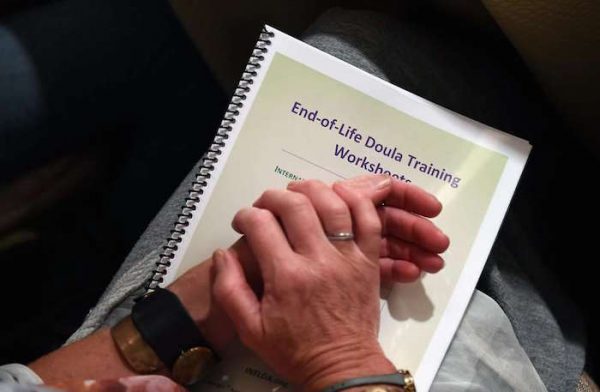
Henry Fersko-Weiss, co-founder and president of the International End of Life Doula Association, conducts a session at the association’s training at the Omni Hotel in San Francisco.
The emotional crumbling started when she was 14 and a friend was killed in a car crash. Three years later, her father died when his helicopter exploded. When she was in her 30s, her brother committed suicide.
By the time a close friend was murdered three years ago, the coping skills Bonnie Ludwig had for dealing with death were shattered — and she found herself one day on her knees on a sidewalk, sobbing obliviously.
Therapy gave healing, which allowed her to help comfort dying dogs at the pet care company she runs — and which soon led to her sitting in a San Francisco hotel room on Friday, learning how to help people die better.
Ludwig, 45, was taking a class in how to become a “death doula,” someone who helps shepherd the dying and their families into loving, peaceful exits. The man who founded the craft in 2003, Henry Fersko-Weiss, is guiding her and 47 other students through a weekend-long course on handling what for many seems like the worst moment possible — but, if handled deftly, can be a beautiful journey to whatever lies just beyond a heartbeat.
‘Learn to let go’
“Humans hold onto life so tightly,” said Ludwig, who flew up from San Diego to take the $600 training at the Omni Hotel. “We need to learn to let go better. We grieve so badly in our culture, and I have found it is sacred and an honor to be with animals when they die. Now I want to be able to do that with people.”
Fersko-Weiss, 68, has trained more than 1,000 people in his discipline, and this was his first session in San Francisco. People come to his trainings for many reasons, he said — some from pain, like Ludwig, some because they’ve already helped others die and feel a calling to do more. But they all have one thing in common.
“I have found that the people who come to these trainings have a great deal of compassion and want to serve people at this incredible period in their lives — death,” said Fersko-Weiss, who lives in the small town of Warwick, N.Y. “They are self-selecting. Like me, they feel this is a way they can really do some good and help. It’s very intense and very important.”
The idea of finding a better way of dealing with the obliteration of life came to Fersko-Weiss when he was a hospice volunteer and saw too many people missing the last breaths, not saying the words they wanted to say before passing, not feeling complete in what they were leaving behind.
Laura Statton attends the training session by the International End of Life Doula Association at the Omni Hotel in San Francisco.
He had a friend who was training at the time as a birth doula — a midwife of sorts, who helps birthing moms and their partners stay comfortable and well-centered — and he found the approach so dynamic he took the course himself.
What he learned there led him to co-found the International End of Life Doula Association. Doula, in ancient Greek, means “woman who serves.”
“It’s just our human nature that we want to be reassured as we die,” Fersko-Weiss said. “We’re going into the unknown, and everybody has fear of passing that boundary between life and death.
“I believe the only thing that counts at the end is having people we love, someone at your bedside, talking to you, telling them how much they love them, reassuring them it’s going to be OK. Those things are important.”
Calming techniques
Students learn techniques for calming the dying and their family and friends, and then they help them find the right kind of intimacy to say the things that need to be said. To cut to the chase about what they want to be remembered for, to compile scrapbooks. To face the end with grace.
Lori Goldwyn attends the training session by the International End of Life Doula Association at the Omni Hotel.
Sometimes doulas ease pain by having the dying visualize soothing times in their lives or by giving therapeutic touch. And they help plan what the final moments will be like. Sometimes people want candles burning, certain clothes, favorite poems read out loud. Doulas stay at the bedside, ready to recognize when death is minutes away — mottled skin, fingernails turning blue, other clues — so everyone can be prepared.
Cynthia Imperatore, who lives in New Jersey and is helping Fersko-Weiss at this weekend’s training, found that sometimes the simplest actions are the most important.
Recently she was helping a son sit vigil with his terminally ill mother, and found herself sitting at the woman’s bedside, holding her hand while the son stood stiffly at the foot of the bed with a TV blaring in the background. The final minutes were near. It didn’t feel right.
“I had him turn off the TV, put on some classical music, and I said, ‘Come here and hold your mother’s hand,’” said Imperatore. “So he came, and then I said, ‘Tell her these things’ — in Spanish, because that’s what his mother spoke. I said, ‘Tell her she’s done everything right. Tell her you’re grateful. Tell her you love her. Tell her what she did mattered.’
“And what happened is that these were the last words she heard,” Imperatore said. “He didn’t have to carry a sense of unfulfillment with him. It was good.
“What we do is not morbid,” she said with a gentle smile. “It’s a privilege to be there when people are dying. Death takes us to a place where we seek meaning, makes you question what is life. And sometimes it can make you appreciate life more.”
Today’s posting comes to us via Clare O’Leary | Palliative Care Educator | Mary Potter Hospice | Wellington, New Zealand
Maori digital stories about caring for kaumatua (elders) at the end of life. Teaching resource for nursing students, nurses and other health professionals who want to know more about Maori whanau (family) end of life needs and priorities.
No. This is a choice made by patients who are already at the end of their life. A dying person will naturally lose interest in food and fluids and progressively become weaker. When the dying person decides to stop eating and drinking altogether, the process of progressive weakness leading to death occurs days to weeks sooner than would happen if the person were to continue eating and drinking.
Most people who choose to voluntarily stop eating and drinking do so to regain or maintain some control over their situation. Reasons people give for making this decision include the desire to avoid suffering, not to prolong the dying process and to take control over the circumstances surrounding their death.
What Kind of Patient Chooses to Stop Eating?
According to a study in the New England Journal of Medicine, which surveyedhospice nurses in Oregon who cared for patients who chose to voluntarily stop eating and drinking, the typical patient is elderly and considers himself to have poor quality of life.
Do Persons Who Choose to Stop Eating Suffer?
Overwhelming evidence says no. The same study in the New England Journal of Medicine found that 94 percent of nurses reported these patients’ deaths as peaceful.
The cessation of eating and drinking is a normal part of the dying process that typically occurs days to weeks before death. Once the body becomes mildly dehydrated, the brain releases endorphins which act as natural opioids, leading to euphoria and often decreased pain and discomfort. When a dying person voluntarily stops eating and drinking, the same process occurs, and they may report feeling better than when taking in nutrition.
Very few patients complain of feeling hungry or thirsty after the first couple of days. Mucous membranes may become dry as dehydration sets in, which is why some patients may want to moisten their mouth with drops of water for comfort.
When death by voluntarily stopping of eating and drinking was compared with death resulting from physician-assisted suicide, nurses reported that patients in the former group had less suffering and less pain, and were more at peace than those in the latter group. Nurses reported that both groups had a high quality of death, which sounds strange but means that their deaths proceeded with lower levels of pain and struggle.
How Long after Does Death Occur?
Once a person stops eating and drinking, death usually occurs within two weeks. The person may continue to take small amounts of water to swallow pills or moisten the mouth, and these small sips of fluids may prolong the dying process by a couple of days.
Is Voluntarily Stopping of Eating and Drinking Right for Me?
This is likely a question you never thought you’d ask. But if you are, be sure to discuss this with your physician. She will likely want to make sure that there aren’t treatable conditions, such as depression or untreated pain, that are contributing to your decision. She may also refer you to a social worker or a member of your religious organization (if applicable) to discuss this decision further.
No one can tell you whether you should voluntarily stop eating and drinking. Depending on your quality of life, amount of suffering and personal belief system, you can decide if this choice is right for you.
In the article she mentions that musician Ben Lee is also a death doula.
In case you’re not familiar with the term, a “doula” is traditionally someone who gives support to a woman during pregnancy and during and after the birth.
A death doula is someone who helps at the other end.
Here, Jaki Fisher, an Australian living in Singapore and studying to be a death doula, writes about her first experience witnessing death.
JENNY was the first person who asked me to be with her when she died.
A single woman in her early 50s with only a couple of nephews she was in touch with, Jenny was being cared for at the Assisi hospice in Singapore where I was a volunteer.
Jenny and I talked a lot about what might happen during the dying process and afterwards and it was then that she told me she wanted me to be with her as she died. I said I would do my very best to make this happen.
After several months, Jenny suddenly got quite a lot weaker but at the same time, something in her shifted. I noticed this and asked her if she felt different and she replied that she felt that she was coming to accept what was happening.
She was hardly eating but I remember that when she would have a sip of coffee, her eyes would light up at the taste and she would savour it with delight. And when she went into the garden, she would marvel at the sun and the wind — simple, present joys became very strong for her.
At the end, Jenny deteriorated rapidly. Her breathing changed and it was clear to the nursing staff that she would not live much longer.
Jenny was the first patient at the hospice to take part in an end of life vigilling program, No One Dies Alone (NODA). Based on one that began in the US, theoriginal was started by a nurse called Sandra Clarke who, after leaving a lonely old patient who begged her to stay, returned after her rounds to find he had died alone. She couldn’t forget this and eventually set up this no-fuss, volunteer-run program that has been implemented in many large hospitals across the US.
With most NODA programs in hospitals, volunteers are called to sit with dying people who are alone, estranged from their families or far away from loved ones when they are actively dying.
At Assisi, from the time an alone person is admitted to the hospital, the NODA volunteers become the family and visit them until they were actively dying and then sit in vigil during the last couple of days of their life — if that’s what they wanted.
Jaki has assembled a group of volunteers for her NODA program.
LAST MOMENTS
I started the vigil and took the first shift, setting up Jenny’s room with music and soft lights. Jenny was not conscious but I believe she knew I was there. I spoke to her and told her I was there to be with her as she had requested. I remember feeling nervous as I went into the room and initially I felt like I had to ‘do’ things, like read poems or inspiring verses.
Gradually, I took some time to ground and centre myself and create an atmosphere of awareness and presence, as we had learnt in our training. Then, I just focused on really being with Jenny, with no distractions.
I was aware that this was not a normal time, that something big was happening. Jenny had had a fever and when I first sat with her, she was moaning a little. This was unsettling but it also seemed quite normal — I was struck by how OK everything was, even though it was also very sad. In some weird way, as humans, we know how to do this end of life thing. Her breathing became very shallow and there were long pauses between each breath. I remember at one point, I thought that perhaps she had breathed her last breath when suddenly she took a big inhale and I jumped in fright. I sort of laughed to myself and thought that Jenny was again teaching me, reminding me that this was not about me, it was about Jenny and I just tried to relax and be with whatever was happening.
She passed away after only 90 minutes, very gently and softly while I was singing quietly to her. I couldn’t help but think that as usual, she didn’t want there to be a fuss.
We had promised her that she would not be alone when she died, and I was so grateful that we could fulfil that promise.
Being with someone when they die is powerful but it is not frightening. Many people make this comparison, but dying is a bit like labouring to give birth. There are urgent bits and struggling bits and then at the end, it all goes quiet. When Jenny actually died, I hardly even realised, it was so soft, a tender sigh.
After Jenny’s death, her nephew told me that her life had been quite hard and often lonely but that she had shared with him that she was amazed that in her last months of life, when things were really difficult, there was so much love and care in her life.
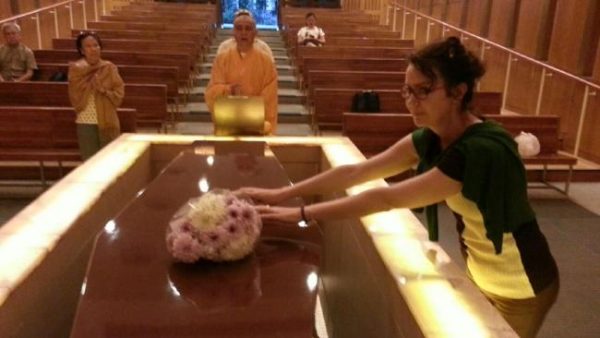
Jaki and NODA volunteers catch up to celebrate Jenny’s memory.
DEATH DOULAS
In the past two years, the NODA team at Assisi has accompanied more than 10 people during the last months of their lives and sat with them during their final hours. Many of the people we have accompanied lived hard, isolated, rough lives and I wish they could have been otherwise, but at least at the end part, they were loved with no expectations.
My dream is that people all over the world will adopt the NODA program in their own way so that we can all start to look after each other, especially at the end of life.
Nowadays, the profession of death doula is garnering a lot of interest. So am I a death doula? I am certainly interested in this area and I am heading off to San Francisco soon to take part in a death doula training and receive certification.
But I have my reservations about this sudden interest and the cynical part of me wonders if it is just the latest trendy thing, like being a yoga teacher was.
However, another part of me celebrates that perhaps this interest might be indicative of people wanting to face their mortality head on. I also like that death doulas are there to help people reclaim death as a natural part of life.
In the past, most people died at home — it was just another of the momentous life events — but in the past 50 years, we’ve pushed it away out of sight.
One thing I do want to say is that it is sometimes easy to romanticise dying but it’s not romantic — death is messy, draining, demanding, challenging, funny, heartbreaking, boring — everything … Death is often also really sad and a big loss, so I don’t really feel comfortable about making it a big celebration, unless of course it is!
I’m also wary of the idea of having a “good death” — that kind of creates a weird sort of pressure — like the one that is given to mums when they are striving to have a natural birth at all costs — our death will be what it will be.
However, what I do think is great is that people are talking about end of life and their choices. This conversation is so crucial and helpful and will make the end of life much clearer at a time when things are so rarely clear. However, once again, I wonder about being too attached to a plan — I think death would chuckle wryly at that idea.
To me, being with someone at the time of death is to become intimately exposed to not knowing — it asks us to be fully present and fully OK with whatever happens and not to impose a preconceived idea of what it should be like. To me, accompanying someone at the time of death is not really about doing anything, it’s about being able to hold and be there for whatever. We like to control everything in our lives but death does its own thing … it’s still the biggest mystery in our lives.
Jaki in her late 20s
‘AN UNNATURAL INTEREST IN DEATH’
I first volunteered at the Assisi Hospice not because of any great altruistic yearning to serve but because I knew that the people there had the inside story about dying. And I had an unnatural interest in death.
I fell into a black swirl of depression at 27 after I tried to fix my face. I went for some kind of noxious peel, a treatment that’s now probably banned. It’s kind of embarrassing — other people get depressed because they lose a loved one or suffer a terrible trauma — me, I thought I’d wrecked my face and down I went into the dark pit. (It’s fine now. Not quite the same but a perfectly serviceable face.)
I was lucky and got treatment and part of the therapy was to do something for others, to forget about “me” for a while. After much sulking and prevaricating I finally started volunteering at the Assisi Hospice.
Jaki with friends in Singapore.
I still remember the first time I went into the wards and saw my first “dying person” — how tiny and fragile, limbs like little birds, and yet how bright the eyes were.
I didn’t really speak Mandarin, Malay or Tamil (three of Singapore’s four official languages) and most of them didn’t speak English — the 4th one. And yet, those people didn’t just teach me about death, they taught me about life and living.
They taught me about bravery, love, tenacity, dignity and they didn’t seem to mind that I was a self-absorbed, self-destructive girl. They didn’t judge me and they let me see them in all their vulnerability and in this strange suspended time of life. Yes, they were dying but they were also very much alive.
I was supposed to be the do-gooder but they were the ones who taught me and showed me that life is all about moments and all about connection and all about love — and that’s about it.
I moved to the US to study Buddhism and then back to Melbourne but I never forgot the Assisi hospice. In 2012 after reading Being with Dying, a book about accompanying people at the end of life by Roshi Joan Halifax, I attended her Buddhist Chaplaincy program in Santa Fe.
Two years on, I was a Buddhist chaplain and also completed a unit of Clinical Pastoral Education at the Royal Melbourne Hospital.
But I was still volunteering at Assisi and as part of my chaplaincy project helped set up the NODA program.
JENNY’S LEGACY
Jenny spoke openly of her anger and frustration. She had accepted that she did not have long to live but she could not accept that she had to wait so long to die. This was another lesson for us. It was hard not to want to ‘fix’ this and make it better for her. At one time, she wondered what the point of her life was and expressed sadness that there were so many things she hadn’t done. I told her that from my point of view, she was teaching us so much and that she would live on so powerfully for us as our first NODA patient.
Jaki and fellow volunteers attend the funeral of Mr Loong, a man who had no friends or relatives in Singapore.
I asked her if we could talk about her after she had gone and whether we should change her
name if we did so. She was adamant — if it would help others gain a deeper understanding
about death, then we could certainly go ahead and use her full name with no changes.
We have been running this program for two years now and all of us involved can feel how it has the potential to touch us all and offer something that is greatly needed in
today’s highly medicalised and hurried world — genuine human companionship at the end of
life, especially for those who have no one to give it to them.
Jenny’s life was certainly not in vain. She lives on in the program and touches
every patient we serve. Because of her willingness to embrace NODA, more and more
people have not died alone — this is Jenny’s precious legacy.
When it comes to the end of life, hospital stays are more intensive and more expensive than alternatives.
People who die in the hospital undergo more intense tests and procedures than those who die anywhere else.
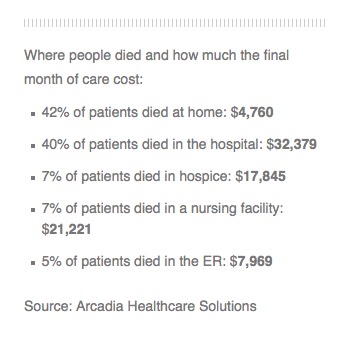
An analysis by Arcadia Healthcare Solutions also shows that spending on people who die in a hospital is about seven times that on people who die at home.
The work confirms with hard data what most doctors and policymakers already know: Hospital deaths are more expensive and intrusive than deaths at home, in hospice care, or even in nursing homes.
“This intensity of services in the hospital shows a lot of suffering that is not probably in the end going to offer people more quality of life and may not offer them more quantity of life either,” says Dr. Richard Parker, chief medical officer at Arcadia.
Arcadia analyzed all the Medicaid claims data for a private Medicaid insurance company in one Western state and detailed how many billable medical procedures each patient received and where. Patients in hospitals were billed for far more medical interventions in the last days of their lives than people who died in other settings. The company declined to name the state or company.
The study showed that 42 percent of patients died at home at a cost of about $4,760 for their last month of life, while 40 percent died in a hospital at a cost of $32,379. Dying in a nursing home was the second most expensive locale, inpatient hospice was third and an emergency room was fourth.
“In the end, everyone died. They all died,” Parker tells Shots. “If we look at this retroactively, retrospectively — and we could go back and ask people — I bet most of them would say I’d rather be home with my family.”
Parker says the cost of hospital deaths paid for by Medicare or private insurance are likely even higher because they pay doctors and hospitals more for their services.
Many studies have shown that people, when asked, say they’d prefer to die at home rather than in a hospital. However, those wishes aren’t always realized if a person hasn’t given clear instructions to a doctor or family member.
Parker says hospitals are designed to cure people who are ill rather than to allow people to die peacefully.
“The culture of American medicine today and for the last several decades is to keep treating patients regardless of the quality of life,” he says. “A lot of physicians have been reluctant to admit that the patient’s life is coming to an end.”
The picture is more complicated than the data show, says Dr. Lachlan Forrow, a professor of medicine and medical ethics at Harvard University.
Many patients move from home to hospice to hospitals and back during the last 30 days of life. And some may end up in the hospital because their pain or symptoms weren’t adequately controlled at home.
Still, he says, hospitals are just not good at caring for dying people.
“We do lots of very expensive things in hospitals to people in the last part of life who would rather be home, and we do those in part because in the hospital they get paid for,” he says.
It’s the only way to justify keeping in a hospital the people who need around the clock nursing care but can’t get it at home.
“If we really tried to make sure people at home could have what they needed at home, we could take better care of them, with less medical system-caused suffering, at lower cost, sometimes much lower cost,” he says.
The dying process usually begins well before death actually occurs.
Death is a personal journey that each individual approaches in their own unique way. Nothing is concrete, nothing is set in stone. There are many paths one can take on this journey but all lead to the same destination.
As one comes close to death, a process begins; a journey from the known life of this world to the unknown of what lies ahead.
As that process begins, a person starts on a mental path of discovery, comprehending that death will indeed occur and believing in their own mortality. The journey ultimately leads to the physical departure from the body.
There are milestones along this journey. Because everyone experiences death in their own unique way, not everyone will stop at each milestone. Some may hit only a few while another may stop at each one, taking their time along the way. Some may take months to reach their destination, others will take only days. We will discuss what has been found through research to be the journey most take, always keeping in mind that the journey is subject to the individual traveler.
The Journey Begins: One to Three Months Prior to Death
As one begins to accept their mortality and realizes that death is approaching, they may begin to withdraw from their surroundings. They are beginning the process of separating from the world and those in it.
They may decline visits from friends, neighbors, and even family members. When they do accept visitors, they may be difficult to interact with and care for. They are beginning to contemplate their life and revisit old memories. They may be evaluating how they lived their life and sorting through any regrets.
The dying person may experience reduced appetite and weight loss as the body begins to slow down. The body doesn’t need the energy from food that it once did. The dying person may be sleeping more now and not engaging in activities they once enjoyed. They no longer need the nourishment from food they once did. The body does a wonderful thing during this time as altered body chemistry produces a mild sense of euphoria. They are neither hungry nor thirsty and are not suffering in any way by not eating. It is an expected part of the journey they have begun.
One to Two Weeks Prior to Death
Mental Changes
This is the time during the journey that one begins to sleep most of the time. Disorientation is common and altered senses of perception can be expected. One may experience delusions, such as fearing hidden enemies or feeling invincible.
The dying person may also experience hallucinations, sometimes seeing or speaking to people that aren’t there.
Often times these are people that have already died. Some may see this as the veil being lifted between this life and the next. The person may pick at their sheets and clothing in a state of agitation. Movements and actions may seem aimless and make no sense to others. They are moving further away from life on this earth.
Physical Changes
The body is having a more difficult time maintaining itself. There are signs that the body may show during this time:
The body temperature lowers by a degree or more.
The blood pressure lowers.
The pulse becomes irregular and may slow down or speed up.
There is increased perspiration.
Skin color changes as circulation becomes diminished. This is often more noticeable in the lips and nail beds as they become pale and bluish.
Breathing changes occur, often becoming more rapid and labored. Congestion may also occur causing a rattling sound and cough.
Speaking decreases and eventually stops altogether.
Journey’s End: A Couple of Days to Hours Prior to Death
The person is moving closer towards death. There may be a surge of energy as they get nearer. They may want to get out of bed and talk to loved ones, or ask for food after days of no appetite. This surge of energy may be quite a bit less noticeable but is usually used as a dying person’s final physical expression before moving on.
The surge of energy is usually short, and the previous signs become more pronounced as death approaches. Breathing becomes more irregular and often slower. “Cheyne-Stokes” breathing, rapid breathes followed by periods of no breathing at all, may occur. Congestion in the airway can increase causing loud, rattled breathing.
Hands and feet may become blotchy and purplish (mottled). This mottling may slowly work its way up the arms and legs. Lips and nail beds are bluish or purple. The person usually becomes unresponsive and may have their eyes open or semi-open but not seeing their surroundings. It is widely believed that hearing is the last sense to go so it is recommended that loved ones sit with and talk to the dyingduring this time.
Eventually, breathing will cease altogether and the heart stops. Death has occurred.
Everyone should ask themselves, “How do I want to die?”
BY MARK FOURRE
As doctors, we are trained to solve problems.
If an arm is broken, we set it. If a heart valve is leaking, we replace it. If infection strikes, we do our best to cure it. There is real satisfaction when, as physicians, we make an accurate diagnosis and deploy an effective treatment.
Perhaps that’s why, when there is no problem to be solved, we don’t always do our best work. Death, after all, is not a solvable problem. All our patients will die. We can’t fix that. And too often, as a result, we don’t do all we should, or could to help our patients accept the inevitable.
Physicians are not alone, of course. Our society generally does a poor job of seeing death as a natural outcome of life. Many of us maintain the myth of our own invincibility long past our 20s. And where death was once something that typically happened at home in the presence of family and friends, it more often happens today in a hospital or nursing home.
When confronted with the question, “How do you want to die?” many of us might answer “I don’t.” But this question, the kind of death we want for ourselves, lives with us every day of our lives. It is true that extending life is a desirable and legitimate goal of our healthcare system, but the quality of our lives — and of our deaths — have a place as well.
None of us can solve death as if it’s a problem, but we can all have goals for the end of our lives. And it is that change, from problem-solving to goal-setting, which can lead us as physicians to do better by our patients when it comes to end-of-life care.
Of course, better end-of life-care, like better health overall, is not just the doctor’s responsibility. Just as everyone needs to do their part in the work of extending and improving life by not smoking, exercising and eating a healthy diet, so, too, must our patients take an active and informed role in good end-of-life planning.
The rewards can be a bit counter-intuitive. Research shows that among those who are given a terminal diagnosis, having an end-of-life plan that includes goal-directed care like hospice leads to care that is not only less costly, but patients on average are happier and actually live longer than those who exhaust every treatment option.
The good news is members of the medical community are beginning to embrace these changes. Across the MaineHealth system, for instance, events were planned around National Healthcare Decisions Day on April 16, organized to raise awareness of better end-of-life planning. And every day the conversation is growing among doctors, nurses and other practitioners about the need to talk to our patients about the benefits of creating advanced directives for healthcare and thoughtful end-of-life options such as hospice care.
For all this good work, though, the most important lessons I learned about death and dying didn’t come as part of my medical training. They came from my parents.
During my internship year, my dad as a relatively young man in his late 50s, had to struggle with the decision of whether to undergo chemotherapy for advanced lung cancer. He decided that his goal was not to pursue more days alive, but rather, to live the rest of his life meaningfully.
He chose to forgo chemotherapy and identified the goals he wanted to meet before dying. He completed the design of a church he was working on. He deliberately and intimately connected with family and friends. He put his financial affairs in order. He even planned his entire visitation service and funeral, including designing the memorial card handed out at his wake.
Importantly, he didn’t do this alone. He had to talk with a lot of people. Everyone important to him knew the plan. His family, his doctor, his business associates and his close friends all understood what to expect. And we all knew that my dad was living the way he always had, in a thoughtful and loving manner.
And, he spent time conversing with his God. “I don’t have a problem with dying,” he would say. “I’m just not sure I agree with the timing.”
My father was able to have the kind of death he wanted because he thought about it beforehand and took steps to insure that he died the way he had always lived.
Years later, my mother died from Parkinson’s disease. I am grateful to this day for the afternoon she spent with me not long after her diagnosis putting her thoughts down into a medical directive that would guide my family through the end stages of that illness. It was a natural and rewarding conversation in part because we didn’t set out to produce a perfect document, just one that would work for my mom and our family.
As a doctor, I have seen the alternatives to these thoughtful deaths.
I remember the first time I responded to a code in the hospital. I was a young medical student. A “code” or “code blue” is called over the intercom system of a hospital when a patient has had an unexpected cardiac arrest.
Amongst all the commotion, the thing that stood out the most to me was the patient. She was very frail, very old — and lifeless. The whole scene struck me as too much. It felt invasive and out of place.
Despite the apparent futility of the efforts, the “code” continued for what seemed to be a very long time. As is the case with the vast majority of “code blues,” the effort was not successful.
There is a reason why 65 percent of older physicians have an advanced directive, compared to 20 percent of the population generally. We know the limits of modern medicine. As a result, we know how we would like to die.
As physicians we must resolve to build end-of-life conversations into the care of all our patients. The time to start the conversation is long before a terminal diagnosis. And as with smoking cessation, progress will depend not on one conversation but instead on an ongoing dialogue.
If you are a patient and your doctor hasn’t brought up end-of-life care, don’t be shy. Ask. The time to start is now, and it is a conversation that should include not only your doctor, but all those close to you.
As an integral and inevitable part of life, death is not a problem. But our failure to plan for it is. Let’s solve it, together.