When sheriff’s deputies in Florida went to perform a welfare check last month on Tori Bowie, the Olympic runner, they made the saddest possible discovery. Bowie and her newborn daughter were dead. Though the full story of Bowie’s last days has yet to emerge, some details are clear: She had died in labor, suffering from eclampsia and respiratory distress.
Expectant moms deserve more from their lawmakers, providers, public health groups and hospitals: more visits before and after pregnancy, better access to the simple drugs and devices that could keep them alive, and expanded insurance coverage.
Since the federal government began keeping records in 1987, America’s maternal mortality rate has only gotten worse. Between 2000 and 2020, the United States was one of eight countries where the situation deteriorated fastest, a list that included Venezuela and Mauritius. There’s no one cause of this long slide: A strained health-care system, a stingy insurance system, a lack of paid leave, the retreat of reproductive rights and endemic racism all contribute.
Covid-19 made a bad situation worse. Pregnant women who contracted the virus were seven times more likely to die than those who avoided infection. But even as vaccination became widespread, pregnant women kept dying from all the more common causes: infections, hemorrhages, hypertensive disorders such as preeclampsia and embolisms. In 2022, 733 American women died while pregnant or shortly after childbirth. That’s a maternal death rate of 20 per 100,000 births — up from 17.6 in 2019, already two or three times the rate of many high-income nations.
For Black women, pregnancy and childbirth bring the toll of racism in the United States into sharp focus. A large body of research shows that being Black in America wears on women’s bodies, leaving them uniquely vulnerable during pregnancy. Black women are 60 percent more likely than White women to experience preeclampsia, for instance. Add to which they experience inequalities in access, quality of care, prescribing, data collection and more. These differences persist even among wealthy, educated women. So stark is the disparity it has come under United Nations scrutiny.
There’s much providers can do to help: A 2019 analysis of preventable maternal deaths by the Centers for Disease Control and Prevention gives a clear list. Open earlier or stay open later to serve patients who work nights. Accept Medicaid. Educate patients early and often about conditions to watch out for. Take patients with headaches or shortness of breath seriously.
And there’s a lot policymakers must do to keep pregnant women safe and healthy. Fortunately, even in this divided, fractious Congress, there’s bipartisan support. Bills introduced by Reps. Lauren Underwood (D-Ill.), Robin L. Kelly (D-Ill.) and Robert E. Latta (R-Ohio) and Sens. Charles E. Grassley (R-Iowa) and Maggie Hassan Wood (D-N.H.) would pull together working groups to identify the best ways forward. One target of Kelly and Latta’s: Finding ways to identify and improve hospitals and doctors who are failing women and babies.
Lawmakers in both parties agree that childbirth and postpartum support from other practitioners matters, too. Evidence is accumulating that access to doula care during labor can lower Caesarean section rates. Doulas offer mothers nonmedical support and advocacy before, during and after delivery. Programs run both by community groups and insurance giants are exploring whether doulas can have a measurable impact on maternal mortality, especially for Black women.
Congress funded some home health visiting programs in the 2022 government appropriations bill. The United States should join other wealthy countries in making sure new mothers get regular visits after they come home from the hospital, when they are still at risk.
It would also help to standardize how Medicaid covers the medicines and devices for pregnant people. An analysis by KFF found glaring gaps. Four state Medicaid programs still don’t cover low-dose aspirin, which can prevent preeclampsia. Ten don’t cover blood pressure monitors for use at home between doctor’s visits. And six states don’t cover glucose monitors, crucial for managing gestational diabetes.
Meanwhile, the federal government could kick-start pilot programs that explore new ways to lower maternal mortality. Examples include payment schemes that compensate providers who do a better job for mothers and babies or demonstration projects that bundle housing and prenatal care in the same setting.
We don’t know whether Tori Bowie and her baby could have been saved with earlier intervention. We do know how to save hundreds of other American mothers.
When a white supremacist murdered Mindy Corporon’s father and eldest son outside the Jewish Community Center in Kansas, the grief and despair were debilitating.
“It physically caused foggy brain and exhaustion, which complicated my return to work,” Corporon tells HRD. “I knew I needed to create something good from this tragedy – something that would help people through the kind of mess I experienced. Workplace Healing is a legacy to my dad and son.”
Sadly, Corporon’s not alone. Unsupported grief in the workplace costs companies up to $225.8 billion every year, according to the Center for Disease Control.
Personal versus professional grieving
Corporon co-founded Workplace Healing – a counselling service to help leaders, managers and care teams support grieving employees. Something Corporon would have appreciated when her own grief hit.
“As the CEO of a wealth management firm, I had to go back to work,” she tells HRD. “I found myself wearing two different hats – the CEO and the griever, and some days I’d be one, the others day I’d be the other. I knew, when I would walk in as the griever, that I shouldn’t be talking to clients. And then as the CEO, I wanted myself back. However, I knew that it was very difficult – I had to teach my team, how to speak to me, when to speak to me what topics to talk about.”
It made for an interesting dichotomy – having to jump between being a leader and being a grieving mother and daughter. The issue with grief is that it’s inherently personal – how we deal with loss differs from person to person. As such, employers need to start educating themselves on how they can help the individual at work – and never shy away from uncomfortable conversations.
“Grief and loss are a part of our human condition, and this can impact each of us in different ways,” says Dr Raeleen Manjak, CHRO at the City of Vernon. “It’s important to remember that these impacts do not dissipate when time away ends. The return to work might find the employee in the midst of their grief in the workplace or they may be struggling to put up a strong front.
“Knowing this, and remembering that grief is a natural response to loss and that all of one’s sense of self can be impacted, it’s important to remember that as employers navigate these often-unpredictable times. As such, grief is an individual experience,” she says.
Most Read
This is best captured in the Kubler-Ross Model of Grief, famously categorizing the five stages of grief – denial, anger, bargaining, depression, and acceptance.
America’s bereavement leave policies
The process of grieving is not helped by America’s limited availability of bereavement leave. There’s no federal law that mandates organizations to provide paid time off after the death of a loved one – that’s entirely up to individual company policies – and there is no mandated paid time off to attend a funeral.
This means employees are using personal days off to deal with funeral arrangements and estate issues – leaving little time to actually grieve. Only two states have local laws – Oregon and California. Oregon state government provides leave to employees according to the Federal Family and Medical Leave Act (FMLA), the Oregon Family Leave Act (OFLA) and the Oregon Military Family Leave Act (OMFLA). This law allows employees to take up to two weeks per family member in a one-year time period.
In California, the new AB 1949 is law requires employers to offer workers – who have been with the company for over 30 days – up to five days’ bereavement leave upon a family member’s death. This leave doesn’t need to be taken on consecutive days – and the leave doesn’t have to be paid.
While it might not be federally mandated in other states, many employers allow employees three to five days off. According to data from BetterUp, 88% of companies offer paid bereavement leave.
Educating leaders on the economics of grief
The situation isn’t just stressful for the employees who’re grieving, it’s unknown waters for managers too. According to data from NCPC, 31% of employers would welcome some help on how to support bereaved employees – especially when it comes to making the first move.
“What we found when we began our focus groups is that people are scared to talk about death,” says Lisa Cooper, co-founder of Workplace Healing. “They’re scared that if they bring up the name of Mindy’s son Reat, that many will remember that Reat was murdered when he was 14. Well, Mindy is never going to forget that. Just as I’m never going to forget that my parents have passed away – and when I tell stories about them, when I share stories, it makes me smile.
“Most people in our society, especially in the United States, are scared to talk about death. It makes them feel uncomfortable. As such, we’re raising the level of grief awareness in the workplace, so that people feel supported and cared about by their teams.”
Supporting an empathic culture
Empathy isn’t a box-ticking exercise for employers, it should emanate into your entire culture – especially in the current talent crisis. According to BusinessSolver’s 2021 ‘State of Workplace Empathy’ annual study, 92% of employees say they’re more likely to stay with an empathetic employer, with 84% of CEOs believing that a company’s financial performance is tied to empathy in the workplace. What’s more, almost 75% of employees are willing to work longer hours for an empathetic employer.
“The impact of grief in the workplace can occur at the individual, department, and organizational levels,” says Manjak. “It’s common to see higher levels of absenteeism – while out of the workplace – or even presenteeism upon return to the workplace. The employer can provide support to those grieving by offering time off and support networks.
“All of this must be reviewed and considered on an individual employee basis. The employer can offer increased levels of support during the transition back to work by offering a discussion about what the employee can manage during this time.”
‘It’s okay to not be okay’
Op top of this, Manjak advises employers to invest in the following essential grief-led benefits;
EAP programs
Critical Incident Response Teams
Training, Learning and Development
Workshops
Employee Resource Groups (ERT’s)
The crux of the issue for leaders is to bring a culture of understanding and empathy to the workplace – one in which employees feel comfortable enough to bring their whole selves to work. No matter how uncomfortable those initial conversations seem.
“A lot of times in corporate America, whether you’re working from home and turning on your laptop in the morning or walking into an office at 8 am, you cannot leave your personal life at the door,” says Cooper. “It’s impossible. The good news is that it’s becoming forefront in our world right now post-COVID to talk about mental health – to say, ‘It’s okay to not be okay.’
Scientists believe that burial practices and funeral rites were reserved for humans with brains and large brains compared to other species, so have scientists been able to find any burial practices other than humans that undermine this idea?
By Nadia Barnett
In a cave in South Africa, scientists have discovered ancient burials dug by a small-brained species known as “Homo Naledi” – 100,000 years earlier than the earliest known burials of “Homo Sapiens”, disrupting the story. According to the “Washington Post” newspaper, scientific research on the theory of evolution is subjecting scientists to fierce debate.The Washington Post)
A team exploring the “Rising Star” cave northwest of Johannesburg said they found limestone walls inscribed with triangles, squares and intersecting lines. years ago.
These results were announced Press conference It was hosted by Stony Brook University in the US on the fifth of June, it appeared Two sheetsTwo Flags Both first editions are published in bioRxiv.
Both studies are still under scientific review before being published in the journal eLife.
💀 Pushing back the first sign of burial by thousands of years
These results are very exciting, and in 2021 it was Old A known burial site dating back 78,000 years belongs to a human child.
These results come after many years discovery The species, which scientists call “Homo naledi,” is characterized by its short stature (about 1.5 meters in length) and its small size, including a brain that weighs about one-third the size of a modern human. Contains both very old and relatively modern anatomical features.
Voluntary Funerals
The skeletal remains were discovered during archaeological excavations that began in 2018, and most of the skeletons found by scientists in one part of the cave date from 335,000 to 241,000 years ago, which is modern times. Humans began to appear in Africa.
Scientists found these graves in burial pits at the end of a tangle of narrow galleries, and the graves were filled with earth, which was originally used to make the pits, indicating that the bodies of these men were buried voluntarily.
However, these results caused controversy among scientists after they were announced, as their opinions differed sharply on the evidence proving that “Homo Naledi” buried his dead, and some scholars pointed out that there is no evidence that these inscriptions are thousands of years old. Old, step to inform Published by National Geographic.
The controversy reflects the degree of tension that our understanding of ancient history and new scientific discoveries periodically monitor, and if the results of the last two studies are correct, it could undermine the practice of burial. The preservation of our species, “Homo sapiens”.
Controversy
And Lee Berger, a paleoanthropologist and head of the research team, said, “People have always wondered about their position in finding another culture as complex as our own human culture … Well, we’re facing one of these now, and it’s a huge moment in human history.”
The findings open the door to the possibility of cremation among hominins with smaller brains and lower intelligence, scientists say.
This idea counters the prevailing view that awareness of death in general, and funerary rituals in particular, are uniquely human, and that these burial practices are a relatively recent thing, known to mankind over 100,000 years ago.
In a statement published by the “Science Alert” website – says Berger.scientific warning)– “We are going to tell the world that this is not true,” he concludes, “and that the symbols carved into the stones also indicate that humans were not the only ones who developed these practices.”
Sherry Campbell, director of Welcome Home, stands with former resident Clint Jackson outside the hospice and medical respite home in Chattanooga, Tennessee, on April 2, 2023.
A few years ago, Mark Adams was diagnosed with colon cancer. His doctors didn’t want to operate, he said, because his recovery could be too risky without a clean place to recuperate. He was living on the street.
Soon, it was too late, his cancer too far along. That’s what they discovered after he moved into Welcome Home, a facility offering long-term medical respite and end-of-life care for unhoused adults.
Instead of getting better, he’ll likely live out the rest of his days there – one of a small number of places in the United States that offers unhoused people a comfortable and dignified option when they are terminally ill.
Sufficient end-of-life care in the United States is a growing problem for the general population, as America’s aging baby boomer generation needs more intensive and expensive help and supply isn’t keeping up. For many unhoused adults — who frequently lack a strong social safety net — long-term medical or hospice care are effectively inaccessible. In the absence of publicly funded solutions, private organizations and nonprofits are trying to plug the gaps, but the patchwork network of end-of-life care homes is far too limited to address the need.
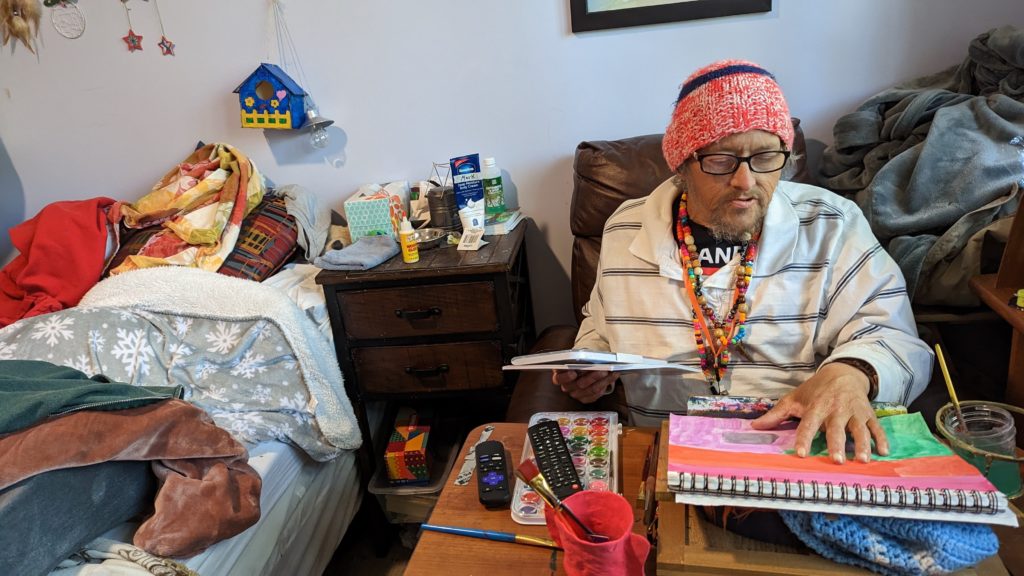
On a mild spring Sunday, Adams worked on a painting in his cozy, eclectic room – filled with vinyl records, potted plants and his own art – while his friend Clint Jackson relaxed nearby. Up the hill, Standrew Parker rested on a wrought iron chair in his yard, soaking up the early afternoon sun and chatting with his new roommate, Heidi Motley. Parker, 40, and Motley, 58, are staying there while undergoing treatment for cancer.
Mark Adams displays his artwork in his room at Welcome Home in Chattanooga, Tennessee, on April 2, 2023.
Across the country, there are a handful of facilities like Welcome Home, which sits on nearly five forested acres in Chattanooga, Tennessee. Some 1,300 miles west, there’s Denver’s Rocky Mountain Refuge for End of Life Care. Salt Lake City is home to The Inn Between, while Washington, D.C. has Joseph’s House. In Sacramento, Joshua’s House plans to open its doors this fall. Dozens more offer medical respite beds, generally for those undergoing long-term medical treatment. But outside of these organizations, experts told the PBS NewsHour that there are few other places where people experiencing homelessness can go for end-of-life or hospice care.
These facilities aren’t massive – Welcome Home has three medical respite rooms in addition to its four hospice beds, and is opening another house with an additional three rooms this month. Rocky Mountain Refuge, the smallest and newest of the group, has three beds solely for end-of-life care.
The need for those beds is great: People who are homeless are at far higher risk for many illnesses and conditions, such as heart disease. Medical research also shows that unhoused people’s bodies have often aged as if they were at least a decade older.
Being without a home is itself “a life-limiting diagnosis,” as Hannah Murphy Buc, a researcher who studies palliative and end-of-life care for people experiencing homelessness, wrote in the journal Caring for the Ages.
When someone is already in poor health, there are basic obstacles of living without a home – not having access to a fridge to store medications or the ability to secure narcotics for pain management, for instance. Some people without permanent addresses, like Adams, have reported they were denied treatment for their cancer due to the physical demands of recovery.
“Hospice and palliative care, but particularly hospice, is completely reliant on having a place to receive it,” Murphy Buc told the NewsHour.
For Adams, 51, living at Welcome Home has been life-changing, even though he often feels sick and he says he knows the cancer will likely kill him.
“I feel good here. I feel like I’m welcome here,” he said.
What we know about deaths among the unhoused
There is no official national data on where, when and how people experiencing homelessness die. According to an analysis by the National Health Care for the Homeless Council (NHCHC), at least 5,800 people died while experiencing homelessness in 2018. That’s almost certainly an undercount, and the report noted the actual number could have been anywhere between 17,500 and 46,500 deaths for that year.
With more people expected to become homeless and as that population ages, that mortality figure expected to rise, said Dr. Margot Kushel, director of UCSF’s Center for Vulnerable Populations and Benioff Homelessness and Housing Initiative.
“The truth of the matter is most of the country is entirely unprepared for this,” Kushel said.
An inspirational sign is displayed near a cookie jar in the kitchen of Welcome Home, in Chattanooga, Tennessee, on April 2, 2023. Residents gather nightly for dinners provided by volunteers as a way of fostering community.
Local reports can help explain what’s happening currently to those who can’t access end-of-life care. Across several months in 2021, deaths among unhoused people in San Francisco occurred primarily outdoors, in places like encampments, vehicles or on the street, a report from the NHCHC found. Others died in medical facilities; motel rooms, either rented by the person or as a shelter-provided space; other people’s homes; and homeless shelters.
Similarly, in King County, Washington, about half of the people experiencing homelessness who died in 2018 perished outdoors, according to a report from the council. Only 26 of the 194 deaths occurred in residences.
A 2022 report from the Colorado Coalition for the Homeless found that among the unhoused individuals who die of so-called “natural causes,” 30 percent died in hospitals or other medical facilities, and 25 percent died outside.
“That means under a bridge, on a sidewalk, behind a bush, in a tent,” said Brother James Patrick Hall, the executive director of Rocky Mountain Refuge.
While in prior decades people experiencing homelessness may have died from acute causes, such as violence or illness, the aging population of unhoused people is now living with the chronic conditions that plague many seniors, such as COPD, heart failure, strokes and cancer.
“These folks often need a lot of personal care. They have pain issues … It’s like a disaster, to be honest,” Kushel said. “What we found in Oakland is [that] a lot of folks just died on the street, short of breath, in pain, incontinent.” Others were admitted to hospitals, and some ended up at nursing homes or acute care facilities, “but it wasn’t where they wanted to be.”
When given a choice, people overwhelmingly want to die at home, according to Murphy Buc. Death at home can lead to healing in relationships and help soothe those left behind. But even when that’s an option, it can be draining for those doing the caretaking, she noted, even with hospice nurses visiting a few times a week.
In the U.S., “we don’t do death well,” Murphy Buc said.
The problem of older people dying on the streets, in motel rooms and in cars is the ultimate result of disinvestment in affordable housing, skilled nursing care and health care, experts at the NHCHC told the PBS NewsHour.
It’s not that people who become homeless are falling through the cracks, said Barbara DiPietro, senior director of policy at the NHCHC. Instead, people are often forced into “gaping caverns” where underfunded social safety nets, such as Medicaid and public housing, fail to catch them.
An older adult who has worked as a manual laborer her entire life might have a stroke and lose employment, be unable to pay rent and end up without a home, said Caitlin Synovec, senior program manager with the council’s medical respite team. Shelters frequently can’t help people with enhanced medical needs, so they have nowhere else to turn.
The unhoused population is also disproportionately vulnerable, low-income and people of color — all groups who have historically experienced disparities and may distrust the nation’s health care and social services systems.
In addition to that added barrier, people may just not know they have medical respite and end-of-life care options, Murphy Buc said. Many of the current residents of these facilities were referred there by health care professionals or social workers, but had not previously heard of them.
‘Health care isn’t housing’
Having a home, in and of itself, can be considered a form of health care, advocates say. Those who work or volunteer at care homes sometimes witness very sick people make dramatic recoveries simply because they have a safe, comfortable and stress-free place to live.
Though each facility operates slightly differently, these homes offer more than just a physical address, providing services like palliative care, case management and transportation. Volunteers and staff can remind residents to take medicine, ask how they’re feeling, and, crucially, drive them to appointments.
Before Standrew Parker lived at Welcome Home, he would have to travel to the hospital from his mother’s house to receive five days of cancer treatment every few weeks. In addition to being an unwelcoming environment, her house was about 45 minutes away by rideshare, which cost around $60 to $70, he said. To avoid the trip back and forth, he would instead often spend his days living outside the hospital.
“We didn’t have that money. So I was in and out, just like hanging out. If I had multiple appointments for days on end there, I just [stayed outside the hospital]. I would have to or I wouldn’t get the correct shots or the treatment,” Parker said.
Crystal Jones, nurse case manager at Joseph’s House in Washington, D.C., works at her desk on April 4, 2023.
Now, volunteers drive him to and from his treatments, and during his weeks off from chemotherapy, he recuperates in his room at Welcome Home. Beyond the care he receives, the empathy and compassion from staff and volunteers helped shift his entire perspective on healing.
“It’s like a world of difference between surviving and actually being able to get well,” he said.
A crucial goal of each facility is to establish a sense of normalcy for people whose lives have been thrown out of balance. Welcome Home serves dinner every night, where residents can gather and rib one another. People living at The Inn Between can join the resident council, which offers both community and a way to effect change, such as what times coffee is available. For the patients who recover enough, these homes can help them adjust to life outside of the facility so they can leave.
When NHCHC began their medical respite programs in the late 1980s, they were originally intended as short-term stabilization. However, some of the programs that specialize in medical respite have begun to consider incorporating end-of-life and hospice care into their models to fill the gap, said Julia Dobbins, director of medical respite at NHCHC’s National Institute for Medical Respite Care.
In contrast, patients without somewhere to go sometimes cycle between a hospital and the street, being readmitted when their problems are acute enough to warrant immediate care, and released when they’re stabilized, Murphy Buc said.
Sending still-sick people back to the streets is called “patient dumping,” and “it’s horrible,” Kushel said. But, she added, the solution can’t be that people live at a hospital for months on end until they die. That’s an inefficient use of resources, not to mention that it’s unlikely to be where a patient wants to spend the rest of her life.
Hospitals don’t want to deny people care, Kushel said. When she heard about Adams’ doctors refusing to treat his cancer while he was experiencing homelessness, she noted that his situation was not uncommon. Doctors worry about harming people who don’t have access to long-term, safe and clean care, but it doesn’t make it an easy decision.
“It happens all the time,” Kushel said. “And when you speak to the surgeons, they actually feel terrible about it.”
In the long run, even medical respite doesn’t solve the problem of where people can live, said NHCHC’s DiPietro.
“We often say housing is health care. Absolutely,” she said. “Unfortunately, health care isn’t housing.”
For many, providing medical respite or end-of-life care to people experiencing homelessness with their own limited resources can feel like a Sisyphean task.
For every person given a bed, there are countless others who need and can’t access one. Each organization can only serve their local community, leaving hundredsof people or more to dieon the street nationally each year.
Beyond what the organizations receive from state and local funding, there’s little — if any — government funding for long-term medical care or end-of-life care for people with no fixed address. These organizations’ funding models are largely reliant on grants and donations, without long-term stability.
“It’s local advocates who are seeing the suffering of their community members, and so they’re creating these programs that are funded by the good of people’s hearts, and that’s it,” Dobbins said.
Rocky Mountain Refuge, which opened its doors a little over a year ago, struggles to find enough funding to stay open, Hall said. That’s an experience echoed across the country.
“One of the stresses for us here is, every year, are we going to be able to keep our doors open because of the funding?” said Kowshara Thomas, director of Joseph’s House in Washington, D.C.
Founded in 1990 during the HIV/AIDS crisis, the three-story house in a quiet residential neighborhood has served community members dying of the disease for decades. This year, however, they lost a major grant that comprised 30 percent of their revenue, which worries Thomas. Other medical respites in the D.C. area receive Medicaid funding, and larger organizations are often better positioned to write grants and secure funding. But Thomas says Joseph’s House, with only eight beds, is too small to follow suit.
A memorial wall of former residents is displayed at Joseph’s House in Washington, D.C., on April 4, 2023.
The organization has largely, though not entirely, pivoted from end-of-life care to medical respite, something Thomas sees as both a result of better health among their community and a way for them to provide continuing care for people after they’re discharged. Joseph’s House has around 25 community members for whom they provide supportive services.
Thomas is also proud of the community that Joseph’s House anchors, with former residents coming back for meetings, social time and sometimes additional long-term or end-of-life care.
“Having a place where you can feel safe and get the support — the medical and the psychosocial support — is really what helps our community,” Thomas said. “Joseph’s House is, for some of our residents, the first time they’ve ever had family or felt like they belonged somewhere and they could just be who they are.”
Watching a loved one face dementia is often heartbreaking and disorienting.
They may forget where they are, repeat themselves, or get confused and agitated. Over time, as memory disorders damage cells in the brain and nervous system, they’ll need someone to care for them. Their speech, personality and thinking can also shift. There might even come a day when they don’t recognize you.
It’s called “the long goodbye.” While groundbreaking new medications could slow Alzheimer’s disease progression, there is still no cure for the estimated 6.7 million Americans with the condition, according to the Alzheimer’s Association.
On average, a person with dementia will live about 10 years or more after diagnosis, said Zaldy Tan, MD, director of Cedars-Sinai’s Memory and Aging Program, medical director of the Jona Goldrich Center for Alzheimer’s and Memory Disorders, and the Carmen and Louis Warschaw Chair in Neurology. Knowing what to expect can help you guide your loved one through those years with dignity.
Respect their wishes
Speak to your relative as early as possible in their illness, while they can still make decisions, about their plans and desires for end-of-life care and their finances—and honor them fully, Tan said.
“Just because they have dementia doesn’t mean they don’t have the right to live the way they choose to,” he said.
Losing independence can be one of the most challenging parts of a memory disorder.
“The trick is knowing how they liked to live before their illness,” he added.
When caring for or visiting with a relative with dementia, try to continue familiar activities they enjoyed. Did they often spend time with friends? Schedule regular meetings with one or two friends weekly or monthly. Did they have a sweet tooth? Then don’t cut out all sweets. Instead, space them out with healthier fruits and vegetables.
“Just because they have dementia doesn’t mean they don’t have the right to live the way they choose to.”
Dementia patients lose short-term memory first
In its initial stages, Alzheimer’s disease often causes patients to lose household or personal items, such as glasses, or to skip important appointments and tasks.
Families can help by offering cues, including placing labels on drawers, cabinets and doors to tell what’s inside and using calendars for medication schedules, meals, doctor’s appointments or due dates for bills.
While neurological diseases block these newer memories, old ones can resurface.
“Sometimes people revert to the past because that’s what’s accessible to them,” Tan said.
Their house and loved ones look different than they remember and therefore unrecognizable, and they might try to return to that past life in an attempt to “make sense of the world,” he explained.
Meet your loved one in their truth
There’s no need to correct them every time they believe or say something inaccurate—and it can do more harm than good.
If the person thinks they’re going to see a friend who died 10 years ago for a poker party, it will just upset and confuse them to mention the death. They’ll also likely forget within a few minutes.
“What does it accomplish?” Tan said. “They may not have the capacity to understand. Their reality is different from yours.”
Play along or change the topic, he suggested.
Use simple, direct and slow communication with yes and no questions (asked one at a time) and eye contact—in a quiet place with few distractions, the Alzheimer’s Association recommends. Visual and sensory signals like touch or pointing can also help you engage.
My family member was clear: She wanted her life to end without extreme measures — to go when it was “her time” with no life support, no CPR, no intubation.
Though my family and her spouse knew this and loved her dearly, the reality of letting her go and following her wishes without “doing more” became difficult as her condition progressed. At the time of her death, medical interventions had sustained her life for several years — against her wishes.
Unwanted, aggressive medical care at the end of life can not only rob you of a peaceful death, it can also place an enormous financial and emotional burden on your loved ones. Fortunately, advances in healthcare delivery at end of life, such as hospice and hospital-at-home options, are combining with more candid and open discussions of end-of-life care to reduce the number of Americans who die hooked up to machines in hospitals against their wishes.
But it takes more than industry shifts and education to ensure that you or your loved one have a desired end-of-life experience. If you want to avoid end-of-life hospital stays, some proactivity is required.
1.Know what documentation you need
What if you were in a car accident? How would you consent to, or decline, mechanical breathing intervention? Advance directives — which can include many different types of documentation — are more than just planning for far-off end-of-life scenarios.
An advance directive should account for any scenario in which you are unable to speak for yourself.
An advance directive should account for any scenario in which you are unable to speak for yourself and need a healthcare proxy to be your voice, whether at the end of a long battle with cancer or after being rendered temporarily incapacitated by a skiing accident. Everyone needs such documentation, not just the sick and elderly.
The documents that set out what a hospital, elder care community or other caregiving entity should and shouldn’t do on your behalf can vary by facility and state, and the methods for ensuring they are considered legally binding can also vary.
2. Designate a healthcare proxy and be real about your choice
The legal and healthcare system will decide for you if you don’t designate a healthcare proxy yourself, with your spouse being the default and adult children second. That’s a pretty solid default, but your closest loved ones may not always be the best choice
Ask yourself: Will they be able to let me go after a long life when I’m ready to rest? Yes? Lovely. But what if I’m in a car accident tomorrow and life support is offered? Will it be fair to ask this particular person to focus on such decisions? It’s quite possible. But it may be kinder and more prudent to say, “I love you, and so you’re not the one to make these decisions. I want you to be holding my hand when I take my last breath, not deciding if I should be on life support.”
For single people without children, it is imperative to have a detailed advance directive.
End-of-life decisions are particularly fraught for unmarried people. While the healthcare system does look for legally binding end-of-life wishes documentation, if no such documentation is found, there’s a possibility that a physician would expend unwanted efforts to extend your life. In extreme cases, the hospital ethics board could become involved in decisions you may have wanted to keep within your circle of loved ones. For single people without children, it is imperative to have a detailed advance directive.
3. Use free resources to plan with your family or doctor
Contrary to popular assumption, you don’t necessarily need an attorney to complete an advance care plan — though it may be advisable in specific circumstances. If you do choose to hire support, weigh that cost against the costs of not planning — which can include unplanned stays at nursing homes, costly interventions that may not result in extending life in a positive way, or family disputes over your end-of-life wishes.
Every state has free, downloadable documents for advanced-care planning available for their residents. If you find them challenging to navigate or understand, your physician can also guide you to social workers and other support. The secure online portal. My Living Voice is one example of a free resource that helps simplify the process of documenting your advance directive. It can help you to think through who your proxy should be, to document your preferences for care during a medical crisis or life-extending care, and to make those wishes both legally binding and known to your physicians, your insurance company, your healthcare proxy and your family.
Prioritize discussing an advance directive at the start of your next physician appointment with a simple ask: “I’d like to do an advanced care plan. How should we go about that?”
4. Share your plans
Too frequently we assume our designated healthcare proxy will “just know” that they are the proxy and how you feel about what decisions will need to be made. Too frequently, that simple communication and documentation doesn’t happen. If the role comes as a surprise to them in the midst of a health crisis (or even an anticipated health event), it can cause undue stress on someone you love.
Another common scenario: You have a living will, but it’s in a file in your closet, completely inaccessible to those who need it most, like your physician
Actualizing your end of life wishes requires that your advance directive is documented, communicated and accessible.
Actualizing your end of life wishes requires that your advance directive is documented, communicated and accessible. If required in your state, get it notarized. Communicate its contents with your loved ones and doctor. Provide your loved ones and healthcare providers with copies, both paper and digital if possible. Furthermore, if you have children, make your plans and proxy designation clear to each one of them to save them from agonizing disputes. Consider the right time to have these conversations with your family based on your unique family dynamic and set a time for that discussion.
Not sure how to start the conversation? Print this article and say, “I was reading this, and it made me think. Can you all read it too and then we can talk?” Legally documenting your wishes can provide your loved ones with peace, structure and protection at a time when they might have their head in their hands, saying, “I don’t know what to do.” Give them the strength and confidence that helps them take the actions you want taken.
— A death doula explains how to respect and accept different end-of-life choices
By Lee Woodruff
I was on the other side of the world when I got the text. “Did you know Karla is dying?” my friend wrote. “They called in hospice and she only has a few days to live.”
My enjoyment of a long-planned vacation with my husband suddenly came to a screeching halt in my brain. How could this be? I’d spoken to Karla * a few months ago and we’d celebrated the news that she was pronounced cancer-free. We’d gabbed away for almost an hour, catching up on kids, her future plans and the challenges with chemo, all with her signature optimism and honesty.
I was never someone Karla would have counted in her inner circle. We were in different places in life, my youngest kids still home at a time when she was enjoying dinners out and weekends away. I’d met her more than 20 years ago as part of a group of moms who sat on the sidelines at their kids’ games and drove one another’s children to playdates and sleepovers. Life had moved us to different cities, and a year or more would easily go by without seeing one another. Any time we spoke, we’d always pick right up where we’d left off. She was that kind of friend.
Listening to the relief in Karla’s voice on that last, long-ago phone call, I recalled that we’d talked about a getaway weekend with girlfriends at the beach and rebooting that group dinner we’d canceled when her doctor unexpectedly discovered a small, pesky tumor. The last of it, she’d said.
When communication stops
For the past two years, Karla had been throwing everything she had at the disease, using a combination of the finest cancer care, physicians and hospitals, with holistic medicines, organic foods and juicing. Nothing that contained any chemical or synthetics was allowed on or in her body. Karla, or so we thought, had won.
How had this rosy picture gone into a death spiral so quietly? It wasn’t so much the shock that the cancer was back. Live long enough and you understand that cancer is a sneaky thief. Anyone who has experienced a brush with cancer never fully lets their breath out. But still…. Days to live? How had someone who had brought us along so fully on the journey, who had grabbed life by the throat and been honest and transparent about her illness gone so quiet? How could we, her friends, not have known?
Next came the wash of guilt. Each person responds to illness or injury so differently. There is no one playbook or template. My style has always been to take the cues from others and to give everyone space to do what was comfortable. But now, knowing I wouldn’t make it back in time to see her, I regretted showing up at her door.
When my journalist husband was injured by a roadside bomb in Iraq 18 years ago, my instincts were to immediately pull the shades down from the outside world. The prognosis was so devastating, I wanted all my energy to tend to him and help our kids process what was happening. I drew my circle tight, initially letting in mostly family and a few trusted friends who helped with critical roles to move life forward. I understood shock and trauma, but it was hard not to personalize it, even though I knew that was ridiculous.
Loss is a part of life
At a certain stage of life, loss becomes a theme. And there is no question that when something strikes out of the blue, a sudden diagnosis, a death, accident, or a spouse who leaves, we cannot help but think of ourselves. How would we handle it? How will we handle it when it’s our time to die? I’d seen people around me die in many different ways, from flinging open the doors and having a party to closing the curtains and going quietly, as Karla had done.
My in-laws never wanted to talk about dying or even do much in the way of preparation. My mother talked about it frequently and matter-of-factly, especially toward the end. She had every detail prepared and outlined, but she lost so many opportunities to live in the moment. There is only so much we can control. What would I choose when it was my time? It was impossible to know.
End-of-life choices
Alex Rosen, 42, from Armonk, New York, is a death doula. Her job is to support, guide and provide companionship and comfort for those at the end of their life. Ideally, Rosen works with people from diagnosis through the transition to the end of their life, from their emotional state to the physical setting, whether it be in a home or hospital.
“How we choose to be and exist at the end of life is our choice and our personal journey,” she says.“When possible, it should look and feel how a person wants it to, within the confines of the medical system.”
Part of the work Rosen does as a doula is helping the person and their family accept death and make it feel as comfortable and safe as possible.
“In our society and culture, talking about death is so taboo. So many things are said privately and behind closed doors,” she says. “Part of being alive is understanding that all of us are going to die. The more we can talk about it, the more we can begin to accept it.”
One of the insights I gleaned from talking with Rosen was the potentially harmful language we use around “battling” disease as a society. While comments about “waging war” against cancer can rally a patient to summon energy and desire to combat a disease, if the disease “wins,” there can be a sense of letdown.
“There’s a societal mentality around losing,” Rosen says. “And people who thought they’d ‘beaten’ the cancer or had the potential to, can experience a feeling that they didn’t fight hard enough, weren’t strong enough, that their body failed them. That mentality can bring a feeling of shame and failure rather than a sense of calm and peace at the end of a physical life.”
Karla was a competitor; I could imagine her devastation as she received the grim news from her doctor after a scan that revealed the cancer was back. The story didn’t sound right. From completely cancer-free to riddled throughout her body? But then again, this wasn’t information I had any right to know. This was Karla’s story to tell and to handle any way she chose. She had already been through so much.
The aftermath
I’m still processing Karla’s loss and the way in which we all learned about her dying. I’m still shocked on some level. The news feels like a rug that got pulled out from under me and others who knew her. And of course, there is still so much guilt and remorse over what I would have done differently, had I known. But guilt is a useless emotion, especially when it comes to death.
Karla wouldn’t have liked all this hand-wringing from her friends, and that thought comforts me. I am also consoled by the knowledge that she chose this. I know that this was the way she wanted it to go down because there were many opportunities to do it differently.
You take the good with the bad, I can imagine Karla saying. And I’ve had a pretty wonderful life.
My hope for Karla is that she got to experience death on her terms. By all accounts, she did.