Filmmaker Sam Green was just about to fly out of Columbus, Ohio when his friend offered to make a quick detour. “She asked if I wanted to see a little pet cemetery that’s across the street from the airport,” Green told The Atlantic. Armed with his camera, Green captured the tombstones of a menagerie of dearly departed animals, some dating back to the early twentieth century. His short film, Julius Caesar was Buried in a Pet Cemetery, featuring an original score from Yo La Tengo, showcases the pets’ final resting place—and the human love they once inspired.
Green said that he finds graveyards for pets especially moving because the headstones tend to be much more emotive than those found in human cemeteries. “You can say, ‘Buster was the best parakeet who ever lived,’” said Green. “With human graves, everything is so much more constrained. People love their animals in such an intense way and are able to express that love in a much freer way than they can about people they’ve lost.”
“You have gone and left such emptiness that time can never fill,” reads a grave for a dog named Jiggs Boy, who died in 1933.
People left their seats to dance and sing along to a live performance of “Mustang Sally” while servers waited in the next room, poised with champagne and chocolate-covered strawberries.
This was not your typical funeral.
Hundreds of family, friends, and members of the public turned out for Audrey Parker’s celebration of life.
Audrey Parker wanted her friends and family to be uplifted by the ceremony and so she planned every detail with that aim before she died on Nov. 1.
“She planned it and she knew that when we walked out of here today we would remember that life is supposed to be a celebration. This is a celebration of life, not just Audrey’s but all of ours,” said her friend Nancy Regan, the master of ceremonies.
Several hundred people gathered at Pier 21 on Friday afternoon to commemorate Parker, the 57-year-old Halifax woman who chose to die with medical assistance as she faced a terminal cancer diagnosis.
Many of the speakers mentioned how popular Parker was, with a large and adoring group of friends and a close-knit family who made up much of the crowd. But the ceremony was also open to the public, who came to know Parker in the final months of her life as she advocated for change in Canada’s assisted dying legislation.
Parker left two legacies: one for the people who knew her and were inspired by her exuberant kindness and another for those in the public who were spurred to take a closer look at a complex law.
“I’m gonna get a little political now, because I want to talk about Aud’s legacy,” said her friend Kimberley King, the last of seven speakers at Friday’s ceremony.
“Audrey knew that she wanted to be a spark, but she never imagined she’d be a national advocate,” King said.
Parker was diagnosed with Stage 4 breast cancer in 2016 and as her illness progressed she experienced excruciating pain from tumours in her bones. She was approved by a doctor for medical assistance in dying (MAID), but as it stands, the law stipulates that patients must give late-stage consent.
It’s a safeguard that’s meant to protect people in a vulnerable state — such as when their physical health and mental faculties may be failing — but Parker said that in her circumstance, all it did was cut her life even shorter.
“I really wish that we had her this Christmas,” said her stepdaughter, Lucie MacMaster, after reflecting at Friday’s ceremony on past holidays they’d shared.
“But here we are,” she added.
Parker chose Nov. 1 for her final day because she knew that she would still be able to give the necessary late-stage consent. The cancer has recently spread to the lining of her brain, and she worried that if she waited much longer, the opportunity would be lost.
Before she died, Parker called on Ottawa to amend MAID so that people like her could give advance consent for their own death. It could not be amended in time for her, but she asked the public to keep pushing for the change.
“She did her part, and now it’s our turn. In Audrey’s honour and memory, I ask you to continue to support her movement. We have an opportunity to amend a federal law so that people who are invoking MAID don’t need double consent and therefore don’t need to die early like our Audrey did,” said King.
Local MLA Darren Fisher has said he’d like to see the legislation go “a little bit further,” but Justice Minister Jody Wilson-Raybould disagreed, telling reporters the day after Parker’s death that there were no plans to change the two-year-old law.
Parker’s friend Robert Zed announced on Friday that there will soon be a permanent memorial for Parker in Halifax’s Point Pleasant Park. A steel bench is to be installed on Monday, facing out toward the water on Sailors Memorial Way.
Mom’s terminal cancer diagnosis took her by surprise. “I always thought I would just fall over dead while I was walking across the backyard,” she told me. “Not me,” I responded. “I’m planning to go out like Uncle Ernest: Go to bed healthy and wake up dead. I think it’s called cardiac arrest.”
We were sitting at Mom’s kitchen table, trying to pretend everything was OK. A few years earlier, Mom had flitted away “a little bit of cancer,” as she called it, with a lumpectomy carefully timed so she did not miss her volunteer gigs. But we knew that this time — two cancers and increasing shortness of breath — was going to be different.
We tried to focus on the peach cobbler in our bowls. In our minds, though, we were coming to grips with the fact that we had fooled ourselves.
Mom and I thought of ourselves as great planners. Our pantries always well-stocked; the menu always worked out weeks before the big family dinner; a hundred-dollar bill always tucked in the sock drawer, just in case.
Mom’s End-of-Life Plan
Mom’s end-of-life plan was to die quickly. It turns out that is not a plan; it’s a hope. And the difference proved terribly sad when it came to the living will she’d prepared (a living will is an advance directive spelling out your desires regarding medical treatment if you’re no longer able to express them).
Like every good planner, Mom had a Plan B if she didn’t get the sudden death she was counting on. She was such an enthusiast for having a living will that I teased her about handing out copies like they were campaign flyers. When she turned 65 or thereabouts, she presented a copy to each of us four kids, her siblings and her doctor, along with a warning that “if you keep me alive on machines, I’ll come back to haunt you.”
That made us laugh. Mom was as threatening as a worn-out quilt. And after Dad died, when they were both in their mid-50s, she devoted the next three decades to making other people’s lives easier. She was a cookie-baking grandma happy to babysit on five minutes notice; the lady who made hash brown casseroles for bereavement dinners at her church.
Mom’s Living Will
Looking back, I wonder where she got all those copies of her living will. In my mind’s eye, I see her — super-white tennis shoes and polyester slacks — standing next to the copy machine at the library, fishing dimes out of her coin purse, while a young library intern pushed the button. “I better get a couple more copies, if you don’t mind. My kids lose things like you wouldn’t believe,” she might have said.
We all knew the living will was Mom’s way of saying she didn’t want to die like my dad did, suffering horribly from lung cancer treatments known to be futile even before they started.
What we didn’t know is that she would suffer horribly because we didn’t adequately plan for her end-of-life care — and that the living will would prove useless.
Our Big Mistake
Mom was of the “whatever you think is best, doctor” generation, but none of her kids are wallflowers. Yet we were unprepared to advocate for Mom’s end-of-life preferences, so we politely acceded to her physician’s auto-pilot protocol of tests and specialists in unfamiliar medical centers and painful blood draws even though Mom was clear from the outset that there would be no chemotherapy and radiation.
Years earlier, my cousin had complained about the hospice nurse that cared for her dad, but I changed the subject, murmuring about how nice the funeral was. So I missed the opportunity to find out what had gone wrong, what was the name of the hospice and, most importantly, how we could avoid the same mistake if we needed hospice services in the future.
That turned out to be our big mistake.
We were caught off-guard on the day that Mom was too weak to get out of bed and I couldn’t turn her. Although we did have options (in-home help, inpatient hospice in the city 75 miles away or the local nursing home), during Mom’s months-long decline, we had not discussed them because we were hoping —there’s that word again — we wouldn’t need them.
The Hospice Trouble We Encountered
I woke up that morning, expecting another day of helping Mom from her lift chair to wheelchair to toilet to hospital bed. When we realized it was not to be, I panicked. I administered the first dose of morphine for the day and, as Mom dosed, started frantically trying to make a plan that should have been made weeks earlier.
The home care agency in her town, it turned out, only served patients not on hospice; they had a list of nurses who moonlighted, but nobody could be arranged on short notice.
The inpatient hospice had an opening, but that would mean Mom spending her last days in the city, too far for her five siblings to visit. Would she want that? In her frail and despairing condition, I couldn’t bring myself to ask.
So we headed to the nursing home, where Mom died 10 days later.
Before all this, I would have said that our one end-of-life plan was that Mom would not die in a nursing home that was just as miserable as we all feared it would be. But what I really meant was that was our hope. We didn’t have a plan.
Virtual reality may be able to transport you to spectacular other worlds, but a large part of its promise is the ability to also put you into the shoes of other people. In doing so, the hope is that VR could help make us more empathetic, since it gives us the ability to literally experience life from another person’s perspective.
That’s what VR studio Embodied Labs hopes to do. Based in Los Angeles — arguably the entertainment capital of the world — Embodied Labs wants to use cutting edge virtual reality to do something more than provide escapism. It wants to use it to promote empathy. And it wants to do it in such a way that can help train tomorrow’s caregivers.
We’ve previously covered Embodied Labs’ work creating a virtual experience intended to simulate the effects of Alzheimer’s disease. Called “The Beatriz Lab: A Journey Through Alzheimer’s Disease,” it follow the fictitious character Beatriz, a math teacher in her 60s, as she grapples with the neurodegenerative disease. Now Embodied Labs is back with another virtual training tool, this time designed to function as an end-of-life simulation for educating staff and medical students in hospices, hospitals, and universities. It’s currently being used at the Gosnell Memorial Hospice House in Scarborough, Maine, as well as by medical students at the University of New England.
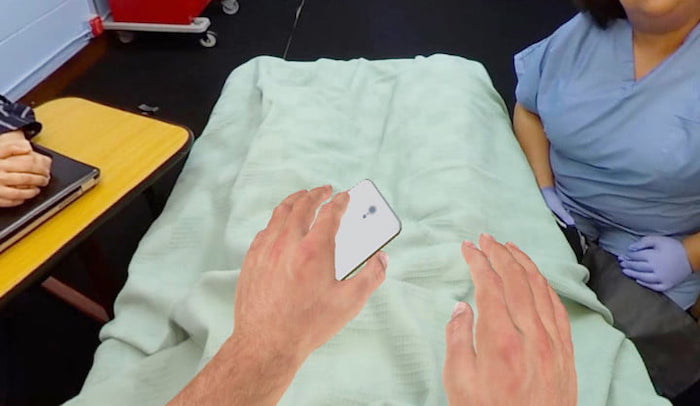
Meet Clay
The 30-minute simulation places users in the role of “Clay,” a 66-year-old lung cancer patient in need of hospice care. During the course of the VR story, Clay has important conversations with family, suffers a fall that puts him in the E.R., and eventually winds up in hospice care. Through simulating physical changes in virtual reality — such as how Clay’s skin alters and his senses dull — the user also gets to feel some approximation of what it would be like to experience end-stage cancer. By the end of the experience, Clay’s eyesight becomes dim as his life comes to a close. For anyone who associates VR predominantly with gaming, the effect is surprisingly poignant.
“The embodied experience includes receiving a terminal diagnosis from your oncologist, counseling from your case manager, and care from your hospice provider and family, and ultimately, it involves reaching the end of your life,” Erin Washington, co-founder and COO at Embodied Labs, told Digital Trends. “By embodying Clay, people gain insights into challenges faced by patients and families when curative treatment is not available, learn how hospice care supports loved ones, and explore the physical, spiritual, and mental changes that may occur at end of life.”
Through its painstakingly created and very human VR experiences, the company has cornered the market on a type of next-generation training tool. It provides an experience that caregivers or clinicians cannot get simply by reading textbooks.
“Embodied Labs creates immersive training and wellness tools for healthcare students, and for professional and family caregivers, so they can feel more empowered and confident in having the difficult conversations that surround end-of-life decisions,” Washington continued. “Organizations such as skilled nursing facilities, medical schools, hospice and home care agencies, and assisted-living providers use Embodied Labs to improve outcomes, operations, and culture.”
In addition to creating its experiences, Embodied Labs creates customized assessment questions to be answered before and after staff and students sample a VR scenario. This qualitative and quantitative data can then be used to provide new insights, on the part of professionals, into things such as how conversations about end-of-life are carried out.
Building empathy
But does this actually work, or is this a case of creating a solution to a problem that doesn’t actually exist? In fact, according to a new piece of research, virtual reality really be prove to be a useful tool in encouraging empathy.
In a study published this month in the open-access journal PLOS ONE, researchers from Stanford University compared the attitudes of people who had read a first-person narrative piece of writing about homelessness, those who had experienced a 2D interactive narrative about it on computer, and those who had undergone a perspective-taking VR scenario on the same topic. They found that the people who had experienced the VR simulation were more likely to sign a petition to support homeless populations. Follow-up surveys also found that they experienced longer-lasting empathetic feelings than those who had done the narrative-reading task.
Of course, there are problematic aspects with the idea of building empathy through VR. A 30-minute simulation about end-of-life conversations is not the same thing as experiencing it for real. A person really experiencing the effects of homelessness or discriminatory activity cannot simply take off their headset when they decide they’ve had enough of their life circumstances. Attempts to “gamify” complex scenarios risk inadvertently diminishing them, and carry the chance of turning something intended for good into something exploitative.
However, properly considered, there is room for virtual reality as a teaching tool. Certainly, it needs the proper care and attention of trained professionals, and it shouldn’t be considered a substitute for other forms of teaching. But as something that we’re glad to see being explored? Absolutely. And if it potentially means more empathetic treatment for yourself and your fellow human beings, you should be, too.
Librarian Marissa Lamer has come to appreciate the powerful messages that can be relayed in graphic novels.
ByMarissa Lamer
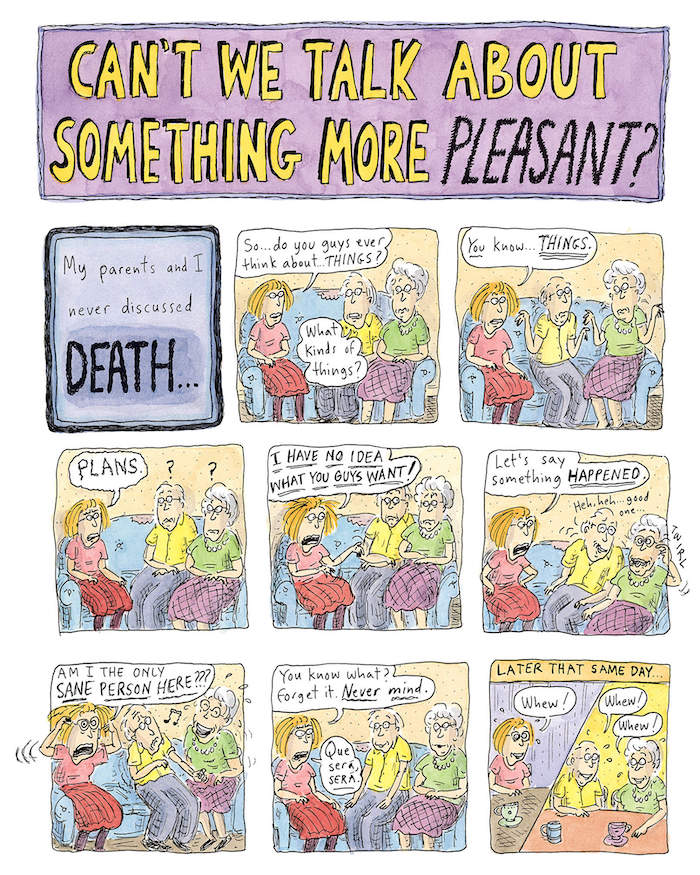
Can’t We Talk About Something More Pleasant? by Roz Chast is a compelling graphic memoir about the struggle Chast goes through as she watches her parents age and eventually die.
Although I have seen my parents grieve the loss of three of my grandparents, I have not yet experienced that kind of loss firsthand. And it’s definitely not an experience my parents felt necessary to discuss with me or vice versa.
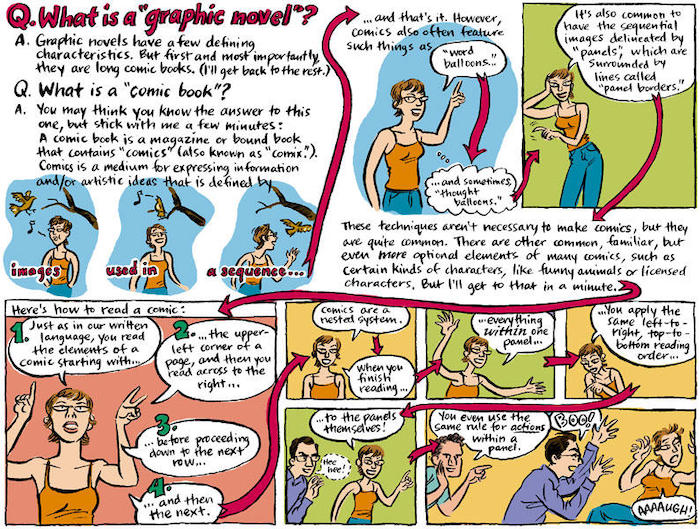
People don’t talk about death and dying in our culture, even though it affects every single person at some point in their lives. However, Chast’s memoir broached the subject in such an endearing and accessible way that it got me thinking: what is it about graphic memoirs that make addressing such difficult, even taboo topics more approachable than a traditional novel?
Hello, this is Marissa Lamer for the Radio Readers Book Club and I am coming to you from the public library in Hays, KS. Growing up I was rarely exposed to any type of graphic novels and comics. As I worked my way through college towards a career as a librarian, graphic novels became a genre of literature that grew increasingly intriguing, especially ones that were memoirs and nonfiction. I hesitantly started with a small graphic novel every now and then but have slowly come to truly enjoy and appreciate the value they add to reading.
Can’t We Talk About Something More Pleasant is a blend of comic strips and paragraphs of memoir. Chast finds the humor in an otherwise depressing time in the life of both her and her parents. For example, her mother’s increasingly outlandish stories help ease the pain of death reflected in more somber moments like when Chast stated “I could see that they were slowly leaving the sphere of TV commercial old age and moving into the part of old age that was scarier, harder to talk about, and not a part of this culture.”
The illustrations provide context and a visual for the parts of Chast’s story that are the most emotional and difficult to express in words.
Graphic memoirs like Chast’s make tough topics more accessible. They provide an abundance of extra layers in the writing style, illustrations, and format of the book that a traditionally written memoir cannot provide.
Scholar Eileen M. Richardson describes this advantage, “graphic novels are more than just stories with pictures; they have engaging illustrations that help readers infer the emotions and motivations of characters as well as more fully understand the twists and turns within the plot.”
Using visuals along with text can provide greater insight into the human condition and subjects that are tough to talk about or lay outside our cultural spheres.
Can’t We Talk About Something More Pleasant? is just the tip of the iceberg when it comes to graphic novels exploring thought-provoking subjects.
Here are a few to add to your reading list: Maus by Art Spiegelman is a two-volume, Pulitzer-Prize-winning graphic novel. The only graphic novel to be awarded such an honor. Animal characters are used to stereotype different races and nationalities illustrating the story of Spiegelman’s parents surviving the Holocaust and his relationship with his father.
Persepolis by Marjane Satrapi is another two-volume memoir of a girl growing up in Iran during the Islamic Revolution. It paints a vivid portrayal of life in Iran during a turbulent time through the eyes of a child.
The March trilogy by John Lewis and Andrew Aydin has won multiple awards and chronicles Lewis’ thoughts, feelings, and experiences throughout the Civil Rights Movement. The illustrator uses emotional black-and-white imagery which captures the raw emotion of people portrayed during this pivotal time in history.
Once again, this is Marissa Lamer coming to you from Hays for the Radio Readers Book Club. I hope you have enjoyed reading Can’t We Talk About Something More Pleasant? and the next time you are deciding what to read, you consider adding a graphic memoir to the list.
We had started down the path of honoring our mother’s wish to have a good death until a hospice nurse figured out that she wasn’t really dying.
Monona Yin, right, with her mother, Fay Hoh Yin, and brother, Duncan Yin.
By Monona A. Yin
Three years ago, my family and I had the experience of going through a full “dress rehearsal” for my mother’s demise. At 83, she had become alarmingly weak from stage IV lymphoma and atrial fibrillation, and asked me and my brother to come home to Delaware for her next oncologist visit.
Mom had already undergone chemotherapy and cardioversion, so we knew there were few treatment options left. Still, we were utterly unprepared when the doctor said, “She probably has less than six months,” and recommended that she begin hospice care.
Widowed at just 37 with two small children, Mom has trained herself to face challenges without flinching. She is that rare Chinese elder who isn’t superstitious about mentioning or planning for her own death.
True to form, when we got home from the oncologist’s office, Mom sat us both down at the kitchen table to discuss her end-of-life wishes. She had witnessed two horrible lingering deaths up close — her mother’s and a longtime friend’s. What she feared most was pointless suffering and the loss of control over her own life. She wanted us to understand that, if she had little hope of recovery, she’d rather go quickly than fall apart slowly and painfully.
My brother, at the other extreme, wanted Mom to pursue every medical option, no matter how long the odds. He believed that doctors were fallible, there was always another treatment out there, and life was worth clinging to. And he couldn’t bear the thought of living without her.
Then there was me, torn between them. I had spent hours listening to Mom’s fears and understood them. A decade earlier, my mother-in-law had died with a feeding tube in her side while her oncologist suggested more surgery — after six months of wasting away from metastatic cancer. It would have been infinitely kinder to allow her to die peacefully in her own bed.
We had given my paternal grandmother just such a “good death.” We sat by her bed and told family stories as she slipped into unconsciousness. We turned away from the outside world and drew close to one another. All was quiet and time seemed to stop. Finally, we held her as she took her last breaths, letting her know how much we loved her but also letting her go. I remember that week as a thing of rare beauty. It taught me that dying well can be a balm and a blessing to all involved.
Recognizing the enormous gulf between those two scenarios, I supported Mom’s right to die on her own terms. Like my brother, I desperately wanted more time with my mother. Despite her failing body, Mom’s mind remained sharp. In recent years, our occasional mother-daughter tensions had subsided, leaving a much warmer and less complicated companionship.
After an emotional week of debate, we all agreed to bring Mom to New York for a second — and final — opinion from the world-class doctors at Memorial Sloan Kettering. If they too determined that nothing more could be done, we would accept the inevitable.
At Sloan Kettering, Mom went through the scans without incident but afterward her blood pressure dropped dangerously low and she was admitted as an inpatient.
By the next night, Mom could hardly breathe at all. It was agonizing to watch her gasping for air. She was terrified of suffocating and on the verge of panic. Finally, she pulled me close to say, “Tell them to stop everything.”
I had promised to honor her wishes, so I found a doctor and activated her D.N.R. In a few minutes, my husband, Steve, and our 14-year-old daughter, Maya, arrived and Mom couldn’t hold back her sobs. “I’m so sorry I won’t see you grow up! I’m sorry I won’t see you graduate or get married!”
We had all been coming to terms with Mom’s mortality for months but the shock and pain were still overwhelming.
Then something that seemed miraculous happened. A hospice nurse, Tracy Kahn, arrived and went in to check on Mom. She came back to tell us that she didn’t think Mom was going to die that night, the next night, or maybe for weeks.
Based on years of observing hospice patients, Tracy did not believe Mom was dying of cancer right then.
Instead, without our realizing it, her heart had been severely weakened by the cardioversion, which required high doses of a toxic drug. Almost two liters of fluid had accumulated in the lining of her right lung.
We immediately reversed the D.N.R. but it would be another 10 days before Mom grew strong enough to have the fluid drained. Over the next month, the hospital’s lymphoma, cardiology and pulmonary teams worked together to bring Mom back from the brink. They administered steroids, gave her blood transfusions, stabilized her immune system, optimized her diuretic and treated her infections.
Mom transferred to a rehabilitation center for another month, then came to live with me in Brooklyn. With our newfound sense of “now or never,” Mom and I fulfilled one of her longtime dreams. We edited and self-published her memoirs, which she’d been writing for years, and she’s enjoyed positive reviews from friends and strangers alike.
Today, Mom still wrestles with neuropathy, shortness of breath, and sometimes crushing fatigue — but she is very much alive. Even more amazing, she has been living on her own for the past two years.
We’ve had time to reflect upon our decisions, how we influenced one another, and what we’d do differently. My central insight is that it took all three of us to steer clear of the twin shoals of dying too soon and dying too late. We made better decisions because we listened to one another and weighed all the conflicting information. In hindsight, my mother acknowledges that she wanted to “pull the plug” too soon because she became overwhelmed by fear.
No one thinks clearly in the grip of panic. That’s why it’s so important to start talking long before the end. Not merely about what constitutes a good death but, more important, what makes even a diminished life worth living. As Atul Gawande writes in “Being Mortal,” “Our ultimate goal, after all, is not a good death but a good life to the very end.”
The end-of-life conversation is equally important to both sides — the dying person and the survivors. One of my mother’s greatest comforts is knowing that her children understand her wishes and will honor them. We proved that during the dress rehearsal.
Only recently have Mom and I realized how much it cost me to be her health care proxy, rather than a grieving daughter who wanted to do anything to save her mother. I’m still going to be torn between those two roles “the next time” but simply being aware of that inner conflict helps mitigate it. And Mom’s future decisions will be informed by all the joy she would have missed had she died that night in late 2015.
When most of us go online to our internet banking account and set up a direct debit to pay a bill, we probably do it swiftly without much thought. But in reality it’s not that easy. In fact, there are a lot of complex processes involved in how we manage our finances, which older people, especially those with dementia, often struggle to deal with.
Dementia affects an estimated 850,000 in the UK, with numbers expected to rise to over a million in the next few years. Each year, dementia care is costing £26.3 billion in the UK alone. Most of this involves care in nursing homes and supporting people with dementia with their daily activities.
If we look at the whole raft of daily activities a person does, such as preparing a hot drink or a meal, or doing the laundry, financial management is one of the earliest tasks to deteriorate in dementia. These processes are complex, which is why people with dementia often struggle to count change, use a cash machine, pay bills or manage tax records sometimes even before their diagnosis.
Daily activities as a whole are often underpinned by a complex network of cognition. This can include different types of memory for past and future events, so the need to remember to do a task at 8pm tonight for example, involves problem solving skills, and attention. But there are other factors that can hinder someone when performing a task, such as motor problems or their environment.
Warning signs
In a recent analysis of a large data set collected from 34 clinical centres across the US, my colleagues and I looked at what kinds of behaviour are a warning sign for problems with paying bills and managing taxes in people with dementia.
When we obtained the data set, we only looked at people with dementia living in the community, who also had a family caregiver, and a diagnosis of the three dementia subtypes: Alzheimer’s disease, behavioural-variant fronto-temporal dementia, and Lewy body dementia. We then performed an analysis using statistical models to help identify the degree to which certain factors – such as language or motor skills – can predict a particular outcome. In this case, paying bills was the outcome for one model, and managing taxes was the outcome for the second model.
We found that between 11% and 14% of the ability to manage those financial tasks is predicted by executive functioning, or problem solving skills, language, and motor problems. So this means, if a person has problems solving difficult tasks, problems with language, they fall frequently and are moving slowly, and are also more likely to also struggle with financial tasks. Slowness and falls are particularly prominent in people with Lewy body dementia, which is different to Alzheimer’s disease, the most common form of dementia.
Get prepared
This knowledge can help people with dementia. Older people, including people with dementia, can often be subject to financial exploitation. This can be through online or telephone scamming, or knocking on someone’s door trying to sell something. And when people with dementia struggle using internet or telephone banking, they may be more prone to telling strangers their bank details.
A helping hand is needed for those living with dementia to manage their finances.
One way to support people in managing their finances may be to provide training to improve their cognition. It’s important to bear in mind that dementia is neurodegenerative. So while we can help people maintain certain skills for longer, there will come a point where full support for finance tasks is needed. This could involve arranging a lasting power of attorney and naming a person that is trusted to look after financial decisions.
Another way may be to adapt the homes of people with dementia to avoid falls and allow them to move around more freely. In our analysis, we found that falls were linked to poor finance management, meaning that noticing your loved one fall more frequently than usual could be a warning sign that they may also struggle managing their finances. If we can drag out the need for full support for as long as possible, we can help someone stay in their own home for longer. And that is exactly where people feel the happiest.
Other, larger financial questions loom for people with dementia, such as inheritance and dealing with payments for formal care – both at home and in future in a nursing home. These are big financial concerns, which should be discussed once a diagnosis is made, but ideally done before. That way the person is better able to judge what they think should be done with their money, and is less likely to be financially exploited than in the later stages of the condition. The Alzheimer’s Society has also produced some good further guidelines on how to deal with financial abuse in dementia.
While it may be the last thing someone wants to think about who has just received a diagnosis, the best way to avoid financial abuse is to put things in place right away. If that isn’t motivation enough, staying independent in all sorts of activities improves well-being. And that is our ultimate goal, whether we have dementia or not.







 Through its painstakingly created and very human VR experiences, the company has cornered the market on a type of next-generation training tool. It provides an experience that caregivers or clinicians cannot get simply by reading textbooks.
Through its painstakingly created and very human VR experiences, the company has cornered the market on a type of next-generation training tool. It provides an experience that caregivers or clinicians cannot get simply by reading textbooks. Of course, there are problematic aspects with the idea of building empathy through VR. A 30-minute simulation about end-of-life conversations is not the same thing as experiencing it for real. A person really experiencing the effects of homelessness or discriminatory activity cannot simply take off their headset when they decide they’ve had enough of their life circumstances. Attempts to “gamify” complex scenarios risk inadvertently diminishing them, and carry the chance of turning something intended for good into something exploitative.
Of course, there are problematic aspects with the idea of building empathy through VR. A 30-minute simulation about end-of-life conversations is not the same thing as experiencing it for real. A person really experiencing the effects of homelessness or discriminatory activity cannot simply take off their headset when they decide they’ve had enough of their life circumstances. Attempts to “gamify” complex scenarios risk inadvertently diminishing them, and carry the chance of turning something intended for good into something exploitative.