To celebrate the 2nd anniversary of the publication of Longfellow And The Deep Hidden Woods I thought I’d share with you a touching review just published on Amazon.
Myste Lyn from Bittersweet Blessing shares her thoughts after reading the Longfellow book
A sweet, simple and soft book… more than a book on loss, it’s a book that reminds us of what is important in life.
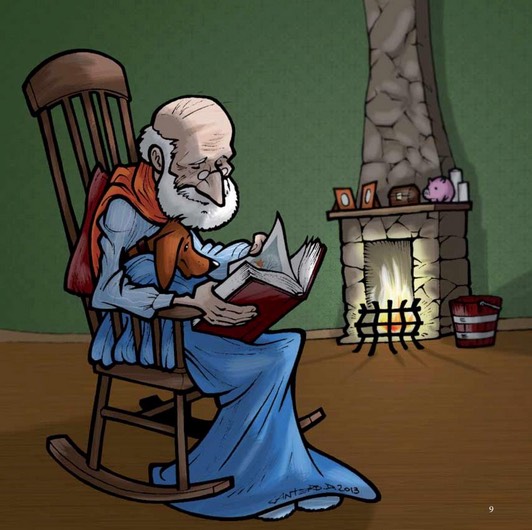
I was surprised by the quiet beauty that gently touched my heartstrings singing songs reminiscent of old times on my grampa’s farm…
The illustrations are equally touching and I’ve included a screenshot of one of my favorites.This one’s a keeper.
Thank you, Myste!
For those of you unfamiliar with Longfellow, allow me to introduce you.
Longfellow, the bravest and noblest weiner dog in the world… As our story begins, Longfellow is a puppy learning how to be a good friend to his human companions, Old Henry and Henry’s nurse Miss O’weeza Tuffy. By the end, he has grown old himself, but is still ready for one final adventure. What happens in between is an unforgettable and heartwarming tale that throws a tender light on the difficult truths of loss and longing as well as on our greatest hopes.
Three years ago, my father died in a fairly typical manner. His heart and his body had given out, he could barely move, he couldn’t feed himself and he was in diapers.
He was in a bit of pain, but the physical suffering was nothing compared to the emotional and psychological side of things. His life was gone and there was no joy in a day. He had no privacy and he hated having to be cared for as he lay in bed helplessly, a witness to his own lingering death, which finally arrived as a friend might, delivering the gift of mercy.
Maybe I’m not as brave as my father, but I knew then that I do not want to die that way and wouldn’t want my loved ones to experience the misery of watching me slowly dissolve.
In some circumstances, death may be the best remaining friend and it is reasonable and moral to accelerate the dying process.– Dan Maguire, professor, Marquette University
So what will I do? I don’t know. I wouldn’t be one to put a gun to my head, as some do. Maybe I’d stop eating and drinking water, but that can be a pretty miserable way to go too.
Gov. Brown, I don’t know if you read about this in my column, but I died once. Just after a knee operation, I went into cardiac arrest and flat-lined. That wouldn’t be a bad way to go, actually. No long, drawn-out affair. No messy stuff. But I was resuscitated, and I’m alive and well for the time being, and I’m asking you to give dying Californians the right to depart on their own terms.
No one seems to know what you will do with the End of Life Option Act that’s in your hands and would give us the same freedom people have in Oregon, Washington and elsewhere.
I know that our democracy is based on a separation of church and state, and that leaders such as you try not to let the tenets of their faith assert undue influence on secular decisions. I know too, however, that our values are usually set early and that religious beliefs are often core to who we are.
So it seems reasonable to note that the Catholic Church opposes what critics call assisted suicide and supporters call aid in dying, yet polls suggest most Catholics — as well as most Californians — want the option of going through a series of steps to get a life-ending prescription from a physician.
I know, governor, that you got a little farther than I did in the Catholic Church. You were a seminarian and I topped out at altar boy.
I don’t know if you still identify as a Catholic, but to me, any religion is about a search for meaning and we all know you’re a thoughtful — even spiritual — man who reflects, quotes Scripture and works from a set of basic moral principles.
So I wanted to share some conversations I’ve had with religious people who came to support aid in dying in the context of their experience and training.
“As a Christian I believe God is love,” the Rev. Ignacio Castuera once told me. “…And the God of love would not want any of God’s creatures to suffer undignified situations, especially at the end of life.”
Castuera grew up Catholic and is now a United Methodist Minister in Pomona. He told me about his ministry in West Hollywood during the AIDS epidemic, and he spoke of the honor of being with those who found a way to purchase life-ending medications and face death bravely with loved ones present.
“Death,” Castuera said, “is not the final stage for humans.” It is, in his mind, a deliverance to God.
The Rev. Sergio Camacho, a Methodist minister in Montclair, shares that view.
“Over the years, I’ve seen so many people dying, from brain tumors and other diseases,” he said. “It’s unbelievable how they suffer.… Before they go, they curse their families, they curse themselves, they curse God. It’s horrible, and God doesn’t want that. He wants us to go in peace. We need to think about this with merciful hearts.”
Dr. Robert Olvera, a Catholic physician and former altar boy who grew up in East Los Angeles, has supported aid in dying since watching his daughter die, at 24, from the leukemia she lived with for 17 years. She was blinded by her disease, he said, painkillers offered no relief and she suffered greatly.
“She was basically living in a black hole,” he said. “She had no quality of life.”
She was wasting away, her face was sunken, she did not want to be seen by anyone and she was in that state for the final three months of a life that ended last year.
“She begged me to give her some sleeping pills,” said Olvera, who couldn’t answer that request, knowing he could be criminally charged and lose his license to practice medicine.
Doctors can and do offer palliative sedation, but Olvera believes they should also have the right to grant a terminal patient’s wish to die at the time of their choosing, provided they are of sound mind and have satisfied the safeguards against abuse or coercion that are written into the end-of-life legislation.
I asked Olvera how he would respond to the argument that the timing of death is not something patients and doctors should decide; that should be left in God’s hands.
Doctors, he said, can unplug ventilators and they can answer a patient’s wish to be taken off dialysis. They can recognize that modern medicine has advanced to the point where people can be kept alive almost indefinitely, but all of us must ask whether, in some cases, we are extending life or prolonging death.
As both a physician and a Catholic, Olvera said, he believes no one should have to experience what his daughter did.
I understand that your education was Jesuit, Gov. Brown.
Well, Dan Maguire studied in Rome, became a Jesuit priest and now teaches moral theology at Marquette University, a Jesuit school. Here’s what he told me:
“For almost 50 years a number of Catholic theologians have taught that for the terminally ill, ending life may, at times, be the best that life offers. In some circumstances, death may be the best remaining friend and it is reasonable and moral to accelerate the dying process.”
According to Scripture, Maguire told me, we are made in the image and likeness of God, and it is our God-given right to decide for ourselves on matters such as aid in dying.
“Thomas Aquinas says with great wisdom that human actions are good or bad depending on the circumstances,” Maguire said. “In certain cases, you could say that life is good, and always to be served as best you can, but there are times when the ending of life is the best that life offers, and moral beings can make that decision for themselves…. That’s what human freedom means.”
It’s true, Gov. Brown, that some fear the life-ending option will be abused, and that those who are disabled or in a state of depression will choose inappropriately or be manipulated by relatives who stand to benefit financially.
It’s true, as well, that we need to be mindful of the potentially dangerous intersection of end-of-life options and cost-cutting by health insurance companies that have a financial disincentive in costly end-of-life procedures going on for long.
But I believe the legislation before you offers safeguards against abuses.
I don’t know if my father — who refused a feeding tube before his life came to a close — would have taken advantage of the End of Life Option Act, had it been available at the time.
I’m certain many people — probably most people — would want no part of it. That’s their choice and they should be entitled to the finest palliative care.
But I know that since writing about his death, I have heard from hundreds of Californians who would take a small measure of comfort in knowing that if they so choose, they can avoid physical or emotional suffering as the inevitable end nears. They believe that, as Dan Maguire put it, there comes a time when death is a friend.
Three terms that may arise in end-of-life care discussions are ‘withholding treatment’, ‘withdrawing treatment’ and ‘palliative sedation’. They are often misunderstood and sometimes confused with physician-assisted suicide or euthanasia. Understanding these terms can assist in decision-making and ensuring quality of life.
Palliative care is about achieving the best quality of life until the end of life. Each person’s situation, experience of illness, goals of care and approach to care are unique. Many factors influence the decision to withhold treatment, withdraw treatment or make use of palliative sedation. Each requires discussion and agreement between the patient and health care providers. If patients are not able to participate in these discussions, family members or substitute decision-makers are involved on their behalf.
Withholding treatment and withdrawing treatment
Traditionally, medicine has been focused on extending life. However as death approaches, extending life may not be in the best interests of the patient. A number of treatments and interventions can artificially extend life at end of life: certain medications, artificial nutrition, treatments such as dialysis, transfusions, radiation, and ventilation for breathing. It is important that patients and families understand the intent and possible risks or benefits of the care they are receiving. In Canada, people with advanced illness, or their substitute decision-makers, who are properly informed and able to make health care decisions can stop or decline treatment, even if that treatment might prolong life. While withholding treatment and withdrawing treatment refer to actions taken by health care providers, the actual decision to decline or discontinue treatment rests with the patient or the patient’s family or substitute decision-maker. Declining or discontinuing treatments that artificially extend life doesn’t mean that symptom control such as pain management and emotional support stop. Care and treatment focused on maintaining comfort continue, allowing the person to die naturally from the disease.
The first three cases below are examples of withdrawing and withholding treatment in the case of advanced disease. The cause of death in each case is the underlying illness. The intention of the plan for care is to treat symptoms and keep the patient as comfortable as possible but not prolong the natural dying process.
Case 1
Withdrawing treatment: Linda wants to stop dialysis
Linda has had diabetes for many years and has developed kidney failure. She has been on dialysis to keep her kidneys functioning. Because of dialysis, she has lived long enough to see the birth of her great grandchild eight months ago. But Linda is now growing weaker; she can do less for herself and always feels tired, especially on her dialysis day. It is getting more difficult for her to get back and forth to the dialysis clinic, and she now thinks dialysis is only prolonging her dying. After discussing her thoughts and feelings with her adult children and health care team, Linda decides to stop the dialysis treatment. The health care team controls Linda’s symptoms caused by kidney failure and she dies two weeks later with her family at her side.
Case 2
Withdrawing treatment: Jorge wants to stop transfusions
For three years, Jorge has had leukemia, a cancer of his blood. The cancer has filled his bone marrow to the point that he can no longer make enough red blood cells to live without transfusions. Similarly, Jorge can no longer make enough white blood cells, so he has had a number of infections. At first, his body could fight off these infections with the help of antibiotics. Then he would feel better and have enough energy to enjoy his photography hobby and his life with his partner. But after the last few infections, Jorge’s energy has not returned enough for him to go out and take photographs. He spends most of his day sleeping and has found it harder to go to the hospital for blood transfusions. His partner and friends are willing to help him with everything. But he is struggling with feeling so dependent.
Jorge talks with his health care team about how his life is now. “I can’t take this anymore,” he says. His team reminds him that he can always decide not to treat another infection when it comes along. He has the right to say no to antibiotics since they no longer help him recover from the infections. He can also stop his transfusions if they no longer help. He has the right to decide to stop all treatments and let nature take its course. Jorge decides to stop the transfusions and to not receive antibiotics if he gets another infection. Jorge’s partner supports his decision. She has noticed changes in Jorge and that the treatments are no longer making him feel better. Two weeks later, Jorge gets an infection. He experiences some shortness of breath but his team controls it with small doses of pain medication. He dies peacefully several days later.
Case 3
Withholding treatment: Marjorie’s family declines life-prolonging treatments
Marjorie is a frail older woman living alone in her own home. She has always told her nephew and niece that if she can no longer live there and manage her own affairs, she doesn’t want to live long. “Don’t put me on machines if I am going to end up being spoon fed,” she has said. One day, in terrible pain from a sudden, dreadful headache, she calls her nephew. Her speech is slurred and he can hardly understand her. By the time he gets to her home, she is barely able to respond to him. When the ambulance comes, the paramedics put a tube down her throat to help her breathe. At the hospital, a scan shows Marjorie has had a massive stroke that she is unlikely to recover from. The emergency doctor explains that if she were to have any chance of surviving, the health care team would need to maintain the breathing tube and connect their aunt to a breathing machine. She would also need drugs to reduce the swelling in her brain. It is expected that even if she does wake up, Marjorie will have physical and maybe cognitive impairments, will not be able to live alone, and will need help with all of her care.
Marjorie’s nephew is her next-of-kin and her substitute decision-maker. He knows that she would not want to live if she were unable to be independent in her own home. He asks if there are any other options. The emergency doctor tells him that since she has almost no chance of returning to her former life, Marjorie’s nephew could decide to remove the breathing tube and not to start the medication to reduce the swelling in her brain. The health care team would focus on treating any pain or other symptoms that she might have and allow her to die a natural death. Since that seems most in keeping with Marjorie‘s wishes, her nephew agrees. He and her niece stay with her until she dies 12 hours later.
Case 4
Withholding treatment: Mabel’s family decides against a feeding tube
Mabel is an 88-year-old woman who has lived with dementia for three years. In recent months she has become weaker, unable to walk, spends most of her day in bed and is having increasing difficulty swallowing food or fluids without coughing. Her daughter worries that she will “starve to death”. The doctor and staff share information with her daughter about the typical course of dementia, and how interest and intake of food and fluids diminishes. After talking with the staff and reading articles on this topic, the daughter understands the natural progression of dementia and that her mother will not experience hunger. She agrees to focus on good end-of-life care that includes sips of fluids or careful hand feeding if her Mom is awake and able to safely swallow, or good mouth care to prevent dryness.
What About Food And Fluids?
Towards the end of a progressive, life-limiting illness, people reach a point where they can no longer eat or drink. They may be too weak and unable to swallow, or always sleeping. When people become too weak to swallow, they may cough or choke on what they are trying to eat or drink. Providing food and fluids at this point usually requires a feeding tube. These tubes can be placed through the nose into the stomach, or they can be surgically placed directly into the stomach through a hole in the wall of the abdomen. At such an advanced point in an illness, our body systems are shutting down and our bodies are not able to use the calories in food. People understandably may be concerned that if someone is not being fed, they are being ‘starved to death’. However in these situations, it is the illness that determines the point where food can no longer be taken in; even if it could be, the body would not be able to use it to become stronger or to live longer. Hunger tends to be absent, and the sensation of thirst is typically related to dryness of the mouth, which can be addressed with good mouth care.
Feeding with the help of medical devices – including feeding tubes – is a medical procedure, similar to providing antibiotics or blood transfusions through an intravenous (“IV”). Therefore, when an advanced illness progresses to the point that someone can no longer eat or drink, the person or substitute decision-maker can indicate that a feeding tube is not wanted as it would only artificially prolong the final phase of illness.
This is a controversial and emotional issue as providing food and fluids feels like a basic way people nurture and care for each other. Nonetheless, patients and substitute decision-makers have the right to decline medical or surgical procedures such as inserting feeding tubes and other medical devices.
Palliative sedation
Palliative sedation involves giving medications to make a patient less aware, providing comfort that cannot be achieved otherwise. A legal and ethical practice in Canada, its goal is not to cause or hasten death but to keep the person comfortable until death. The decision to begin palliative sedation is made after an in-depth conversation between the patient (if able) or the family or substitute decision-maker, and the physician. Palliative sedation is considered a last resort in the last days of life, when all possible treatments have failed to relieve severe and unbearable symptoms such as pain, shortness of breath, or agitation from confusion.
While the person is sedated, the health care team monitors and reviews his or her condition and comfort and the family’s reaction to the treatment. The medications and dosages can be adjusted, resulting in a range from a slight calming effect to full sleep. The sedation can also be reversed, so the person is not completely asleep during the dying process. Research has shown that palliative sedation does not shorten life. People die from their disease – not from sedatives.
The two cases below are examples of how palliative sedation eases suffering and keeps a person comfortable until he or she dies from disease.
Case 5
Palliative sedation: Jim is confused, agitated and frightened
Jim has severe liver failure from hepatitis C. He can’t have a liver transplant because of other medical problems. His liver is not cleaning his blood as it should and toxins are building up in his blood. The toxins are causing confusion and in the end will cause death in less than a week. Until two days ago, Jim was able to understand and agree to his treatment. Now, he tries to get out of bed during the night, doesn’t recognize his family, and is agitated and frightened. Jim’s family is distressed.
Jim’s health care team does some tests to see what is causing his confusion and agitation. The team finds that his liver function is extremely poor, and there are no other causes for his distress they can correct. This type of confusion is called delirium. Since the medications usually used to control mild to moderate delirium are not effective, the health care team and Jim’s family meet to discuss further treatment. The health care team recommends sedation to allow Jim to rest in bed and feel calm. The family agrees and the medication is given. Jim receives enough medication to help him lie peacefully in bed, and sleep comfortably. On the third day, the team reduces the medication, but Jim again becomes restless and agitated, so the medication is increased to the point where he is resting comfortably. Jim dies comfortably from his illness on the fourth day with his family at his bedside.
Palliative sedation: Roberto wants to see his children one last time
Roberto has cancer which has spread to his liver and lungs. A large tumour in his pelvis where the cancer recurred causes him severe pain. He has received chemotherapy and radiation therapy, and is receiving multiple pain medications. Until two weeks ago, Roberto’s pain was under control. Then he came to the hospital seeking relief. Roberto is becoming weaker every day. He is likely to die in the next week because of the cancer in his liver and lungs. He desperately wants to live until his ex-wife brings his two young children to visit; however they no longer live in the same city. Although the health care team is controlling his pain as much as possible, Roberto is distressed by the pain and the waiting.
The team offers Roberto some sedation to make him unaware of his pain and reduce his distress. They promise they will reverse the sedation when his children arrive. Roberto agrees and the team starts the medication, increasing the dosage until Roberto is able to sleep. Roberto sleeps for a day and a half. When the team knows Roberto’s children are about to visit, they stop the sedation, and he is able to see them for the last time. After their visit, Roberto chooses to be sedated because of his pain. He dies two days later from his cancer.
Patients and families living with advanced illness will be faced with many decisions related to their care. It is important that they be able to discuss the risks and benefits of possible treatments and interventions with their healthcare team so that they can make informed decisions that are consistent with their goals of care
SOME PEOPLE JUST want to die. Not because they are trapped by depression, anxiety, public embarrassment, or financial ruin. No, these poor few have terminal illnesses. Faced with six months to live, and the knowledge that the majority of those 180 days will be bad ones, they seek a doctor’s prescription for an early death.
Soon, terminal patients in California could have that option. Currently sitting on Governor Jerry Brown’s desk is a bill that, if signed into law, would allow doctors to prescribe life-ending drugs. Not surprisingly, this is controversial. Proponents believe the law would save diseased people from the worst days of their prognoses. Opponents say the law violates the sanctity of life, and can be exploited by ill-meaning family, physicians, and insurance companies at the patient’s expense.
But there’s a third group who believe this debate misses the real problem: that the American health care system is just an all around miserable place to die.
In the 1990s, Dr. Jack Kevorkian’s name became synonymous with so-called assisted suicide. He argued, famously and flamboyantly, that patients should have the right to euthanasia if the suffering from age, disease, even mental illness overwhelmed their will to live. “The patient’s autonomy always, always should be respected, even if it is absolutely contrary, the decision is contrary to best medical advice and what the physician wants,” he once said in court.
Kevorkian lost his court battles, and spent eight years in a Michigan prison. But his fight was not in vain. Four states have since legalized physician-aided death (and would-be fifth New Mexico has a law in legal review). The first was Oregon, and its Death With Dignity Act has become the model for the rest. There the patient must first have a six-months-to-live prognosis. Then, the patient has to write a request to the physician (who may refuse on moral grounds). Two witnesses have to sign that request, one of whom is not related to the patient, not in the patient’s will, and not the patient’s physician or an employee of the patient’s health care facility.
If the first doctor approves the request, the patient has to give it to a second doctor, who examines medical records to confirm the diagnosis and make sure the patient has no mental illnesses that might affect his or her decision-making ability. After a fifteen-day waiting period, the patient has to confirm that he or she still wants the doctor’s aid in dying. Only then will the doctor prescribe the lethal prescription. And the patient is under no obligation to take it, either.
In fact, since it was passed into law, only about 65 percent of the 1,327 people prescribed the medication have used it.
Raising the stakes in California
On December 31, 2013, California resident Brittany Maynard had a master’s degree in education, several years of experience teaching abroad in orphanages, and a husband. On January 1, 2014, she had stage two brain cancer. She went through surgery, and the doctors cut away the cancerous parts of her brain. But in April, the disease returned. Stage four glioblastoma, with little hope of treatment. Her doctor informed her she had six months to live.
Given the choice, Maynard said she would rather die before the cancer’s debilitating final stages destroyed her health completely. A few months later, she moved from California to Oregon.
Maynard took her lethal dose of medication on November 1, 2014. Her last message, posted on her Facebook profile, read:
“Goodbye to all my dear friends and family that I love. Today is the day I have chosen to pass away with dignity in the face of my terminal illness, this terrible brain cancer that has taken so much from me … but would have taken so much more.”
Maynard’s broadcasted decision put the public behind California’s bill. Like the other states’ laws, it is modeled after Oregon’s, with some some add-ons meant to assuage opponents. California patients would have to request aid in dying three times instead of twice. “The physician who prescribes the medication must have a one-on-one conversation with the patient, to verify that it is their choice, and that no one is putting any pressure on the patient,” says Ben Rich, a lawyer and expert in end-of-life bioethics, from the University of California, Davis. And after ten years, the law would expire.
Missing the point
But for some in the palliative care community—the doctors, nurses, and caregivers that manage end-of-life care—the battle over aid in dying is a distraction from the real problems that dying people face. “I think it’s a moot debate that’s divorced from the reality of end-of-life care,” says David Magnus, a bioethicist at Stanford Medical School. That reality is clear in a report published last year by the Institute of Medicine of the National Academies of Science.
Titled Dying in America, it showed that patients often can’t get—or don’t know about—the type of treatment they actually need to be comfortable and pain-free in their final months, weeks, days, and hours. This is probably tied to the fact that America only has half as many palliative care physicians as it needs.
That’s not all. Magnus says insurance companies favor big lifesaving efforts and shiny technology. “We put a lot of emphasis on technology and innovations, and this tends to downgrade communication,” says Magnus. And clear communication about death is probably the first prescription is probably what most terminal patients need most.
As a result, patients end up getting treatment that doesn’t help them have a more comfortable death. In fact, it become the opposite. “You’ve got a patient who is sick, going though a roller coaster ride,” says Magnus. This includes cycles of chemotherapy and remission, trips to surgery to intensive care to therapy to home, then back again. “And each time, it’s much more difficult on the patient and on the patient’s family,” he says.
“A lot of what we see are patients who have some sense that their condition is bad but are not told explicitly how bad their prognosis is,” says Magnus. For example, many patients don’t understand the difference between palliative and curative treatments. “When they hear that their condition is treatable, they think there is a chance that they can be cured,” says Magnus. But treatable, to physicians talking to a terminal patient, often mean simply easing that patient’s suffering. Treatable has nothing to do with living or dying.
Palliative communication
Other studies back up Dying in America. Last year, scientists published in the Journal of Oncology that with better communication, more terminal patients might choose hospice rather than more radiation or chemotherapy. A2005 study showed that doctors regularly missed opportunities to convey information to patients that would affect their decisions about end-of-life care. Magnus has also done research on doctor-patient communication, and what he sees is usually pretty dismal.
“The caveat, is it’s very hard to communicate bad news to families,” says Magnus. He says it’s understandable that doctors hedge their discussions towards the positive. This goes back to the end-of-life training that doctors do not receive in medical school.
But until the medical system gets fixed (don’t hold your breath), patients can circumvent the assisted death circus by getting advanced care directives, such as a living wills. These are legal documents that outline how you should be treated in the event of a severe illness, accident, or just plain growing old. “100 percent of us are going to die, and only a quarter of Americans have engaged in formal advanced care planning,” says Nathan Kottkamp, founder and chair of National Healthcare Decisions Day, which advocates that people use April 16 to sit down, discuss, and develop their advanced care plan. The groups website has resources for drafting up the legal documents in every state.
In California, Governor Brown has until October 71 to sign the aid in dying bill into law. While he hasn’t tipped whether his pen will enact or veto, he has criticized the legislative gymnastics that let supporters get the bill voted on without first going through scrutiny by committees. Adding to speculation that he may veto, Brown is also a former Jesuit seminarian (Catholic groups oppose the bill).
But the bill has a groundswell of public support. According to a bipartisan public opinion poll, 69 percent of Californians are in favor of physician-aided death. “Why is this touching a nerve? Why is it millions of people want these laws on the books?” asks Magnus. He doesn’t believe it’s because so many people are terrified of having a sickness steal away their preferred choice: Life. Rather, he says it speaks to a more common fears: dying in pain, without control, without dignity, surrounded by people they do not know in a place they do not want to be. The choice that concerns them is not whether to die, it’s how.
1 UPDATE: Correction 12:12am ET 9/30/2015 The original story said the enactment deadline was September 28. In California, the governor has 12 working days to act on bills (such as the End of Life Option Act) passed in special Assembly sessions. But, that time began when the bill landed on the governor’s desk (which was September 25), not when the bill cleared the Assembly (September 11). If the governor doesn’t sign or veto within that deadline, the bill automatically becomes law.
David Langton-Gilks died from a brain tumour in August 2012 at the age of 16 but before his death his mum Sacha planned a peaceful passing for him at home surrounded by his family
Loving: Sacha and David
Death. It’s the final taboo, isn’t it? Especially when it’s a child. We can’t – or won’t talk – about it.
Sacha Langton-Gilks, the lead champion for The Brain Tumour Charity’s HeadSmart campaign for earlier diagnosis of brain tumours in children and young people shatters that taboo.
To help other parents, she talks about how her son David, who died from a brain tumour in August 2012 at the age of 16, had a peaceful death at home surrounded by his family.
She emphasises that, just like we make birth plans, we should make death plans and how being able to die peacefully at home was her last act of love for her cherished son.
Family: David Langton-Gilks before his death with his mum Sacha
Here Sacha tells her story:
Days before he died, the last lucid words my 16-year-old son David, or DD as we like to call him, said were: ‘I love it here.’ He was looking out his bedroom window into the treetops where, at night, owls – one of his passions – would come to call.
It was just a few days before London 2012 Paralympics and for five years, since being diagnosed with an aggressive, cancerous brain tumour at the age of 11, DD had endured everything globally available on the NHS, including 11 brain operations, years of chemotherapy, weeks of radiotherapy, blood transfusions and a stem cell transplant.
His cancer had now spread down his spine and throughout his brain, leaving him with severe dementia. Unfortunately someone’s child has to be in the 25 percent that don’t survive this type of brain tumour, a medulloblastoma .
Smile: David Langton-Gilks before his death which left his family devastated
Three years on, I can honestly say that giving my child a ‘good’ death – without pain, calm and comfortable in his own bed, in the arms of his family with his beloved cat sitting on the bed, will be my greatest life achievement. And it gives me immense comfort in my grief.
I am speaking out to break a taboo because I remember the silence that hung over parents in the children’s cancer ward when a family ‘went home.’
We all knew that meant the child was going to die but no one could say it.
Fear overwhelmed us. If you cannot even say the word, how are you going to be able to discuss what choices best suit your family for end of life care?
Mum: Sacha Langton-Gilks, the lead champion for The Brain Tumour Charity’s HeadSmart campaign
With brain tumours being the biggest cancer killer in the UK of children and adults under 40, The Brain Tumour Charity’s feedback from many parents is that they feel completely isolated with no information.
Even doctors do not say the D word because they have been trained to ‘fix’ things and view death as somehow a failure on their part.
But I see my doctors and nurses as geniuses for enabling a fabulous quality of life for my child right up to his death. This taboo about death has to be shattered so that we can improve how we care for our loved ones at the end of their lives.
When I was asked to give a speech to parents and doctors at The Brain Tumour Charity’s first paediatric brain tumour information day about how we managed DD’s death, the process itself, I didn’t know if I could do It. But then I remembered that voiceless fear in parents’ eyes at the hospital.
I call this an ‘ante-mortem class’ – one parent sharing their experience with another parent just as you would at an ante-natal class.
After all, you wouldn’t dream of giving birth without talking to another mum, reading books or going to a class, would you?
Lack of information about end of life care for children breeds fear and stops parents from even being able to articulate questions to their doctors.
Tough: David before his death with his family
On top of this is our society’s obsession with being ‘positive’ with hope. The fear that somehow by saying the D word means we ourselves might have made it happen by not being positive enough, by giving up hope. It is our punishment for being cowards.
But death is part of life and comes to us all. So how can it be negative or positive? It just is what it is – ceasing to be.
When we ‘went home’ after DD’s final scan in May 2012, which showed his cancer was everywhere and he had weeks to live, we were not doing nothing or stopping treatment – there was a detailed advanced care plan in place.
He was having full palliative care treatment co-ordinated by Southampton General Hospital which included Gold Standards Framework for end of life care at our GP’s surgery and also involved Marie Curie.
It centred on the relief of his symptoms of pain and vomiting to give him quality of life.
It just was not curative treatment as this was no longer possible.
Tragic: David Langton-Gilks before his death
But we still had hope – we had changed that hope from one that DD could be cured to one where he had the best quality of life possible in the limited time he had left.
Some people do a bucket list, but DD just wanted to hang out at home with me and his dad Toby, his brother Rufus, now 17, and sister Holly, now 13.
He didn’t want to spend another second in hospital and wanted to have a party with his friends. So we did.
If we had not faced up to the fact that he was going to die soon, we would have spent hours of that incredibly precious time in hospital trying to convince ourselves that the chemotherapy on offer would cure him.
DD would have hated it and we’d have been traumatised by each successive scan, contradicting what we longed to see.
My biggest agony was knowing that helping my child to suffer less meant I might have less time with him.
Nothing will ever be as painful as letting DD go, but how could I have made him suffer pain on my account? That would have made me the most selfish mother alive and I couldn’t have lived with that.
So the biggest battle was actually me.
In Childhood Cancer Awareness Month, from one parent to others going through the same thing, as a gift from my heart, I am sharing how my son died to shatter the taboo and make your battle less.
Traditional, mythic accounts of the origin of death extend back to the earliest hunter-gatherer cultures. Usually these stories are morality tales about faithfulness, trust, or the ethical and natural balance of the elements of the world.
In Asante Culture the death of a person is seen as a blow to the entire community and everybody shares the grief.
According to an African Asante myth, although people did not like the idea or experience of death, they nevertheless embraced it when given the choice, as in the tale of an ancient people who, upon experiencing their first visitation of death, pleaded with God to stop it. God granted this wish, and for three years there was no death. But there were also no births during that time. Unwilling to endure this absence of children, the people beseeched God to return death to them as long as they could have children again.
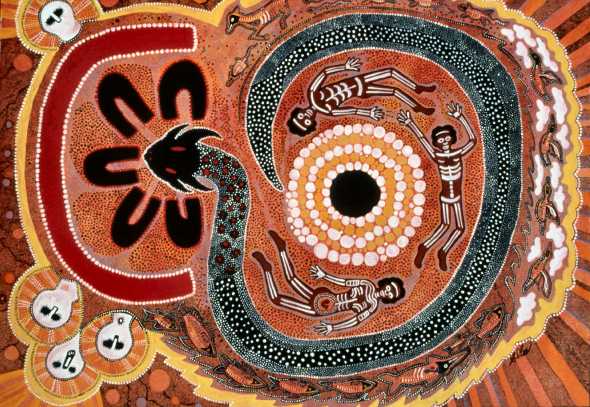
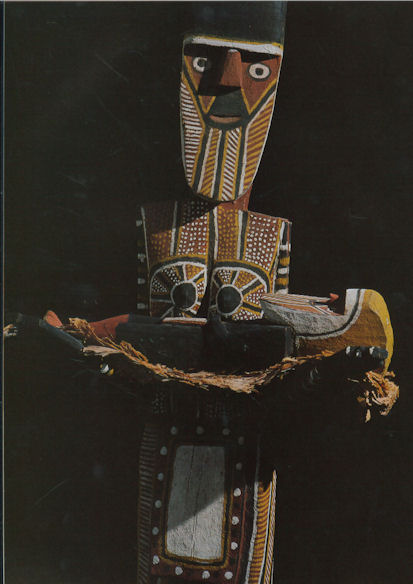
The death myths of aboriginal Australia vary enormously among clans and linguistic groups. Among most of them, however, death is often attributed to magic, misfortune, or to an evil spirit or act. Occasionally death is presented as the punishment for human failure to complete an assignment or achieve a goal assigned by the gods. Still other stories arise from some primordial incident that strikes at the heart of some tribal taboo. Early myths about death frequently bear these moral messages.
Among the Tiwi of Bathurst and Melville Islands in northern Australia, the advent of death is explained by the Purukapali myth, which recounts a time before death entered the world, when a man lived with his infant son, his wife, and his younger brother. The younger brother was unmarried and had desires for his brother’s wife. He met her alone while she was gathering yams, and they spent the rest of the afternoon in sexual union. During this time, the husband was minding his infant son, who soon became hungry. As the son called for feeding, the husband called in vain for his missing wife. At sunset, the wife and younger man returned to find that the infant son had starved to death. Realizing what had happened, the husband administered a severe beating to his brother, who escaped up to the sky where he became the moon. His injuries can still be seen in the markings of the moon every month. The husband declared that he would die, and, taking the dead infant in his arms, performed a dance—the first ceremony of death—before walking backwards into the sea, never to be seen again.
The Berndts, Australian anthropologists, tell another ancient myth about two men, Moon and Djarbo, who had traveled together for a long while but then fall mortally ill. Moon had a plan to revive them, but Djarbo, believing that Moon’s idea was a trick, rebuffs his friend’s help and soon dies. Moon dies also, but thanks to his plan, he managed to revive himself into a new body every month, whereas Djarbo remained dead. Thus, Moon triumphs over bodily death while the first peoples of that ancient time followed Djarbo’s example, and that is why all humans die.
Death As a Being
None of these stories is meant to suggest that aboriginal people do not believe in spiritual immortality. On the contrary, their lore is rich in accounts of immortal lands. These are accounts of the origin of physical rather than spiritual death.
The idea of death as a consequence of human deeds is not universal. The image of death as a being in its own right is common in modern as well as old folklore. In this mythic vein, death is a sentient being, maybe an animal, perhaps even a monster. Sometimes death is disguised, sometimes not. Death enters the world to steal and silence people’s lives. In Europe during the Middle Ages death was widely viewed as a being who came in the night to take children away. Death was a dark, hooded, grisly figure—a grim reaper—with an insatiable thirst for the lives of children. Children were frequently dressed as adults as soon as possible to trick death into looking elsewhere for prey.
The film industry produced two well-known films, the second a remake of the first, which examined this idea of death as a being who makes daily rounds of collecting the dead: Death Takes a Holiday (1934) and Meet Joe Black (1998), both of which portrayed death as perplexed at his victim’s fear of him. In a wry and ironic plot twist, a young woman falls in love with the male embodiment of death, and it is through an experience of how this love creates earthly attachment that death comes to understand the dread inspired by his appearance.
But the idea of death as a humanlike being is mostly characteristic of traditional folktales that dramatize the human anguish about mortality. By contrast, in the realm of religious ideas, death is regarded less as an identifiable personal being than as an abstract state of being. In the world of myth and legend, this state appears to collide with the human experience of life. As a consequence of human’s nature as celestial beings, it is life on Earth which is sometimes viewed as a type of death. In this way, the question of how death enters the world in turn poses the question of how to understand death as an essential part of the world.
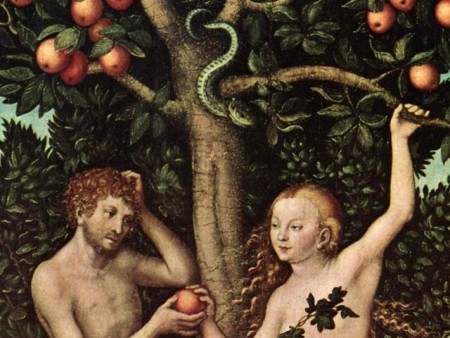
The Garden of Eden
In the book of Genesis, the first man, Adam, wanders through the paradisiacal Garden of Eden. Pitying his solitary nature, God creates the first woman, Eve, from Adam’s rib. Adam and Eve are perfectly happy in the Garden of Eden and enjoy all its bounty with one exception: God prohibits the couple from eating from the Tree of Knowledge.
The Garden of Eden is utopian. Utopia, in its etymological sense, is literally “no place.” It is a perfect, probably spiritual domain for two celestial beings who, bearing the birthmarks of the God who created them, are immortal. These two beings eat from the Tree of Knowledge, which ironically, distracts them from their awareness of God and his omnipresence. As a result of this error, Adam and Eve become the embodiment of forgetfulness of the divine. In other words, they become material beings, as symbolized in their sudden awareness of and shame in their nakedness.
Adam and Eve thus “fall” into the flesh, into the world as it is known, with the entire legacy that embodiment entails: work, suffering, and physical death. Paradoxically, the Tree of Knowledge heralds ignorance of their divine nature, and the fall into flesh signals their sleepwalking indifference to that nature. Human beings therefore need God’s help through the divine mercy of his Son or the sacred texts of the Bible to awaken them to their divine destiny. Without this awakening, the wages of sin are eternal death—an eternal darkness spent in chains of ignorance, a blindness maintained by humans’ attachment to mere earthly concerns and distractions. This famous story thus embodies all the paradoxical elements of creation, implying that human life is actually no life at all, but its opposite: death.
In the kernel of this local creation story lies the archaic analogy of all the great stories about how life is death and death is the beginning of true life. The cycles of life and death are not merely hermeneutic paradoxes across different human cultures, but they are also the fundamental narrative template upon which all the great religions explain how death entered the world and, indeed, became the world.
In Greek mythology, as Mircea Eliade has observed, sleep (Hypnos) and death (Thanatos) are twin brothers. Life is portrayed as a forgetfulness that requires one to remember, or recollect, the structures of reality, eternal truths, the essential forms or ideas of which Plato wrote. Likewise, for postexilic Jews and Christians, death was understood as sleep or a stupor in Sheol, a dreary, gray underworld in the afterlife. The Gnostics often referred to earthly life as drunkenness or oblivion. For Christians, the exhortation was also to wake from the sleep of earthly concerns and desire and to watch and pray. In Buddhist texts, the awakening is a concern for recollection of past lives. The recollection of personal history in the wheel of rebirth is the only hope anyone has of breaking this cycle of eternal return.
Sleep, then, converges with death. Both have been the potent symbols and language used to describe life on earth. It is only through the remembering of human’s divine nature and its purpose, brokered during an earthly life of asceticism or discipline, or perhaps through the negotiation of trials in the afterlife, that one can awaken again and, through this awakening, be born into eternal life.
Modern Accounts
The humanistic trend of twentieth-century social science and philosophy has diverged from this broadly cross-cultural and long-standing view of death as earthly existence and true life as the fruit of earthly death. Contemporary anthropology and psychoanalytic ideas, for example, have argued that these religious ideas constitute a “denial of death.” The anthropologist Ernest Becker and religious studies scholar John Bowker have argued that religions generate creation myths that invert the material reality of death so as to control the anxiety associated with the extinction of personality and relationships.
Like-minded thinkers have argued that philosophical theories which postulate a “ghost in the machine”—a division of the self into a body and a separate spirit or soul—are irrational and unscientific. But, of course, the assumptions underlying these particular objections are themselves not open to empirical testing and examination. Criticism of this kind remains open to similar charges of bias and methodological dogma, and tends, therefore, to be no less speculative than religious views of death.
Beyond the different scientific and religious arguments about how life and death came into the world, and which is which, there are several other traditions of literature about travel between the two domains. Scholars have described the ways in which world religions have accounted for this transit between the two halves of existence—life and death. Often, travel to the “world of the dead” is undertaken as an initiation or as part of a shamanic rite, but at other times and places such otherworldly journeys have been part of ascetic practices of Christians and pagans alike.
In the past half century psychological, medical, and theological literature has produced major descriptions and analyses of near-death experiences, near-death visions, visions or hallucinations of the bereaved, and altered states of consciousness. Research of this type, particularly in the behavioral, social, and clinical sciences, has reignited debates between those with materialist and religious assumptions about the ultimate basis of reality.
Traditionally confined to the provinces of philosophy and theology, such debates have now seeped into the heretofore metaphysics-resistant precincts of neuroscience, psychology, and medicine. What can these modern psychological and social investigations of otherworldly journeys tell experts about the nature of life and death, and which is which?
The religious studies scholar Ioan Peter Couliano argues that one of the common denominators of the problem of otherworldly journeys is that they appear to be mental journeys, journeys into mental universes and spaces. But such remarks say more about the origin of “mental” as a term of reference than the subject at hand. The glib observation that otherworldly journeys may be mere flights of fancy may in fact only be substituting one ambiguous problem with yet another.
As Couliano himself observes, people in the twenty-first century live in a time of otherworldly pluralism—a time when such journeys have parallels in science and religion, in fantasy and fact, in public and private life.
Conclusion
Death has permeated life from the first stirrings of matter in the known universe—itself a mortal phenomenon, according to the prevailing cosmological theory of contemporary physics. Death came incorporated in the birth of the first star, the first living molecules, the birth of the first mammoth, the first cougar, the first human infant, the first human empire, and the youngest and oldest theory of science itself. Early cultures groped with the meaning of death and its relationship to life. The very naming of each, along with the attendant stories and theories, is an attempt to somehow define and thus master these refractory mysteries. All of the major myths about how death entered the world are, in fact, attempts to penetrate below the obvious.
Most have concluded that Death, like Life, is not a person. Both seem to be stories where the destinations are debatable, even within their own communities of belief, but the reality of the journey is always acknowledged—a continuing and intriguing source of human debate and wonderment.
“I live my sadness every day, but I don’t resent it any more,” Zelda Williams recently wrote in an Instagram post about depression and grieving her father, the late Robin Williams. “I do it now so that the wonderful moments of joy I do find are not in order to forget, but to inhabit and enjoy for their own sake.”
Williams is certainly not the only one grappling with the complex process of grief. Most people experience loss at some point in their lives. Yet stigmas and rigid stereotypes about the experience persist. Here are eight lies we need to stop perpetuating about the simultaneously universal yet deeply personal experience of grief.
1. Grief is finite.
“Society as a whole is extremely understanding when it comes to acknowledging that the days immediately following a loss are hard,” Vivian Nunez, founder of the organization Too Damn Young, told Mic. But after the funeral has been planned and final goodbyes said, “the understanding begins to dwindle.”
People are expected to “get over their grief, move on and have closure,” psychologist and grief counselor Heidi Horsley told Mic.
But in reality, grief is an individual process that arguably may never definitively end.
“Loss has a very long arc,” Rebecca Soffer, co-founder and CEO of Modern Loss, told Mic. “It’s something you live with in various forms throughout the rest of your life.”
Though sometimes interminable, grief is a dynamic process that becomes incorporated into one’s life.
“We transform our grief, but we don’t get over it,” Horsley said. Nunez described grief as an emotion that “morphs into something you learn to walk alongside of, but it never goes away.”
2. Grief is a linear progression.
On Grief and Grievingauthors Elisabeth Kübler-Ross and David Kessler write that there are five stages of grief: denial, anger, bargaining, depression and acceptance. But while these stages may provide a useful framework, “grief is as individual as our lives,” rather than a concrete, universal timeline.
“There’s a bigger chance of you jumping between stages than there is that you’ll go in order,” Nunez said.
“There’s literally no rhyme or reason to what you’re going to go through because every human being is different, every loss experience is different,” Soffer said. “Loss is a very complex process.” It’s rare to have had complete closure with a loved one before losing them, which means stages of grief can manifest in “a completely haphazard format with endless permutations and combinations,” she added.
3. There’s a “right” way to grieve.
Grieving individuals often feel caught in a double standard of emotionality: Especially beyond a certain age, people are often regarded as cold-hearted if not emotional enough or wallowing if their grief is too palpable. Should they fall somewhere in the middle, as many do, they may feel judged, or misunderstood.
Teens and young adults who participate in the Too Damn Young community often experience this, Nunez said, and feel “ashamed” or like “they’re carrying baggage” when their grief “doesn’t fit a set norm or the one-size-fits-all formula.”
“So many people were expecting me to be crying 24/7,” one community member, 18-year-old Selena, told Mic of her experience after losing her mother. “When I went back to school, everyone was staring at me waiting for me to break down in the middle of the room.”
“The way a person grieves is very much their own to experience,” Nunez said. “Unless you’re harming yourself or others, there’s no wrong way to grieve. No two grief experiences are the same, but there is comfort in knowing we all start from the same place — the simple fact we’ve lost someone.”
Ultimately, “everyone has their own ways of coping, and whatever is working for you is the right way for you,” Selena said. “Don’t feel bad if you aren’t crying all day. Don’t feel bad if you’re not a complete mess.”
4. There’s a right way to support somebody who is grieving.
The single worst thing one can say to somebody who is grieving, according to Horsley? Nothing.
“People feel like if they say something it might upset you, but by saying nothing, you’re not acknowledging that anything ever happened,” Horsley said.
Acting as a sounding board for those experiencing loss may be the best approach, Soffer said. Some may worry that the reminder of their loss will cause more emotional damage, she said, but asking them about the person they lost and asking them to tell stories about them can be helpful to them. That’s the idea behind the Too Damn Young community’s campaign #TellUsAboutThem.
“The goal is to remind people that our loved ones are more than just their deaths, they are the lives and moments they lived before they died,” Nunez said.
5. Either make a sweeping gesture or don’t bother.
There are easy ways one can acknowledge and support others’ loss — like setting a calendar reminder to check in with a grieving friend, Soffer suggests. A simple task like cleaning for them or bringing them dinner can be just as meaningful, if not more, than a concerted, serious conversation about their loss.
Support can also take the form of moderating one’s own reaction to those who are grieving. “You have no idea what’s going on behind closed doors,” Soffer said. “Try and stop yourself if they do something to frustrate you, or are a little obnoxious. Just remember that they’ve gone through something that’s really profoundly sad and life-altering and identity-altering and give them the benefit of the doubt.”
While supportive gestures likes these need not be daunting, Soffer said, they should go beyond a text or a Facebook like. While doing so may make grieving individuals briefly feel better, she encourages people to “use these amazing tools of connectivity to be a trigger for more thoughtful action.”
6. Other factors of one’s identity are irrelevant to their grief.
Gender may uniquely affect one’s response to loss, according to the experts.
“Men tend to grieve shoulder to shoulder, not face to face,” Horsley said. Men “have been socialized to suck it up, walk it off, that real men don’t cry,” she said, but “women haven’t been socialized with those kinds of beliefs.”
Research backs this up: According to a study released by the Comfort Zone Camp, 38% of women, compared to 29% of men strongly agreed that losing a parent in childhood was “the toughest thing [they] ever had to deal with.” While 57% of men who had lost a parent in childhood surveyed agreed that people need to get over death because it’s part of life, only 36% of women agreed.
On the other hand, men who lose their wives “are often unprepared,” Rochester Institute of Technology professor Javier Espinosa, a lead researcher of the study, told the Telegraph. Men’s health may be affected more by losing “their caregiver, someone who cares for them physically and emotionally,” than women who lose their husbands, since “this same mechanism is likely weaker,” Espinosa said.
Age can also be hugely impactful. “There are different challenges that come with grieving as a young person because you’re figuring yourself out a bit more,” Nunez said. “When a significant person in your life dies, you begin to ask the bigger questions at a much younger age. It’s hard to face mortality at an age when you feel as though you and those around you are essentially invincible.”
7. Talking about it is morbid and inappropriate.
“I was once a kid in a classroom, under the age of 20, who had lost her mom, and I never knew anyone else who had,” Nunez said. “This is where having a conversation around grief could significantly impact those who are in the shadows about those they lost.”
Soon after Nunez launched Too Damn Young, she received multiple emails confirming she wasn’t the only one who felt they couldn’t discuss the experience of loss.
Surrounding oneself with others who have experienced loss and sharing those experiences, Horsley said, can be hugely beneficial.
“When you’re with other people who have been there and made it, you know you can too,” she said. “You’re not alone and other people have been on this journey of grief that you’re on. You need to reach out and grieving in community is a great way to find hope.”
8. You should feel guilty about moving on.
“Sometimes we hold on to the pain even longer than we need to because the pain represents that person and the loss, and we feel guilty about moving forward and moving farther away from them, even though the reality is when we’re in a positive space,” Horsely said.
But in reality, moving past grief can be an enlightening experience all its own.
“When you experience a loss like this, you get to see a really wild new amount of life,” NPR producer Rachel Ward wrote in a Medium blog post about her experience losing her husband. “Suddenly the range of the type of sad you can feel, to the type of happy you can feel, is busted open. The spectrum from happy to sad isn’t a foot wide anymore ?—? it’s as far as your arms can stretch and then to the edges of the room and then up the block and over into the next neighborhood.”
Ultimately, Ward noted, grief — and life more generally — is not about seeking or even achieving constant contentment. Rather, she wrote, she found that accepting the feeling of “being uncomfortable is a very effective way to be a human.”

 Myste Lyn from Bittersweet Blessing shares her thoughts after reading the Longfellow book
Myste Lyn from Bittersweet Blessing shares her thoughts after reading the Longfellow book