[T]he Art of Natural Death Care raises awareness of an alternative way in which families can care for their loved ones at the time of death. The Sophia Center for Life Studies Crossings Care Community, along with many forward thinking people around the country, are bringing death care back to family and community. Natural home death care is legal, even without a funeral director in most states, and is an alternative to the conventional way in which death has been handled in the United States over the last century. This growing movement of home funeral and green burial care is driven by the belief that this way can be more meaningful, affordable, and environmentally friendly. Families can care for their loved ones at the time of death bringing individuality, sacredness, love and reverence. The Art of Natural Death Care can help get the conversation started about end of life choices.
The Sophia Center for Life Studies would like to thank filmmaker Katelyn LaGrega for donating her time and energy and dedicating her heart and soul in creating this film. We believe that this film can serve individuals and organizations across the country who are dedicated to educating about Natural Death Care options. We are passionate about this work and encourage the use and sharing of this film to support this movement and raise awareness. Donations for the creation and production of this film can be made HERE!
[M]irrors reflect the truth of what strikes their surface. The eyes of a dying patient are the clearest mirrors I have ever known. In their gaze, there is simply no place to hide. Over the years, the habits of my life have been reflected in those eyes.
Once while washing the back of a hospice patient named Joe he turned toward me and said, “I never thought it would be like this.” I asked what he had thought it might be like. He answered, “I guess I never really thought about it.” Death had taken him by surprise. Perhaps we are not so different.
In the sacred, Hindu epic poem the Mahabharata there is a question that speaks to this tendency. “In all of the worlds what is most wondrous?” The answer that is given is; “That no man no woman though they see people dying all around them believes it will happen to them.”
We make an enormous effort to keep death at arms-length. We spend more than 50% of our healthcare dollars in the final six months of life, literally throwing money at death. We shut away our elders in nursing homes to avoid confronting their pain and our destiny. We have a multi-billion-dollar cosmetics industry that tries to keep us all looking young. We even put rouge on people in the coffin.
Death is the fulcrum issue of our life and yet we can barely use the word. People don’t die they “pass away” or they “expire” like credit cards. We make plans for all sorts of activities; when to get married, the number of children we will have, where to go on vacation, which career moves to make or how we will spend our retirement—all of which may never happen. But death, the one event that is certain to occur, barely receives a sidelong glance.
Dying is at its heart a sacred act; it is itself a time, a space, and process of surrender and transformation. The sacred is not separate or different from all things, but rather hidden in all things. Dying is an opportunity to uncover what is hidden.
Walking the gauntlet of thirty beds on the long single hospice ward at Laguna Honda Hospital, I noticed Isaiah out of the corner of my eye. An African-American man raised in Mississippi, Isaiah was actively dying. His breathing was labored, and he was sweating up a storm. I sat down next to him.
“You look like you’re working really hard,” I said.
Isaiah raised his arm, pointed to the distance, and said, “Just gotta get there.”
“I forgot my glasses. I can’t see that far in the distance. Tell me what you see.”
Isaiah described a bright green pasture and a long hill leading to a grassy plateau.
I asked, “If I promise to keep up, can I come?”
He grabbed my hand tight, and Isaiah and I started climbing together. His breathing got shorter, and he perspired more with every step. It was a long walk. Not an easy one.
“What else do you see?” I asked.
He described a one-room red schoolhouse with three steps leading up to a door.
My training informed me that Isaiah was disoriented to time and location. I could have told the old man that his visions were likely being caused by brain metastasis and morphine. I could have reminded him that we were in a ward at Laguna Honda Hospital. But that was only true on the most superficial level.
The deeper truth was that we were walking to a little red schoolhouse.
I asked, “Do you want to go in?”
Isaiah sighed. “Yeah. I’ve been waitin’.”
“Can I go with you?” I asked.
“Nope.”
“Okay, then, you go,” I said.
A few minutes later, Isaiah died quite peacefully.
The great spiritual and religious traditions have any number of names for the unnamable: the Absolute, God, Buddha Nature, True Self. All these names are too small. In fact, all names are too small. They are fingers pointing at the moon. I invite you to connect with what you know and trust most in your heart of hearts.
I use the simple term Being to point at that which is deeper and more expansive than our personalities. At the heart of all spiritual teachings is the understanding that this Being is our most fundamental and benevolent nature. Our normal sense of self, our usual way of experiencing life, is learned. The conditioning that occurs as we grow and develop can obscure our innate goodness.
Some part of us, deep in our hearts has known this truth. If not, we would not long for a return to it. And this part of our being knows that we will never be satisfied until our whole being is immersed in this oneness.
In 2016, the first year health-care providers were allowed to bill for an end-of-life consultation, nearly 575,000 Medicare beneficiaries took part in the conversations, new federal data obtained by Kaiser Health News show.
[T]he 90-year-old woman in the San Diego-area nursing home was quite clear, said Dr. Karl Steinberg. She didn’t want aggressive measures to prolong her life. If her heart stopped, she didn’t want CPR.
But when Steinberg, a palliative-care physician, relayed those wishes to the woman’s daughter, the younger woman would have none of it.
“She said, ‘I don’t agree with that. My mom is confused,’ ” Steinberg recalled. “I said, ‘Let’s talk about it.’ ”
Instead of arguing, Steinberg used an increasingly popular tool to resolve the impasse last month. He brought mother and daughter together for an advance care-planning session, an end-of-life consultation that’s now being paid for by Medicare.
In 2016, the first year health-care providers were allowed to bill for the service, nearly 575,000 Medicare beneficiaries took part in the conversations, new federal data obtained by Kaiser Health News shows.
Nearly 23,000 providers submitted about $93 million in charges, including more than $43 million covered by the federal program for seniors and the disabled.
Use was much higher than expected, nearly double the 300,000 people the American Medical Association projected would receive the service in the first year.
That’s good news to proponents of the sessions, which focus on understanding and documenting treatment preferences for people nearing the end of their lives. Patients, and often, their families, discuss with a doctor or other provider what kind of care they want if they’re unable to make decisions themselves.
“I think it’s great that half a million people talked with their doctors last year. That’s a good thing,” said Paul Malley, president of Aging with Dignity, a Florida nonprofit that promotes end-of-life discussions. “Physician practices are learning. My guess is that it will increase each year.”
Still, only a fraction of eligible Medicare providers — and patients — have used the benefit, which pays about $86 for the first 30-minute office visit and about $75 for additional sessions.
Nationwide, slightly more than 1 percent of more than 56 million Medicare beneficiaries who enrolled at the end of 2016 received advance-care planning talks, according to calculations by health-policy analysts at Duke University. But use varied widely among states, from 0.2 percent of Alaska Medicare recipients to 2.49 percent of those enrolled in the program in Hawaii.
“There’s tremendous variation by state. That’s the first thing that jumps out,” said Donald Taylor Jr., a Duke professor of public policy.
In part, that’s because many providers, especially primary-care doctors, aren’t aware that the Medicare reimbursement agreement, approved in 2015, has taken effect.
“Some physicians don’t know that this is a service,” said Barbie Hays, a Medicare coding and compliance strategist for the American Academy of Family Physicians. “They don’t know how to get paid for it. One of the struggles here is we’re trying to get this message out to our members.”
There also may be lingering controversy over the sessions, which were famously decried as “death panels” during the 2009 debate about the Affordable Care Act. Earlier this year, the issue resurfaced in Congress, where Rep. Steve King, R-Iowa, introduced the Protecting Life Until Natural Death Act, which would halt Medicare reimbursement for advance-care planning appointments.
King said the move was financially motivated and not in the interest of Americans “who were promised life-sustaining care in their older years.”
Proponents like Steinberg, however, contend that informed decisions, not cost savings, are the point of the new policy.
“It’s really important to say the reason for this isn’t to save money, although that may be a side benefit, but it’s really about person-centered care,” he said. “It’s about taking the time when people are ill, or even when they’re not ill, to talk about what their values are. To talk about what constitutes an acceptable versus an unacceptable quality of life.”
That’s just the discussion that the San Diego nursing-home resident was able to have with her daughter, Steinberg said. The 90-year-old was able to say why she didn’t want CPR or to be intubated if she became seriously ill.
“I believe it brought the two of them closer,” Steinberg said. “Even though the daughter didn’t necessarily hear what she wanted to hear. It was like, ‘You may not agree with your mom, but she’s your mom, and if she doesn’t want somebody beating her chest or ramming a tube down her throat; that’s her decision.’ ”
Stacie Alves and Dr Julia Spade administer acupuncture and laser therapy to a dog with arthritis. Last Wishes has assisted more than 5,000 families with their petâs care since November 2012. Earlier this year, the organization opened the first compassionate comfort care center for pets in Houston. The center features comfort rooms that are used for hospice and pain management consultations, therapeutic laser, acupuncture, and compassionate sedation-euthanasia.
By Vagney Bradley
People and their pets can build a strong bond together, and losing a pet can be difficult. When a pet becomes terminally ill, Last Wishes, Houston’s first pet hospice service, steps in to take care of a geriatric pet, from moment of diagnosis through death and aftercare.
Dr. Christie Cornelius is the owner and veterinarian of Last Wishes. She also co-owns Earthman Last Wishes, Texas’ first water-based cremation service for pets. Cornelius and her associate, Dr. Julia Spade, will become the first two veterinarians in the state of Texas to become certified in Veterinary Hospice and palliative care in October.
“I started imagining a better way to offer end of life services after a few years of general practice. I saw how difficult it was for pet owners to bring in their painful or otherwise ailing companions into an unfamiliar, sterile, noisy, scary environment for euthanasia,” Cornelius said.
“I started offering home services through a feline practice I was working for at the time and found it extremely rewarding to be able to provide a peaceful passing for a pet in their own environment, surrounded by loved ones. As the years went by, I convinced myself there was a real need and desire for this type of service in our community.”
In 2012, Cornelius branched out and started Last Wishes while working full time at another veterinary clinic.
Last Wishes has assisted more than 5,000 families with their pet’s care since November 2012. Earlier this year, the organization opened the first compassionate comfort care center for pets in Houston. The center features comfort rooms that are used for hospice and pain management consultations, therapeutic laser, acupuncture, and compassionate sedation-euthanasia.
Cornelius’ goal is to help educate the community about pet hospice, comfort care, pain management, and gentle water-based aftercare services for pets.
Dr Christie Cornelius and assistant Betty Rose Bryant perform an exam on a dog.
Some of the common conditions the organization works with includes, but are not limited to, cancer, heart disease, liver disease, osteoarthritis, organ failure, cardiovascular and neurological disease, and vestibular disease.
“Last Wishes is unique in that we want to make the most of the time that every pet has left with their family. Our doctors and staff don’t just focus on making euthanasia as comfortable as possible when it is ultimately needed,” Spade said. “Our expertise in multiple forms of hospice techniques allows us to consider what is truly beneficial for each case and help strengthen the bond between the pet and their family.”
The majority of services are done in the comfort of the family’s home and in the pet’s environment. Services at the center include consultations, acupuncture, laser, sedation-euthanasia, pet loss support groups, and aftercare. Last Wishes also provides pet loss support groups and continuing education.
“We have established a network of providers, such as our very own grief counselor, pet sitters, pet groomers, and volunteers set up to meet all of our patients and family’s needs when it comes to providing care for an ailing pet diagnosed with a terminal disease,” Cornelius said. “In addition, we sponsor twice monthly pet loss groups and host a private Facebook pet loss support page.”
Additionally, the organization assists disadvantaged families and individuals with their pet’s end of life care through the Last Wishes Fund, a non-profit organization funded by public donations.
Last Wishes provides provide a folder of pet loss/grief information for each family, a clay paw print memorial keepsake, and gentle transport of the pet for aftercare services from the client’s home.
“It is such an honor to be invited into the homes and lives of the families of Houston,” said Jennifer Rames, Last Wishes office manager. “While euthanasia is never easy, we feel honored to provide our services so that these precious furry family members can pass with dignity, in the place they feel safest and happiest, and surrounded by the people who love them the most.”
Cornelius and grief counselor, Marilyn Ladin, are developing a pet loss support program. The program offers in-person and online individual and group therapy.
“Our goal is to heal some long-broken hearts,” Cornelius said. “We also aspire to help other veterinarians and veterinary staff struggling with compassion fatigue, depression, and anxiety among other issues. Too many of our colleagues are causing their own deaths.”
This month Last Wishes plans to unveil of a public pet memorial gardens in Cypress. The garden will include four gardens and handmade stepping stones as a tribute to the pets the organization has helped. The memorial will also feature a special Rainbow Bridge. Families will have access to the garden on Sunday mornings as an opportunity to visit their pet in a peaceful and natural setting.
Making death masks of notorious criminals was common in the 19th century, such as this cast of murderer William Burke at the University of Edinburgh’s Anatomy Museum.
[T]hese days many people know they are dying long before death finally arrives. Yet death, a natural event, is often seen as a failure of medicine. Despite the additional time modern healthcare may provide us, we still begin our conversations about the wishes of the dying and their families too late – or not at all. This reluctance to accept our own mortality does not serve us well.
This taboo around death is a fairly modern, Western phenomenon. Past and present, societies have dealt with death and dying in diverse ways. It is clear from, for example, the outpouring of grief at Princess Diana’s death, and the conversations opening up around the 20th anniversary of the event, that these outlets are needed in our society too. High-profile celebrity deaths serve as sporadic catalysts for conversations that should be happening every day, in everyday lives.
Recent bereavement theory has moved on from thinking of grief as a series of stages, to a continuous process in which the bereaved never fully return to some “pre-bereaved” status quo. It is increasingly recognised that the living form various sorts of continuing bonds with the dead, as put forward by the sociologist Tony Walter and psychologist Dennis Klass and colleagues – and this is certainly something that can be seen in death practices today across the globe, and among those practised in the past.
In Neolithic Turkey, one funerary rite included the creation of plastered skulls – family members were buried under the floors of their house and after some time the skull was removed and a plaster face lovingly recreated over it. Many of these plastered skulls show evidence of wear and tear, breakage and repair, suggesting that they were used in everyday life, perhaps displayed and passed around among the living. Similarly, in modern-day Indonesia, the dead are kept in houses, fed and brought gifts for many years after death. While in this state they are considered to be ill or asleep – in this case their biological death does not entail social death.
It was not so long ago in the UK that public outpouring of grief and practices that kept the dead close were acceptable. For example, in Victorian England, mourning clothes and jewellery were commonplace – Queen Victoria wore black for decades in mourning for Prince Albert – while keeping tokens such as locks of hair of a deceased loved one were popular.
However, today death has been outsourced to professionals and, for the most part, dying happens in hospitals or hospices. But many doctors and nurses themselves feel uncomfortable with broaching the subject with relatives. Perhaps there are lessons to be drawn from the attitudes of others far removed from us in time and space: the past, and societies on the other side of the globe, are easier to discuss, yet act as prompts to help us discuss more personal experiences.
The Continuing Bonds Project brings together healthcare practitioners and archaeologists at the University of Bradford and LOROS Hospice in Leicester to explore what we can learn from the past, using archaeology to challenge modern perceptions of and attitudes towards death and dying, and as a vehicle through which people can discuss their own mortality and end-of-life care.
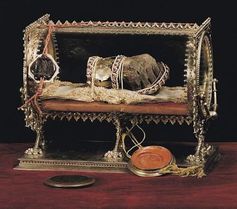
Hungary which has been on display since 1038. Though saints’ relics – generally body parts – have been a large part of Christian culture in the past and were not uncommon, they are something many are uncomfortable with today. One workshop participant describes the display of St Stephen’s hand as “selfish”, as if he is being exploited beyond the grave. What responsibilities do we have towards the dead? What constitutes “respect” for them? Archaeology shows us that it is a fluid and culturally embedded concept which differs wildly between societies and individuals.
Memorialisation, through photographs or statues (that served the same purpose in the past), appears to be fundamental to “respectful” treatment of the dead. Death masks – plaster castings of a dead person’s face – and later even photos of the recently departed, were not uncommon as a way to memorialise the dead, even into the 20th century. Yet while taking photographs of the departed in life are celebrated, photographs of dead bodies themselves are less palatable today.
The vast stone bust of Ramses II in the British Museum.
Another example for workshop participants is the statue of the Egyptian pharaoh Ramesses II, the bust of which
resides at the British Museum, while the feet remain in situ at the Ramesseum in Luxor, Egypt. Given that this individual lived in Egypt nearly 3,000 years ago, the statue has kept his memory alive. Yet its fragmented and dispersed nature prompted our participants to wonder how long their loved ones’ memories of them would persist after their death, and what legacies they would want to leave.
101 uses for mortal remains
Memorialisation of the dead takes a very different form at the 16th-century Capela dos Ossos in Évora, Portugal, where monks desiring to save the souls of some 5,000 people from overcrowded local cemeteries used their remains to create a chapel of bones. Individual bones were used to create decorative features such as arches and vaulted ceilings.
Workshop participants were unhappy that bones had been removed from their resting place without the permission of the deceased. But for how long can our wishes be accommodated after death? The other feature that unsettled them was the dismantling of the skeletons – in the West today, our identity sits firmly with us as individuals, bounded by our physical bodies. Fragmenting our skeletal remains strikes firmly at this sense of identity – and so our sense of social presence. Such scattered remains are nameless, faceless – lacking the very thing that memorials seek to preserve.
In other cultures – and in the past – identity is less individualistic and resonates within larger kin or community groups. Here, distributing bones may be less problematic and a part of the process whereby the recently deceased joins the host of communal ancestors.
‘Nice chapel, I love what you’ve done with the space.’
Though some of the topics were difficult to discuss, many workshop participants felt they had improved confidence in talking about death, dying and bereavement as a result. The range of practices from the past reminds us of the diverse ways through which death can be negotiated and the extent to which practices that we take for granted today are in fact culturally embedded, relative and subject to change. Persistent Facebook profiles of dead friends and family to which loved ones post on each anniversary are an example of how traditions are changing.
In a world where death has become increasingly outsourced and medicalised, the diverse ways we treated and remembered our dead in the past should highlight the choices available to us and prompt us to consider those now banned or taboo. At the entrance of the Capela dos Ossos, the monks who built the chapel left an inscription, a momento mori that reminds us: “We bones that are here, for yours await”.
The Bios Urn mixes cremains with soil and seedlings. It automatically waters and cares for the memorial sapling, sending updates to a smartphone app.
By Glenn McDonald
[E]arlier this summer, a modest little startup in Barcelona, Spain, unveiled its newest product — a biodegradable, Internet-connected funeral urn that turns the ashes of departed loved ones into an indoor tree. Just mix the cremains with soil and seedlings, and the digital-age urn will automatically water and care for your memorial sapling, sending constant updates to an app on your smartphone.
At first glance, the concept seems gimmicky — evidently, we’re running out of ideas for smart appliances. But the Bios Incube system can also be seen as the latest example of a gradual transformation in modern culture.
Technology is fundamentally changing how we deal with death and its attendant issues of funerals, memorials and human remains. Much of this change is for the good. Some developments are a little spooky. But one thing is for sure: You can do a lot of cool things with ashes these days.
</center.
The Bios Incube system, which went on sale in June after a successful crowdfunding campaign, is the latest iteration of a much older idea in which ashes are essentially used as compost for a memorial tree or plant. But the Incube system adds some high-tech twists. The biodegradable urn is placed within a 5-gallon planter with an elegant, off-white, minimalist design vibe — call it the iUrn.
Roger Moliné, co-founder of Bios Urn, says the company offers two versions of its system. One provides the basic biodegradable urn and planter at $145. The more expensive version — if you want all the high-tech bells, whistles, atmosphere sensors and smartphone apps — tops out at $695.
“Interestingly enough, we have found so far that most have opted voluntarily for the high-tech option,” Moliné says.
He has a theory on that.
“Most of us are connected to the digital world, and we have become used to it,” he says. “Perhaps by tying together this process with technology, there can be a sense of comfort that comes from using a familiar process with a new experience. We hope that it will push people in a new direction and perhaps make this process easier for those experiencing loss.”
The Bios Urn is part of a high-tech system in which the ashes of a departed loved one are used to help grow a tree.
The Bios Urn concept is indeed part of a larger transformation in which technology is changing how we think about death and dying, says Candi Cann, author of the book Virtual Afterlives: Grieving the Dead in the Twenty-first Century.
“Their approach implies a different sort of afterlife than the religious one — an afterlife that theoretically we can partake in,” says Cann, who teaches religion and world culture at Baylor University.
“Recent theories on mourning reveal that having continued bonds with the deceased allow us to navigate everyday life while renegotiating our relationships with loved ones who are no longer present,” she says. “So in this way, the Bios Urn might actually foster a healthy type of mourning that allows us to look after the dead in an active, daily way.”
Caring for the dead via a smartphone app may seem strange, Cann says, but it makes perfect sense for those of us living in a perpetually connected world: “The generation today has grown up with online spaces and smartphones, so this is their medium.”
Cann has done extensive research on modern mourning rituals around the planet, and the various ways that technology is impacting how we deal with death and dying. The Internet has certainly changed the way we do things. Obituaries are posted online, funeral arrangements are sent by email or text, and social media platforms like Facebook now offer a range of memorial pages and legacy contact options.
In general, this is all good healthy progress, Cann says. “Smartphones and social media spaces have forced a decline in the importance of a controlled obituary narrative, as more people can contribute to the communal memory of a person and the meaning of their life,” she says.
A recurring theme in Cann’s work concerns an odd and abiding reticence in mainstream Western attitudes toward death: In short, we just don’t like to talk about it. Our aversion leads to a lot of unhealthy sublimation in the culture. “I would argue that the reason we see so much death in the media and in video games is precisely because we are not having real conversations about death,” Cann says.
Technology is helping in that arena, too. Cann points to online communities like Death Cafe, which use Internet forums to arrange local meetups for people wanting to talk about death.
Then there is the issue of what to do with the remains. We humans have been navigating this dilemma since the dawn of civilization, but recent technological advances have opened up some options. You can have ashes incorporated into jewelry, blended into oil paintings, mixed into tattoo ink, submerged into coral reefs or even pressed into vinyl records. And don’t forget about the festive fireworks option.
While developing the Bios Urn system, Moliné explored how other cultures are processing cremains, like Tokyo’s unique Ruriden columbarium, which utilizes LED Buddha statues and digital smart cards.
The Ruriden columbarium houses futuristic alters with glass Buddha statues that correspond to drawers storing the ashes of the deceased.
“I’ve seen some interesting things in China and Japan,” he says. “Both have run of out burial space in larger cities and have created interesting ways of commemorating those who have passed.”
Cann says that these new modern rituals, facilitated by various technologies, can help us get a little friendlier with death.
“In Brazil, I went to a public crematorium that cremates a body every 15 minutes, and is an actively used public park and picnic space,” he says. “Families were playing and picnicking among the ashes. If we see deathscapes as friendly places, rather than where the dead are banished, we might be able to utilize them in healthier and more creative ways.”
Looking to the future, however, Cann addresses more worrisome technologies.
“One of the areas I’m thinking more about is the use of artificial intelligence and digital avatars,” Cann said. “These are people intending to upload themselves, via AI, into digital avatars.”
Proponents of this idea contend that uploading the mind into a computer is entirely plausible. But science fiction has some cautionary tales in this area — any technology that promises to defy death is usually nothing but trouble. Ask Dr. Frankenstein. Even speculating on this sci-fi scenario can get a bit dodgy, Cann says.
“Whenever people focus more on extending life rather than examining its quality, death loses its importance,” Cann says. “If we are spending more time trying to deny death or prolong dying, then I think we are not living well.”
In this light, the Bios Urn seems like a fairly gentle step forward. Technology can’t yet provide us with digital immortality, but it can help us grow a memorial tree in our living room. What’s not to like?
Death is often a taboo subject, so when death anxiety comes into play, it is hard to know how to face it.
By Maria Cohut
[D]eath is something that we all, sooner or later, have to face. But how do we respond to it? Why are some of us more afraid than others? And what is it, exactly, that scares us about death? We offer an overview of theories related to death anxiety, and what you can do to address it.
To a greater or lesser extent, it is likely that we are all scared of death – whether it be the thought of our own cessation or the fear that someone we love might pass away. The thought of death is not a pleasant one, and many of us avoid such morbid musings, naturally choosing to focus on what life has to offer, as well as on our own wishes and goals, instead.
Yet, as Benjamin Franklin once famously wrote, “In this world nothing can be said to be certain, except death and taxes,” so it is no surprise that death-related worries sometimes take us by storm.
Fear of death is sometimes referred to as “thanatophobia,” deriving from the Ancient Greek words “Thanatos,” the name of the god of death, and “phobos,” meaning “fear.”
Notably, thanatophobia – which is called “death anxiety” in a clinical context – is not listed as a disorder in its own right in the Diagnostic and Statistical Manual of Mental Disorders. Still, this rarely spoken-about anxiety has the potential to seriously affect people’s lifestyles and emotional health.
Thanatophobia: Natural or trauma-driven?
Thanatophobia was first tackled by Sigmund Freud, who did not consider it to be fear of death, as such. Freud thought that we cannot truly believe in death as a real occurrence, so any death-related fears must stem from unaddressed childhood trauma.
But it was the theory put forth a little later by an anthropologist called Ernst Becker that ended up informing most current understandings of death anxiety and its causes. Becker believed that death anxiety comes naturally to all people who find the thought of death and dying unacceptable.
That is why, he argued, everything everyone does – the goals we set, our passions and hobbies, and the activities we engage in – is, in essence, a coping strategy, and that these are things we focus on so we that need not worry about our eventual death.
Becker’s work gave rise to “terror management theory” (TMT), which posits that humans must constantly deal with an internal conflict: the basic desire to live against the certainty of death. TMT emphasizes individuals’ self-consciousness and their drive to achieve personal goals, motivated by the awareness of mortality.
Also, according to TMT, self-esteem is key for the degree to which individuals experience death anxiety. People with high self-esteem are better at managing fear of death, while people with low self-esteem are more easily intimidated by death-related situations.
Some newer approaches suggest a “middle way” between TMT and another theory referred to as “separation theory,” which highlights the importance of early trauma, reinforced by an awareness of mortality later in life.
Another recent approach to understanding and explaining death anxiety is that of “post-traumatic growth theory” (PTG). According to PTG, going through a distressing event – such as the death of a loved one or receiving a worrying health diagnosis – can actually have a positive effect, causing individuals to appreciate the small things in life a lot more, or to become more goal-oriented.
Death anxiety as a disorder
Although it is likely that we will all be worried about death or a death-related situation at some time in our lives, death anxiety is only pathological when it reaches extreme levels, disrupting the normal lifestyle of an individual.
One account of death anxiety – as reported by a man’s worried wife – emphasizes how this kind of fear can become obsessive and get out of control.
“The fear is specifically of death (not pain or dying as such) and the emptiness of it (he’s not religious) and the fact that he will no longer be here. […] this is an irrational, emotional fear that he has trouble controlling. Recently it has got worse – he’s not sure why – but it has made him feel panicky and the thoughts have been straying into the daytime.”
Who is afraid of death?
Dr. Robert Kastenbaum has reviewed various psychology theories and studies related to the concept of death, outlining which populations are most likely to express a persistent fear of death. Drs. Patricia Furer and John Walker summarize the findings in an article published in the Journal of Cognitive Psychotherapy.
Women are more likely than men to experience death anxiety, and this tends to peak twice: once in their 20s and again in their 50s.
The majority of individuals are afraid of death. Most people tend to fear death, but they usually only exhibit low to moderate levels of anxiety.
Women tend to be more afraid of death than men. Additionally, a newer study has found that while death anxiety seems to surface in both women and men during their 20s, women also experience a second surge of thanatophobia when they reach their 50s.
Young people are just as likely to experience death anxiety as elderly people.
There appears to be some correlation between a person’s educational and socioeconomic status and reduced death anxiety.
No association has been found between religious engagement and reduced death anxiety.
Other studies show that people exhibiting health anxiety, or hypochondriasis, are also affected by death anxiety, as it naturally correlates with an excessive worry about health.