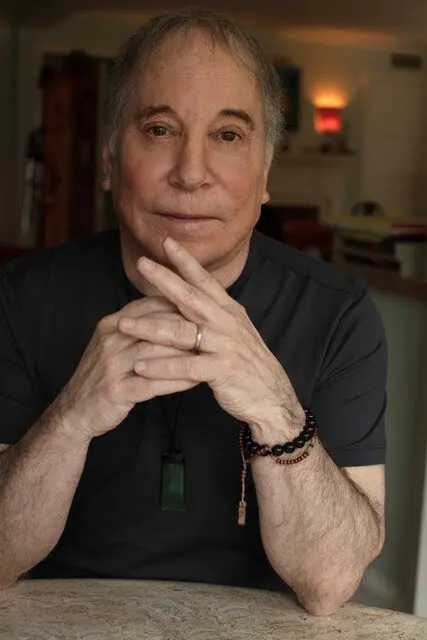
— The 81-year-old songwriter ruminates on mortality, faith and meaning in an album that could be a farewell.
On a new album, Paul Simon is thinking about time, love, culture, family, music, eternity and God, striving to balance skepticism and something like faith.
What do songwriters do when they feel death approaching? As time runs out, some choose to spend it by determinedly creating music to outlive them.
“Seven Psalms” sounds like a last testament from the 81-year-old Paul Simon. It’s an album akin to David Bowie’s “Blackstar” and Leonard Cohen’s “You Want It Darker,” which those songwriters made as mortality loomed; they each died days after the albums were released.
Their generation of singer-songwriters has dedicated itself to chronicling their entire lives, biographically and metaphorically, from youth through last words. “Blackstar” was turbulent and exploratory; “You Want It Darker” was stoically bleak. “Seven Psalms” stays true to Simon’s own instincts: observant, elliptical, perpetually questioning and quietly encompassing.
The album is constructed as a nearly unbroken 33-minute suite, nominally divided into seven songs that circle back to recurring refrains. It has places of lingering contemplation and it has sudden, startling changes; its informality is exactingly planned.
Simon begins the album in his most casual tone. Over calmly precise and rhythmically flexible guitar picking, he sings, “I’ve been thinking about the great migration.”
Almost immediately, it becomes clear that the migration is from life to death, a transition the singer is preparing to make himself. He’s thinking about time, love, culture, family, music, eternity and God, striving to balance skepticism and something like faith. “I have my reasons to doubt/A white light eases the pain,” Simon sings in “Your Forgiveness.” “Two billion heartbeats and out/Or does it all begin again?”
Simon’s songwriting has never been particularly religious. Over the years, he has drawn on gospel music for songs like “Bridge Over Troubled Water” and “Loves Me Like a Rock,” which bring religious imagery to secular relationships, and his 2011 album, “So Beautiful or So What,” had touches of Christian imagery — but also imagined “The Afterlife” as one last bureaucracy, where arrivals have to “Fill out a form first/And then you wait in a line.”
“Seven Psalms” is more humble and awe-struck. Its refrains return to, and work variations on, the album’s opening song, “The Lord.” As in the psalms of the Bible — which, as Simon notes in “Sacred Harp,” were songs — Simon portrays the Lord in sweeping ways: wondrous and terrifying, both protector and destroyer, sometimes benign and sometimes wrathful. The Lord, Simon sings, is “a meal for the poorest, a welcome door to the stranger.” Then he turns to naming 21st-century perils: “The Covid virus is the Lord/The Lord is the ocean rising.”
Much of the music sounds like solitary ruminations: Simon communing with his guitar, which has been the subtly virtuosic underpinning of most of his lifetime of songs. As his fingers sketch patterns, he latches onto melody phrases and then lets them go, teasing at pop structures but soon dissolving them. And around him, at any moment, sounds can float out of the background: additional supportive guitars, the eerie microtonal bell tones of Harry Partch’s cloud-chamber bowls, the jaunty huffing of a bass harmonica and, in the album’s final moments, the voice of his wife, Edie Brickell.
In the course of the album, Simon sings about personal distress and societal tensions. In “Love Is Like a Braid,” a song of gratitude and vulnerability, he sings, “I lived a life of pleasant sorrows until the real deal came/Broke me like a twig in a winter gale.” In “Trail of Volcanoes,” he juxtaposes youthful exploits with adult realities: “The pity is the damage that’s done/Leaves so little for amends”
Meanwhile, Simon’s tartly aphoristic side reappears in “My Professional Opinion,” a swipe at social media context collapse set to a country-blues shuffle. “All rise to the occasion/Or all sink into despair,” he sings. “In my professional opinion/We’re better off not going there.”
He ends the album — possibly his last — with a song called “Wait.” He protests, “My hand’s steady/My mind is still clear.” Brickell’s voice arrives to tell him, “Life is a meteor” and “Heaven is beautiful/It’s almost like home.” At the end, he harmonizes with her on one word, extended into five musical syllables: “Amen.” It sounds like he’s accepting the inevitable.
Amy Pickard wants you to talk about death. Specially, she wants you to make your healthcare planning and end-of-life arrangements known to your loved ones.
She knows that talking about death is going to make most people squirm. But the Southern Californian, who runs the end-of-life consulting company Good to Go!, says an awkward but respectful conversation now lessens the grief of a loss when the inevitable happens and allows people to honor a deceased loved one’s wishes.
“I tell adult children to tell their parents, ‘Hey, I’m getting organized with all my advance planning, and I just realized that if I don’t know what I want, you guys certainly wouldn’t know,’” she said. “‘And then I thought if something happens to you guys, I wouldn’t have a clue what to do, and that terrifies me.’”
For some people, it comes from a fear of dying, said author Cameron Huddleston. She said having to talk about end-of-life arrangements feels like being forced to think about mortality.
“However, avoiding the subject doesn’t mean you can avoid the inevitable,” she said. “It just means that you probably won’t have a plan for your death, and you’ll make things harder for those you leave behind.”
Why we need the death talk
Pickard and other advocates for end-of-life planning find that sharing their personal experiences helps normalize the conversation. Pickard shares with clients her experience of grieving the loss of her mother, who died unexpectedly at age 67.
“So I’m in the wilderness of grief, and at the same time I had to suddenly be an accountant, a florist, a detective, a travel agent, an estate appraiser and just all these things. And I was none of those things,” she said.
Her mom didn’t leave any instructions or wishes. Pickard described the work of wrapping up her mother’s life as overwhelming emotional labor.
In the midst of grieving a parent’s death, you might also have to plan the memorial, end monthly magazine subscriptions and notify others of their death. It’s not easy to juggle these tasks or final wishes if you don’t know what someone wants or where their information is stored.
That’s compounding grief with tasks that are frustrating in the best of times. To avoid it, you’ll have to have a difficult conversation that a parent might not be ready for. Asking if your parent would prefer to be buried or cremated (or something else entirely) could elicit responses like “I’m not that old” or “Why, are you trying to get rid of me?” No, you aren’t, but you can’t be their advocate without knowing what they want.
“It’s OK to acknowledge that the topic is uncomfortable, but you could say that you would be even more uncomfortable making arrangements for them without their input,” Huddleston said.
What do you do when someone dies?
Because we find death so hard to talk about, there are probably lots of things people wonder but don’t know. We have answers.
Not having a parent’s healthcare wishes and end-of-life instructions could leave a child wondering whether they made the right decisions.
It can also be an overwhelming experience to sort through a person’s belongings for information.
When Pickard’s mother died, she had no directions to follow. The minute she arrived at her mother’s condo in Chicago to cancel the utility bills and take care of other death duties, Pickard realized that she didn’t know the name of the electric company that kept the lights on.
“I would have given anything to talk to my mom again,” she said. “Not to tell her I loved her, but to get her Wi-Fi password.”
At the end of the day, having this information at the ready allows people to focus on love, Pickard said — how much that person was loved and how much people loved them.
This future peace of mind extends to the person who made their end-of-life wishes known. Pickard says these instructions aren’t just mundane bill canceling. For an adult child, it can be the last time a mother, father or guardian takes care of them.
Huddleston added, “Think of letting your family know what your final wishes are as a gift — your final gift to them. You’ll make it easier for them during a difficult time by having a detailed plan that they can follow.”
Starting the conversation
There isn’t one right way to approach this conversation. It really depends on whom you are talking with.
If you know your person doesn’t like to be taken by surprise, give them a heads up, said Kate DeBartolo of the Conversation Project, an initiative of the Institute for Healthcare Improvement. For example, DeBartolo said, if you’re planning a two-week visit with your parent, let them know beforehand that this topic is on your mind and that you would like to talk about it with them.
This gives the person the opportunity to think about what they want if they haven’t already.
You can sit down and talk about it over coffee or sprinkle it into everyday conversation when it feels natural.
If you’re watching a TV show or movie that depicts a funeral, that could prompt the conversation. You could say, “That made me realize I’m not sure of what you would want in that situation” or “Do you agree with the decision that character made for their parent?” DeBartolo said.
It could be a one-on-one conversation or it could be done with several people.
“I heard a woman who said she made desserts for her family at Thanksgiving and she held them all hostage and said, ‘No pumpkin pie until you tell me how you want to die,’” DeBartolo said. “And everybody would go around the table and talk about it, and that worked for her family.”
Having the conversation
Before you broach the subject, DeBartolo wants you to keep in mind the following:
Your questions won’t be solved with one conversation. The more you discuss it, the easier it will be for someone to talk about and share their thoughts.
Don’t wait until the end of someone’s life to talk about their wishes. There’s a misconception that this conversation should happen with older adults. DeBartolo argues that everyone over 18 should get their arrangements in order or at least start talking about it. Keep in mind that the information will need to be updated whenever you move, get married, divorced or have a child.
Don’t start the conversation with financial questions. You might give a person the wrong impression — that you only care about their money.
Be an active listener. The person you’re talking with might not give you a straight answer. DeBartolo said a grandmother might say that she wants “home” to be a part of her end-of-life care. Ensuring that Grandmother is at home might not be feasible, but “home” could mean having home-cooked meals, living in a facility that allows her cat or having personal effects with her.
Lastly, when you’re ready to reach out to someone, remember to frame the conversation with compassion. This doesn’t have to be a painful talk, DeBartolo said. It can be loving, a time to share memories.
In the conversation, Huddleston said, find out the following information at the very least:
How the person wants their remains handled. If burial is their choice, ask if a plot has been purchased or where they would prefer to be buried.
What type of memorial service they want, including music choices and who will speak.
The names and contact information of the people they would like to be notified of their death.
Information for the obituary.
The location of wills, trusts and any life insurance policy.
A list of assets and accounts, including things like the names of their utility companies — and their computer login and Wi-Fi information.
Any specific instructions for how they want heirs to handle their inheritance.
Arrangements for children or pets.
Some people will never want to talk out loud about this, and DeBartolo said that’s OK too. Let them know you’re open to hearing how they’d like the end of their life handled in any way they feel comfortable communicating it. If they can send you an email or a text of a few instructions or tell you where their important documents are, that can be enough.
Good to Go! sells a “departure file” and offers consulting services in a private or group setting. The latter is called “Good to Go! Parties,” an upbeat gathering to talk, eat, drink and fill out the departure files.
CaringInfo, a program of the National Hospice and Palliative Care Organization, has guides and resources to help clarify the difference between hospice and palliative care or what you need to create an advance directive.
Death Cafes, in-person or online, are group-directed discussions of death with no agenda, objective or theme. It’s a discussion group and not grief support or counseling.
Karen Lerner sits at the kitchen table of her Bellingham home. She has been a PeaceHealth palliative care patient since her cancer diagnosis two and a half years ago. Lerner is switching to remote palliative care through Seattle’s Fred Hutchinson Cancer Center because PeaceHealth is reducing its program on May 26. “That was devastating to me,” she said.
PeaceHealth in Whatcom County is ending comprehensive outpatient palliative care on May 26, reducing staff to one nurse and one social worker for in-home care of seriously ill patients.
Criticism of the decision has been harsh, with some patients and observers saying it goes directly against PeaceHealth’s mission.
“This community, Whatcom County, has really been a leader in serious-illness and end-of-life care for the past decade, and I just feel like they cut us off at the knees,” said Marie Eaton, whose title is community champion at the Palliative Care Institute at Western Washington University.
Eaton and others, including retired PeaceHealth physician Meg Jacobson, who was board-certified in palliative medicine, said PeaceHealth broke a promise when it decided to cut palliative care after convincing donors to give more than $2 million to launch the program several years ago.
“PeaceHealth had assured us that we would keep it going,” Jacobson said. “And they just lied. I don’t know what they’re telling donors.”
In a May 16 statement to Cascadia Daily News, Bryan Stewart, system vice president for PeaceHealth’s Home and Community Division, said the health care provider couldn’t justify continuing the program, given the high cost of palliative care.
“On average, insurance reimbursement only covers 15–20 percent of the palliative care program costs,” Stewart said. “With rising costs across all service lines, it was simply not feasible to continue offering the comprehensive outpatient palliative program.”
Eaton said she understood PeaceHealth’s financial difficulties, but “the decimation of the outpatient palliative care program is particularly disturbing.”
“We raised millions of dollars with the promise that PeaceHealth would take it over in five years,” Eaton said. “I frankly feel betrayed.”
Stewart said the PeaceHealth St. Joseph Medical Center Foundation received a single, $1.25 million gift to launch the outpatient palliative care program, with an additional $1 million contributed by community members.
Stewart confirmed PeaceHealth had made a promise — with a caveat.
“The Foundation was clear with donors at the onset that PeaceHealth’s commitment was to support the palliative care program beyond the five-year Foundation investment, understanding that as the program evolved over time, operational changes might be necessary,” Stewart said. “Unfortunately, the stress caused by the pandemic on our health care system, coupled with under-reimbursement, high program expenses and relatively low number of patients served, led to the recently announced changes.”
In a recent review of its programs, PeaceHealth also decided to close its allergy clinic and overnight sleep lab.
A patient’s story
Karen Lerner was diagnosed with metastatic melanoma two and a half years ago, after doctors found a bleeding tumor in her brain. She learned about the cuts to palliative care on a recent phone call with her pharmacist.
“That was devastating to me and, I’m sure, to them,” Lerner said, referring to the palliative care workers who supported her. “It’s an amazing team of care providers and volunteers that can’t be replaced, as great as my personal care physician is.
Palliative care goes the extra mile for patients who are in extreme circumstances. PeaceHealth’s program cared for people diagnosed with cancer; chronic obstructive pulmonary disease, or COPD; congestive heart failure; and those who “graduated from hospice,” Eaton said.
Lerner was an unusual case. The side effects to her treatments included painful reactions that even made certain clothing unbearable.
“My doctor says that I’m an outlier, but my skin hurts all the time,” Lerner said. Her palliative care pharmacist, nurse and physician “have been really good about never giving up, in terms of trying to find the best medication regimen for me.”
“A normal pharmacist, [primary care physician] or oncologist, they don’t have the time or the ability to really look into things and help solve problems.”
Lerner said PeaceHealth staff couldn’t tell her where to turn for comprehensive palliative care after May 26. She considers herself fortunate, however. She lined up remote palliative care through Fred Hutchinson Cancer Center in Seattle, where she has been receiving her cancer treatments.
“There are so many people who are isolated and don’t have the resources that I do, that are just going to fall through the cracks with this, I’m sure,” she said.
After the cuts to palliative care, Eaton predicts that many of the patients currently in the program will begin to cycle in and out of the emergency room.
“One hundred people is too much for one nurse and one social worker to manage,” Eaton said. “To be able to stay in your home and have your symptoms managed by a social worker, nurse, physician and chaplain means your quality of life is so much better.”
Stewart put the number of in-home palliative care patients at 64. He also emphasized that cancer patients will get additional care. An oncology physician assistant, he said, will “focus exclusively on the palliative care needs of this vulnerable population.”
PeaceHealth’s mission
Eaton said that palliative care may not be a money-maker for a health care provider, but it can be a money-saver.
“It gets people into hospice sooner, where they can be covered by Medicare,” she said. “It reduces the number of [emergency department] visits.”
Jacobson also acknowledged that palliative care places a financial burden on health care systems, noting that they can’t bill for the services of a social worker or a chaplain.
“And doctors who do palliative care don’t see enough patients to make money for the institution,” Jacobson said. “So it was always going to be something that they were going to have to commit to, as a mission-driven service.”
PeaceHealth’s mission statement, posted online, says, “We carry on the healing mission of Jesus Christ by promoting personal and community health, relieving pain and suffering, and treating each person in a loving and caring way.”
Lerner, a cancer patient, took a dim view of the statement.
“The ironic thing, if you look at the PeaceHealth mission statement, it’s supposed to be for the care and relief of pain and suffering,” she said. “Instead, it’s more like, ‘for-profit, tax-exempt.’ That seems to be their mission.”
Over the past 25 years, Barry Whelan has made more than 20,000 visits to palliative care clients and their families.
The recently retired palliative care counsellor from Poowong, in Victoria’s south-east, has guided people of different faiths and backgrounds through the final stages of their life.
It’s given him insight into what happens when someone is at the end of their life.
“When someone is diagnosed with a terminal illness, they run through a milieu of emotions,” Mr Whelan says.
“Most people get to their 30s or 40s or 50s and think they’ve got 30 years left, then all of a sudden they’re told that they’ve got something that’s going to terminate their life.”
Resolution of an ongoing family dispute is an important part of the dying and grieving process.
He says common reactions to a terminal diagnosis include shock, denial, or anger followed by questions such as ‘Why me? Why now?’ and ‘What happens when I die?’
“I often get asked, ‘What’s it like to die?’ and my favourite line is ‘I don’t know, I’ve never done it, but I can teach you how to live before you die’.”
Palliative care primarily involves nursing in co-ordination with services such as occupational therapy, art and music therapy, counselling, and pastoral and spiritual care.
“When I first started back in 1997, it was probably a 95 to 98-per-cent death rate, but now with the advances in modern medicine, people survive a lot longer,” he says.
Despite significant advances in pain management with terminally ill patients, Mr Whelan said the mental anguish around death and dying remained a challenging personal journey for individuals.
A good death
Mr Whelan says initial visits with palliative clients were about determining a client’s goals, priorities and what they wanted to achieve in the time they have left.
“A good death to me is someone who is at peace with themselves, at peace with their family or surroundings and at peace with whatever they believe in,” he says.
As a counsellor, he has helped clients work through their stress, anxiety, guilt and past issues to reach a point of comfort.
“One of the first patients I had, the lady wanted to jump from a parachute. She survived the parachute jump but within a few weeks she had passed away,” he says.
“It was something that she wished to achieve”.
Barry Whelan with Palliative Care South East (PCSE) chief executive Kelly Rogers (left) and co-founder Dr Ruth Redpath.
Mr Whelan says the most heartbreaking cases that he witnessed as a chaplain in aged care facilities was when terminal patients who had not had a visitor for months and even years were suddenly set upon by relatives.
“Where there’s a will there’s a relative,” he says.
Likewise, he says that family dispute resolutions were an important part of the dying and grieving process.
“I’ve seen people sit on one side of the chapel with other family on the other side [and] it was all over some trivial thing that happened 40 years before,” he says.
“It’s amazing what drives people apart, and how little it can be to bring them back together.”
The body follows the mind
Mr Whelan says he has observed that terminal patients can linger on for days or weeks if there is something unresolved that they wish to sort out.
“I think the body follows the mind in this, both in living and in dying,” he says.
“A lot of people, once they come to that peace they can accept the dying, but a lot of people hang on.”
He recalls the story of a woman who was sent home to die in October 2007, whom he later visited in February 2008.
He says she was determined to see out her 47th wedding anniversary, then she willed herself to live for her 70th birthday celebrations, and later her son’s wedding in May 2008.
“That lady went right through for the two and half years that I visited her, until finally we made the decision at work that she wasn’t really palliative anymore,” he says.
“She was still having chemotherapy, but she didn’t really need us.
“We all have aims and goals.”
She eventually passed on in 2015, living for seven years beyond her life expectancy.
Barry Whelan estimates he has counselled more than 2,500 terminally ill clients since starting in 1997.
Mr Whelan has witnessed countless occasions where clients have seen through a birthday or milestone celebration, waited until a relative had arrived from overseas, or met a new addition to the family before passing within days of an occasion.
“The other thing that I see is that sometimes people wait until their loved ones have left the room, and then they will simply just close their eyes and they’re gone,” he says.
Mr Whelan believes that self-will plays a key role in a person’s ability to hang on to life. In the same way that people without particular purpose, attachment, direction or will to live, can make a call on when they’ve ‘had enough’.
He says it is not unusual for widowers to pass on not long after losing a lifelong spouse and soul mate.
“If a person doesn’t feel wanted, doesn’t feel needed, I think they lose the will to live,” he says.
“I have seen people who have gone to hospital and not been visited by their loved ones, and they’ve died within a few days. So again, it’s this will to live.”
Terminally ill patients have a tendency to determine when they’ve ‘had enough’.
In illustrating an example of a sustained will to live, Mr Whelan refers to the stories of concentration camp survivors and prisoners of war who manage to make the best of every day despite horrific circumstances.
“I guess my motive has been to survive as best you can for as long as you can with the best conditions you can manufacture from what you’ve got,” he says of his philosophy on life.
After 25 years witnessing people in their final stages of life, Mr Whelan says that he has learned to value everything he has.
“My advice to people is just, ‘enjoy what you’ve got, while you’ve got it, because you can’t go to a doctor and ask for a prescription for tomorrow’.”
Four days after her mother died, Shelley Anson walked into a candlelit room at a funeral home. There, her mother Lorraine lay on a bed, tucked in as though she were just asleep. A cooling mat to slow decomposition was humming away beneath her body.
“She looked so beautiful. She had colour in her face, even her lips. I asked if it was make-up, but it was from massage. I was in absolute disbelief and awe, I cried and cried,” Anson says.
“I was kissing her and she was cold to the touch, but that was OK. I was telling her how much I loved her, how grateful for her I was and how happy that she was reunited with my dad.”
For the next three hours, Anson cuddled her mother, brushed her hair and washed her face, arms, torso and legs with warm water and myrrh oil. Finally, she dressed her in her favourite sequined maroon dress for the funeral.
The experience, in December, was transformative for Anson’s grief.
“It was perfect in every way. It brought me absolute, great peace,” she says. “I could have stayed longer, but I felt like I’d finally done enough and that it was OK to go home.”
In contemporary Australia, much as in the rest of the Western world, our eyes are closed to the realities of death. The dead are often hurried away from a hospital room by an appointed funeral director and not seen again, unless a family chooses to farewell them with an open casket.
But there is a growing push towards keeping vigil with a loved one after their death and taking on the care of their body, either at a private house or a funeral home.
Advocates of what’s been termed the “death-positive movement” say our modern, sanitised practice interrupts our grieving process, creates a fear of death and has contributed to the loss of centuries-old rituals of caring for our loved ones.
A bereavement casting made by Pia Interlandi of Shelley Anson’s hand clasping her mother’s.
Libby Moloney is the founder of Natural Grace, a Victorian holistic funeral company that has been at the forefront of shifting the narrative around after-death care.
“In the 1900s we surrendered the care of our dead to well-meaning strangers in what we now know as the funeral industry. In a way death was sterilised and outsourced. It’s a model that’s very much about easing your burden, taking away the stress,” she says.
But Moloney says this robs families of a pivotal point in the mourning process that comes from the act of being with the body of their loved one, of feeling the stillness of their hand.
“It happens to everybody, and it’s deeply sacred,” Moloney says. “It takes the human mind and body about three days, where there’s a visceral, profound knowing that ‘I’m ready’ – ready to separate from the body of my person and I can now go on to the next steps. It’s unbelievably empowering.”
She says at least 80 per cent of her clients have an element of death care, with roughly half choosing to do this at home, the other half at her Woodend or Fairfield sanctuaries. These rituals usually take place over a three-day period before a funeral ceremony and burial or cremation.
Tasmania-based Bec Lyons spent six years in the mainstream funeral industry before becoming a death doula and independent funeral practitioner. Today, she leads both the Australian Home Funeral Alliance and Natural Death Advocacy Network, which aim to raise awareness of family-led funerals, death care and natural burials.
Death care is not for everybody, but Lyons’ goal is to teach people that there isn’t just one way to grieve. Most Australians don’t know that they don’t have to appoint a funeral director, and that it’s perfectly legal and safe to care for the body of their loved one. In NSW, the deceased can stay at home for up to five days; in Victoria, there is no prescribed limit. The key requirements are to register the death and arrange a burial or cremation.
Australian Bureau of Statistics data shows there were more than 171,000 registered deaths in 2021, up from almost 147,000 10 years earlier. It’s estimated that by 2066, the number of annual deaths will be over 430,000.
“There’s a pertinent conversation around what are we going to do with all those bodies? Death needs to move back into the home,” Lyons says.
With 70 per cent of Australians wanting to die at home, Lyons believes that the older generation, having watched their parents die in nursing homes, want to do things differently.
She says the number of home funerals she’s facilitated has doubled in the last 12 months, which she puts down to increased understanding of death, as well as financial considerations: they can be half the cost of a typical funeral.
Lyons says more people began to explore the idea of after-death care and home funerals (meaning a dead person is kept at home until they are put to rest) during COVID-19, when restrictions stripped away usual mourning practices. Holding vigil at home was still possible.
“In conventional Western society, the only vehicle we have to mourn is the funeral ceremony. For people who want that, that’s fantastic. But when COVID-19 hit, you ended up with grief that had no outlet,” she says. “Grief is an emotion that needs something to do.”
Anson’s mother died at age 79, 2½ years after a brain cancer diagnosis. Anson, an end-of-life doula and nurse, cared for her at home for the first seven months until, emotionally, she couldn’t do it any longer. But putting her mother in a nursing home weighed heavily.
It’s why after-death care and being with her mother’s body was extraordinarily healing: “That was my way of giving that last bit of love that I felt I hadn’t been able to give.”
Melbourne Chevra Kadisha CEO Simon Weinstein with volunteer Yaelle Schachna.
Several religions and cultures have preserved ancient death care rituals. In Islam, it’s customary for same-sex relatives to wash the bodies of their dead, usually three times, then wrap them in sheets. Hindu families traditionally wash a body with holy ingredients such as milk, honey and ghee before dressing them.
Simon Weinstein is chief executive of the Melbourne Chevra Kadisha, a funeral home that serves much of the city’s Jewish community and delivers funerals according to Orthodox laws and traditions.
In Judaism, a burial should happen as quickly as possible, preferably within a day, and until that happens, a body is guarded – an act called “shemirah” – by family sitting close by to protect and comfort the soul.
The body is also washed in a ritual of purification and immersed in a holy bath. Weinstein says this process, tahara, is done by trained, same-sex volunteers as children and grandchildren of the dead cannot be involved to preserve modesty – but the community is tight-knit, and there is often a connection with at least one volunteer. “It’s an act of ultimate kindness and respect,” he says.
The cotton shrouds for the ritual of tahara are ironed at Melbourne Chevra Kadisha.
The dead person is then dressed in white cotton shrouds, and it’s at the end of this process that close relatives sometimes enter the room to place a cap on the head or tie a final bow.
“A common theme that comes out is how angelic they look. It’s very comforting for families,” Weinstein says.
Yaelle Schachna was praying in a room next door when her late grandmother was undergoing tahara. She joined for the final stage. “I gave my grandmother a kiss and it was very peaceful for me to see her. I could say goodbye.”
Last year, Schachna became a Chevra Kadisha volunteer. She this week helped send off her great aunt in a purifying ritual.
“For the first time, I stood there and was teary the whole time,” she says. “It was a beautiful send-off. I think you can hear in my tone the holiness I feel.”
There are two methods of looking after a dead body. One is through cleaning and cooling, which slows rather than stalls decomposition. The other is with embalming, which involves injecting chemicals such as formaldehyde and methanol to prevent the corpse from degrading.
Death positive advocate Dr Pia Interlandi, here pictured in 2014, runs Garments for the Grave.
RMIT senior lecturer Dr Pia Interlandi has been involved with the death-positive movement for a decade, creating bereavement casts – one of which she made for Anson of her and her mother’s clasped hands – and running Garments for the Grave.
Interlandi believes the movement goes together with attitudes on living sustainably. “If you love composting and the environment, it doesn’t make sense to be embalmed with chemicals and put in a box lined with plastic,” she says.
“Embalming is sold as a perceived psychological protection to seeing the dead body of a person you love. The natural death movement is about saying ‘you can cope with this’.”
Interlandi says that it might feel “strange” to see a dead body at first, but the slowness of death care allows you to move through the shock. “Dressing my nonno [grandfather] was the most transformative moment of my life,” she says.
Moloney explains that dead bodies become cold and pale, while limbs stiffen and get heavy, but these changes act as signals that the person is ready to be returned to nature. “It’s incredibly powerful and healthy to see those gentle changes; they inform our subconscious that we need to prepare to separate from their body.”
Ana and Thea Lamaro pictured together before Ana’s death in 2016.
Thea Lamaro’s mother, Ana, began to prepare for her death two years before she died of breast cancer in 2016. She decided she wanted her body to be taken home to her apartment after her death, and not be left alone for three days.
Ana’s body was washed and dressed in a shroud by family and friends and Thea spent time talking to and holding her mother.
“I felt so comforted by having her body in the house. When I woke up throughout the night I could go to her,” Thea says.
“[It] helped me so much to integrate the fact she had finally died. It was a very gentle way of saying goodbye.”
Thea, who is developing a podcast series called Approaching The End speaking to people preparing to die, says she appreciated being able to decide the moment her mum’s body left the house: “I was letting her go rather than having her taken from me.”
Interlandi hopes that our conversations on death evolve past the question “do you want to be buried or cremated?” and towards: What type of funeral do you want? Who do you want to be cared for by? How do you want to be dispersed?
“People think it’s hippie woo-woo, and it’s not. There is a spiritual component, of course, because this is ritual – but it’s about choice and how you identify yourself in life goes into how you identify yourself in death.”
— As much as I may have resented it, cursed it, allowed myself to become embittered at times, I did what I chose to do. And I would do it all over again.
By Tracy Grant
I was my mother’s primary caregiver in the final three years of her life, as she struggled with dementia and the physical and emotional tortures that visit the afflicted.
If I am to be honest, I did it out of a sense of duty but not always joy or love.
I spent three or four days a week with her, including every weekend, not because anyone told me I needed to, but because I was the woman she had raised: the good Irish Catholic daughter of immigrants who never stopped craving her mother’s approval and affection. But during those three years, there were times when I would have sold my soul to not visit her, struggle with the wheelchair as we went for a drive, cajole her to eat and talk (endlessly) about the weather.
There were times when her eloquence about her condition moved me to tears, including when she told a neurologist that it “felt like my mind is shrinking in my head, doctor.” There were times when she would talk about “praying to God to just make me stronger.” And toward the end, there were times when she would say she just wanted to die.
I have never felt more helpless, searching for answers that would bring her some measure of joy, of comfort, of peace in a dynamic that was endlessly changing but inexorably heading toward a known conclusion.
That conclusion came March 1 when my mom died. I hope it was the blessing for her that I imagine it to be.
The author’s mother, Alice Ramsey, at Brookside Gardens in Maryland in 2022.
On the days when I’m a believer, I can imagine her reunited with my dad, her parents, her siblings and even my own husband. I can see her dancing, laughing and chiding, bringing her unique style to the Pearly Gates: “St. Peter, have you thought about changing out the drapes for window shades?”
On the days when I’m not a believer, I console myself with the knowledge that she is at least free. Free of the anguish that tormented her as her mind was stolen from her; free of the physical pain and infirmity that had marked those last years, months and days.
In those days before her demise — both the believer and nonbeliever days — I had prayed for her death. For her, yes. But, shamefully, for me, too.
The author’s mom Alice Ramsey and son Andrew at her house in Illinois in 2019.
The last good afternoon
Mom fell in her assisted living apartment on a Saturday, just hours after I had taken her to lunch at her favorite restaurant and we had sat by the fire in the common area and chatted with other residents. By the massively diminished standards she lived by, it had been a good afternoon. The last good afternoon.
We would spend hours in an emergency room before getting the dreaded diagnosis: broken hip. We had multiple conversations with doctors about treatment. She needed surgery they said at the same time they warned that survival beyond a few months in someone her age, with her underlying conditions was unlikely. “Why,” I asked, “should I put her through surgery?”
The answers that came back were disparate and betrayed how even well-trained, caring doctors (which all of them were) struggle to deal with end-of-life issues
The cardiologist seemed to indicate that while she could tolerate surgery, he, too, was unsure of the end goal. The hospitalist (a reasonably new specialty that I had not heard called this before) made the most compelling argument that without surgery any movement for however long she lived would be excruciating.
The surgeon, not surprisingly, looked at me as if I were insane. Surgeons operate; they fix things — or they delude themselves into thinking they are fixing things.
In the end, Mom had the surgery, but when she nearly choked to death two days later because she couldn’t remember how to chew, I asked to see the palliative care doctors: Hospice was the only route left.
The author’s mom, Alice Ramsey, and son Andrew and the author’s dad, Frank Ramsey, with her other son, Christopher, in the late 1990s.
The hospice team at the hospital, in the county where Mom lived, and at her assisted living were phenomenal. And my being able to bring Mom back to her beautiful apartment, surrounded by a lifetime of carefully chosen mementos, was a gift to both of us.
A peaceful last hour
She lived for six weeks, eating next to nothing. In her last cogent conversation with me, I told her: “Mom, I just want you to know how much I love you.” And her reply, fully my mom, was: “Will you shut the hellup? I’m tired of hearing you say you love me, when you won’t kill me.”
She was ready. I was ready. And for six weeks, I sat with her, trying to calm her as she clearly hallucinated seeing dead people. Praying for her to die. Begging God to take her. Believing there was no God because how could a loving God allow her last days to play out this way? Thinking “What would be the harm?” in advancing the inevitable. And forcing myself to get up and go for a walk when the voice in my head asking that question became too loud.
In the end, Mom died in my arms, listening to music from the playlist I had made for her early in the pandemic. The last hour was incredibly peaceful, and it allowed me to forgive God some of the previous six weeks — and three years. I said some things that needed to be said and hoped she heard me.
The visceral reality of grief
But now, almost two months after her death, what I feel is not the relief I had anticipated. I go to the grocery store and have to remind myself not to buy bananas for her. Alexa, the voice assistant, still reminds me that I might want to order again the jellied fruit candy that she loved so much.
I feel adrift, untethered, without my mom to care for. As much as I resented the role of caregiver at times, I can’t help but think she would love to feel the warmth of the spring sun on her face; I can’t help but wish that we could go for one more trip to see the tulips at Brookside Gardens.
The author (left) and her sister Paula Antosik (right) with their mom Alice Ramsey at the author’s home in Silver Spring in 2020.
As much as I may have resented it, cursed it, allowed myself to become embittered at times, I did what I chose to do. And I would do it all over again, because sometimes, in the last three years, I made my mom laugh. Sometimes we sang a mean duet to one of those tunes on the playlist. Sometimes she admitted that she needed help and let me be the person who helped her.
And that’s the thing about grief and loss. They pay no heed to logic or reason. The rational statement: “Mom is at peace” can be absolutely true and completely irrelevant when juxtaposed against the visceral reality of grief.
The number of people dying in their own homes has risen since the Covid pandemic and one Scottish health board has taken the controversial step of cutting hospice beds to provide more palliative care in the community.
Over the past three years, NHS Fife has adapted its service by closing more than half its hospice beds to try to reach more patients at home.
The move has caused local controversy, with many calling for hospice beds in Dunfermline to be reinstated, but specialist teams say they are now able to respond more quickly and flexibly to people in pain and distress.
Lisa Potter is one of those receiving end-of-life care after at her home in Dunfermline.
The 52-year-old was first diagnosed with cervical cancer in 2017 but had been all-clear for almost five years when hip pain was revealed to be cancer and it was incurable.
Lisa said the hardest part was for her family as they watched her get more ill.
“They’re all there and they feel helpless and don’t know what to do,” she said.
“There’s nothing they can do, they’ve just got to stand-by and hope for the best and hope that I’m comfortable.”
After a stay in hospital, her health deteriorated and Lisa wanted to be cared for at home where she has enjoyed the “little things” like family TV nights and her own bed.
She said “there’s not a lot of independence” with her illness but that she wanted to stay at home as long as she was comfortable then die in the hospice.
“I think it’s great I’ve got that choice,” she said.
“It makes it easier for me. I know I’m getting the choice to go to the hospice and my family are not watching me die upstairs.”
Deaths at home
Most people still die in hospital but the number of people dying at home has been increasing in recent years.
It reached a peak level in early 2020 at the height of the Covid pandemic but has remained high since then.
Figures for March 2023 show there were 1,782 deaths at home or in non-institutional settings, which was 17% above the five-year average.
The latest figures show that last week almost a third of deaths were at home (365).
As more people live longer with long-term conditions and advanced illnesses the demand has grown for end-of-life care a home.
In Fife, palliative teams work with GPs, district nurses, care home staff, hospital clinicians and charities to support people living with terminal conditions.
Dr Jo Bowden, a consultant in palliative medicine, described the greatest value of her specialist team as their ability to respond when people’s needs changed quickly – whether that was because of distress, physical symptoms or family circumstances.
She said work had been ongoing for years to change the service but at the start of the pandemic fewer people wanted to come into the hospice so they had too many nurses and doctors in that facility but not enough working in the community.
“Preferences often change with time but very clearly most people would choose to spend most of their time as their illness advances and towards the end of life at home,” she said.
“It’s not possible for every person but even for those people who need to come in either for a short spell or at the end of their lives the majority of their life lived will be at home.
“So that tells us that the majority of our resource needs to be there,” Dr Bowden said.
Inpatient care
Eleven beds in the hospice were closed to free-up staff and provide care that had only previously been available in the hospice setting. That has left eight hospice beds in the area.
Prior to the pandemic, the specialist team could look after a maximum of 19 patients but that has increased to 60 people under the changes.
Staff had previously only been able to work in particular settings but have changed to being able to work in any care setting on any day.
Demand for hospice care remains significantly lower than pre-pandemic in Fife. Since the changes, waits for a hospice bed have halved to one and a half days.
Before the pandemic 80% of the service budget was spent on inpatient care.
“We absolutely acknowledge that whenever bed closures are talked about, it causes anxiety,” Dr Bowden said.
“What we believe very firmly is that we’re delivering more for more people by using our resources more effectively.”
Jane Morris worked as a district nurse before moving to work with the specialist palliative care team. She can see a big difference for patients.
She said: “We struggled to get care to keep people at home before but now we’ve got it on tap.”
Proposals to permanently maintain these changes to the palliative care service in Fife are due to be considered at an Integration Joint Board meeting later this month.
However, more than 2,000 people have signed a petition launched by Claire Baker MSP calling for hospice beds in Dunfermline to be reinstated after closure of the ward at the start of the year. All inpatient hospice beds are now in the Victoria Hospital in Kirkcaldy.
The Fife Labour politician believes palliative care should be provided as locally as possible to support families and give people the choice so she wants to see the plans to make these changes permanent paused.
A new Scottish government palliative care strategy is due to be published later this year.