steve accused her of “killing” John by giving him too much morphine—a common fear among relatives, who sometimes can’t bear to up the dose as pain gets worse. At that moment, the hospice nurse arrived by chance, and calmly and gently explained to Steve, “Your brother is dying, and this is what dying looks like.”
The death was communal. People flowed in and out, night and day, talking of what they loved about John and things that annoyed them, bringing food, flowers, candles, and photographs until John’s worktable looked like a crowded altar. Buddhists lit incense and chanted. Someone set up a phone tree, someone else made arrangements with a funeral home, and one of the Buddhists planned the memorial service.
Most of the organizing, however, fell to Anne. It may take a village to die well, but it also takes one strong person willing to take ownership—the human equivalent of the central pole holding up a circus tent. In the final two weeks, she was in almost superhuman motion. She leaned in, she said, “into an element of the universe that knows more than I know. I was making it up as I went along. People contributed and it became very rich.
“That’s not to say there weren’t times when it was phenomenally stressful. I was dealing with all the logistics, and with my own mixed emotions about my brother. I was flooded with memories of our very complicated relationship, and at the same time I knew my intention was that he be laid to rest in the most gentle way possible.”
Hospice was a quiet support in the background. Over the two years of his illness, John’s care had perfectly integrated the medical and the practical, shifting seamlessly from prolonging his life and improving his functioning— as thalidomide and the doctors at UW had done—to relieving his suffering and attending his dying, as the hospice nurses and those who loved him had done.
There were no demons under the bed or angels above the headboard. Nor were there beeping monitors and high-tech machines. His dying was labor-intensive, as are most home deaths, and it was not without conflict.
A few days before he died, two siblings beseeched Anne to call a priest to give John last rites in the Catholic church. “It was a point of love for my siblings. They were concerned that John was going to burn in hell,” Anne said. “But John hated priests.” In tears, Anne called the Seattle church that handled such requests, and the priest, after a brief conversation, asked her to put her sister Dottie on the phone. Yes, Dottie acknowledged, John was a Buddhist. No, he hadn’t requested the sacraments. Yes, his children were adamantly opposed. No, the priest told her, under the circumstances he couldn’t come. It wasn’t John’s wish.
Ten days after the family’s last walk through Pike Place Market, the hospice nurse examined John early one morning and said, “He won’t be here tomorrow.” She was seeing incontrovertible physical signs: John’s lips and fingertips were blue and mottled. He hadn’t opened his eyes in days. His breathing was labored and irregular, but still oddly rhythmic, and he looked peaceful. The hospice nurse left. Anne, helped by John’s daughter Keely and his sister Dottie, washed and turned John and gave him his meds. Then they sat by his side. Anne had her hand on his lap.
“It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.
“He just had this one-room apartment with a little half-wall before the kitchen. I walked over to put water on to make coffee, and Keely said, ‘His breathing’s changed.’”Anne stopped, ran over, sat on the bed, and lifted her brother to a sitting position. He was light. She held him close, and during his last three breaths she chanted Nam Myoho Renge Kyo, as her brother had always done, three times, whenever he left his house. “I was really almost mouth-to-mouth chanting, and he died in my arms,” she said. “We just held him, and then my sister Dottie said her prayers over him.”
Anne sat next to her brother and said, “John, I did well.”
“I know he would not have been able to orchestrate it any better than how it unfolded,” she said.
“It was a profound experience for me. I realized what a good death could be.”
Dr. Susan MacDonald reflects on ‘Leo’ and whether she should have told him about assisted death
Dr. Susan MacDonald, a palliative care doctor in St. John’s, wonders if more could have been done for her patient ‘Leo.’
By Ariana Kelland
Susan MacDonald can’t quite pick one reason why Leo sticks with her, pushing her to put pen to paper to tell the story of her patient, and how she feels she failed him.
Asked what sets Leo — a pseudonym — apart from the rest, the palliative-care doctor shakes her head and sets her gaze away, “About Leo … I think, for one, I really liked him. I just really liked him.”
The second fact, MacDonald said, is that his death — suicide by taking his own opioids for insufferable pain — was not his only option.
Medically assisted death would have allowed Leo to die without having health-care professionals standing over him in a fruitless attempt at reversing his overdose, she said.
“He was such an intensely private person and his death was so public, and it didn’t need to be that way,” MacDonald said. “There were options. It just really struck me and made me think.”
MacDonald, an associate professor of medicine and family medicine at Memorial University of Newfoundland, reflected on her patient and what she could have done differently, in an article in the Canadian Medical Association Journal, titled Leo Died The Other Day.
The patient died within the last couple of years, MacDonald said, unable to comment further due to physician–patient confidentially.
To raise — or not to raise — the option of assisted dying
For five months, she and Leo worked hard to control his intense nerve pain. But Leo’s death was inevitable. He had cancer, and by MacDonald’s estimation, had only weeks — maybe months — to live.
Whether it was the physical pain that became too unbearable or the emotional struggle of his impending death, MacDonald doesn’t know why he took his own life.
“It was a very distressing clinical case for me because I felt, at the end of the day, I hadn’t done the best I could for this particular patient,” MacDonald said.
“It was a reflective exercise for me to look back and say, ‘What could I have done better? Where are the problems? And what do we need to do about it?'”
MacDonald said she never raised medically assisted death as an option for Leo. Neither did he. But she wonders if some patients want to bring it up but can’t.
Medically assisted death in Canada is legal. However, MacDonald said, there are no strict guidelines on how a doctor should broach the topic with a patient.
Changing the way she does things
Until Leo’s death, MacDonald would wait for the patient to bring it up, but the manner in which he died has her pausing for second thought.
“There may be people like Leo, who could avail of that option if they knew about it or if it was offered to them,” she said.
“On the other hand, you have the potential to do harm by raising that question,” she said, adding doctors run the risk of offending patients by even mentioning assisted dying as a option.
Medically assisted death is legal in Canada. However, there are no strict rules guiding how physicians should broach the topic with patients.
“I’ve been doing this for 25 years now, and I still haven’t figured out always the right thing to say and the right thing to do for people.”
MacDonald hasn’t gotten many more inquires about medically assisted death since it was legalized, she said. “Not nearly as many as you’d think.”
Now, as she continues caring for those whose deaths are inescapable, she has Leo to think about.
But can genealogy help predict how long I will live?
By Debra Bruno
Fascinated with genealogy, I’ve started spending too many hours chasing snippets of family stories. I figure if I can learn something about my family tree, it might shed light on my health and how long I will live.
I’ve become obsessed with two ancestors in particular: Permelia Van Valkenburgh and her son Amasa Matoon Van Valkenburgh.
Permelia was my great-great-great grandmother. Married at 17 to a distant cousin who shared her last name, she gave birth to 10 children over 18 years and died in 1855 at age 42.
Permelia was a 19th-century farm wife in the Catskill Mountains, a place where people didn’t roam alone at night for fear of panther attacks. Two of her 10 children died in infancy and one at 20. Her next-to-last child, Amasa, was my great-great grandfather. He was 9 years old when his mother died.
What killed her? If it was childbirth, there is no record of a child born or buried the year she died. If it was flu or tuberculosis or another contagious disease, there is no evidence of anyone else in her family dying in May 1855, although both were common causes of death in 19th-century communities. Maybe it was a laceration that became infected, picked up in unrelenting farm and housework. The month of May in the high Catskills could be chilly, and the winter stores of food would have been nearly depleted. Crops would not yet have produced anything. There was the occasional flash flood in the nearby creeks, so maybe she drowned.
Curious about what killed people in rural New York in the mid-19th century, I found the U.S. Census Mortality Schedules for the state from 1850 to 1880. The United States recorded this information once every 10 years and listed only those who died the year of the survey. Even so, I found some interesting details for Greene County, where she lived, in 1850: consumption (tuberculosis), cholera, dysentery, whooping cough, infection of lungs, infection of hand, infection of brain, asthma, childbirth, drowning and cancer were listed as causes of death. The most frequent cause was cholera. Many times, the named cause of death for people in their 80s and 90s was “old age.”
Did any of this have any meaning for me? Probably not. “The big picture is the shift from infectious disease as a major cause of death to chronic diseases,” said Charles Rosenberg, professor of history of science at Harvard. Causes of death such as tuberculosis were “background noise,” he said, so common that they were unremarkable. What drew more attention were cholera epidemics or influenza sweeping through communities.
Susan Speaker, a historian with the National Library of Medicine at the National Institutes of Health, said that before the 1920s, more Americans died of “microbe-caused diseases” than anything else. The balance started to shift by the 1930s and ’40s, she said.
In other words, a farm wife living in the country — while not exposed to the overcrowding and bad water of cities — would have had a number of other health challenges.
For instance, “if you came down with appendicitis in the 1900s in the country, you might be out of luck,” said Speaker, “unless you had a local practitioner who was a decent surgeon.”
While I was getting closer at making an educated guess at the cause of death, my mother and I ventured into the Catskill Mountains one Sunday morning in August after services at the First Reformed Church in Athens, N.Y., the village on the Hudson River where we both grew up and where many of our ancestors now rest.
We drove high into the mountains until the ski resorts and gift shops dropped away, the houses became more spread out, and the forests got thicker in the Catskill State Park, land first preserved by the state in 1885. Finally we reached the turnoff to Westkill, the hamlet of a hamlet, tucked between hills in a valley.
The cemetery was small, with maybe 40 stones. The grass had been newly mowed, and damp cuttings thrown by a power mower still plastered the white sides of the Westkill United Methodist Church (built in 1848) and, next to it, the Westkill Baptist Church (built in 1830). One or two graves had collapsed, leaving a deep, grass-lined trench in the earth. We peered inside the churches, but both had been long abandoned. Even the pews were gone.
Back at the far edge of the cemetery, just before the ground dropped off to a creek, I found a dark, mottled headstone. It read:
PERMELIA A.
Wife of Jacob Van Valkenburgh
Died May 7, 1855
Aged 42 years, 3 mo, 5 ds
Near her was the stone of James, the 20-year-old son who died just two years before her. Along with losing babies Elizabeth, Huldah and George, did James’s death in 1853 lead to her decline?
Just a few steps away was her son Amasa, my great-great grandfather.
Amasa M. Van Valkenburgh
Died July 1, 1890
Aged 44 years
Here was another ancestor who died young. Amasa married at age 24, had five children with his wife, Christina Smith, and died in the middle of the summer.
Town records in Lexington, N.Y., eventually turned up his cause of death: “acute peritonitis,” which is an inflammation of the abdominal wall. Untreated, as it would have been in pre-antibiotic times, peritonitis leads to sepsis and death. What is still a mystery is what caused the peritonitis. It could have been a puncture wound to the stomach. It also could have been cirrhosis of the liver, which often leads to peritonitis. NIH’s Speaker said it would be impossible to know whether the peritonitis resulted from cirrhosis, a perforated gastric ulcer, a burst appendix or a ruptured gall bladder.
Buried alongside him was his wife, Christina. She went on to remarry and outlive a second husband. Christina passed away in 1946 at age 96. She would have remembered the Civil War, World War I, women getting the right to vote and World War II.
Of her five children with Amasa, two lived into their 90s, and another to 87. And her grandson, my grandfather Orrin, lived to 97.
Does this mean, then, that I could count on a longevity gene?
A study published in Genetics shut down that fantasy. Looking at 400 million people born between 1800 and 1920, whose information had been collected from public family trees in Ancestry.com, investigator Graham Ruby found that only about 10 percent of human longevity is inherited. Previous estimates ranged from 15 to 30 percent.
Our intuition is that long life spans run in families, Ruby said. And yes, genetics does contribute to life span, he said, “but to a much lesser extent than we thought.”
“Honestly, all of us were a little surprised,” said Catherine Ball, chief scientific officer at Ancestry, which collaborated with Ruby at Calico, a California research-and-development company.
“What this work has shown is not that longevity isn’t inherited,” she said. “It is inherited, but the cause is not often genetics.” In other words, humans also inherit money, property and social status, which also influence longevity.
Both Ruby and Ball said that a much more important role in longevity is “assortative mating.” In other words, people tend to marry people who are similar to them in location, socioeconomic status and education, and those factors also influence longevity. People are more likely to match the longevity of their in-laws than their ancestors, Ruby said.
The research showed fascinating patterns such as a drop in longevity about 1918, when World War I and the Spanish flu were killing millions, Ball said.
“Over time, the types of things that caused mortality were very different,” she said. “Infectious disease was a much more important killer then than now. Childbirth was not something you really wanted to go through.”
In other words, both researchers said, much of what foreshadows our longevity today involves healthy lifestyles and access to medical care more than genes. I didn’t necessarily uncover any clues about my own health ancestry in my research, but I did develop a greater respect for the enormous achievements of modern medicine.
Windblown rain lashes against the hospital windows in an uncertain rhythm that seems even more unsteady as I enter the patient’s room near the nursing station. There is music in this room. Two people sit in chairs by the bed of a patient, a woman who is lying very still. I recognize the voice of Elton John coming from a tablet computer on the bedside table. He’s singing “Crocodile Rock.”
“She liked this,” says the woman’s daughter, smiling and rolling her eyes, as though to say “Elton John, really?” The dying woman’s husband glances at his daughter, then at me, and says, “We followed the advice from one of the nurses to play some music in her last few hours and days.” He smiles slightly, as if in apology for the jaunty tune ( I never knew me a better time and I guess I never will ) in this solemn setting.
His wife’s eyes are closed. Her breathing is steady. Her pulse is fine, about 90 beats per minute. She is much calmer than yesterday, when she was flushed, frowning and seemed in considerable pain. But she is dying. We are giving her as much support as we can to help her be free of distress or discomfort.
I’m a palliative care doctor. I work in Britain in a general hospital, a cancer hospital and a hospice. Sitting with someone you know and love who is dying can stir a craving for a bit of normality in what otherwise might seem a surreal setting. Not that dying isn’t “normal,” but nowadays death and dying are often hidden away in hospital wards or nursing homes, and many people don’t know what to do, or what not to do.
I often tell the family and friends of a dying person that they needn’t speak in hushed tones, that they are welcome to chat or share a joke or call out crossword clues. Or play some tunes. Putting on a favorite song can become a ritual celebration as you enjoy a moment you shared many times before.
Some people don’t need any encouragement — I have seen plenty of terminally ill patients die with music playing in the background. But in the past few years, as the benefits of music in these settings have become more apparent to me, I have paid more attention to what is on.
Music can even help with those who are severely ill but recovering. The father of one of my younger patients put his playlist on while his daughter was in critical condition. Through her delirium, she complained when a well-known rap song from the ’90s came on. Later, after she awoke and was more responsive, her father defended his back catalogue of music, and a debate about good taste ensued — their conversation accompanied by the usual hospital soundtrack of beeps and infusion drip alarms and squeaking cart wheels.
Listening to familiar musical passages can prompt significant emotional responses, causing the release of neurotransmitters such as dopamine. In particular, they are released in an ancient segment of our brains, known as the striatum, which is associated with emotional responses to rewarding inputs such as food, sex, drugs and . . . rock-and-roll.
What happens to the brain in our dying moments? The shutting-down process is not as straightforward as you might imagine. Most of the research on the topic has been done with rodents, so we may not be able to extrapolate too much. But dying rats experience heightened activity in their frontal cortical areas, when the oxygen and glucose have been taken away and there is a huge influx of calcium into their brain cells. Our ability to have conscious thought and experience depends on the strength of the connections between the frontal areas of the brain, associated with mental abilities, and those nearer the back of the brain that process sensory information. These connections, in dying rats, actually strengthened by five to eight times after cardiac arrest, compared with waking moments.
Such a surge in the human brain may explain why some people who have near-death experiences report heightened sensory information. Those who are dying may also be able to process auditory information better than is generally assumed. It is entirely feasible that, in our dying moments, we are more aware of what is happening around us than previously believed.
Any pet owner will tell you that losing them is as great a pain as losing any member of the family. It’s in these moments we’re at our most vulnerable. One brave photographer has taken on the task of capturing such fragile moments in a series that documents owners struggling to cope in the last moments of their animal’s life.
Ross Taylor’s powerful new series is one that’s sure to bring a tear to the eye of any pet owner. His inspiration came after being “profoundly moved” by witnessing a friend struggle with the deteriorating health of her pet and her subsequent decision of euthanasia. The collection of images, he says, explores the intimacy of the human-animal bond, specifically “the last moments before and after the passing of a pet at home with their owner.”
Leigh Zahn fights back tears as she lays with her dog, Spencer, in her lap a final time, just moments after Spencer passed.“She’s always been my companion. Coco was there for me when he was on deployment,” said Rebecca Cassity, as she fights back tears. Her husband, Drew, was in the military. Dr. McVety reassures her with a hug and consoling words: “This is better treatment than any one of us would get.”
The images were taken in Tampa Bay, Florida throughout 2017-18 and involved working closely with the families involved. The pet owners seen in the images were aided by veterinarians from Lap of Love, a pet euthanasia service that allows for a peaceful passing at home. Founded by Dani McVety, the organization has been working with Caring Pathways, all of whom Taylor expresses utmost gratitude for. “It couldn’t be done without their willingness to participate and belief in the project… They have my respect,” Taylor said.
In one of the most intense moments I’ve ever witnessed, Wendy Lehr cuddled beside her dog, Mimosa, shortly after she passed. The muffled sounds of her cries filled the empty room as she nuzzled against her face. She cried out: “Oh my baby, oh my baby. What am going to do without you?”“It’s tough saying goodbye,” said Carrie Peterson after she dropped sunflowers over the grave of her dog, Asia. The smell of freshly turned earth is what I remember and how peaceful Asia looked within it.
While difficult, the at-home euthanasia process can be one that mitigates some of the painful reality of the end of life. It’s worth noting that the vets I’ve worked with are some of the most compassionate people I’ve met and always offer the families a chance to have a respectful moment afterwards with their beloved pet. It’s in stillness of these moments that I sometimes felt the most emotional for everyone involved.
Bob Zahn touches his dog, Spencer, just moments after the dog passed. His wife, Leigh, left the room immediately, as it was too much for her to take. “She’s going to take it harder maybe than the loss of her parents. Your parents can tell you when something’s wrong, but your dog can’t.”Vanessa Gangadyal consoles her son, Ian, 8, while her husband, Michael Gangadyal, pets their dog, Ally, shortly after its passing.“When I was sick, she knew something was wrong,” said Bob Lutz about their dog, Heidi, who looked up at them moments before she was euthanized due to recent substantial declines in health. His wife, Cindy, added: “she helped take away our pain.” At right, watching, is their other dog, Winnie.
If you were as moved as we were by this powerful series, you can see more of Taylor’s work (some of which saw him nominated for a Pulitzer Prize) at his website and Instagram.
It is common wisdom that nobody ever wished he’d spent more time at the office when he’s at death’s door.
That certainly makes sense, but Michael Ent, a social psychologist at Towson University, did what researchers do when confronted with unproven beliefs. He wondered if it was true. Then he tried to find out.
He and Mary Gergis, a nurse who also teaches at Towson, asked hospice nurses what dying people really talk about at the end of their lives. The 124 nurses from the Hospice and Palliative Nurses Association who responded to an online survey said patients are often more consumed with worries about how their families will fare after their deaths than they are with their own fates. They are about as likely to savor lives well led as to grapple with regrets. Many are worried about legacy and finances, a sign, Ent thinks, that some of them do indeed wish they’d worked more, or at least done a better job of managing their money.
Ent said the information, which has been accepted for publication in the journal Death Studies, could be helpful to caregivers. Some may be reluctant to push patients to engage in “life review” — end-of-life discussions of life history that have been shown to help alleviate anxiety and depression. “Sometimes patients might feel that it’s intrusive for a stranger to start asking them about their personal lives,” Ent said. However, if patients bring up some of the topics the nurses mentioned, that could be an opening for a deeper conversation.
Ent, whose wife is a nurse who has worked with hospice patients, said he was interested in what we could learn from the dying. Most of the academic studies he was able to find were more focused on practical aspects of support for the dying than on trying to harvest their wisdom. He couldn’t find anything about which subjects were on their minds. He read The Five Invitations: Discovering What Death Can Teach Us About Living Fully, written by a Buddhist hospice founder, but Ent wanted to do something more concrete and systematic. He read The Top Five Regrets of the Dying, also written by a hospice worker, and particularly questioned the top regret: “I wish I’d had the courage to live a life true to myself, not the life others expected of me.”
Again, Ent was skeptical. “I couldn’t imagine that being a top deathbed reflection,” he said.
For the survey, Ent and Gergis asked the nurses to list up to five “reflections” they heard most frequently from hospice patients. He concedes it would have been better to talk to patients themselves, but said privacy rules make them harder to reach. The nurses’ answers covered a wide range, from regrets to pride to faith in an afterlife. “I don’t want to be a burden” was a common sentiment, and many patients worried about how survivors would cope after they died. Some wished they had taken better care of themselves. Some said they were ready to go, while others wished for more time. They were thinking about whether their lives had mattered.
Ent categorized the comments and found that concern about loved ones was the most common response. Half of the nurses mentioned it. Regrets — these included people who thought they’d worked too much — came up 42 percent of the time, compared with 36 percent for gratitude. Concerns about legacy were cited by 29 percent of the nurses. Some of those people wished they had achieved more. About the same number of nurses said patients often said they were not ready to die (29 percent) as said they were ready (28 percent).
Ent said that the survey results show that hospice workers may want to spend more time allaying patients’ fears about how their deaths will affect family members.
He also thinks that research on what dying patients regret could help healthy people plan for the inevitable. Maybe fewer of us would be “blindsided” by our deaths if we talked more openly about mortality. Better financial planning could prevent many of the worries about unpaid bills.







 “It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.
“It was January in Seattle,” Anne said. “The sun was coming through the window and we could hear the market below beginning to wake up. We were just the three of us, talking and sharing our stories about him and the things we loved and didn’t love, the things that had pissed us off but now we laughed about. I can’t ever, in words, express the sweetness of that moment.











