A conversation with Anita Hannig, author of ‘The Day I Die: The Untold Story of Assisted Dying in America’

By Richard Harris
Like taxes, death is still a certainty. But in America, the end of life isn’t what it used to be.
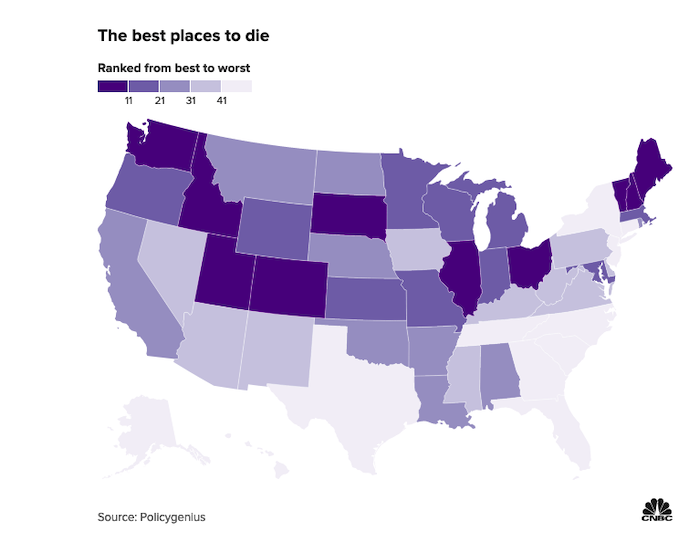
Today, one in five Americans lives in a state that permits medical aid in dying, sometimes simply called assisted dying. The idea is terminally ill individuals who have six months or less to live can apply for a medically assisted death to limit their suffering. And if they meet the criteria, they can have some say when they will take their last breath.
It’s been nearly 25 years since the country’s first assisted death law — Oregon’s Death With Dignity Act — went into effect. And since then, eight other states — Washington, Vermont, California, Colorado, Hawaii, New Jersey, Maine and New Mexico, as well as Washington, D.C., have enacted their own versions. What all jurisdictions with medical aid in dying have in common is the requirement that the patients must be of sound mind, have less than six months to live and they must be able to self-administer the lethal medication, prescribed by a physician, to end their lives.
Eleven other states have introduced medical aid in dying bills during the 2021-22 legislative session. It’s a growing movement that’s largely under the radar, much as death is in this society.
Assisted death is “not the path of least resistance. For many it’s the path of most resistance.”
In the latest survey by Susquehanna Polling & Research, two out of three voters (67%) said if they “had an incurable, terminal illness, still had a sound mind but less than six months to live and met the legal requirements,” they would want the option of medical aid in dying.
As the baby boomers age, medical aid in dying is expected to be an even bigger issue in the years ahead.
Anita Hannig, associate professor of anthropology at Brandeis University in Waltham, Massachusetts, says assisted death is “not the path of least resistance. For many it’s the path of most resistance.”
Indeed, the assisted dying laws in the ten U.S. jurisdictions are among the most restrictive in countries with such laws. That hasn’t stopped opposition from some religious and right-to-life groups, among others.
For her new book, “The Day I Die: The Untold Story of Assisted Dying in America,” Hannig spent hundreds of hours over five years on the frontlines of assisted dying in the Pacific Northwest, including witnessing several deaths among those who availed themselves of the law.
Next Avenue: You’ve taken a very deep dive into assisted dying in America, a world few families have experienced. As a cultural anthropologist, you’ve gone from researching birth and the beginning of life in Ethiopia to the opposite end of the life cycle. Why the shift?
Anita Hannig: I was showing a film called ‘How to Die in Oregon’ in my Medicine and Religion class at Brandeis. It’s such a lovely documentary about the law in Oregon and about all those assisted dying volunteers who go and help people die. And I was immediately hooked and thought, wow, birth and death are like bookends. You have home births and home deaths. And so I was curious to go over to the other side. I was very surprised by what I found.
You must have a unique perspective on birth and death as an anthropologist studying assisted dying and as a new mother who also lost a child during an earlier pregnancy.
Definitely. We’re so used to thinking about birth and death as opposites when they’re actually very similar. One of the main figures in my book, a former nurse and longtime assisted dying volunteer in Oregon, Derianna Mooney, taught me that birth and death are both sacred transitions — from one state of being to another, from nonbeing into being and being into nonbeing. And culturally we revere one, but we shun the other.
“I think part of the issue is that we have all the technology now, but our ethical and moral compass hasn’t really caught up with how we should use it.”
As a new mother, I can see people’s eyes light up when they watch us stroll by with our oversized pram. There’s so much positive attention. And all of this has to do with the fact that we love the beginning. It holds so much promise.
And yet we’re so afraid of the end. Similar to a birth, people do need help at the end of life. I love when Derianna says, “You’re going to the gate with them and you are letting them go, but you’re nurturing them through the gate.” What a beautiful vision.
One of the vexing issues surrounding death in our country especially is the role high-tech medicine plays in extending life — even when a longer life doesn’t always promise more quality. Is the assisted dying movement a sign that technology is frequently not making our final years better?
Yes. I think part of the issue is that we have all the technology now, but our ethical and moral compass hasn’t really caught up with how we should use it. And it’s not just in the United States. My 87-year-old grandmother, who passed away in Germany in March, underwent radiation for her breast cancer when she was two weeks away from dying. I’m flabbergasted when I think about why we offer this extremely invasive treatment to somebody who is close to dying. Thankfully, she was soon admitted to a beautiful hospice by a lake to spend what became her final days.
I got interested in this topic when a friend’s husband, suffering from Parkinson’s and no longer able to feed himself, was forced to starve himself to death since he lived in Maryland, a state without a medical aid in dying law. For people consigned to such a horrific death, can a doctor truly say they are following the Hippocratic Oath that tells physicians to do no harm?
That’s exactly the conclusion that a lot of doctors who help patients die come to because in that case doing nothing — such as not helping somebody die — is doing harm. Physicians who are at the forefront of assisted dying say their task is to prevent suffering. And how you prevent suffering in many of these cases is to help somebody die. I always come back to this question: Who is telling these patients that they need to hang on? For what? For whom? Sometimes they themselves are ready to go, but they want to stick around for the family or because there’s a societal expectation to fight.
At the beginning of your book, you almost took my breath away when you were helping one of the volunteers opening the capsules of Seconal and pouring powder into a bowl in one room while the patient, Ken, was waiting in the next room to receive the lethal medication. What were your thoughts as you prepared the medicinal mix that you knew would end a man’s life?
It’s a really good question. Anthropologists have a tool in our toolbox called “participant observation.” And that means you’re never just an impartial observer because your presence alone already changes what’s happening in the room. In order to really relate and put ourselves and the reader into the shoes of these people, you have to bring yourself into the situation wholeheartedly and authentically. And often that means becoming a participant in what is happening.
It’s an extreme privilege to be invited into that kind of intimate space. So, it would have felt very off- putting to just be sitting in the corner taking notes. Everybody in the room is carrying this person over the threshold together. And so you just kind of take your cues from what’s happening.
You don’t want to feel like a voyeur?
Exactly. You want to be in the moment and going through all the emotions other people are going through. It’s a different way of being present that allows you to faithfully experience the death alongside the people whose loved one is dying.
But this must have been a difficult moment for you. In your book, you described “a heavy sense of transgression rise up inside” of you as prepared the lethal medication.
You know what I think it is? It’s the feeling of internalizing some of the stigma that we carry and some of the taboo with which we treat death. And so being part of somebody’s death in this participatory way makes you ask, ‘Am I doing something wrong? Am I, in some bizarre way, enabling that person to die?’
But even if I hadn’t been there, things would have gone probably in a very similar way. I think it’s the cultural baggage that we feel around what it means to hasten the end of your life. Everyone there knew this is what Ken wanted. He chose this with one-hundred percent of his cognitive abilities. His wish was to be delivered from this world and you are enabling that transition.
Among the deaths you researched but didn’t witness was that of Louis, who was an outlier. His experience turned into a nightmare for the person who supervised his assisted death. Louis actually woke up after taking the lethal medication. What happened?
“Everybody in the room is carrying this person over the threshold together.”
Medicine is a human art and as an art, is prone to failure. And it just goes back to the ways the laws are written. They insist on self-administration. But when you are limited that way, you’re going to run into a bunch of problems such as people with gastrointestinal issues who can’t quite absorb the medication. And then you have people who can’t physically self-administer, like a lot of folks with ALS or other illnesses that affect their mobility or their hand range or who can’t drink something on their own or push the syringe on their feeding tube.
And people are getting a little more innovative with things like rectal catheters now, but there’s still a requirement that this has to be an act of volition — you have to be the one to push the plunger on your feeding tube or catheter, what have you. And in almost all other countries, you don’t have that requirement. A doctor can administer if you’re unable to administer yourself.
So after immersing yourself in this world of assisted dying for five years, what‘s your takeaway from this experience?
As a society, we have to make a concerted effort to become less alienated from death and dying. Of course, one could ask how alienated are we when the biggest newspaper in the country, the New York Times, can post images of corpses in Ukraine on its front page? But that doesn’t create closeness or connection. That just creates more fear.
Ideally, I think everybody should have to take a class on death and dying that could cover estates, hospice, and what life-extending procedures there are. In my death and dying class, I talk about people in South Korea who fill an entire gymnasium with coffins and the public comes in and gets inside the coffin to simulate what it would be to die. And they come out of this experience with a totally new zest for life.
This is what contemplating our mortality can do for us. It can take away some of the fear and some of the surprise when a loved one passes away because you will have thought about it in advance. I’m not saying assisted death is the way to go for everyone. We really need to pay more attention to end-of-life issues and prepare for the inevitable and have all of that be less stigmatized.
As the country’s pandemic death toll inches toward one million, has America’s attitude toward death changed at all?
Certainly it’s brought death into the lives of lots of people but not in a way to make them feel more connected to death. Many people weren’t able to see their loved ones in assisted living homes or couldn’t go to the funeral or they weren’t allowed to be present at a nursing home.
When I see the way that we’re tumbling back into life as it was before the pandemic, I don’t know that we’ve really thought critically about death. We just have this big fear-based relationship with death and it’s not lifting the curtain, really. I think people are thrilled to have escaped the pandemic. They see themselves on the other end of that mostly unscathed.
They dodged a bullet?
That’s exactly what it is. But I don’t think it’s made us really contemplate our mortality that much more.
So what will give you a signal that something has shifted in the American attitude toward death?
That people don’t automatically associate the topic of death with fear. And when people begin to realize what I witnessed and write about in the book — some of the empowerment that can come from determining the end of your life and even some of the joy. I hope I’m not out of line to call it joy. When I think of the deaths I witnessed, they weren’t unambiguously sad. There were also serene and heartfelt moments, some laughter and families felt at ease because their loved one wanted to die and they were helping them.
And those who chose to end their lives wanted their death to resonate beyond themselves and their families. Jean, one of the people whose death I witnessed, unbelievably spent the last few minutes of her life promoting her chosen way to die. I still remember her words:
“There are all these baby boomers who will want a better way to die. Our society doesn’t recognize that yet. They will someday.”
Complete Article ↪HERE↩!