With continual advances in modern medicine, we’re enjoying longer lives. As the population ages, and particularly as many people are living longer with cancers and chronic diseases, end-of-life care is adapting and changing.
People who are approaching the end of their lives will usually spend some or most of their time at home, requiring care and support to do so. Family members might not always be available to provide this care. When they are, the process can be rewarding, but it can also be challenging and complex, often leading to a severe emotional burden for the carer.
Gaps in our health and social care systems are starting to be filled by death doulas. But beyond providing practical support, families are increasingly seeking the services of death doulas to help navigate the experience of dying. Those nearing the end of their lives, too, may bring in a death doula to ensure they can die the way they want to.
We urgently need a conversation about death doulas and new models of care at the end of life. We are continuing to build an evidence base through research with the death doula community and via consultation with the health services that interface with death doulas.
Defining the death doula
We’ve seen a similar concept in midwifery, where birth doulas have long been providing social, emotional and practical support to help women through the process of childbirth. This has been shown to have positive outcomes for mothers and their babies.
Like birth doulas, death doulas’ roles and functions are non-medical; these can include advocating, supporting (spiritually and sometimes physically), guiding, and providing emotional support to the person and their family, mainly in the home.
We undertook a systematic review of the literature to find available evidence about the death doula role. We found little formal academic literature describing the role, their training, or contribution to individuals, families and the health system.
But what we do know is that each death doula enacts the role differently. They might spend time with the dying person, offering emotional and spiritual support, and sometimes providing physical care. They might support the family carers in the work they are doing. Some death doulas are only present in the last days of life, offering “vigiling” – sitting with the dying person so they are not alone.
Some doulas offer after-death rituals such as helping families prepare the body or keeping the deceased at home.
A death doula can provide additional support to family members acting as caregivers at the end of life.
Some death doulas are paid by families who engage their services. Families have often found their chosen doula online or through word-of-mouth. Other death doulas work voluntarily, in a similar way to a hospice volunteer. But, because there are no formal structures or registers, we don’t know how many death doulas there are.
In Australia and elsewhere, palliative care nurses, social workers and those from the funeral industry work as death doulas. This seems to be a natural progression, but it’s a grey area: doulas are providing care, but are not registered or supervised.
There is little formal assessment to guide patient and family choice or to inform end-of-life care provided by professionals.
How can doula care be formalised?
Providing care in homes can be informal. It may be provided by families, friends, or community groups. Care can also be formally negotiated and provided by health services, aged care providers or private agencies.
It’s necessary to understand the implications of the death doula role. For example, they could become part of formal care arrangements such as home care packages or via private health insurance funding.
We also need to look at how these new roles are authorised to represent the dying person, as they are neither a family member nor a qualified health professional. It’s also important that they are appropriately trained and insured (if providing paid services).
There are personal, social and cost advantages in enabling care in the home for a dying person. For families, being able to support the person in a familiar environment can be a powerful motivator to engage a death doula to fill the gaps in care provision.
For the health system, care in the home is seen as positive. It can avoid unnecessary hospital use and help spread the costs of caring.
For the dying person who may prefer to die at home, it is a way of achieving this. Importantly, death doulas can improve the dying person’s ability to control their own care.
The death doula role may well incorporate some of the direct care provided by families and help them to navigate the complex needs and planning required at the end of life. If so, death doulas could represent an important opportunity to improve dying outcomes.
We need to ensure our community is informed, health service provision crosses both hospitals and homes, and that those providing care – regardless of setting – have skills and knowledge appropriate to their role.
Death and grief are natural parts of the human experience, but mourning a loss is also an incredibly complex process.
When a young child loses a loved one, parents often grapple with the challenge of explaining the concept of death and helping their little one through the grieving process (all while grieving themselves).
To help inform these difficult conversations, HuffPost spoke to a number of child mental health experts. Of course, a family’s cultural and religious background may steer the discussion, but there are certain guiding principles that are helpful for everyone to keep in mind.
Here are some expert suggestions for parents and caregivers when they prepare to talk about death and grief with children.
Be Honest And Straightforward
“Tell them the ‘facts’ about the death,” clinical psychologist John Mayer told HuffPost. “Don’t sugarcoat what death is or use ‘baby talk’ with a child. Do not use phrases like, ‘Grammy is sleeping.’ This is an opportune time to teach them about death. Don’t shy away from it.”
Board certified licensed professional counselor Tammy Lewis Wilborn echoed this sentiment, noting that using “cutesy language” and euphemisms in an attempt to protect kids from the realities of death and loss can actually do more harm than good.
“Children tend to think concretely, not abstractly, so when you use language that’s euphemistic, it can actually be more confusing or frustrating,” she explained. When people say things like “Dad is in the clouds” or “Your dad is taking a really long nap,” a young child may not understand the permanence of the fact that their father died and might even look for him in the clouds or expect him to wake up at some point.
Words like “death,” “died” or “dying” may sound harsh, but this is still developmentally appropriate language, Wilborn noted, and it’s important for children to have the language to understand the permanence of death.
Ask And Answer Questions
The kind of conversation a parent has with a child following the death of a loved one depends on the child’s relationship with the person who died. It should also vary based on the child’s developmental age and their understanding of what happens when someone dies. To that end, it’s useful to ask kids questions or offer to answer any questions they might have.
“Starting with questions can be a way in,” said Wilborn. “And you don’t necessarily need to give the specific details of how the person died, particularly if we’re dealing with traumatic grief. They don’t need all of the information, but they need enough age-appropriate details to understand that a person has died and isn’t coming back.”
Sometimes children may have witnessed something related to the loved one’s death, like being present at the scene of an accident or visiting the person in the hospital. In these cases, they need help understanding what they saw, said Chandra Ghosh Ippen, an expert in early childhood trauma and the associate director of the Child Trauma Research Program at the University of California, San Francisco.
Parents should try to shrink themselves down to the size of their child and walk through what they’ve experienced. Seeing someone in a hospital with tubes coming out of them or watching paramedics perform lifesaving procedures may be frightening for a small child, so it’s necessary for adults to appreciate how scary things might look to them.
“Create space for them to share how it might’ve affected them, and try to help them understand that doctors and paramedics were trying to help their loved one,” Ghosh Ippen explained.
It’s an ongoing conversation. “Young children will often come back to you after your very excellent explanation of death and still ask, ‘Am I going to see so-and-so?’” Ghosh Ippen said. “It’s not that they didn’t understand you, but little kids tend to repeat their questions. It’s sort of their way of mulling it over and making meaning. This can be painful for caregivers, but appreciate that the child did hear you and is just having a difficult time wrapping their head around the concept of death.”
Know That Their Emotions Are Complicated
“Grief is a complex process, so it comes with a range of thoughts, emotions and behaviors,” Wilborn explained. While parents may expect their child to feel sad, angry, confused or even guilty about a loss, there are other behavioral changes that can be harder to understand, like changes in sleeping and eating patterns or school performance issues.
Sometimes parents may feel confused about a perceived lack of sadness in their kids. “Young children have a short sadness span,” said Ghosh Ippen. “A child can suffer a devastating loss and feel really sad, and then they can go play. You may be thinking, ‘Were they really affected by what happened?’”
While adults tend to immobilize and sink into sadness, kids often discharge it by running around or trying to do something else. “They kind of go in and out of sadness, and that can put us at odds with them if we’re thinking, ‘Oh, my God, do they not care?’” she continued. “But recognize that they did care.”
Be Patient
Wilborn noted that grief is a long process, so parents should reject the tendency to want to rush past it and wonder when their kids are going to be over it.
“Grief is a process that you cannot go around. You have to go through it. So you need to be OK with the pace of the process,” she said. “It can take some time for a child to return to his or her normal.”
Mayer emphasized the power of this experience and of talking to kids about death as a way to build major developmental coping skills. “This is a positive and helps them cope with loss in their life in the future and even transitions in their life, such as leaving one school to another, advancing to high school or college, and losing relationships.”
Encourage Expression
“Children need to see that their parents are a resource; home is a resource where grief is welcome,” Wilborn said, noting that parents should encourage age-appropriate expressions of grief.
“For example with a school-aged, play is their language, so you want to lean into ways that children play to promote communication ― things like drawing pictures, playing games, dolls, puppet shows at home,” she added. “With older kids, you might encourage them to journal, draw, write songs, create poems.”
Mayer noted that being a resource for your child creates a sense of safety and security that will serve them in later life events. “They know they can depend on you, and it is wonderful modeling for them.”
Create Rituals
Creating rituals around remembering and honoring a loved one who died is another significant form of expression. “Explain that this person may not be here with us, but we can still remember him or her and celebrate their life as a family,” said Wilborn.
“When the death is really traumatic, sometimes caregivers stop talking about the person who died,” Ghosh Ippen explained. “And what’s hard in those cases is that children lose their ‘angel memories’ ― times when they really felt loved and cared for with that person. It’s normal for grown-ups in mourning to find it hard to talk about the person who died, but it’s important to memorialize them.”
The death of a loved one offers an opportunity to talk to your child about your cultural and religious beliefs.
Many cultures and religions promote rituals around saying goodbye and making meaning of death. Mayer noted that losing a loved one presents an opportunity for parents who have religious belief systems to explain these tenets to their children.
“Religious or not, it is also very helpful to teach your children that all the experiences and memories you have had with this loved one do not get erased with their death. People always live in our hearts and our minds forever, and no one or nothing can take that away,” he explained. “Say something like, ‘Where’s Aunt Susie right now? She’s not in this room with us right now, correct? That doesn’t mean she doesn’t exist.’ Aunt Susie is here (point to your head) and here (point to your heart). We have to keep our memories and good times with Aunt Susie alive.”
Make Sure They Know It’s Not Their Fault
“Sometimes children have this really uncanny way of assigning blame to themselves for things that have nothing to do with them,” said Wilborn.
With that in mind, caregivers need to help kids understand that the death is in no way their fault, and it’s not their responsibility to put on a strong face or hide their feelings.
Use Books And Other Resources
There are many great resources for parents navigating this difficult topic with their children. Ghosh Ippen and Wilborn both recommend Sesame Street’s online grief toolkit, which provides talking points, videos, activities, storybooks and more. Ghosh Ippen and Wilborn also pointed to the National Child Traumatic Stress Network as another great source of online resources.
There are many children’s books that cover the experience of loss.
Beyond books and online resources, Wilborn emphasized the value of community resources, such as school counseling, support groups, play therapy and peer counseling.
Let Them See You Grieve
The way a child’s parents or caregivers respond to a loss is instrumental in helping them cope. “They need to see you grieve,” said Wilborn. “But they also need to see you taking care of yourself and engaging in self-care, which may or may not include professional help. If you don’t, they may feel like they have to take care of you because you’re not managing grief in a way that’s healthy.”
It’s OK to cry in front of your children and show the value of expressing emotions and having shared emotions among family members. It’s OK to say things like “I’m feeling really sad because my dad died” or “Daddy is sad because he misses his mom.”
“Within our culture, we often have a sense that we have to be tough, so many parents are trying to help their kids by putting on a brave or overly cheery face,” said Ghosh Ippen. “But that can seem really odd and confusing. The child is feeling sad because it’s devastating that this person is gone, but then the parent is cheery ― which can feel eerie and weird.”
Ultimately, it’s about conveying the idea that “Mom is sad, and Mom is also strong,” she continued. If the feelings of grief become overwhelming, parents should seek help from other sources because it’s not their child’s role to help them.
“It’s important for little kids to believe that grown-ups are bigger, wiser and stronger,” said Ghosh Ippen. “We are not going to fall apart, and if we are going to fall apart, other grown-ups are going to help us.”
Nothing so alters a person as learning you have a terminal illness.
Ronni Bennett, who writes a popular blog about aging, discovered that recently when she heard that cancer had metastasized to her lungs and her peritoneum (a membrane that lines the cavity of the abdomen).
There is no cure for your condition, Bennett was told by doctors, who estimated she might have six to eight months of good health before symptoms began to appear.
Right then and there, this 77-year-old resolved to start doing things differently — something many people might be inclined to do in a similar situation.
No more extended exercise routines every morning, a try-to-stay-healthy activity that Bennett had forced herself to adopt but disliked intensely.
No more watching her diet, which had allowed her to shed 40 pounds several years ago and keep the weight off, with considerable effort.
No more worrying about whether memory lapses were normal or an early sign of dementia — an irrelevant issue now.
No more pretending that the cliche “we’re all terminal” (since death awaits all of us) is especially insightful. This abstraction has nothing to do with the reality of knowing, in your gut, that your own death is imminent, Bennett realized.
“It colors everything,” she told me in a long and wide-ranging conversation recently. “I’ve always lived tentatively, but I’m not anymore because the worst has happened — I’ve been told I’m going to die.”
No more listening to medical advice from friends and acquaintances, however well-intentioned. Bennett has complete trust in her medical team at Oregon Health & Science University, which has treated her since diagnosing pancreatic cancer last year. She’s done with responding politely to people who think they know better, she said.
And no more worrying, even for a minute, what anyone thinks of her. As Bennett wrote in a recent blog post, “All kinds of things . . . fall away at just about the exact moment the doctor says, ‘There is no treatment.’ ”
Four or five times a day, a wave of crushing fear washes through her, Bennett told me. She breathes deeply and lets it pass. And no, psychotherapy isn’t something she wants to consider.
Instead, she’ll feel whatever it is she needs to feel — and learn from it. This is how she wants to approach death, Bennett said: alert, aware, lucid. “Dying is the last great adventure we have — the last bit of life — and I want to experience it as it happens,” she said.
Writing is, for Bennett, a necessity, the thing she wants to do more than anything during this last stage of her life. For decades, it’s been her way of understanding the world — and herself.
In a notebook, Bennett has been jotting down thoughts and feelings as they come to her. Some she already has shared in a series of blog posts about her illness. Some she’s saving for the future.
There are questions she hasn’t figured out how to answer yet.
“Can I still watch trashy TV shows?”
“How do I choose what books to read, given that my time is finite?
“What do I think about rationale suicide?” (Physician-assisted death is an option in Oregon, where Bennett lives.)
Along with her “I’m done with that” list, Bennett has a list of what she wants to embrace:
Ice cream and cheese, her favorite foods. Walks in the park near her home. Get-togethers with her public affairs discussion group. A romp with kittens or puppies licking her and making her laugh. A sense of normalcy, for as long as possible. “What I want is my life, very close to what it is,” she explained. And deep conversations with friends. “What has been most helpful and touched me most are the friends who are willing to let me talk about this,” she said.
On her blog, she has invited readers to “ask any questions at all” and made it clear she welcomes frank communication.
“I’m new to this — this dying thing — and there’s no instruction book. I’m kind of fascinated by what you do with yourself during this period, and questions help me figure out what I think,” she told me.
Recently, a reader asked Bennett if she was angry about her cancer. No, Bennett answered. “Early on, I read about some cancer patients who get hung up on ‘why me?’ My response was ‘why not me?’ Most of my family died of cancer and, 40 percent of all Americans will have some form of cancer during their lives.”
Dozens of readers have responded with shock, sadness and gratitude for Bennett’s honesty about subjects that usually aren’t discussed in public.
“Because she’s writing about her own experiences in detail and telling people how she feels, people are opening up and relaying their experiences — things that maybe they’ve never said to anyone before,” Millie Garfield, 93, a devoted reader and friend of Bennett’s, told me in a phone conversation.
Garfield’s parents never talked about illness and death the way Bennett is doing. “I didn’t have this close communication with them, and they never opened up to me about all the things Ronni is talking about,” she said.
For the last year, Bennett and her former husband, Alex Bennett, have broadcast video conversations every few weeks over YouTube. (He lives across the country in New York City.) “What you’ve written will be valuable as a document of somebody’s life and how to leave it,” he told her recently as they talked about her condition with poignancy and laughter.
Other people may have very different perspectives as they take stock of their lives upon learning they have a terminal illness. Some may not want to share their innermost thoughts and feelings; others may do so willingly or if they feel other people really want to listen.
During the past 15 years, Bennett chose to live her life out loud through her blog. For the moment, she’s as committed as ever to doing that.
“There’s very little about dying from the point of view of someone who’s living that experience,” she said. “This is one of the very big deals of aging and, absolutely, I’ll keep writing about this as long as I want to or can.”
Why is my awareness here, while yours is over there? Why is the universe split in two for each of us, into a subject and an infinity of objects? How is each of us our own center of experience, receiving information about the rest of the world out there? Why are some things conscious and others apparently not? Is a rat conscious? A gnat? A bacterium?
These questions are all aspects of the ancient “mind-body problem,” which asks, essentially: What is the relationship between mind and matter? It’s resisted a generally satisfying conclusion for thousands of years.
Chalmers thought the mind-body problem should be called “hard” in comparison to what, with tongue in cheek, he called the “easy” problems of neuroscience: How do neurons and the brain work at the physical level? Of course they’re not actually easy at all. But his point was that they’re relatively easy compared to the truly difficult problem of explaining how consciousness relates to matter.
Over the last decade, my colleague, University of California, Santa Barbara psychology professor Jonathan Schooler and I have developed what we call a “resonance theory of consciousness.” We suggest that resonance – another word for synchronized vibrations – is at the heart of not only human consciousness but also animal consciousness and of physical reality more generally. It sounds like something the hippies might have dreamed up – it’s all vibrations, man! – but stick with me.
How do things in nature – like flashing fireflies – spontaneously synchronize?
All about the vibrations
All things in our universe are constantly in motion, vibrating. Even objects that appear to be stationary are in fact vibrating, oscillating, resonating, at various frequencies. Resonance is a type of motion, characterized by oscillation between two states. And ultimately all matter is just vibrations of various underlying fields. As such, at every scale, all of nature vibrates.
Something interesting happens when different vibrating things come together: They will often start, after a little while, to vibrate together at the same frequency. They “sync up,” sometimes in ways that can seem mysterious. This is described as the phenomenon of spontaneous self-organization.
When fireflies of certain species come together in large gatherings, they start flashing in sync, in ways that can still seem a little mystifying.
Lasers are produced when photons of the same power and frequency sync up.
The moon’s rotation is exactly synced with its orbit around the Earth such that we always see the same face.
Examining resonance leads to potentially deep insights about the nature of consciousness and about the universe more generally.
External electrodes can record a brain’s activity.
Sync inside your skull
Neuroscientists have identified sync in their research, too. Large-scale neuron firing occurs in human brains at measurable frequencies, with mammalian consciousness thought to be commonly associated with various kinds of neuronal sync.
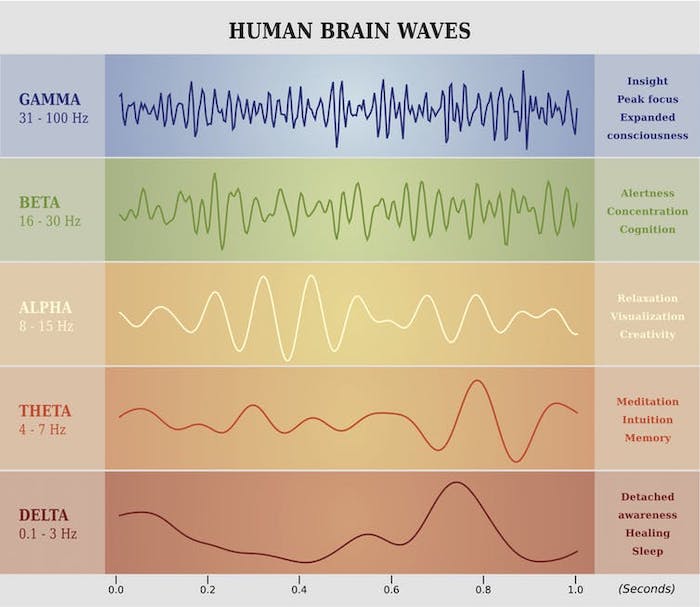
Fries focuses on gamma, beta and theta waves. These labels refer to the speed of electrical oscillations in the brain, measured by electrodes placed on the outside of the skull. Groups of neurons produce these oscillations as they use electrochemical impulses to communicate with each other. It’s the speed and voltage of these signals that, when averaged, produce EEG waves that can be measured at signature cycles per second.
Each type of synchronized activity is associated with certain types of brain function.
Gamma waves are associated with large-scale coordinated activities like perception, meditation or focused consciousness; beta with maximum brain activity or arousal; and theta with relaxation or daydreaming. These three wave types work together to produce, or at least facilitate, various types of human consciousness, according to Fries. But the exact relationship between electrical brain waves and consciousness is still very much up for debate.
Fries calls his concept “communication through coherence.” For him, it’s all about neuronal synchronization. Synchronization, in terms of shared electrical oscillation rates, allows for smooth communication between neurons and groups of neurons. Without this kind of synchronized coherence, inputs arrive at random phases of the neuron excitability cycle and are ineffective, or at least much less effective, in communication.
A resonance theory of consciousness
Our resonance theory builds upon the work of Fries and many others, with a broader approach that can help to explain not only human and mammalian consciousness, but also consciousness more broadly.
Based on the observed behavior of the entities that surround us, from electrons to atoms to molecules, to bacteria to mice, bats, rats, and on, we suggest that all things may be viewed as at least a little conscious. This sounds strange at first blush, but “panpsychism” – the view that all matter has some associated consciousness – is an increasingly accepted position with respect to the nature of consciousness.
The panpsychist argues that consciousness did not emerge at some point during evolution. Rather, it’s always associated with matter and vice versa – they’re two sides of the same coin. But the large majority of the mind associated with the various types of matter in our universe is extremely rudimentary. An electron or an atom, for example, enjoys just a tiny amount of consciousness. But as matter becomes more interconnected and rich, so does the mind, and vice versa, according to this way of thinking.
Biological organisms can quickly exchange information through various biophysical pathways, both electrical and electrochemical. Non-biological structures can only exchange information internally using heat/thermal pathways – much slower and far less rich in information in comparison. Living things leverage their speedier information flows into larger-scale consciousness than what would occur in similar-size things like boulders or piles of sand, for example. There’s much greater internal connection and thus far more “going on” in biological structures than in a boulder or a pile of sand.
Under our approach, boulders and piles of sand are “mere aggregates,” just collections of highly rudimentary conscious entities at the atomic or molecular level only. That’s in contrast to what happens in biological life forms where the combinations of these micro-conscious entities together create a higher level macro-conscious entity. For us, this combination process is the hallmark of biological life.
The central thesis of our approach is this: the particular linkages that allow for large-scale consciousness – like those humans and other mammals enjoy – result from a shared resonance among many smaller constituents. The speed of the resonant waves that are present is the limiting factor that determines the size of each conscious entity in each moment.
As a particular shared resonance expands to more and more constituents, the new conscious entity that results from this resonance and combination grows larger and more complex. So the shared resonance in a human brain that achieves gamma synchrony, for example, includes a far larger number of neurons and neuronal connections than is the case for beta or theta rhythms alone.
What about larger inter-organism resonance like the cloud of fireflies with their little lights flashing in sync? Researchers think their bioluminescent resonance arises due to internal biological oscillators that automatically result in each firefly syncing up with its neighbors.
Is this group of fireflies enjoying a higher level of group consciousness? Probably not, since we can explain the phenomenon without recourse to any intelligence or consciousness. But in biological structures with the right kind of information pathways and processing power, these tendencies toward self-organization can and often do produce larger-scale conscious entities.
Our resonance theory of consciousness attempts to provide a unified framework that includes neuroscience, as well as more fundamental questions of neurobiology and biophysics, and also the philosophy of mind. It gets to the heart of the differences that matter when it comes to consciousness and the evolution of physical systems.
It is all about vibrations, but it’s also about the type of vibrations and, most importantly, about shared vibrations.
The three sisters came to Lakeland Regional Health for what they thought would be a lecture.
Being retired educators, they’ve heard a lot of those.
Instead, they gathered in small groups to play a game with card-sized booklets and chips, laughing as they answered some questions asked and looking pensive as they thought about others.
“It gets to your emotions and thoughts,” said Janie Rambert, 61.
“You hear what other people have to say and it makes you think.”
Programs about advance directives, living wills and the like can come across as a thou-should-do-this talk.
Some may convey the benefits of those documents, but fall short at helping you start conversations about your wishes for medical care and support from family or friends if you become ill or incapacitated.
Colinette McGriff, 65, said she’d been holding back on having an advance directive or living will.
“I put it off because it seemed negative in a sense,” she said.
“The older I get, I think, ‘I should have done it years ago because I don’t want it on my kids.’”
Fewer than 4 in 10 people in the United States, about 37 percent, complete any kind of directives, concluded an analysis published in the July 2017 issue of Health Affairs.
How to make the numbers increase is a major goal of the Rev. Eileen Stone, a chaplain at Lakeland Regional; others involved in palliative care; and Lauren Springfield, manager of its community health program.
They invited members of Harmony Missionary Baptist and New Mt. Zion Missionary Baptist churches, along with community members, to the Hello Community Game Day held Sept. 29.
Middle sister Trudy Williams, 63, said she came hoping the program would “awaken me to my true feelings about how I actually feel.”
At the end, she and her siblings agreed, it helped achieve that.
“I’m going to discuss more with my husband and family about what I want to do and see how they feel about it,” Williams pledged.
They played “Hello,” a Common Practice conversation game. Participants write answers to questions and share their answers with others in their small groups.
Springfield and Stone called it “a game about living and dying and what matters most to each person.”
The teal-blue booklets in which they answered questions were for use with Project Talk, Conversations that Matter, a research program at Penn State Milton S. Hershey Medical Center.
The Hospice Foundation of America chose Lakeland Regional as one of 15 organizations to take part in research for a project the foundation is doing with Penn State Health.
People first wrote down any fears they may have had about playing the game and what they hoped to learn from it.
“I wanted to learn more about living wills and regular wills because we travel on the highway a lot,” Rambert said.
Then it was on to questions like what you would do if you knew you had three months to live, non-medical facts you would want a doctor to know about you; and who you would want to sing at your memorial service if you could choose anyone in the world.
Would you want your healthcare team to know your religious or spiritual beliefs?
Do you worry more about not getting enough care at the end of life or about getting too much?
What music do you want to be listening to on your last day alive?
Those were some of the questions in the booklets, which participants were able to take home.
There were no wrong answers. People could change their minds.
The chips given each person could be gifted to fellow participants for insightful, emotional and moving answers.
Not all questions got answered that day. The sisters, who taught in Polk County schools, said they plan to consider them further and talk about them with others.
Rambert, contacted Oct. 22, said she found her husband, Dwayne, more open to doing it than she was.
“You have to have someone there to keep you directed,” she said.
Springfield said she would like to help arrange other Hello game days at local religious institutions.
“People feel more comfortable coming to events at churches than they do at the hospital,” she said.
For some who are terminally ill, hastening their own death may be the answer.
By Samuel P. Harrington
Four months before he died, my father, a widower of six years and a hospice patient, asked me to discuss techniques for hastening his death, although he did not use that term: “I have lived too long. What can I do?”
He was living in Wisconsin where medical aid-in-dying, which allows terminally ill patients to obtain a lethal dose of medicine from a physician, was not legal. At first, I was afraid that he was asking me, a physician, to go around the law and supply him with a lethal dose of sedatives. Fortunately, he was not. He was dying of lymphoma and geriatric “failure to thrive” (old age), but it was a slow and unpleasant process. What could he do, he wanted to know, to move things along? He was ready
It was Christmas Day and I was cooking a few of my mother’s traditional dishes. Gradually, and recognizing the irony of simultaneously baking his favorite pie, I eased into a conversation about refusing to eat and drink. We had had this conversation in the past and it always ended the same way. Unlike most of my terminally ill patients, my father had not lost his appetite and would not give up the pleasure that food brought him.
The next day, he had come to decision: He would no longer take any medications designed to prolong his life, he announced to his family, caregivers and hospice nurses. These included heart pills, blood pressure pills and electrolyte supplements. He would, however, continue palliative medications, including tranquilizers and pain pills. My father died painlessly exactly four months later from the effects of multiple ministrokes.
According to the Center for Disease Control and Prevention, 90 percent of people over age 65 die of six chronic illnesses (heart failure, cancer, lung disease, stroke, dementia and diabetes). If I am fortunate enough to live to a ripe old age, I expect that I will suffer from one of these illnesses. If treatments are ineffective and a prolonged dying process is intolerable, perhaps I, like my father, will want to hasten my death.
As a doctor, I have found that having a sense of some control at the end can be reassuring to people. Yet it’s not easy — nor should it be — for someone to say, “I’m ready to be done with this,” and then have it be so.
In general, three ways are available where a terminally ill patient can speed up the process of dying without the assistance of someone else. One is by declining (or discontinuing) medical treatments that prolong life without improving the quality of life. Stopping his non-palliative medications was my father’s variation on this theme.
Another approach is to refuse to eat or drink. Known as voluntarily stopping eating and drinking, VSED (pronounced “V-said”) is an effective technique that takes advantage of the natural tendency for the terminally ill to lose their appetite to the disease process. This means that there are minimal hunger pains. Patients die of dehydration, which sounds bad but dehydration, by itself, is a pain-free condition. Most people have easily managed symptoms of thirst that stop as things progress. About 10 percent have significant, hard-to-manage symptoms of thirst. Most people slip into a coma in two to four days and pass away in 10 to 14 days.
The third approach is to take a lethal dose of medication. Medical aid-in-dying is legal in seven states and the District. The vast majority of terminally ill patients who choose to exit life this way slip into a coma in minutes and die painlessly within hours.
Having tended many terminally ill patients, I’ve often wondered what I would do if faced with a prolonged death from a chronic illness. If told I had less than six months to live, I would certainly enter hospice care, where the focus of doctors and other health-care professionals is on preserving quality — not quantity — of life. But then what?
Discontinuing or declining medical treatment includes everything from refusing life support or turning it off after a catastrophic stroke, infection or heart attack to discontinuing a pacemaker, a feeding tube or kidney dialysis.
It can also mean no antibiotics for a pneumonia or bladder infection in a bedbound hospice patient. Comforted by palliative treatments — narcotics and sedatives that induce comfort and sedation — any of these decisions will result in a comparatively comfortable death.
My quandary with this method for hastening death is that it relies on the random development of a disease or complication (stroke, infection or heart attack, for example). It is not a proactive strategy offering a better sense of control.
Medical aid-in-dying is proactive and it is effective. It is an option that I believe people should have available to them. Yet it comes with an unanticipated scheduling complication that gives me pause.
The laws allowing medical aid-in-dying are written to protect chronically ill patients from impulsive decision-making, coercion and premature deaths. Most require that patients themselves initiate the process; be certified by two physicians as terminally ill (defined as a life expectancy of less than six months) and mentally competent (without serious depression); undergo a two-week waiting period between the time of certification and acquisition of the medications; and remain mentally competent and physically capable of self-administration at the time of ingestion.
One woman I interviewed lives in Oregon, where medical aid-in-dying has been available for more that 20 years. Her story epitomized the scheduling conundrum.
When her husband was dying of rapidly progressive cancer, they scheduled a family gathering at which time he planned to take his lethal potion. One week before the event, progressive disease threatened his ability to self-administer the medication and they had to hurriedly reschedule with their children and the end-of-life volunteers who mix the medications and witness the process. One son could not reschedule. The wife felt rushed and disappointed that her son could not make it in time.
That scheduling artifice bothers me and supports the nagging sense of prematurity that I associate with many aid-in-dying deaths.
Yet if I lived in a state where it was available, I would consider it, particularly under two conditions: If I were suffering from poorly controlled pain or if I could not be kept clean because of uncontrollable incontinence. (I have seen this in men and women who have suffered complications from pelvic radiation, surgery or cancer itself.)
For me, under most circumstances, that leaves VSED. It cannot really be premature or impulsive. It accelerates the body’s natural decline. And it takes 48 to 96 hours of self-controlled commitment before the patient slips into a self-propagating coma. It would offer me control and demonstrate to my family that my death is appropriate and appropriately timed.
How I will face the final phase of my life is of course unknowable. But I am sure that a sense of control is the most important attribute of a good death and that advance care planning helps more patients achieve their end-of-life wishes.
I know that I do not want to be a burden on my family. I want my values and my legacy to be affirmed and appreciated. I want to be clean and comfortable. I want to optimize my relationships and bring closure to as many problems as possible. And I want my death to be appropriate in time and place.
To achieve all this requires discussions with doctors, family and friends. It also requires understanding one’s disease and likely prognosis and then deciding when to say “no” to aggressive treatment and when to say “yes” to hospice care.
These are not easy conversations or decisions. Yet to reach the peaceful end that most of us wish for, one might require a plan to hasten the process.
The sunrise burns off the morning mist over the remains of trenches in the Newfoundland Memorial Park at Beaumont Hamel on November 09, 2018 in Albert, France.
Despite growing up in a death-denying culture, place and time in Canada, pretty long past the days where dead bodies were openly displayed and waked at a family home instead of a funeral home, I have come as far as my 57th year (starting this week) with an openness to conversations about death and dying not normally heard among my peers.
There are many experiences that may have contributed to this. Perhaps being born in November, the Month of the Dead, just two days after Remembrance Day, had an impact. Being named after Ireland’s Deirdre of the Sorrows (not intentionally, my mom assures me) who is said to have died by suicide, perhaps by having her head smashed on a rock by the passing royal chariot (nice touch), may have played a part in my ability to banter about death more freely than others.
Becoming a Catholic, when I was 15, introduced me to ways of ritualizing death and praying for the dead just in time to help me cope with the deaths of seven of my high school peers in three separate car accidents and my stepbrother’s death by suicide a year later.
I also credit my love of excellent rock music for giving me a healthy outlook on death. Take Pink Floyd, for instance.
“And I am not frightened of dying, any time will do, I don’t mind. Why should I be frightened of dying? There’s no reason for it, you’ve gotta go sometime.”
Lying in bed (just like Brian Wilson did) as a teenager, falling asleep, high, with giant headphones blasting these lyrics into my brain, coupled with Trooper’s, “We’re here for a good time, not a long time,” has pretty much described my approach to death, and therefore life, or my approach to life, and therefore death.
It’s that approach, 14 years of parish ministry and more that I have been bringing to what’s called a “Social Innovation Lab.” In this case, the laboratory includes 25 or so palliative care clinicians, social activists, consumers, policy and system leaders, health care leaders and change agents from across Canada to concentrate for six solid days on one question: “How can we change the culture of our health system so the palliative approach, which creates a truly person-centred system, becomes the norm across the whole system?”
This “Palliative Care and Complexity Science Laboratory” is what brought me to be sitting in a circle of a dozen or so residents from a local seniors’ apartment building with three palliative care doctors, discussing monothanatophobia — the fear of dying alone. Although the word itself was brand new to me and all of the people who accepted our invitation to come and discuss it, the concept wasn’t.
We chose our topic after reading about the man who died alone in Hamilton’s social housing recently and went undiscovered for a couple of days before a woman below found some of his remains leaking into her apartment. Nobody wants that to be the story of their last days alive — or dead — on Earth.
There is strong evidence to show why we need to be more intentional about building community now and in the days ahead. Data about living situations from the 2016 Canadian census show for the first time that the number of one-person households has surpassed all other types of living situations. More than a quarter of all households were people living alone.
Applying the principles of palliative care means having conversations about living, not dying. It’s more than making sure community exists to support people in their final days of life. It’s also making sure people are connected while they’re living in a way that respects privacy yet decreases social isolation so no one dies alone.
One great read I recommend on the topic of death and dying is “Talking About Death Won’t Kill You,” by Dr. Kathy Kortes-Miller.
With an essential chapter for anyone on social media called, “Posting, Tweeting and Texting: Dying in a Digital World,” I urge you to make this a holiday gift to your family so you can “out” the conversation of death and dying to make it, as Kortes-Miller says, a logical extension of our living.”